
The Impact of SARS-CoV-2 Pandemic on Patients Undergoing Radiation Therapy for Advanced Cervical Cancer at a Romanian Academic Center: A Four-Year Retrospective Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Background, Design, and Ethics
2.2. Inclusion Criteria, Patient Characteristics, and Study Variables
2.3. Statistical Analysis
3. Results
3.1. Comparison of Baseline Characteristics
3.2. Comparison of Cervical Cancer Characteristics
3.3. Comparison of Radiotherapy Characteristics
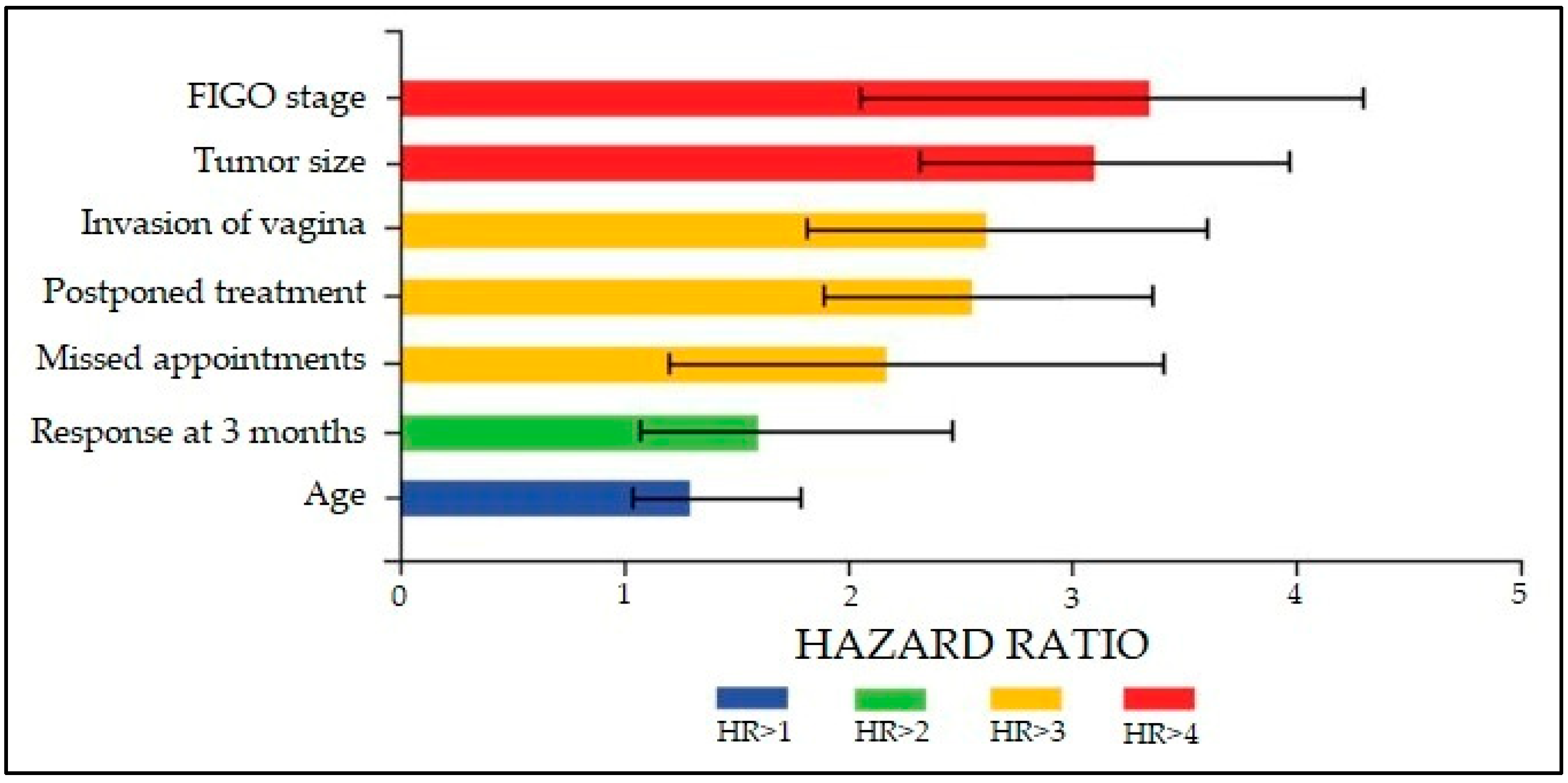
3.4. Cox Regression Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Castanon, A.; Tataru, D.; Sasieni, P. Survival from Cervical Cancer Diagnosed Aged 20–29 Years by Age at First Invitation to Screening in England: Population-Based Study. Cancers 2020, 12, 2079. [Google Scholar] [CrossRef] [PubMed]
- Daponte, A.; Michail, G.; Daponte, A.-I.; Daponte, N.; Valasoulis, G. Urine HPV in the Context of Genital and Cervical Cancer Screening—An Update of Current Literature. Cancers 2021, 13, 1640. [Google Scholar] [CrossRef] [PubMed]
- Sladič, M.; Taneska, P.; Cvjetičanin, B.; Velikonja, M.; Smrkolj, V.; Smrkolj, Š. Cervical Intraepithelial Neoplasia Grade 3 in a HPV-Vaccinated Patient: A Case Report. Medicina 2022, 58, 339. [Google Scholar] [CrossRef]
- Okayama, K.; Kimura, H.; Teruya, K.; Ishii, Y.; Fujita, K.; Fujii, M.; Oda, M.; Sasagawa, T.; Okodo, M. Correlation between Human Papillomavirus Codetection Profiles and Cervical Intraepithelial Neoplasia in Japanese Women. Microorganisms 2020, 8, 1863. [Google Scholar] [CrossRef] [PubMed]
- Gil-Ibañez, B.; Gil-Moreno, A.; Torné, A.; Martín Jimenez, A.; Gorostidi, M.; Zapardiel, I.; Tejerizo Garcia, A.; Diaz-Feijoo, B.; on behalf of SEGO Spain-GOG Cervical Cancer Task Forcé. Tumor Size and Oncological Outcomes in Patients with Early Cervical Cancer Treated by Fertility Preservation Surgery: A Multicenter Retrospective Cohort Study. Cancers 2022, 14, 2108. [Google Scholar] [CrossRef] [PubMed]
- Popescu, A.; Craina, M.; Pantea, S.; Pirvu, C.; Radu, D.; Marincu, I.; Bratosin, F.; Bogdan, I.; Hosin, S.; Citu, C.; et al. COVID-19 Pandemic Impact on Surgical Treatment Methods for Early-Stage Cervical Cancer: A Population-Based Study in Romania. Healthcare 2022, 10, 639. [Google Scholar] [CrossRef]
- Margan, R.; Margan, M.-M.; Fira-Mladinescu, C.; Putnoky, S.; Tuta-Sas, I.; Bagiu, R.; Popa, Z.L.; Bernad, E.; Ciuca, I.M.; Bratosin, F.; et al. Impact of Stress and Financials on Romanian Infertile Women Accessing Assisted Reproductive Treatment. Int. J. Environ. Res. Public Health 2022, 19, 3256. [Google Scholar] [CrossRef]
