


Seat Pressure Asymmetries after Cycling at Constant Intensity

1
Institute of Sport Sciences and Physiotherapy, Faculty of Medicine, University of Tartu, 51008 Tartu, Estonia
2
Institute of Technology, Estonian University of Life Sciences, 51006 Tartu, Estonia
*
Author to whom correspondence should be addressed.
Symmetry 2024, 16(3), 270; https://doi.org/10.3390/sym16030270
Submission received: 2 February 2024
/
Revised: 16 February 2024
/
Accepted: 21 February 2024
/
Published: 24 February 2024
(This article belongs to the Special Issue Symmetry and Asymmetry in Sport Sciences)
Abstract
:The aim of this study was to compare seat pressure asymmetries before and after 30 min cycling at constant intensity in association with pelvic anthropometric parameters and skeletal muscle fatigue. Twelve male road cyclists aged 18–30 years (mean training experience 9.9 ± 2.5 years) participated. Pelvic anthropometric data and body composition were measured with dual-energy X-ray absorptiometry. Participants performed 30 min cycling at 50% peak power output at constant intensity on a cyclus-2 ergometer. Muscle fatigue during cycling was assessed by surface electromyogram spectral mean power frequency (MPF) for the back, gluteal, and thigh muscles. The pressure mapping system was used to assess sitting symmetry before and after the cycling exercise. At the end of cycling, MPF was decreased (p < 0.05) in the dominant side’s erector spinae muscle and the contralateral gluteal muscle. After the exercise, a significant (p < 0.05) asymmetry in seat pressure was observed under the ischial tuberosity based on the peak pressure right to left ratio, whereas peak pressure decreased under the left ischial tuberosity. After the exercise, the relationship (p < 0.05) between pelvis width and pressure under the ischial tuberosity occurred on the dominant side of the body. In conclusion, an asymmetry was revealed after the constant-load cycling exercise by peak pressure ratio right to left side. Further studies should address the role of seat pressure asymmetries before and after cycling exercises at different intensities and durations.
1. Introduction
Cycling is one of the most popular forms of transportation, sport, recreation, and fitness. Regular cycling prevents many chronic diseases (e.g., obesity, cardiovascular diseases, diabetes, hypertension) [1,2,3]. Many individuals use constant cycling instead of intermittent cycling as a warm-up activity. However, they are unaware that constant-load exercise can negatively impact sitting afterwards and could lead to musculoskeletal problems.
Cyclists tend to preferentially use one side of their body during cycling [4]. This lateral preference in cycling may cause bilateral asymmetry, increasing the risk of injuries [4]. Furthermore, cycling overuse injuries can result from excessive mechanical loads on musculoskeletal structures, depending on body position and training load [5,6,7,8]. According to research, cyclists adapt their body positions and muscle activation patterns, as fatigue occurs to maintain performance [9,10,11]. But, the question is whether the pressure asymmetry exists under the ischial tuberosity or the general gluteal area after the cycling exercise at constant intensity. Therefore, it is essential to learn how to prevent non-traumatic cycling-related injuries as well as improve public awareness and health among cyclists.
The most common overuse injuries include back and neck pain, upper extremity nerve compression, saddle sores, and knee, ankle, and foot pain [7,8,12]. Bini and Hunter [6] reported similar prevalence of pain (knee and lower back) among competitive road and recreational cyclists, so the findings in our study would hold also for recreational cyclists who may not have the same adaptation to such exercise as observed in athletes. There are many recommendations to reduce these non-traumatic bicycle riding injuries, such as alteration of bike fitting or technique or just adequate rest [13,14], but there are more effective tools to reduce discomfort in riders’ buttocks when cycling, e.g., estimating the individual ischial tuberosity to determine seat size [15,16]. Researchers have studied the sensitivity of the ischial tuberosities to pressure and it has been found that the buttocks’ sensitivity is dependent on the size of the contact area in which the pressure is exerted [15,16]. It is critical to understand that sitting in the saddle for a long time without breaks is harmful to the human body and muscles, regardless of how ergonomic the bicycle’s saddle or seated position is [17,18,19]. When sitting, the pressure under the ischial bones increases, which limits blood flow in the tissues and causes pain or discomfort [20].
There is a strong correlation between bicycle seat pressure and bicycle seat injuries, such as pain in the ischial tuberosity [19,21]. Seat pressure distribution measurement is one method used to study long-term sitting. There has been research showing that high pressure at the ischial tuberosities is closely related to high spinal load, which can lead to lower back pain [22,23]. Measuring seat pressure distribution is a reliable and objective method to assess subjective discomfort ratings [24].
To date, there have been numerous studies regarding seat pressure during cycling [10,17,18,25,26,27,28], but the effects of before and after constant-load cycling exercise on the relationship between pelvic anthropometric parameters, muscle activity, and seat pressure variables have not been investigated. These changes in seat pressure could predict overuse injuries [5,7,8].
The aim of this study was to compare acute seat pressure changes before and after constant intensity cycling in association with pelvic anthropometric parameters and skeletal muscle fatigue in competitive male road cyclists.
2. Materials and Methods
2.1. Participants
In total, 12 male participants completed data collection and were included in the analysis. Participants were screened for the study using a self-administered questionnaire. After receiving information about this study, all participants signed a consent form. Table 1 summarizes the characteristics of participants. Each participant’s dominant leg was determined based on kicking preference and all cyclists had right leg dominance. This study was approved by the Research Ethics Committee of the University of Tartu (Report nr 217/T-3). All participants were aged between 18 and 30 years, were healthy, and had no musculoskeletal or bone-related injury in the past 6 months according to their health and history questionnaires. Road cyclists also had to be registered racers of the Estonian Cycling Federation in the category men elite or under 23. They had to be currently racing professionally or as an amateur in Europe. In accordance with the participant classification framework, cyclists were classified as level 3—highly trained/nationally experienced [29]. The exclusion criteria included health history conflicts and commitment issues.
2.2. Experimental Design
The experimental design of this study is presented in Figure 1. One to two weeks before testing in the laboratory, all participants performed an incremental cycling test to exhaustion to determine the highest level of oxygen uptake (VO2max) and peak power output (Wpeak). The test was conducted by a sports medicine doctor. Cyclists performed a graded exercise test on an electronically braked cycle ergometer (Corival V3, Lode, Groningen, The Netherlands). The exercise protocol consisted of a 5 min warm-up at 100 W power level and was followed by the incremental cycling exercise. The cadence was set at 90 ± 5 revolution/min (rpm). The initial workload was 100 W with 25 W increments every 2 minutes until exhaustion (when the cyclist could no longer maintain a 70 rpm cadence). Subjects were verbally encouraged to exert themselves maximally. During the cycle ergometer test, gas samples were automatically collected for every 30 s period in breath-by-breath mode for measurement of oxygen consumption using a portable open circuit spirometry system (MetaMax 3B, Cortex, Leipzig, Germany). Computer analysis of all data was conducted using standard software (MetaMax-Analysis 3.21, Cortex, Leipzig, Germany). VO2max was measured and Wpeak was determined. Cycling exercise intensity described as 50% of Wpeak was included in future analyses.
An experiment in the laboratory consisted of three single sessions of measurement. At the beginning, participants were asked to change into cyclists’ pants without underwear and instructed to complete an anthropometric measurement. In single session one, the ConforMat Research pressure mapping system was used to assess sitting distribution. In session two, all participants performed the same predesigned indoor constant cycling exercise with a total duration of 30 min at 50% of Wpeak. Surface electromyogram (sEMG) spectral mean power frequency (MPF) over the erector spinae at L3, gluteus medius, biceps femoris, vastus lateralis, and rectus femoris muscles was recorded. Average and maximum pedal force was measured automatically with various sensors by a cyclus-2 ergometer throughout the workout. In single session three, the participants were asked to sit again on the adjusted table with a pressure mapping device placed over the table for seat distribution measurement.
2.3. Dual Energy X-ray Absorptiometry
One to two weeks before testing in the laboratory, all participants took radiologic measurements using a DXA machine (DXA, Expert-XL, Lunar Corp., Madison, WI, USA), which is the most effective and accurate method for analyzing ischial tuberosities [30]. Objects made of plastic, metal, or other dense materials were removed before the participant was positioned on the DXA table. During the scan, participants lay supine and placed their hands at their sides as instructed by the manufacturer. Ischial tuberosity size and pelvis height and width were determined (Figure 2a, Table 2). Whole body mass (kg) was measured and body fat % was calculated (Table 2). Analyses were performed using the manufacturer’s software (Version 1.91). All scans and analyses were performed by the same experienced physician.
