Efficacy of Nutritional Interventions on Inflammatory Markers in Haemodialysis Patients: A Systematic Review and Limited Meta-Analysis

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
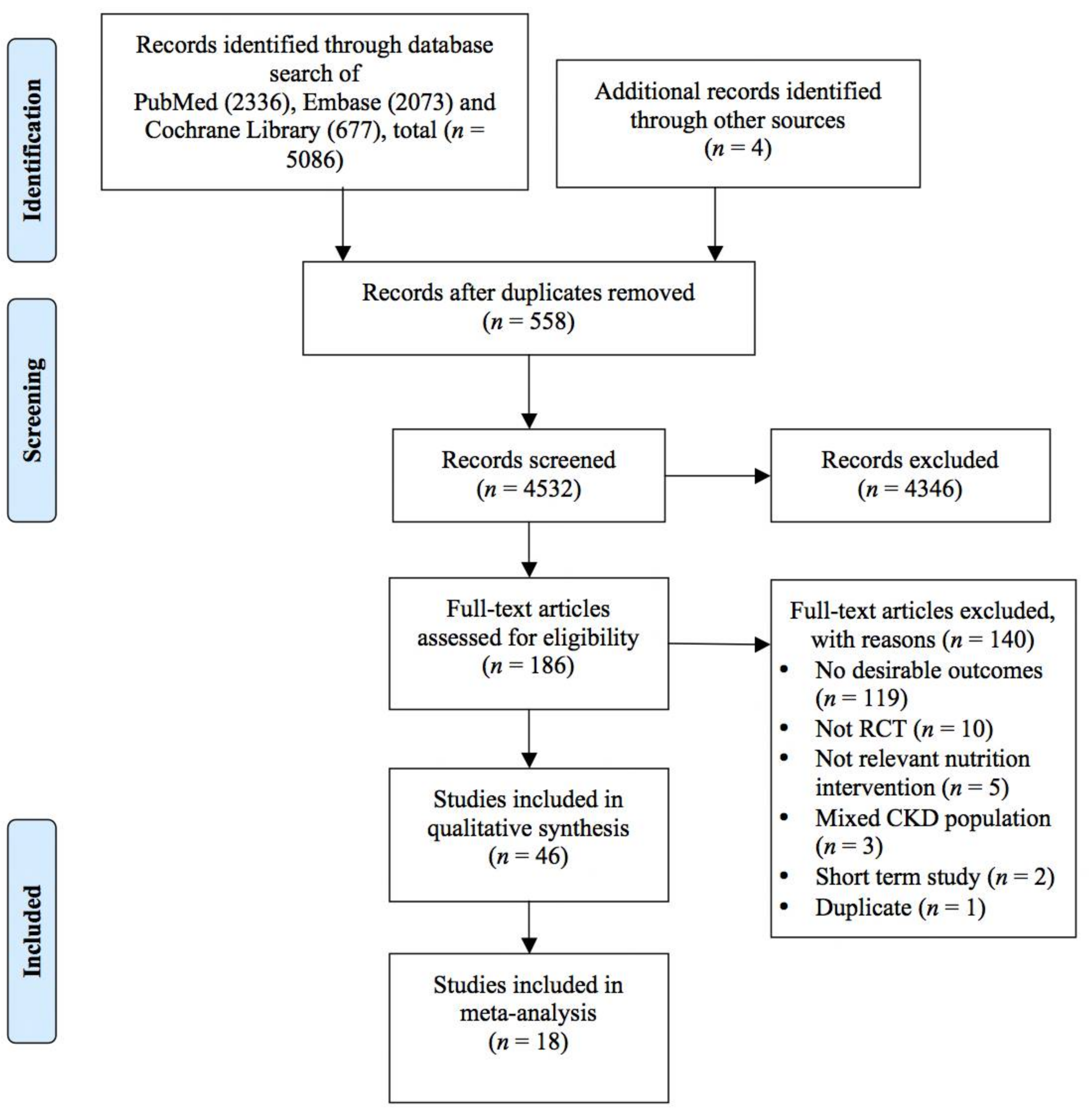
2.1. Data Sources, Searches, and Selection
2.2. Quality Assessment
2.3. Statistical Analysis
3. Results
3.1. Polyphenols
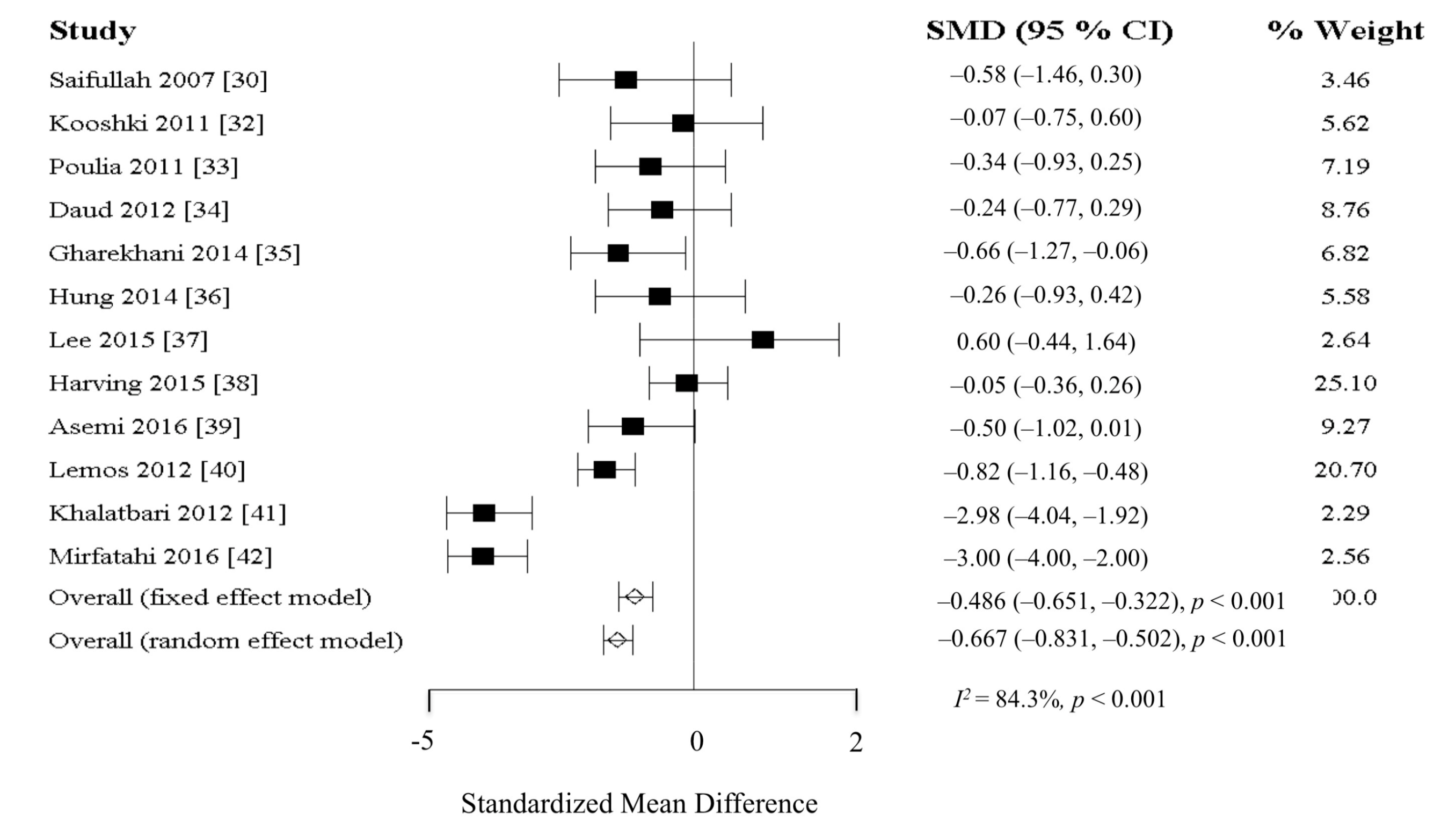
3.2. Omega-3 Fatty Acids
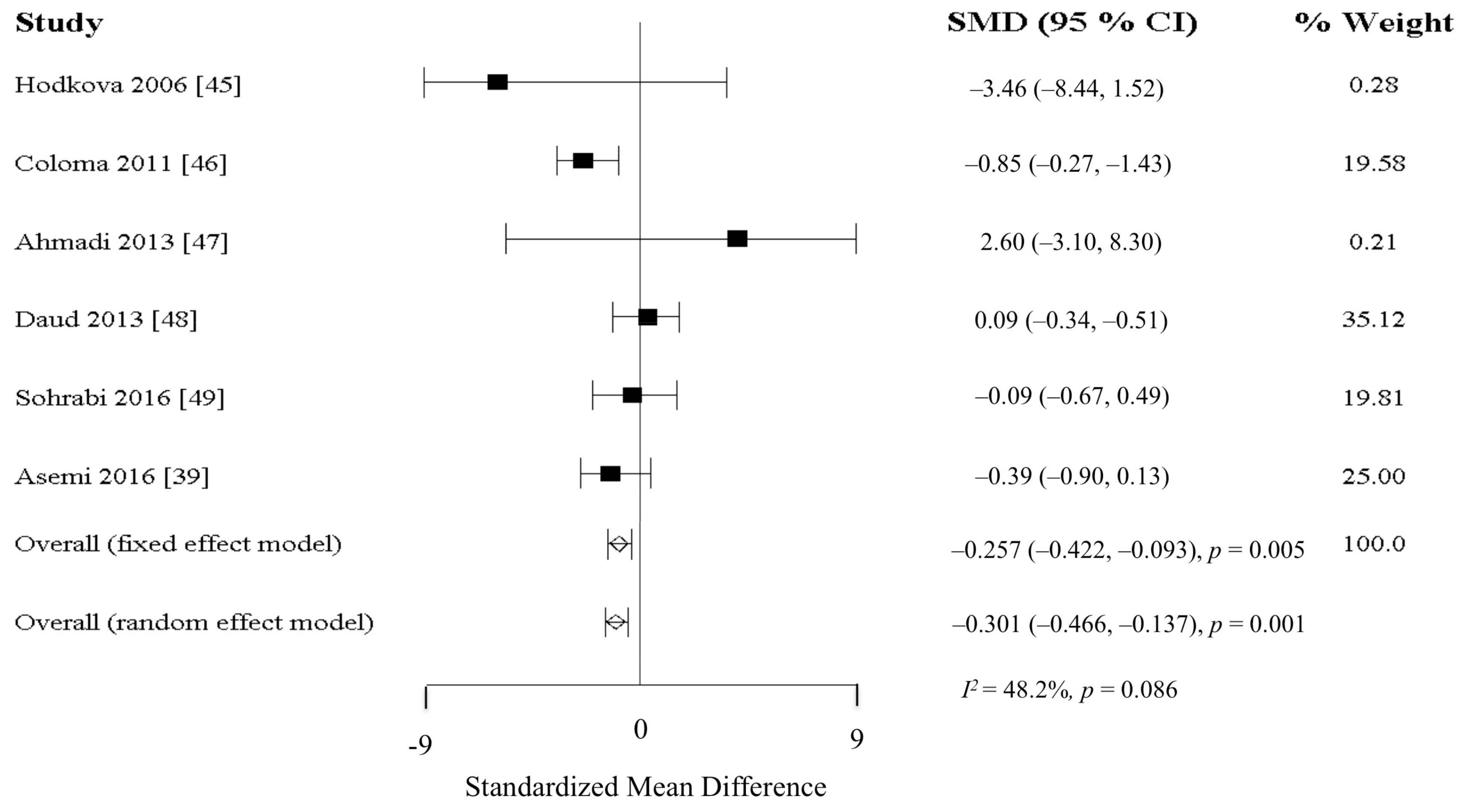
3.3. Antioxidants
3.4. Vitamin D
3.5. Fibres and Probiotics
3.6. Combinations
4. Discussion
4.1. Polyphenols
4.2. Omega-3 Fatty Acids
4.3. Antioxidants
4.4. Vitamin D
4.5. Fibers and Probiotics
4.6. Limitations
5. Conclusions
Supplementary Materials
Acknowledgment
Author Contributions
Conflicts of Interest
References
- United States Renal Data System. 2017 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health: Bethesda, MD, USA; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2017. [Google Scholar]
- Kilpatrick, R.D.; McAllister, C.J.; Kovesdy, C.P.; Derose, S.F.; Kopple, J.D.; Kalantar-Zadeh, K. Association between serum lipids and survival in hemodialysis patients and impact of race. J. Am. Soc. Nephrol. 2007, 18, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D. The phenomenon of altered risk factor patterns or reverse epidemiology in persons with advanced chronic kidney failure. Am. J. Clin. Nutr. 2005, 81, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Alvestrand, A. Inflammation in end-stage renal disease: Sources, consequences, and therapy. Semin. Dial. 2002, 15, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Medzhitov, R. Origin and physiological roles of inflammation. Nature 2008, 454, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Bazeley, J.; Bieber, B.; Li, Y.; Morgenstern, H.; de Sequera, P.; Combe, C.; Yamamoto, H.; Gallagher, M.; Port, F.K.; Robinson, B.M. C-reactive protein and prediction of 1-year mortality in prevalent hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2011, 6, 2452–2461. [Google Scholar] [CrossRef] [PubMed]