- Tirnea, L.; Bratosin, F.; Vidican, I.; Cerbu, B.; Turaiche, M.; Timircan, M.; Margan, M.-M.; Marincu, I. The Efficacy of Convalescent Plasma Use in Critically Ill COVID-19 Patients. Medicina 2021, 57, 257. [Google Scholar] [CrossRef]
- Dehelean, L.; Papava, I.; Musat, M.I.; Bondrescu, M.; Bratosin, F.; Bucatos, B.O.; Bortun, A.-M.C.; Mager, D.V.; Romosan, R.S.; Romosan, A.-M.; et al. Coping Strategies and Stress Related Disorders in Patients with COVID-19. Brain Sci. 2021, 11, 1287. [Google Scholar] [CrossRef]
- Timircan, M.; Bratosin, F.; Vidican, I.; Suciu, O.; Turaiche, M.; Bota, A.V.; Mitrescu, S.; Marincu, I. Coping Strategies and Health-Related Quality of Life in Pregnant Women with SARS-CoV-2 Infection. Medicina 2021, 57, 1113. [Google Scholar] [CrossRef]
- Marincu, I.; Bratosin, F.; Vidican, I.; Bostanaru, A.-C.; Frent, S.; Cerbu, B.; Turaiche, M.; Tirnea, L.; Timircan, M. Predictive Value of Comorbid Conditions for COVID-19 Mortality. J. Clin. Med. 2021, 10, 2652. [Google Scholar] [CrossRef] [PubMed]
- Timircan, M.; Bratosin, F.; Vidican, I.; Suciu, O.; Tirnea, L.; Avram, V.; Marincu, I. Exploring Pregnancy Outcomes Associated with SARS-CoV-2 Infection. Medicina 2021, 57, 796. [Google Scholar] [CrossRef] [PubMed]
- Cerbu, B.; Pantea, S.; Bratosin, F.; Vidican, I.; Turaiche, M.; Frent, S.; Borsi, E.; Marincu, I. Liver Impairment and Hematological Changes in Patients with Chronic Hepatitis C and COVID-19: A Retrospective Study after One Year of Pandemic. Medicina 2021, 57, 597. [Google Scholar] [CrossRef] [PubMed]
- Citu, I.M.; Citu, C.; Gorun, F.; Neamtu, R.; Motoc, A.; Burlea, B.; Rosca, O.; Bratosin, F.; Hosin, S.; Manolescu, D.; et al. Using the NYHA Classification as Forecasting Tool for Hospital Readmission and Mortality in Heart Failure Patients with COVID-19. J. Clin. Med. 2022, 11, 1382. [Google Scholar] [CrossRef]
- Citu, C.; Gorun, F.; Motoc, A.; Ratiu, A.; Gorun, O.M.; Burlea, B.; Neagoe, O.; Citu, I.M.; Rosca, O.; Bratosin, F.; et al. Evaluation and Comparison of the Predictive Value of 4C Mortality Score, NEWS, and CURB-65 in Poor Outcomes in COVID-19 Patients: A Retrospective Study from a Single Center in Romania. Diagnostics 2022, 12, 703. [Google Scholar] [CrossRef]