2.4. Seat Pressure Distribution
Before and immediately following the cycling exercise, participants were seated on a table equipped with a pressure mapping device (ConforMat; Tekscan Inc., Boston, MA, USA) that measured 618.5 mm in width, 539.2 mm in length, and 0.762 mm in height (Figure 2b).
This device comprised 1024 pressure-sensitive elements organized in a 32 × 32 matrix, with each element measuring 14.7 mm × 14.7 mm. The pressure mapping device was fixed to the table with adhesive tape. The initial seat position was hips and knees at 90° flexion and thighs in full contact with the pressure map, performed with arms crossed. No backrest support was used in this study. Participants were instructed to sit continuously for a minute. The pressure mapping device was divided into four horizontal regions (right and left femoral, and right and left gluteal parts), which allowed for the description of the pressure distribution of each region (Figure 3).
Participants’ seat pressure distribution data were recorded using a seat pressure mat with a specific-designed program (ConforMat Research, version 7.10c; Tekscan Inc., Norwood, US) and continuously sampled at a frequency of 5 Hz throughout the 1 min period. A linear calibration method was used to calibrate the device according to the manufacturer’s instructions. Auto-adjust sensitivity was selected. The seat pressure distribution was determined through the following variables:
- Distribution of contact area (%) of the right and left femoral, and right and left gluteal parts. The relative contact area was divided into four parts based on the center of pressure (COP) coordinates.
- Peak pressure (N/cm2) under the ischial tuberosity on a 3.2 cm2 area. This was calculated between the maximum four adjacent sensing elements of the seat pressure mapping sensor. The ischial tuberosity ratio was calculated by dividing the peak pressure of the right side with the peak pressure of the left. Asymmetry was determined by an unequal relationship between these parameters.
- Length of COP trajectory (cm) to measure sitting stability.
2.5. EMG Recording and Analysis during Cycling
In single session two, while the cycling exercise at 50% Wpeak at constant intensity was performed, sEMG was recorded bilaterally from the erector spinae at L3, gluteus medius, biceps femoris, vastus lateralis, and rectus femoris muscles using an electromyograph ME6000 (Mega Electronics Ltd., Kuopio, Finland). sEMG activity was recorded with surface electrodes T-601. For proper cleaning, the skin under the electrodes was shaved, abraded, and soaked in alcohol. A conducting gel was applied to obtain good signal transfer from the skin to the electrodes. Electrodes were placed according to SENIAM guidelines [31]. Electrode ten positions were marked with ink to ensure reliable electrode replacement. In order to prevent shifting, wires between the electrodes and the computer were secured to the skin with adhesive tape. Raw EMG signals were amplified, digitized, and acquired by PC software MegaWin (Mega Electronics, Koupio, Finland) at a sampling rate of 1 kHz. EMG signals were band-pass filtered at 5–500 Hz using a 4th order zero-phase-shift Butterworth filter and were divided into 3 s epochs. For each epoch, MPF was calculated based on Fourier transform [32]. MPF of the measured muscles was recorded twice by electromyograph for 30 s periods at the beginning (0–1 min) and the end (29–30 min) of the exercise.
2.6. Statistical Analysis
All data are presented as means and standard deviation (±SD) and percentage differences between “before “and “after” exercise. Statistical significance was assessed using the paired samples t-test for paired groups. The relationships between the sEMG MPF of skeletal muscles, maximum pedal force, ischial tuberosity size, and cyclist anthropometry and seat pressure distribution variables were examined using Pearson correlation coefficients. One-way analysis of variance (ANOVA) followed by Bonferroni post hoc comparisons were used to test for differences between data obtained before and after the cycling exercise. Cohen’s d effect sizes for identifying statistical differences were determined [33]. The strength-of-effect size coefficients were interpreted according to Hopkins [34] with values of 0–0.09, trivial; 0.10–0.29, small; 0.30–0.49, moderate; 0.50–0.69, large; 0.70–0.89, very large; 0.90–0.99, nearly perfect; and 1.00, perfect. Statistical analyses were performed using SPSS statistics software, version 20.0 (SPSS Inc., Chicago, IL, USA). For all the above-mentioned analyses, p-values p < 0.05 were considered statistically significant.
3. Results
Table 2 presents DXA measurements of body composition and anthropometry before the cycling exercise.
The mean variables during the cycling exercise are presented in Table 3.
SEMG MPF was significantly decreased after exercise on the left gluteus medius muscle (p = 0.03) and on the right erector spinae muscle at L3 (p = 0.01) (Table 4). For all other measured muscles, MPF changes were not significant (p > 0.05).
Peak pressure decreased significantly under the left ischial tuberosity (p = 0.01) (Figure 4). Mean pressure indicators of the gluteal area changed significantly after the exercise on the left and right sides (left gluteal area p = 0.02; right gluteal area p = 0.01), but the differences between gluteal area right and left body sides were unsignificant (before exercise p = 0.44; after exercise p = 0.11) according to mean pressure indicators (Figure 5). The observed peak pressure of effect size for the right ischial tuberosity was 0.06 and 0.6 for the left ischial tuberosity. The ischial tuberosity peak pressure ratio of right to left after exercise was significant (p = 0.005; Cohen’s d = 0.96) (Figure 6).
Ischial tuberosity peak pressure variables had high correlation with pelvis width before the exercise on both sides (left r = 0.72; p < 0.01; right r = 0.91; p < 0.001), but after the exercise, only on the dominant right side (r = 0.65; p < 0.05). Maximum pedal force during the cycling exercise was positively correlated with muscle activity on right m. erector spinae L3 (r = 0.64, p < 0.05) and right rectus femoris (r = 0.82, p < 0.001) and negatively with MPF left biceps femoris (r = −0.62, p < 0.05) (Figure 7). Maximum pedal force was positively related to the size of ischial tuberosities (right r = 0.66, p < 0.05; left r = 0.70, p < 0.01) (Figure 7). Cyclists’ heights correlated with pressure under left ischial tuberosities (r = 0.60; p < 0.05) before the exercise and with contralateral pressure under ischial tuberosities (r = 0.60; p < 0.05) after the exercise. Cyclists’ body masses were positively correlated with pressure on left gluteal areas (r = 0.69, p < 0.01) before the cycling exercise and with pressure on left femoral areas (r = 0.79, p < 0.01) after the cycling exercise.