- Panichi, V.; Maggiore, U.; Taccola, D.; Migliori, M.; Rizza, G.M.; Consani, C.; Bertini, A.; Sposini, S.; Perez-Garcia, R.; Rindi, P.; et al. Interleukin-6 is a stronger predictor of total and cardiovascular mortality than C-reactive protein in haemodialysis patients. Nephrol. Dial. Transplant. 2004, 19, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, A.; Regolisti, G.; Karupaiah, T.; Sahathevan, S.; Sadu Singh, B.K.; Khor, B.H.; Salhab, N.; Karavetian, M.; Cupisti, A.; Fiaccadori, E. Protein-energy wasting and nutritional supplementation in patients with end-stage renal disease on hemodialysis. Clin. Nutr. 2017, 36, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Carrero, J.J.; Stenvinkel, P. Inflammation in end-stage renal disease—What have we learned in 10 years? Semin. Dial. 2010, 23, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Oberg, B.P.; McMenamin, E.; Lucas, F.L.; McMonagle, E.; Morrow, J.; Ikizler, T.A.; Himmelfarb, J. Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int. 2004, 65, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Caglar, K.; Peng, Y.; Pupim, L.B.; Flakoll, P.J.; Levenhagen, D.; Hakim, R.M.; Ikizler, T.A. Inflammatory signals associated with hemodialysis. Kidney Int. 2002, 62, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, M.; Hung, A.; Kovalchuk, O.; Bitzer, M.; Mokrzycki, M.H. The initial vascular access type contributes to inflammation in incident hemodialysis patients. Int. J. Nephrol. 2012, 2012, 917465. [Google Scholar] [CrossRef] [PubMed]
- Susantitaphong, P.; Riella, C.; Jaber, B.L. Effect of ultrapure dialysate on markers of inflammation, oxidative stress, nutrition and anemia parameters: A meta-analysis. Nephrol. Dial. Transplant. 2013, 28, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Libetta, C.; Sepe, V.; Esposito, P.; Galli, F.; Dal Canton, A. Oxidative stress and inflammation: Implications in uremia and hemodialysis. Clin. Biochem. 2011, 44, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.K. Does the interdependence between oxidative stress and inflammation explain the antioxidant paradox? Oxid. Med. Cell. Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef] [PubMed]