- Goshen-Lago, T.; Szwarcwort-Cohen, M.; Benguigui, M.; Almog, R.; Turgeman, I.; Zaltzman, N.; Halberthal, M.; Shaked, Y.; Ben-Aharon, I. The Potential Role of Immune Alteration in the Cancer–COVID19 Equation—A Prospective Longitudinal Study. Cancers 2020, 12, 2421. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Margan, M.-M.; Craina, M.; Neamtu, R.; Gorun, O.M.; Burlea, B.; Bratosin, F.; Rosca, O.; Grigoras, M.L.; et al. Calcium, Magnesium, and Zinc Supplementation during Pregnancy: The Additive Value of Micronutrients on Maternal Immune Response after SARS-CoV-2 Infection. Nutrients 2022, 14, 1445. [Google Scholar] [CrossRef]
- Seth, G.; Sethi, S.; Bhattarai, S.; Saini, G.; Singh, C.B.; Aneja, R. SARS-CoV-2 Infection in Cancer Patients: Effects on Disease Outcomes and Patient Prognosis. Cancers 2020, 12, 3266. [Google Scholar] [CrossRef]
- Cerbu, B.; Grigoras, M.L.; Bratosin, F.; Bogdan, I.; Citu, C.; Bota, A.V.; Timircan, M.; Bratu, M.L.; Levai, M.C.; Marincu, I. Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis. J. Clin. Med. 2022, 11, 652. [Google Scholar] [CrossRef]
- Nadarajan, G.D.; Omar, E.; Abella, B.S.; Hoe, P.S.; Shin, S.D.; Ma, M.H.-M.; Ong, M.E.H. A conceptual framework for Emergency department design in a pandemic. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 118. [Google Scholar] [CrossRef]
- Barragán Martín, A.B.; Molero Jurado, M.d.M.; Pérez-Fuentes, M.d.C.; Santillán García, A.; Jiménez-Rodríguez, D.; Fernández Martínez, E.; Herrera-Peco, I.; Martos Martínez, Á.; Franco Valenzuela, R.; Méndez Mateo, I.; et al. Adaptation to Change Questionnaire for Nurses: Validation and New Needs in the Context of COVID-19. Healthcare 2021, 9, 1762. [Google Scholar] [CrossRef] [PubMed]
- Cannedy, S.; Bergman, A.; Medich, M.; Rose, D.E.; Stockdale, S.E. Health System Resiliency and the COVID-19 Pandemic: A Case Study of a New Nationwide Contingency Staffing Program. Healthcare 2022, 10, 244. [Google Scholar] [CrossRef] [PubMed]
- Boilève, A.; Stoclin, A.; Barlesi, F.; Varin, F.; Suria, S.; Rieutord, A.; Blot, F.; Netzer, F.; Scotté, F. COVID-19 management in a cancer center: The ICU storm. Support. Care Cancer 2020, 28, 5037–5044. [Google Scholar] [CrossRef] [PubMed]
- Marincu, I.; Citu, C.; Bratosin, F.; Bogdan, I.; Timircan, M.; Gurban, C.V.; Bota, A.V.; Braescu, L.; Grigoras, M.L. Clinical Characteristics and Outcomes of COVID-19 Hospitalized Patients: A Comparison between Complete mRNA Vaccination Profile and Natural Immunity. J. Pers. Med. 2022, 12, 259. [Google Scholar] [CrossRef]
- Citu, I.M.; Citu, C.; Gorun, F.; Sas, I.; Tomescu, L.; Neamtu, R.; Motoc, A.; Gorun, O.M.; Burlea, B.; Bratosin, F.; et al. Immunogenicity Following Administration of BNT162b2 and Ad26.COV2.S COVID-19 Vaccines in the Pregnant Population during the Third Trimester. Viruses 2022, 14, 307. [Google Scholar] [CrossRef]