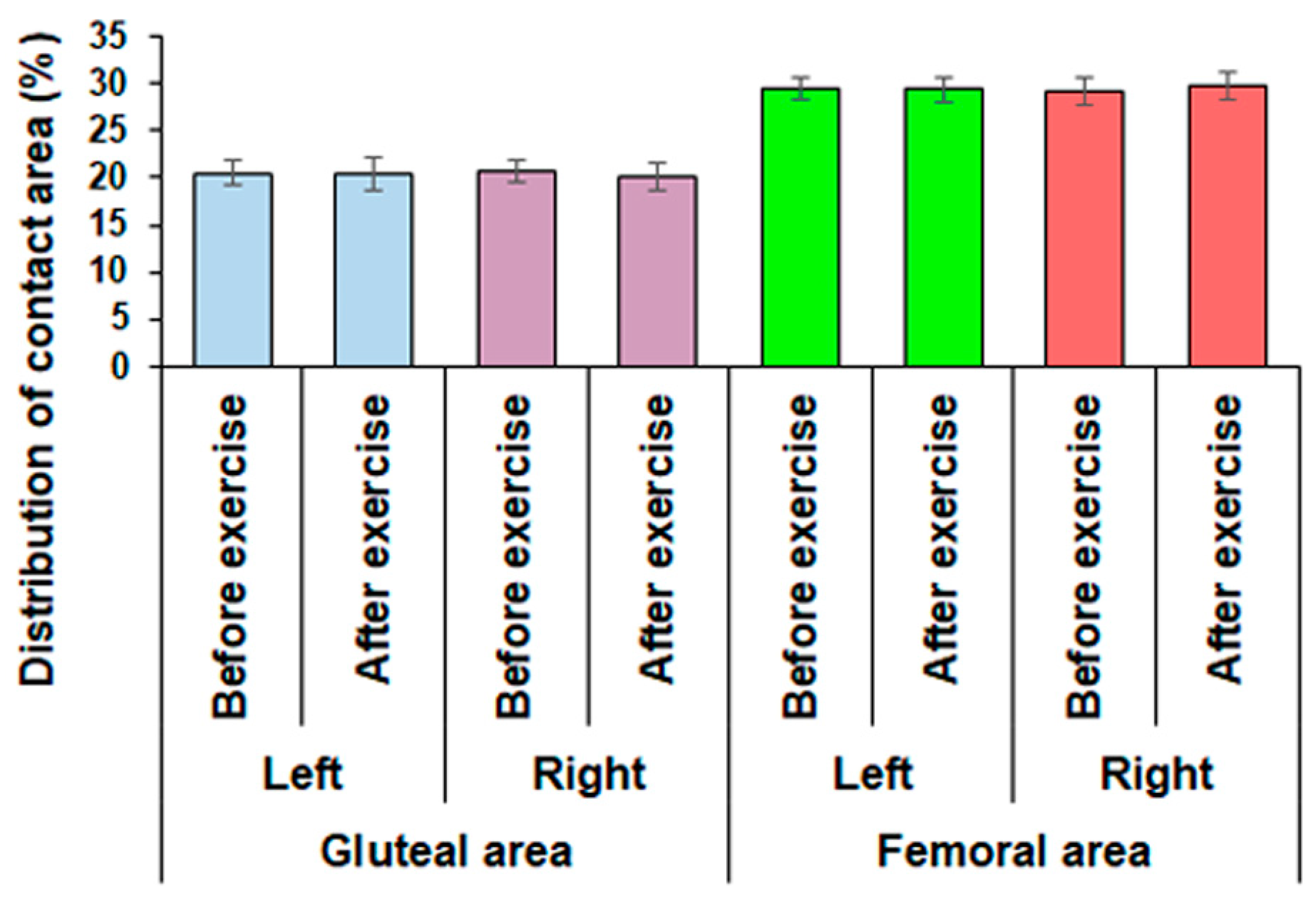
Finally, no relationships between pelvis height, ischial tuberosity size, and pressure values under ischial tuberosity were observed in male road cyclists (p > 0.05). There were no significant differences in the sitting stability evaluated by the length of COP trajectory (p > 0.05) and sitting relative contact area (p > 0.05) (Figure 8) after the 30 min cycling exercise at 50% Wpeak at constant intensity.
4. Discussion
This study described seat pressure changes before and after constant-intensity cycling in association with pelvic anthropometric parameters and skeletal muscle fatigue in competitive male road cyclists. A significant asymmetry in sitting was observed after exercise under the ischial tuberosity, measured by the peak pressure ratio on the right and left sides of the body.
Our first major finding was that significant fatigue of right erector spinae and left gluteus medius muscle occurred after the 30 min constant-intensity cycling exercise, evaluated by the decrease in sEMG power frequency MPF. Several parameters are used in EMG studies to evaluate fatigue, e.g., an increase in EMG signal amplitude or a decrease in mean/median power frequency [14,23,35,36,37]. Also, in this study, the sEMG signal followed this temporal pattern. It has been suggested that decreased muscle fiber conduction velocity and synchronization of motor unit firing may contribute to MPF decreases [38,39]. In a study by Gibson and colleagues [40], it was shown that fatigue occurs as a result of metabolic changes that decrease the force-generating capacity of the skeletal muscles during prolonged bicycling. In the present study, sEMG analysis during cycling showed that MPF of left gluteus medius muscle and right erector spinae muscle at L3 was decreased significantly by 4% and 14%, respectively, at the end of the exercise compared with the beginning of the exercise, whereas the MPF decrease in thigh muscles was unsignificant. The results of this study are consistent with those of previous studies showing that the lower back is the most common site of pain, since fatigue may cause pain [8,10,31]. Conversely, knee pain has also been reported, although we did not observe significant changes in the thigh muscle pattern. In addition, there was a positive association between maximum pedal force and decrease in dominant side back muscle and rectus femoris MPF frequency. Interestingly, a negative correlation was found between maximum pedal force and a decrease in left biceps femoris MPF. These findings may indicate that competitive male road cyclists experience compensatory mechanisms after constant-load cycling exercises towards their dominant side. Because of high adaptation to cycling, cyclists’ muscle patterns have been altered primarily in the back and gluteal muscles rather than the thigh muscles. As a result, if we observe an increase in maximum pedal force during constant-load cycling, the muscle pattern may have changed. As we reduce these changes, there will be fewer musculoskeletal disorders, including those related to sitting.
The present study revealed that, although mean seat pressure of the gluteal area significantly changed after the exercise on both sides of the body, the difference between body sides was unsignificant based on the gluteal area mean pressure right to left ratio before (p = 0.44) and after the exercise (p = 0.11). In contrast, peak pressure under the left ischial tuberosity decreased significantly (p = 0.01) following the 30 min constant-load cycling exercise. The results of the present study are consistent with the study by Bressel et al. [17], which showed that predictors of mean seat pressure are not the same as for peak pressure. The present study indicated that 30 min of cycling at 50% Wpeak resulted in an increase in discomfort according to muscle activity, despite no change of gluteal mean pressure between body sides. In terms of postural shift, we observed significant (p = 0.005) asymmetry according to the ischial tuberosity peak pressure ratio of right to left after exercise (Figure 6). This suggests that a significant decrease in blood flow under the ischial tuberosity may occur. The effects of all of these changes may adversely impact cyclists’ sitting positions after exercise, which could lead to overuse injuries in the long term. It has been shown that reducing asymmetry may prevent cyclists from suffering from injuries [4].
Despite the presence of a strong correlation between pelvis width and pressure under the ischial tuberosity prior to exercise, the study indicated that, after cycling for 30 min at constant intensity, pressure under the dominant side of the ischial tuberosity was more strongly correlated with pelvis width. Furthermore, this had no relationship with the size of the ischial tuberosity or the height of the pelvis. Previous studies have shown that the saddle should be widened to provide better support for the ischium because an increase in the pressure area results in a dispersion of the maximum and mean pressures [15,41]. It has been reported that different saddle widths result in different pressure distributions, and that these distributions depend on the size of the pelvis and the area that is in contact with the saddle during training [15,28]. Lin et al. [41] found that a saddle 1 cm wider than the cyclist’s ischial tuberosity width may improve pressure distribution over the contact area and increase comfort while cycling. There is a proportionality between the width of the pelvis and the width between the ischial tuberosities, which means that both greater parameters may reduce the load on the posterior bone structure [15,27,41]. Our results demonstrated a positive relationship before the cycling exercise between cyclists’ body masses and pressure on left gluteal areas. After the exercise, it was seen only on the left femoral area, as confirmed by a decrease in pressure parameters on the gluteal area. Cyclists with a lower body mass did not display significantly greater pressure than heavier cyclists in our study, as was seen in the study by Bressel [17], who proposed that it was because of less subcutaneous tissue covering the ischiopubic bone. However, our study indicated that taller instead of heavier cyclists had a relationship with the non-dominant side of pressure under the ischial tuberosity before exercise and after the constant-load cycling exercise, as seen on the contralateral side.
This study’s results are similar to Holliday et al.’s study [42], indicating that the mean pressure of the saddle increases with an increase in the pedaling load. However, in this study, we measured seat pressure before and after exercise and found a correlation between maximum pedal force and the size of ischial tuberosities. In some cases, muscle activation and pedal force changes may represent subconscious strategies for maintaining power output [9]. According to our study, it is also important to consider the size of the ischial tuberosity and the width of the pelvis when assessing this relationship.
To the extent of our knowledge, there are no studies that have analyzed seat pressure after a constant-intensity cycling exercise. A novel approach of this study was to measure the size of ischial tuberosities by DXA rather than evaluating the distance between the ischial tuberosity (the pelvis’ points of contact) using a foam block or saddle as has usually been performed in different studies [25,27,28,43]. It is essential to measure the distribution of pressure in the saddle and there are studies where saddle pressure is recorded also in static mode without pedaling [44]; however, it is also important to show that these changes may persist when the cyclist sits after exercise on other surfaces in addition to the saddle, as demonstrated in our study.