- Sanz, A.B.; Sanchez-Nino, M.D.; Ramos, A.M.; Moreno, J.A.; Santamaria, B.; Ruiz-Ortega, M.; Egido, J.; Ortiz, A. Nf-kappab in renal inflammation. J. Am. Soc. Nephrol. 2010, 21, 1254–1262. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.L.; Kalantar-Zadeh, K.; Vaziri, N.D. The gut as a source of inflammation in chronic kidney disease. Nephron 2015, 130, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, A.; Regolisti, G.; Brusasco, I.; Cabassi, A.; Morabito, S.; Fiaccadori, E. Alterations of intestinal barrier and microbiota in chronic kidney disease. Nephrol. Dial. Transplant. 2015, 30, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Machowska, A.; Carrero, J.J.; Lindholm, B.; Stenvinkel, P. Therapeutics targeting persistent inflammation in chronic kidney disease. Transl. Res. 2016, 167, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P. Inflammation in end-stage renal disease: The hidden enemy. Nephrology 2006, 11, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Fanti, P.; Asmis, R.; Stephenson, T.J.; Sawaya, B.P.; Franke, A.A. Positive effect of dietary soy in ESRD patients with systemic inflammation—Correlation between blood levels of the soy isoflavones and the acute-phase reactants. Nephrol. Dial. Transplant. 2006, 21, 2239–2246. [Google Scholar] [CrossRef] [PubMed]
- Siefker, K.; DiSilvestro, R.A. Safety and antioxidant effects of a modest soy protein intervention in hemodialysis patients. J. Med. Food 2006, 9, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Tomayko, E.J.; Kistler, B.M.; Fitschen, P.J.; Wilund, K.R. Intradialytic protein supplementation reduces inflammation and improves physical function in maintenance hemodialysis patients. J. Ren. Nutr. 2015, 25, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Shema-Didi, L.; Sela, S.; Ore, L.; Shapiro, G.; Geron, R.; Moshe, G.; Kristal, B. One year of pomegranate juice intake decreases oxidative stress, inflammation, and incidence of infections in hemodialysis patients: A randomized placebo-controlled trial. Free Radic. Biol. Med. 2012, 53, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.T.; Fitschen, P.J.; Kistler, B.M.; Jeong, J.H.; Chung, H.R.; Aviram, M.; Phillips, S.A.; Fernhall, B.; Wilund, K.R. Effects of pomegranate extract supplementation on cardiovascular risk factors and physical function in hemodialysis patients. J. Med. Food 2015, 18, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Rassaf, T.; Rammos, C.; Hendgen-Cotta, U.B.; Heiss, C.; Kleophas, W.; Dellanna, F.; Floege, J.; Hetzel, G.R.; Kelm, M. Vasculoprotective effects of dietary cocoa flavanols in patients on hemodialysis: A double-blind, randomized, placebo-controlled trial. Clin. J. Am. Soc. Nephrol. 2016, 11, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Janiques, A.G.; de Oliveira Leal, O.; Stockler-Pinto, M.B.; Moreira, N.X.; Mafra, D. Effects of grape powder supplementation on inflammatory and antioxidant markers in hemodialysis patients: A randomized double-blind study. J. Bras. Nefrol. 2014, 36, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Pakfetrat, M.; Basiri, F.; Malekmakan, L.; Roozbeh, J. Effects of turmeric on uremic pruritus in end stage renal disease patients: A double-blind randomized clinical trial. J. Nephrol. 2014, 27, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Saifullah, A.; Watkins, B.A.; Saha, C.; Li, Y.; Moe, S.M.; Friedman, A.N. Oral fish oil supplementation raises blood omega-3 levels and lowers C-reactive protein in haemodialysis patients—A pilot study. Nephrol. Dial. Transplant. 2007, 22, 3561–3567. [Google Scholar] [CrossRef] [PubMed]
- Bowden, R.G.; Wilson, R.L.; Deike, E.; Gentile, M. Fish oil supplementation lowers C-reactive protein levels independent of triglyceride reduction in patients with end-stage renal disease. Nutr. Clin. Pract. 2009, 24, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Kooshki, A.; Taleban, F.A.; Tabibi, H.; Hedayati, M. Effects of omega-3 fatty acids on serum lipids, lipoprotein (a), and hematologic factors in hemodialysis patients. Ren. Fail. 2011, 33, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Poulia, K.A.; Panagiotakos, D.B.; Tourlede, E.; Rezou, A.; Stamatiadis, D.; Boletis, J.; Zampelas, A. Omega-3 