- Davies, J.M.; Spencer, A.; Macdonald, S.; Dobson, L.; Haydock, E.; Burton, H.; Angelopoulos, G.; Martin-Hirsch, P.; Wood, N.J.; Thangavelu, A.; et al. Cervical cancer and COVID-an assessment of the initial effect of the pandemic and subsequent projection of impact for women in England: A cohort study. BJOG Int. J. Obstet. Gynaecol. 2022, 129, 1133–1139. [Google Scholar] [CrossRef]
- Perkins, R.B.; Guido, R.S.; Castle, P.E.; Chelmow, D.; Einstein, M.H.; Garcia, F.; Huh, W.K.; Kim, J.J.; Moscicki, A.-B.; Nayar, R.; et al. 2019 ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. 2019 ASCCP Risk-Based Management Consensus Guidelines Committee. J. Low. Genit. Tract Dis. 2020, 24, 102–131. Available online: https://journals.lww.com/jlgtd/Fulltext/2020/04000/2019_ASCCP_Risk_Based_Management_Consensus.3.aspx (accessed on 9 October 2020). [CrossRef] [Green Version]
- Grigoraş, M.L.; Ar-ghirescu, T.S.; Folescu, R.; Talpoş, I.C.; Gîndac, C.M.; Zamfir, C.L.; Cornianu, M.; Anghel, M.D.; Levai, C.M. Expression of E-cadherin in lung carcinoma, other than those with small cells (NSCLC). Rom. J. Morphol. Embryol. 2017, 58, 1317–1325. [Google Scholar]
- Chino, J.; Annunziata, C.M.; Beriwal, S.; Bradfield, L.; Erickson, B.A.; Fields, E.C.; Fitch, K.; Harkenrider, M.M.; Holschneider, C.H.; Kamrava, M.; et al. Radiation Therapy for Cervical Cancer: Executive Summary of an ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2020, 10, 220–234. [Google Scholar] [CrossRef]
- Bhatla, N.; Berek, J.; Cuello, M.; Denny, L.A.; Grenman, S.; Karunaratne, K. New revised FIGO staging of cervical cancer. Abstract S020.2. In Proceedings of the FIGO XXII World Congress of Gynecology and Obstetrics, Rio de Janeiro, Brazil, 14–19 October 2018. [Google Scholar]
- Hong, K.H.; Lee, S.W.; Kim, T.S.; Huh, H.J.; Lee, J.; Kim, S.Y.; Park, J.-S.; Kim, G.J.; Sung, H.; Roh, K.H.; et al. Guidelines for Laboratory Diagnosis of Coronavirus Disease 2019 (COVID-19) in Korea. Ann. Lab. Med. 2020, 40, 351–360. [Google Scholar] [CrossRef]
- Bogdan, I.; Citu, C.; Bratosin, F.; Malita, D.; Romosan, I.; Gurban, C.V.; Bota, A.V.; Turaiche, M.; Bratu, M.L.; Pilut, C.N.; et al. The Impact of Multiplex PCR in Diagnosing and Managing Bacterial Infections in COVID-19 Patients Self-Medicated with Antibiotics. Antibiotics 2022, 11, 437. [Google Scholar] [CrossRef] [PubMed]
- Popescu, A.; Craina, M.; Pantea, S.; Pirvu, C.; Chiriac, V.D.; Marincu, I.; Bratosin, F.; Bogdan, I.; Hosin, S.; Citu, C.; et al. COVID-19 Pandemic Effects on Cervical Cancer Diagnosis and Management: A Population-Based Study in Romania. Diagnostics 2022, 12, 907. [Google Scholar] [CrossRef] [PubMed]