This study has several limitations. First of all, the small sample size is due to the difficulty of recruiting highly trained/national-level male road cyclists. Secondly, the participants were healthy competitive male road cyclists, and it is uncertain whether the findings can be generalized to individuals with compromised loading, such as those who have recently experienced musculoskeletal disorders, surgeries, or injuries affecting the seated position. Thirdly, we had only male participants in this study, so future studies could take into consideration female participants. Lastly, it is important to note that this study only assessed acute changes in seat pressure. Therefore, we could not determine whether bilateral postural imbalances, which are known to affect sitting, also modify sitting patterns.
In order to help cyclists and clinicians who are interested in preventing or relieving symptoms related to bicycle seat injuries, the following variables related to bicycle seat pressure may be useful. The importance of understanding that sitting in the saddle for a long period of time without breaks is detrimental to the body and muscles cannot be overstated. Despite how ergonomic the bicycle’s saddle or seated position may be, selecting variable intensities with body movements could prevent these asymmetries, as seen in this study. It is helpful to know that sometimes changes occur under ischial tuberosities even if the cyclist seems balanced overall. In order to determine whether asymmetry differences could be prevented after constant-load cycling exercise, cyclists should be tested in asymmetrical cycling pants, which have a higher pad under the dominant ischial tuberosity and a lower pad under the ischial tuberosity of the non-dominant body side. By doing so, many musculoskeletal problems arising from asymmetrical sitting can be prevented.
5. Conclusions
The seat pressure asymmetry occurred after the constant-load cycling exercise by peak pressure ratio right to left side. Also, skeletal muscle fatigue in male road cyclists was observed more in the back and gluteus muscles than the thigh muscles, according to the significant decrease in MPF of the EMG power spectrum of the erector spinae and gluteus medius muscles during the constant-load cycling exercise.
A strong relationship between pelvis width and pressure under the ischial tuberosity occurred bilaterally before exercise, but this relationship was only seen on the dominant side after exercise.
To further support our findings, additional studies comparing seat pressure after cycling exercises at different intensities and durations in cyclists with a variety of qualifications are warranted.
Author Contributions
L.L.: conceptualization, study design/methodology, data collection, formal data analysis, writing—original draft preparation, writing—reviewing and editing, resources, project administration. J.E. and M.R.: study design/methodology, data collection, formal data analysis, software. M.P.: conceptualization, study design/methodology, data collection, writing—reviewing and editing, supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank the cyclists for their volunteer involvement in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Oja, P.; Titze, S.; Bauman, A.; de Geus, B.; Krenn, P.; Reger-Nash, B.; Kohlberger, T. Health benefits of cycling: A systematic review. Scand. J. Med. Sci. Sports 2011, 21, 496–509. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.; Charlesworth, S.; Ivey, A.; Nettlefold, L.; Bredin, S.S. A systematic review of the evidence for Canada’s physical activity guidelines for adults. Int. J. Behav. Nutr. Phys. Act. 2010, 11, 7–39. [Google Scholar] [CrossRef] [PubMed]
- Chavarrias, M.; Carlos-Vivas, J.; Collado-Mateo, D.; Pérez-Gómez, J. Health benefits of indoor cycling: A systematic review. Medicina 2019, 55, 452. [Google Scholar] [CrossRef] [PubMed]
- Carpes, F.P.; Mota, C.B.; Faria, I.E. On the bilateral asymmetry during running and cycling—A review considering leg preference. Phys. Ther. Sport 2010, 11, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Krosshaug, T.; Bahr, R. Overuse injuries in professional road cyclists. Am. J. Sports Med. 2010, 38, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- Bini, R.R.; Hunter, J.R. Pain and body position on the bicycle in competitive and recreational road cyclists: A retrospective study. Sports Biomech. 2023, 22, 522–535. [Google Scholar] [CrossRef] [PubMed]
- Visentini, P.J.; McDowell, A.H.; Pizzari, T. Factors associated with overuse injury in cyclists: A systematic review. J. Sci. Med. Sport 2022, 25, 391–398. [Google Scholar] [CrossRef] [PubMed]
- De Bernardo, N.; Barrios, C.; Vera, P.; Laíz, C.; Hadala, M. Incidence and risk for traumatic and overuse injuries in top-level road cyclists. J. Sports Sci. 2012, 30, 1047–1053. [Google Scholar] [CrossRef]
- Dingwell, J.B.; Joubert, J.E.; Diefenthaeler, F.; Trinity, J.D. Changes in muscle activity and kinematics of highly trained cyclists during fatigue. IEEE Trans. Biomed. Eng. 2008, 55, 2666–2674. [Google Scholar] [CrossRef]
- Verma, R.; Hansen, E.A.; de Zee, M.; Madeleine, P. Effect of seat positions on discomfort, muscle activation, pressure distribution and pedal force during cycling. J. Electromyogr. Kinesiol. 2016, 27, 78–86. [Google Scholar] [CrossRef]
- MacIntosh, B.R.; Neptune, R.R.; Horton, J.F. Cadence, power, and muscle activation in cycle ergometry. Med. Sci. Sports Exerc. 2000, 32, 1281–1287. [Google Scholar] [CrossRef]
- Rooney, D.; Sarriegui, I.; Heron, N. “As easy as riding a bike”: A systematic review of injuries and illness in road cycling. BMJ Open Sport Exerc. Med. 2020, 9, 6. [Google Scholar] [CrossRef]
- Yum, H.; Kim, H.; Lee, T.; Park, M.S.; Lee, S.Y. Cycling kinematics in healthy adults for musculoskeletal rehabilitation guidance. BMC Musculoskelet. Disord. 2021, 22, 1044. [Google Scholar] [CrossRef]
- Holliday, W.; Swart, J. A dynamic approach to cycling biomechanics. Phys. Med. Rehabil. Clin. N. Am. 2022, 33, 1–13. [Google Scholar] [CrossRef]
- Chen, Y.L. Predicting external ischial tuberosity width for both sexes to determine their bicycle-seat sizes. Int. J. Ind. Ergon. 2018, 64, 118–121. [Google Scholar] [CrossRef]
- Goossens, R.H.M.; Teeuw, R.; Snijders, C.J. Sensitivity for pressure difference on the ischial tuberosity. Ergonomics 2005, 48, 895–902. [Google Scholar] [CrossRef]
- Bressel, E.; Larson, B.J. Bicycle seat designs and their effect on pelvic angle, trunk angle, and comfort. Med. Sci. Sports Exerc. 2003, 35, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Bressel, E.; Reeve, T.; Parker, D.; Cronin, J. Influence of bicycle seat pressure on compression of the perineum: A mri analysis. J. Biomech. 2007, 40, 198–202. [Google Scholar] [CrossRef]