fatty acids supplementation does not affect serum lipids in chronic hemodialysis patients. J. Ren. Nutr. 2011, 21, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Daud, Z.A.; Tubie, B.; Adams, J.; Quainton, T.; Osia, R.; Tubie, S.; Kaur, D.; Khosla, P.; Sheyman, M. Effects of protein and omega-3 supplementation, provided during regular dialysis sessions, on nutritional and inflammatory indices in hemodialysis patients. Vasc. Health Risk Manag. 2012, 8, 187–195. [Google Scholar] [PubMed]
- Gharekhani, A.; Khatami, M.R.; Dashti-Khavidaki, S.; Razeghi, E.; Noorbala, A.A.; Hashemi-Nazari, S.S.; Mansournia, M.A. The effect of omega-3 fatty acids on depressive symptoms and inflammatory markers in maintenance hemodialysis patients: A randomized, placebo-controlled clinical trial. Eur. J. Clin. Pharmacol. 2014, 70, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Hung, A.M.; Booker, C.; Ellis, C.D.; Siew, E.D.; Graves, A.J.; Shintani, A.; Abumrad, N.N.; Himmelfarb, J.; Ikizler, T.A. Omega-3 fatty acids inhibit the up-regulation of endothelial chemokines in maintenance hemodialysis patients. Nephrol. Dial. Transplant. 2015, 30, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Son, Y.K.; Kim, S.E.; An, W.S. The effects of omega-3 fatty acid on vitamin D activation in hemodialysis patients: A pilot study. Mar. Drugs 2015, 13, 741–755. [Google Scholar] [CrossRef] [PubMed]
- Harving, F.; Svensson, M.; Flyvbjerg, A.; Schmidt, E.B.; Jorgensen, K.A.; Eriksen, H.H.; Christensen, J.H. N-3 polyunsaturated fatty acids and adiponectin in patients with end-stage renal disease. Clin. Nephrol. 2015, 83, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Soleimani, A.; Shakeri, H.; Mazroii, N.; Esmaillzadeh, A. Effects of omega-3 fatty acid plus alpha-tocopherol supplementation on malnutrition-inflammation score, biomarkers of inflammation and oxidative stress in chronic hemodialysis patients. Int. J. Nephrol. Urol. 2016, 48, 1887–1895. [Google Scholar] [CrossRef] [PubMed]