- Faye, M.D.; Alfieri, J. Advances in Radiation Oncology for the Treatment of Cervical Cancer. Curr. Oncol. 2022, 29, 928–944. [Google Scholar] [CrossRef] [PubMed]
- Lazzari, C.; Karachaliou, N.; Bulotta, A.; Viganó, M.; Mirabile, A.; Brioschi, E.; Santarpia, M.; Gianni, L.; Rosell, R.; Gregorc, V. Combination of immunotherapy with chemotherapy and radiotherapy in lung cancer: Is this the beginning of the end for cancer? Ther. Adv. Med. Oncol. 2018, 10, 1758835918762094. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-F.; Fan, Y.; Zhang, P.; Ruan, J.-Y.; Mu, Y.; Li, J.-K. Cervical Cancer Recurrence and Patient Survival after Radical Hysterectomy Followed by Either Adjuvant Chemotherapy or Adjuvant Radiotherapy with Optional Concurrent Chemotherapy: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 823064. [Google Scholar] [CrossRef]
- Biplab, M.; Tapas, M.; Debarshi, L.; Sanjoy, R.; Prabir, C.; Dilip, R.K. Intensity modulated radiotherapy in carcinoma cervix with metastatic para-aortic nodes: An institutional experience from a Regional Cancer Centre of Eastern India. Rep. Pract. Oncol. Radiother. 2021, 26, 400–407. [Google Scholar] [CrossRef]
- Furtunescu, F.; Bohiltea, R.E.; Neacsu, A.; Grigoriu, C.; Pop, C.S.; Bacalbasa, N.; Ducu, I.; Iordache, A.-M.; Costea, R.V. Cervical Cancer Mortality in Romania: Trends, Regional and Rural–Urban Inequalities, and Policy Implications. Medicina 2022, 58, 18. [Google Scholar] [CrossRef]
- Acampora, A.; Grossi, A.; Barbara, A.; Colamesta, V.; Causio, F.A.; Calabrò, G.E.; Boccia, S.; de Waure, C. Increasing HPV Vaccination Uptake among Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 7997. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Before COVID-19 (n = 104) | During COVID-19 (n = 104) | p-Value * | |
|---|---|---|---|
| Background | |||
| Age, years (mean ± SD) | 54.1 ± 16.1 | 54.0 ± 16.6 | 0.965 ** |
| BMI, kg/m2 (mean ± SD) | 25.8 ± 3.6 | 26.4 ± 3.3 | 0.211 ** |
| Smoking history | 36 (34.6%) | 31 (29.8%) | 0.458 |
| Menopausal status | 0.331 | ||
| Menopausal | 55 (52.9%) | 48 (46.2%) | |
| Premenopausal | 49 (47.1%) | 56 (53.8%) | |
| Number of parities | 0.915 | ||
| None | 33 (31.7%) | 35 (33.7%) | |
| 1–2 | 58 (55.8%) | 55 (52.9%) | |
| >2 | 13 (12.5%) | 14 (13.5%) | |
| Place of origin | 0.564 | ||
| Rural | 40 (38.5%) | 36 (34.6%) | |
| Urban | 64 (61.5%) | 68 (65.4%) | |
| Occupation | 0.177 | ||
| Employed | 64 (61.5%) | 55 (52.9%) | |
| Unemployment | 17 (16.3%) | 28 (26.9%) | |
| Retired | 23 (22.1%) | 21 (20.2%) | |
| Level of income | 0.748 | ||