- Bressel, E.; Nash, D.; Dolny, D. Association between attributes of a cyclist and bicycle seat pressure. J. Sex. Med. 2010, 7, 3424–3433. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Varacallo, M. Ischial bursitis. In StatPearls; StatPearls Publishing: St. Petersburg, FL, USA, 2023. [Google Scholar]
- Dettori, N.J.; Norvell, D.C. Non-traumatic bicycle injuries a review of the literature. Sports Med. 2006, 36, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Makhsous, M.; Lin, F.; Bankard, J.; Hendrix, R.W.; Hepler, M.; Press, J. Biomechanical effects of sitting with adjustable ischial and lumbar support on occupational low back pain: Evaluation of sitting load and back muscle activity. BMC Musculoskelet. Disord. 2009, 10, 17. [Google Scholar] [CrossRef]
- Srinivasan, J.; Balasubramanian, V. Low back pain evaluation for cyclist using sEMG: A comparative study between bicyclist and aerobic cyclist. IFMBE Proc. 2009, 23, 1140–1143. [Google Scholar] [CrossRef]
- De Looze, M.P.; Kuijt-Evers, L.F.M.; Van Dieën, J. Sitting comfort and discomfort and the relationships with objective measures. Ergonomics 2003, 46, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Carpes, F.P.; Dagnese, F.; Kleinpaul, J.F.; Martins, E.d.A.; Mota, C.B. Effects of workload on seat pressure while cycling with two different saddles. J. Sex. Med. 2009, 6, 2728–2735. [Google Scholar] [CrossRef] [PubMed]
- McDonald, R.; Holliday, W.; Swart, J. Muscle recruitment patterns and saddle pressure indexes with alterations in effective seat tube angle. Sports Med. Health Sci. 2022, 4, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Vicari, D.S.S.; Patti, A.; Giustino, V.; Figlioli, F.; Alamia, G.; Palma, A.; Bianco, A. Saddle pressures factors in road and off-road cyclists of both genders: A narrative review. J. Funct. Morphol. Kinesiol. 2023, 8, 71. [Google Scholar] [CrossRef]
- Potter, J.J.; Sauer, J.L.; Weisshaar, C.L.; Thelen, D.G.; Ploeg, H.L. Gender differences in bicycle saddle pressure distribution during seated cycling. Med. Sci. Sports Exerc. 2008, 40, 1126–1134. [Google Scholar] [CrossRef]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining training and performance caliber: A participant classification framework. Int. J. Sports Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef]
- Gemery, J.M.; Nangia, A.K.; Mamourian, A.C.; Reid, S.K. Digital three-dimensional modelling of the male pelvis and bicycle seats: Impact of rider position and seat design on potential penile hypoxia and erectile dysfunction. BJU Int. 2007, 99, 135–140. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for semg sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Y.; Ma, A.; Ma, G.; Ye, Y.; Li, R.; Lu, T. A comparative study of EMG indices in muscle fatigue evaluation based on grey relational analysis during all-out cycling exercise. Biomed. Res. Int. 2018, 2018, 9341215. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Lindström, L.; Kadefors, R.; Petersen, I. An electromyographic index for localized muscle fatigue. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1977, 43, 750–754. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, V.; Jagannath, M.; Adalarasu, K. Muscle fatigue based evaluation of bicycle design. Appl. Ergon. 2014, 45, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Masuda, K.; Masuda, T.; Sadoyama, T.; Inaki, M.; Katsuta, S. Changes in surface emg parameters during static and dynamic fatiguing contractions. J. Electromyogr. Kinesiol. 1999, 9, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Bigland-Ritchie, B.; Furbush, F.; Woods, J.J. Fatigue of intermittent submaximal voluntary contractions: Central and peripheral factors. J. Appl. Physiol. 1986, 61, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Arendt-Nielsen, L.; Mills, K.R. Muscle fibre conduction velocity, mean power frequency, mean emg voltage and force during submaximal fatiguing contractions of human quadriceps. Eur. J. Appl. Physiol. Occup. Physiol. 1988, 58, 20–25. [Google Scholar] [CrossRef]
- St Clair Gibson, A.; Schabort, E.J.; Noakes, T.D. Reduced neuromuscular activity and force generation during prolonged cycling. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2001, 281, 187–196. [Google Scholar] [CrossRef]
- Lin, Z.-J.; Wang, H.-H.; Chen, C.-H. Effect of bicycle saddle widths on saddle pressure in female cyclists. J. Sports Sci. Med. 2023, 22, 425–430. [Google Scholar] [CrossRef]
- Holliday, W.; Fisher, J.; Swart, J. The effects of relative cycling intensity on saddle pressure indexes. J. Sci. Med. Sport 2019, 22, 1097–1101. [Google Scholar] [CrossRef]
- Albero, J.R.; Pérez-Soriano, P.; Encarnación-Martínez, A. The effect of saddle setback and cycling intensity on saddle pressures and comfort in male and female recreational cyclists. J. Sports Sci. 2023, 41, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Sanford, T.; Gadzinski, A.J.; Gaither, T.; Osterberg, E.C.; Murphy, G.P.; Carroll, P.R.; Breyer, B.N. Effect of oscillation on perineal pressure in cyclists: Implications for micro-trauma. J. Sex. Med. 2018, 6, 239–247. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Experimental design of this study. VO2max—highest level of oxygen uptake; Wpeak—peak power output; DEXA—dual energy X-ray absorptiometry; sEMG—surface electromyography.
Figure 1.
Experimental design of this study. VO2max—highest level of oxygen uptake; Wpeak—peak power output; DEXA—dual energy X-ray absorptiometry; sEMG—surface electromyography.
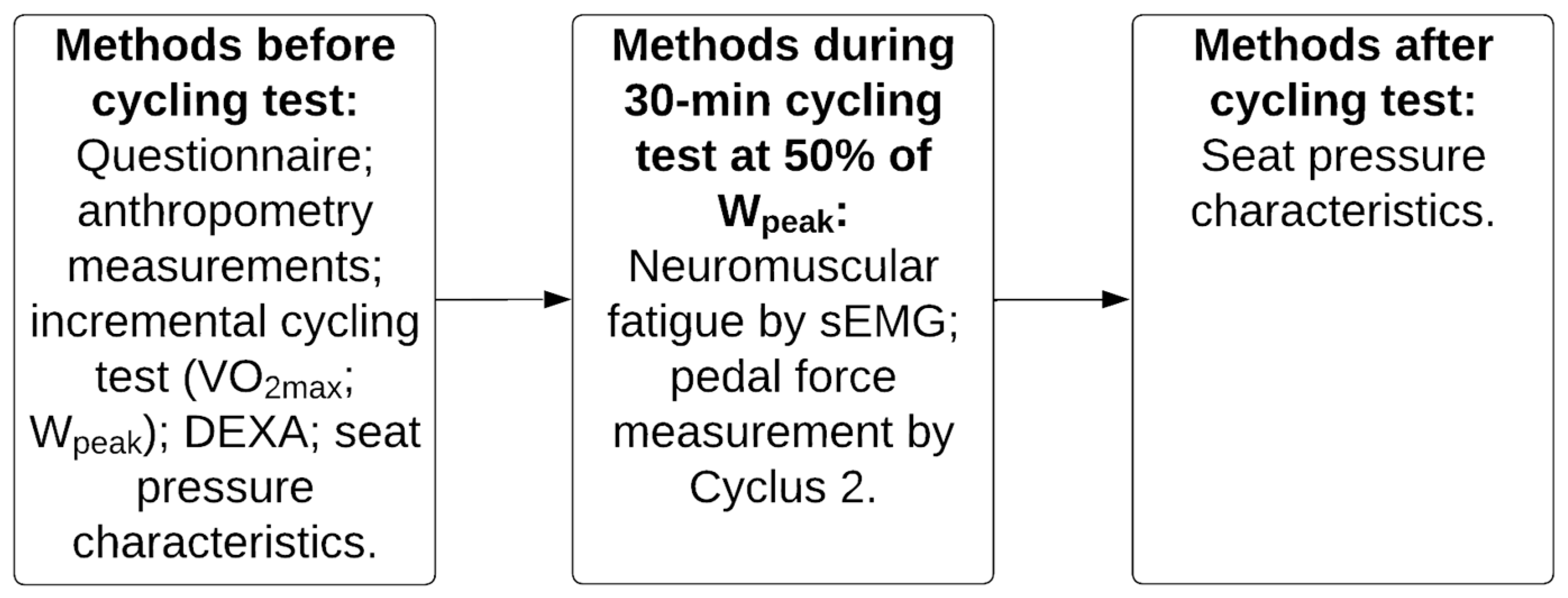
Figure 2.
An example assessment of pelvis height and width and ischial tuberosity size of male road cyclists using a DXA machine (a) and cyclist position on the table during assessment of sitting distribution with a pressure mapping device (b).
Figure 2.
An example assessment of pelvis height and width and ischial tuberosity size of male road cyclists using a DXA machine (a) and cyclist position on the table during assessment of sitting distribution with a pressure mapping device (b).

Figure 3.
Pressure mapping illustrates distribution of contact area of four horizontal regions (right and left femoral (F), and right and left gluteal (G) parts) after exercise in one participant. (a) Distribution of contact area in %; (b) distribution of contact area in N/cm2. Red indicates peak pressure area; orange, yellow, green, blue and black indicate decreasing pressure areas.
Figure 3.
Pressure mapping illustrates distribution of contact area of four horizontal regions (right and left femoral (F), and right and left gluteal (G) parts) after exercise in one participant. (a) Distribution of contact area in %; (b) distribution of contact area in N/cm2. Red indicates peak pressure area; orange, yellow, green, blue and black indicate decreasing pressure areas.