- Lemos, J.R.; Alencastro, M.G.; Konrath, A.V.; Cargnin, M.; Manfro, R.C. Flaxseed oil supplementation decreases C-reactive protein levels in chronic hemodialysis patients. Nutr. Res. 2012, 32, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Khalatbari Soltani, S.; Jamaluddin, R.; Tabibi, H.; Mohd Yusof, B.N.; Atabak, S.; Loh, S.P.; Rahmani, L. Effects of flaxseed consumption on systemic inflammation and serum lipid profile in hemodialysis patients with lipid abnormalities. Hemodial. Int. 2013, 17, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Mirfatahi, M.; Tabibi, H.; Nasrollahi, A.; Hedayati, M.; Taghizadeh, M. Effect of flaxseed oil on serum systemic and vascular inflammation markers and oxidative stress in hemodialysis patients: A randomized controlled trial. Int. J. Nephrol. Urol. 2016, 48, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Fumeron, C.; Nguyen-Khoa, T.; Saltiel, C.; Kebede, M.; Buisson, C.; Drueke, T.B.; Lacour, B.; Massy, Z.A. Effects of oral vitamin C supplementation on oxidative stress and inflammation status in haemodialysis patients. Nephrol. Dial. Transplant. 2005, 20, 1874–1879. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Li, Y.; Cheng, X.; Liu, L.; Bai, W.; Guo, W.; Wu, L.; Zuo, L. Cross-over study of influence of oral vitamin C supplementation on inflammatory status in maintenance hemodialysis patients. BMC Nephrol. 2013, 14, 252. [Google Scholar] [CrossRef] [PubMed]
- Hodkova, M.; Dusilova-Sulkova, S.; Kalousova, M.; Soukupova, J.; Zima, T.; Mikova, D.; Malbohan, I.M.; Bartunkova, J. Influence of oral vitamin E therapy on micro-inflammation and cardiovascular disease markers in chronic hemodialysis patients. Ren. Fail. 2006, 28, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Coloma, R.S.; Jocson, V.R.A. Effects of vitamin E on a biomarker of inflammation and precursors of atherogenesis in chronic hemodialysis patients. Philipp. J. Intern. Med. 2011, 49, 206–215. [Google Scholar]
- Ahmadi, A.; Mazooji, N.; Roozbeh, J.; Mazloom, Z.; Hasanzade, J. Effect of alpha-lipoic acid and vitamin E supplementation on oxidative stress, inflammation, and malnutrition in hemodialysis patients. Iran. J. Kidney Dis. 2013, 7, 461–467. [Google Scholar] [PubMed]