| Low | 22 (21.2%) | 26 (25.0%) | |
| Medium | 58 (55.8%) | 53 (51.0%) | |
| High | 24 (23.1%) | 25 (24.0%) | |
| Civil status | 0.862 | ||
| Married | 87 (83.7%) | 84 (80.8%) | |
| Single | 6 (5.8%) | 7 (6.7%) | |
| Divorced/Widowed | 11 (10.6%) | 13 (12.5%) | |
| SARS-CoV-2 infection | - | 18 (17.3%) | - |
| Before COVID-19 (n = 104) | During COVID-19 (n = 104) | p-Value * | |
|---|---|---|---|
| Comorbidities | |||
| Hypertension | 39 (37.5%) | 41 (39.4%) | 0.775 |
| Diabetes mellitus | 17 (16.3%) | 19 (18.3%) | 0.713 |
| Ischemic heart disease | 9 (8.7%) | 11 (10.6%) | 0.638 |
| Others | 28 (26.9%) | 33 (31.7%) | 0.446 |
| Cancer histology | 0.724 | ||
| Squamous cell carcinoma | 85 (81.7%) | 83 (79.8%) | |
| Adenocarcinoma | 19 (18.3%) | 21 (20.2%) | |
| Tumor size | 0.037 | ||
| <3 cm | 59 (56.7%) | 44 (42.3%) | |
| ≥3 cm | 45 (43.3%) | 123 (57.7%) | |
| Invasion of vagina | 0.046 | ||
| Not invaded | 23 (22.1%) | 15 (14.4%) | |
| Upper third | 41 (39.4%) | 30 (28.8%) | |
| Middle Third | 27 (26.0%) | 34 (32.7%) | |
| Lower third | 13 (12.5%) | 25 (24.0%) | |
| Parameters | 0.204 | ||
| Not invaded | 82 (78.8%) | 89 (85.6%) | |
| Invaded | 22 (21.2%) | 15 (14.4%) | |
| Differentiation grade | 0.853 | ||
| Grade 1 | 57 (54.8%) | 53 (51.0%) | |
| Grade 2 | 30 (28.8%) | 33 (31.7%) | |
| Grade 3 | 17 (16.3%) | 18 (17.3%) | |
| FIGO stage | 0.032 | ||
| IB2 | 11 (10.6%) | 6 (5.8%) | |
| IIA1-IIB | 48 (46.2%) | 36 (34.6%) | |
| IIIA-IIIC2 | 40 (38.5%) | 47 (45.2%) | |
| IVA-IVB | 5 (4.8%) | 15 (14.4%) | |
| Radical hysterectomy | 24 (23.1%) | 29 (27.9%) | 0.426 |
| Relapse | 17 (16.3%) | 29 (27.9%) | 0.044 |
| Local | 8 (47.1%) | 9 (31.0%) | 0.337 |
| Regional | 5 (29.4%) | 7 (24.1%) | |
| Distant | 4 (23.5%) | 13 (44.8%) | |
| Palliation | 50 (48.1%) | 66 (63.5%) | 0.025 |
| Reason for palliation | 0.034 | ||
| Adjacent organ infiltration | 48 (46.2%) | 41 (39.4%) | |
| Distant metastasis | 40 (38.5%) | 56 (53.8%) | |
| Poor performance status | 16 (15.4%) | 7 (6.7%) | |
| Hospitalization required | 26 (25.0%) | 33 (31.7%) | 0.281 |
| Days of hospitalization | 5.1 ± 3.8 | 6.0 ± 4.1 | 0.102 ** |
| Before COVID-19 (n = 104) | During COVID-19 (n = 104) | p-Value * | |
|---|---|---|---|
| Radiation therapy type | 0.601 | ||
| External Beam Radiotherapy | 82 (78.8%) | 85 (81.7%) | |
| Brachytherapy | 22 (21.2%) | 19 (18.3%) | |
| Moderate/Severe acute toxicity | |||
| Upper GI | 25 (24.0%) | 22 (21.2%) | 0.618 |
| Lower GI and pelvis | 48 (46.2%) | 51 (49.0%) | 0.677 |
| Genitourinary | 21 (20.2%) | 26 (25.0%) | 0.407 |
| Anemia | 63 (64.4%) | 69 (66.3%) | 0.770 |