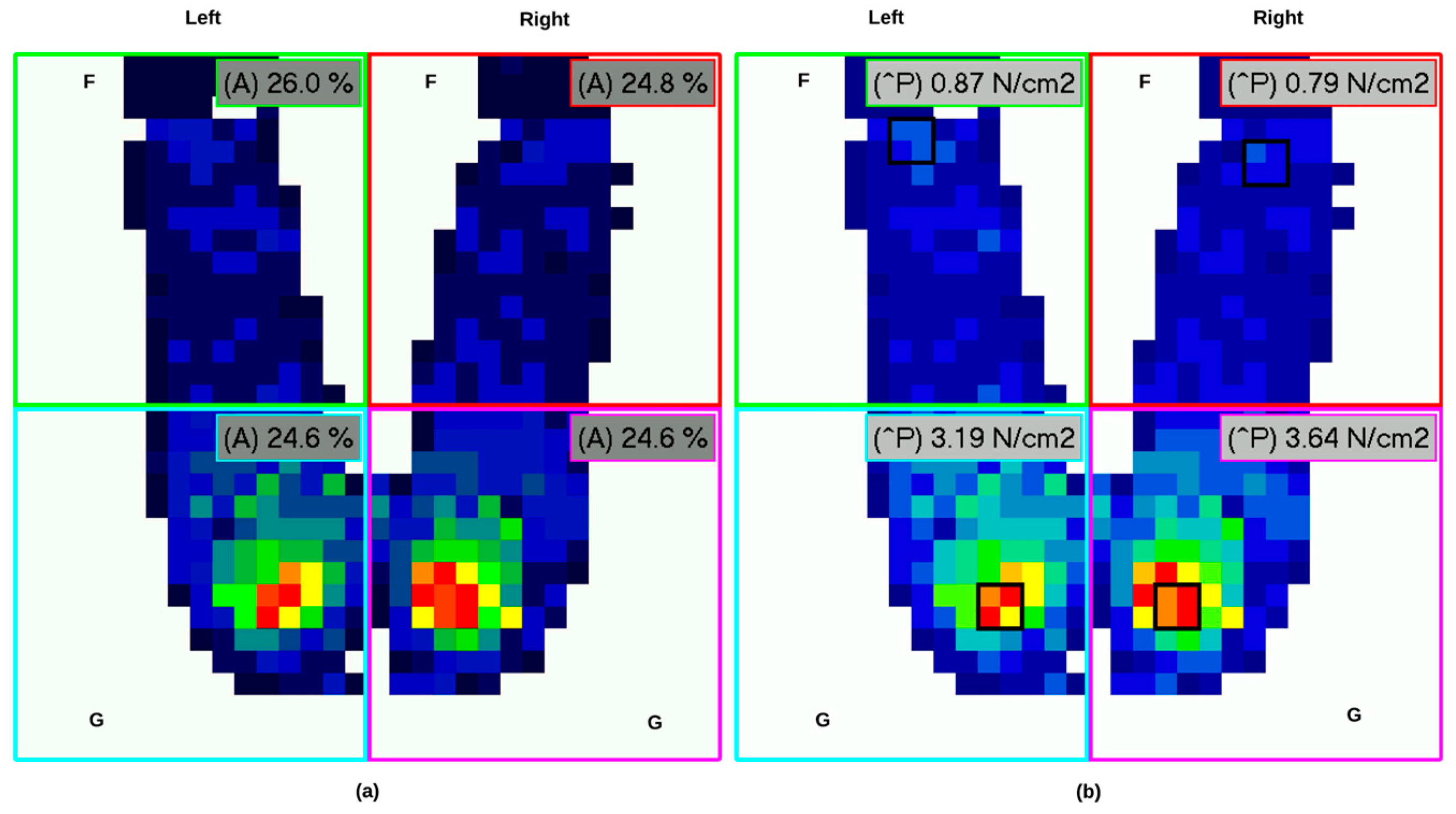
Figure 4.
Mean (±SD) peak pressure under right ischial tuberosity and left ischial tuberosity before and after 30 min constant-load cycling exercise in male road cyclists (n = 12). * p < 0.05.
Figure 4.
Mean (±SD) peak pressure under right ischial tuberosity and left ischial tuberosity before and after 30 min constant-load cycling exercise in male road cyclists (n = 12). * p < 0.05.
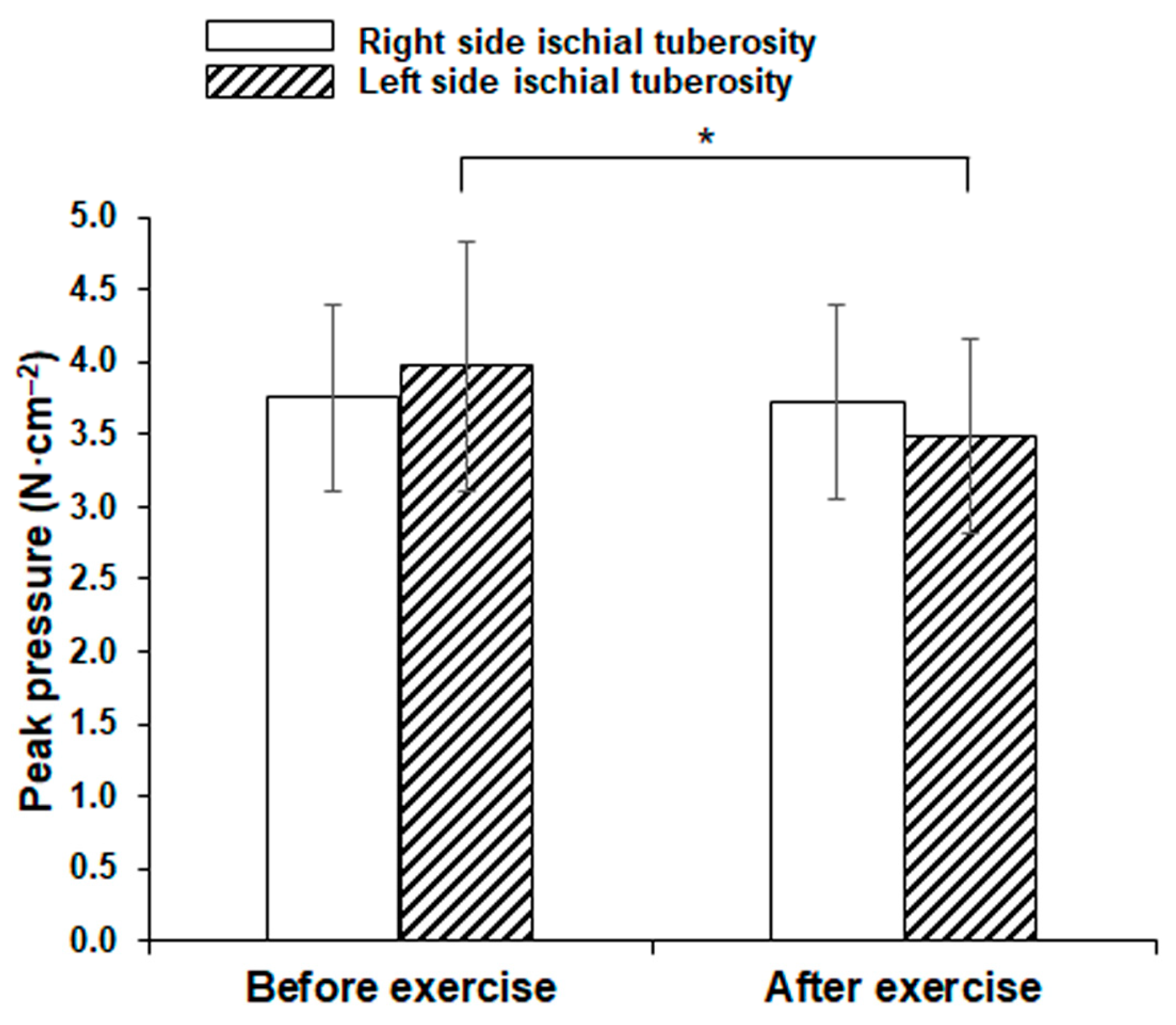
Figure 5.
Mean (±SD) gluteal mean pressure before and after 30 min constant-load cycling exercise in male road cyclists (n = 12). * p < 0.05; ** p < 0.01.
Figure 5.
Mean (±SD) gluteal mean pressure before and after 30 min constant-load cycling exercise in male road cyclists (n = 12). * p < 0.05; ** p < 0.01.
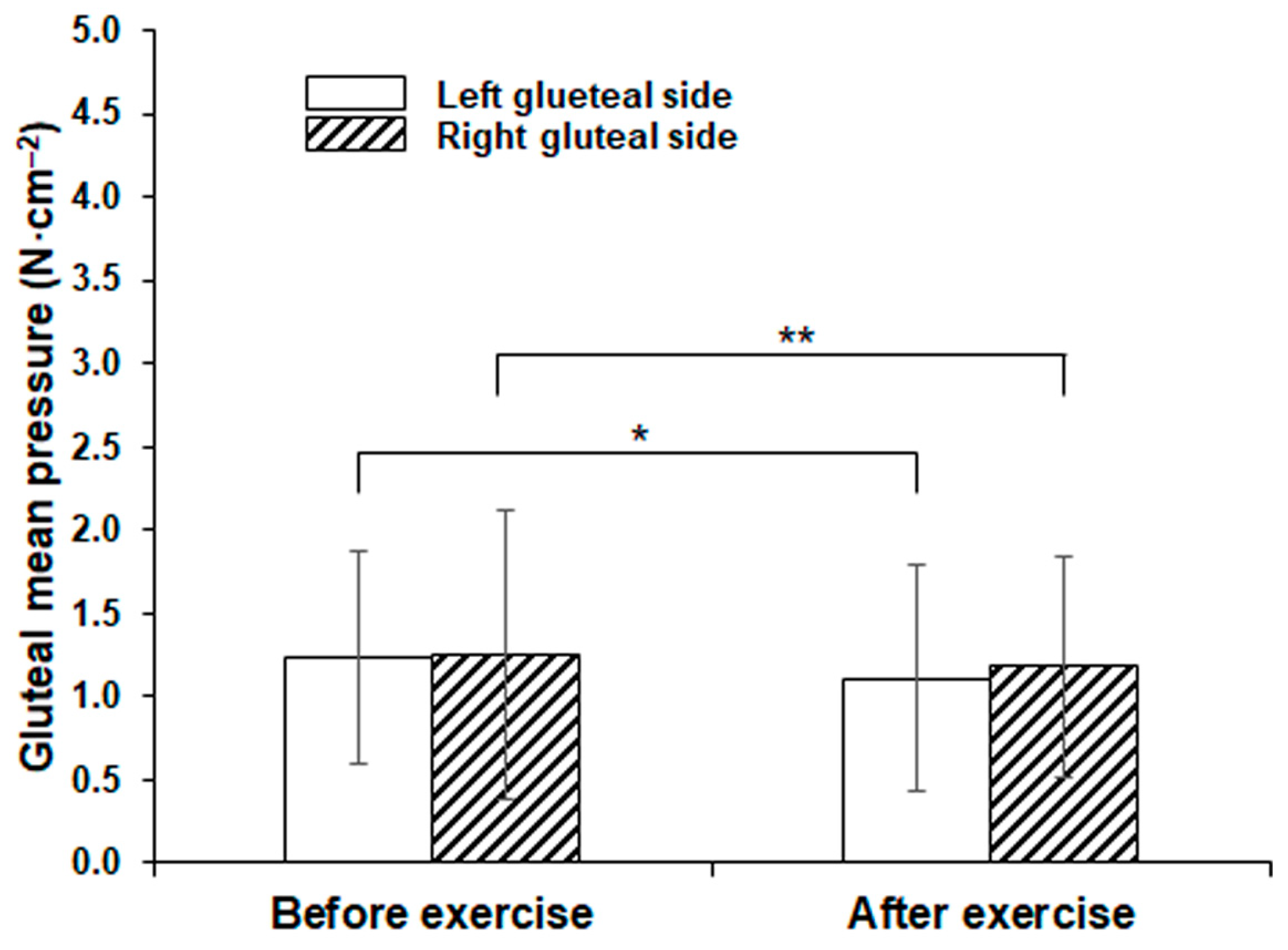
Figure 6.
Mean (±SD) peak pressure ratio right to left before and after 30 min constant-load cycling exercise in male road cyclists (n = 12). *** p < 0.001.
Figure 6.
Mean (±SD) peak pressure ratio right to left before and after 30 min constant-load cycling exercise in male road cyclists (n = 12). *** p < 0.001.
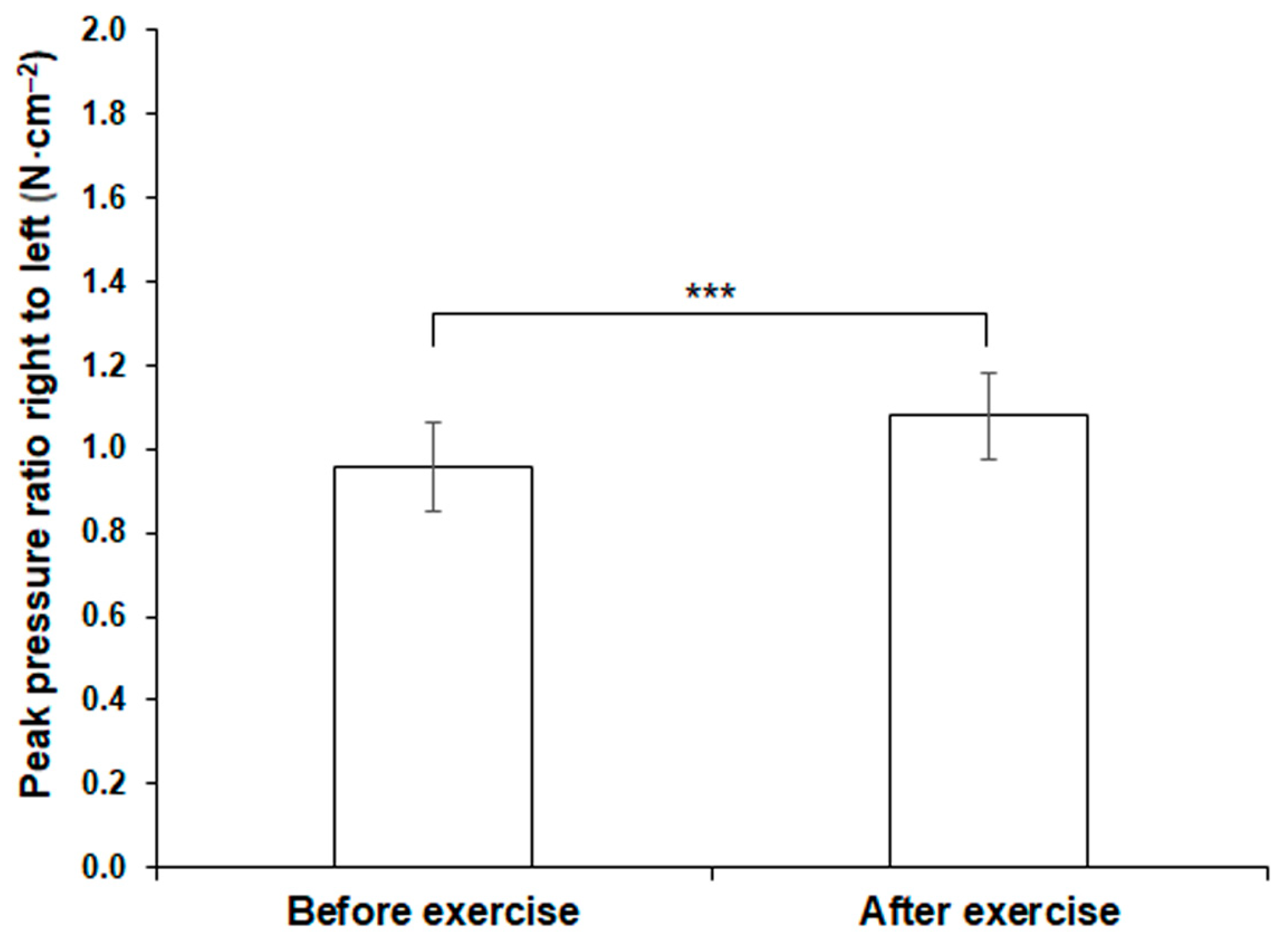
Figure 7.
Correlations with maximum pedal force during the cycling exercise; ischial tuberosity size and skeletal muscle fatigue. * p < 0.05; ** p < 0.01; *** p < 0.001.
Figure 7.
Correlations with maximum pedal force during the cycling exercise; ischial tuberosity size and skeletal muscle fatigue. * p < 0.05; ** p < 0.01; *** p < 0.001.