| Leucopenia | 60 (57.7%) | 57 (54.8%) | 0.674 |
| Skin toxicity | 52 (50.0%) | 55 (52.9%) | 0.677 |
| Moderate/Severe late toxicity | |||
| Bladder | 9 (8.7%) | 13 (12.5%) | 0.367 |
| Intestines | 28 (26.9%) | 32 (30.8%) | 0.540 |
| Kidney | 4 (3.8%) | 5 (4.8%) | 0.733 |
| Skin | 2 (1.9%) | 0 (0.0%) | 0.155 |
| Response to treatment at 3 months | 0.045 | ||
| Complete response | 82 (78.8%) | 77 (74.0%) | |
| Partial response | 10 (9.6%) | 4 (3.8%) | |
| Disease progression | 12 (11.5%) | 23 (22.1%) | |
| Referral source | 0.025 | ||
| Primary care | 67 (64.4%) | 51 (49.0%) | |
| Secondary care | 37 (35.6%) | 53 (51.0%) | |
| Referred to and received treatment | 0.021 | ||
| Yes | 87 (83.7%) | 73 (70.2%) | |
| No | 17 (16.3%) | 31 (29.8%) | |
| Outcomes | |||
| Change in treatment plan | 14 (13.5%) | 26 (25.0%) | 0.034 |
| Postponed treatment | 10 (9.6%) | 22 (21.2%) | 0.021 |
| Missed appointments | 11 (12.5%) | 24 (23.1%) | 0.015 |
| Risk Factors | HR | CI | p-Value |
|---|---|---|---|
| FIGO stage | 3.39 | 2.06–4.21 | <0.001 |
| Tumor size | 3.12 | 2.24–4.00 | <0.001 |
| Invasion of vagina | 2.58 | 1.82–3.73 | <0.001 |
| Postponed treatment | 2.51 | 1.90–3.46 | 0.001 |
| Missed appointments | 2.24 | 1.18–3.53 | 0.001 |
| Response to treatment at 3 months | 1.66 | 1.09–2.52 | 0.014 |
| Age | 1.35 | 1.01–1.84 | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popescu, A.; Pantea, S.; Radu, D.; Gluhovschi, A.; Dumitru, C.; Dahma, G.; Mocanu, A.G.; Neamtu, R.; Dema, S.; Tigmeanu, C.V.; et al. The Impact of SARS-CoV-2 Pandemic on Patients Undergoing Radiation Therapy for Advanced Cervical Cancer at a Romanian Academic Center: A Four-Year Retrospective Analysis. Diagnostics 2022, 12, 1488. https://doi.org/10.3390/diagnostics12061488
Popescu A, Pantea S, Radu D, Gluhovschi A, Dumitru C, Dahma G, Mocanu AG, Neamtu R, Dema S, Tigmeanu CV, et al. The Impact of SARS-CoV-2 Pandemic on Patients Undergoing Radiation Therapy for Advanced Cervical Cancer at a Romanian Academic Center: A Four-Year Retrospective Analysis. Diagnostics. 2022; 12(6):1488. https://doi.org/10.3390/diagnostics12061488
Chicago/Turabian StylePopescu, Alin, Stelian Pantea, Daniela Radu, Adrian Gluhovschi, Catalin Dumitru, George Dahma, Adelina Geanina Mocanu, Radu Neamtu, Sorin Dema, Codruta Victoria Tigmeanu, and et al. 2022. "The Impact of SARS-CoV-2 Pandemic on Patients Undergoing Radiation Therapy for Advanced Cervical Cancer at a Romanian Academic Center: A Four-Year Retrospective Analysis" Diagnostics 12, no. 6: 1488. https://doi.org/10.3390/diagnostics12061488