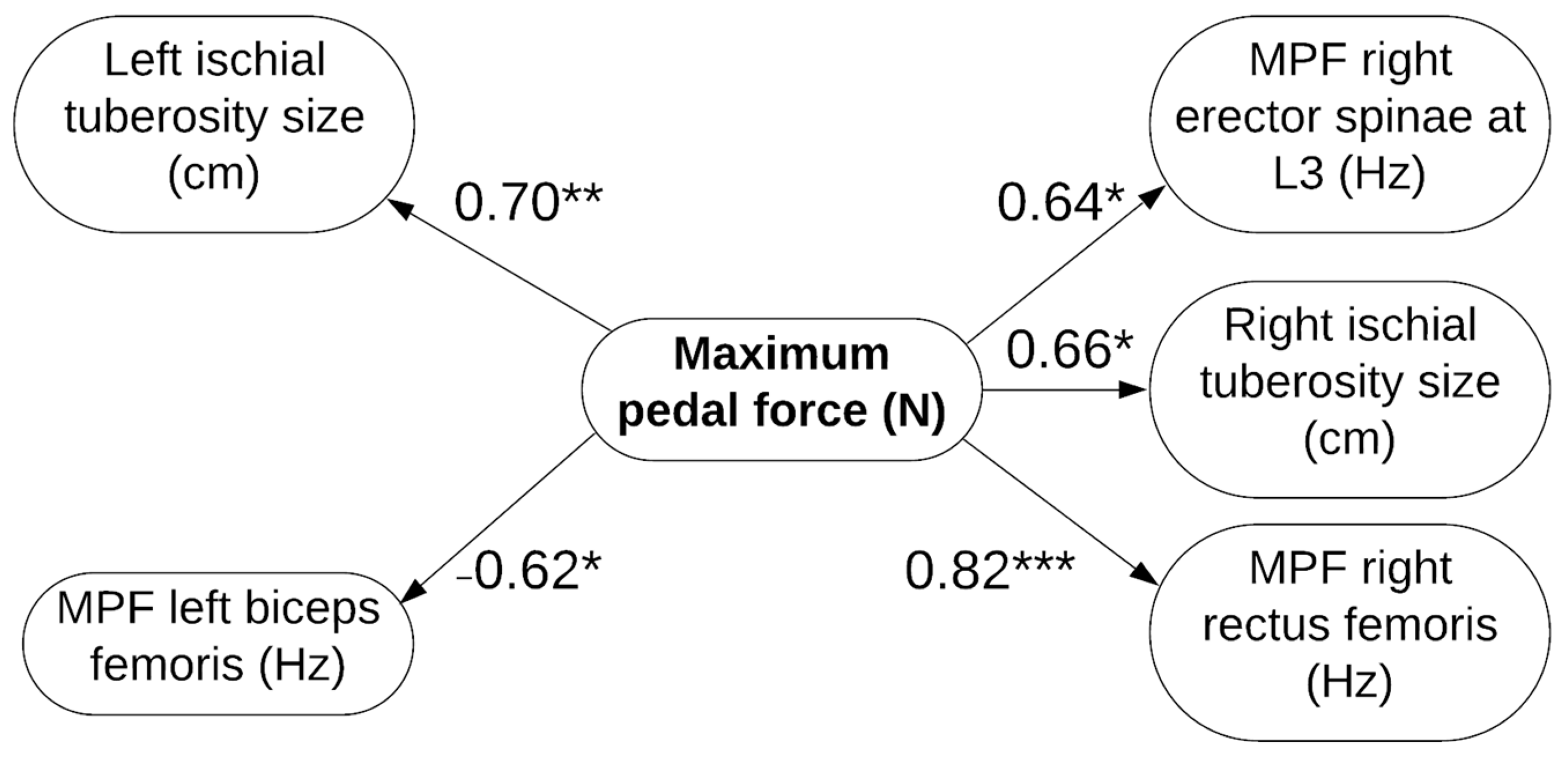
Figure 8.
Mean (±SD) distribution of contact area of the left and right gluteal area, and left and right femoral area. There were no significant differences in distribution of contact area before and after the exercise.
Figure 8.
Mean (±SD) distribution of contact area of the left and right gluteal area, and left and right femoral area. There were no significant differences in distribution of contact area before and after the exercise.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Mean (±SD) descriptive characteristics of male road cyclists (n = 12).
| Main Outcomes | Mean | SD |
|---|---|---|
| Age (years) | 23.2 | 3.5 |
| Body mass (kg) | 74.5 | 6.2 |
| Height (cm) | 185.1 | 5.5 |
| Body mass index (kg/m2) | 21.8 | 1.8 |
| Training history (years) | 9.9 | 2.5 |
Table 2.
Mean (±SD) anthropometry and body composition values in male road cyclists (n = 12).
| Main Outcomes | Mean | SD |
|---|---|---|
| Body fat (%) | 13.6 | 1.8 |
| Pelvis height (cm) | 24.3 | 1.5 |
| Pelvis width (cm) | 26.4 | 2.7 |
| Right ischial tuberosity size (cm) | 4.1 | 0.3 |
| Left ischial tuberosity size (cm) | 4.2 | 0.4 |
Table 3.
Mean (±SD) variables during 30 min constant-load cycling exercise in male road cyclists (n = 12).
Table 3.
Mean (±SD) variables during 30 min constant-load cycling exercise in male road cyclists (n = 12).
| Main Outcomes | Mean | SD |
|---|---|---|
| 50% Wpeak (W) 1 | 208 | 22.7 |
| Cadence per min | 85.3 | 5.0 |
| Heart rate per min | 140.1 | 6.8 |
| Pedal force (N) | 133.4 | 15.4 |
| Maximal pedal force (N) | 361.5 | 174.7 |
1 Wpeak—peak power output.
Table 4.
Mean (±SD) and % change in surface electromyogram (sEMG) spectral mean power frequency (MPF, Hz) in male road cyclists (n = 12) during 30 min constant-load cycling exercise (first minute and last minute). * p < 0.05.
Table 4.
Mean (±SD) and % change in surface electromyogram (sEMG) spectral mean power frequency (MPF, Hz) in male road cyclists (n = 12) during 30 min constant-load cycling exercise (first minute and last minute). * p < 0.05.
| MPF (Hz) | |||||
|---|---|---|---|---|---|
| Variable | First min | Last min | % Change | p-Value | Effect Size (Cohen’s d) |
| Right erector spinae L3 | 58.5 ± 14.0 | 50.1 ± 15.1 | −14.3 | 0.01 * | 0.55 |
| Left erector spinae L3 | 55.4 ± 16.3 | 56.8 ± 20.8 | 2.6 | 0.84 | 0.07 |
| Right m. gluteus medius | 76.5 ± 14.2 | 77.3 ± 14.8 | 1.1 | 0.72 | 0.05 |
| Left m. gluteus medius | 85.7 ± 24.2 | 82.7 ± 23.2 | −3.5 | 0.03 * | 0.12 |
| Right m. biceps femoris | 61.5 ± 14.9 | 66.1 ± 20.0 | 7.4 | 0.47 | 0.25 |
| Left m. biceps femoris | 74.4 ± 22.8 | 69.0 ± 21.4 | −7.2 | 0.43 | 0.23 |
| Right m. vastus lateralis | 98.3 ± 14.6 | 98.8 ± 17.6 | 0.6 | 0.84 | 0.03 |
| Left m. vastus lateralis | 96.8 ± 20.4 | 96.2 ± 26.7 | −0.7 | 0.87 | 0.02 |
| Right m. rectus femoris | 79.3 ± 9.9 | 81.2 ± 10.3 | 2.4 | 0.35 | 0.18 |
| Left m. rectus femoris | 84.4 ± 17.6 | 79.1 ± 19.2 | −6.3 | 0.37 | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lepasalu, L.; Ereline, J.; Reinvee, M.; Pääsuke, M. Seat Pressure Asymmetries after Cycling at Constant Intensity. Symmetry 2024, 16, 270. https://doi.org/10.3390/sym16030270
AMA Style
Lepasalu L, Ereline J, Reinvee M, Pääsuke M. Seat Pressure Asymmetries after Cycling at Constant Intensity. Symmetry. 2024; 16(3):270. https://doi.org/10.3390/sym16030270
Chicago/Turabian StyleLepasalu, Laura, Jaan Ereline, Märt Reinvee, and Mati Pääsuke. 2024. "Seat Pressure Asymmetries after Cycling at Constant Intensity" Symmetry 16, no. 3: 270. https://doi.org/10.3390/sym16030270
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.