- Daud, Z.A.; Tubie, B.; Sheyman, M.; Osia, R.; Adams, J.; Tubie, S.; Khosla, P. Vitamin E tocotrienol supplementation improves lipid profiles in chronic hemodialysis patients. Vasc. Health Risk Manag. 2013, 9, 747–761. [Google Scholar] [PubMed]
- Sohrabi, Z.; Eftekhari, M.H.; Eskandari, M.H.; Rezaianzadeh, A.; Sagheb, M.M. Intradialytic oral protein supplementation and nutritional and inflammation outcomes in hemodialysis: A randomized controlled trial. Am. J. Kidney Dis. 2016, 68, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Sohrabi, Z.; Ekramzadeh, M.; Fallahzadeh, M.K.; Ayatollahi, M.; Geramizadeh, B.; Hassanzadeh, J.; Sagheb, M.M. Selenium supplementation improves the nutritional status of hemodialysis patients: A randomized, double-blind, placebo-controlled trial. Nephrol. Dial. Transplant. 2013, 28, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Omrani, H.R.; Rahimi, M.; Nikseresht, K. The effect of selenium supplementation on acute phase reactants and thyroid function tests in hemodialysis patients. Nephrourol. Mon. 2015, 7, e24781. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.W.; Lee, E.K.; Kim, T.H.; Min, W.K.; Chun, S.; Lee, K.U.; Kim, S.B.; Park, J.S. Effects of alpha-lipoic acid on the plasma levels of asymmetric dimethylarginine in diabetic end-stage renal disease patients on hemodialysis: A pilot study. Am. J. Nephrol. 2007, 27, 70–74. [Google Scholar] [CrossRef] [PubMed]
- El-Nakib, G.A.; Mostafa, T.M.; Abbas, T.M.; El-Shishtawy, M.M.; Mabrouk, M.M.; Sobh, M.A. Role of alpha-lipoic acid in the management of anemia in patients with chronic renal failure undergoing hemodialysis. Int. J. Nephrol. Renovasc. Dis. 2013, 6, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Khabbazi, T.; Mahdavi, R.; Safa, J.; Pour-Abdollahi, P. Effects of alpha-lipoic acid supplementation on inflammation, oxidative stress, and serum lipid profile levels in patients with end-stage renal disease on hemodialysis. J. Ren. Nutr. 2012, 22, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Safa, J.; Ardalan, M.R.; Rezazadehsaatlou, M.; Mesgari, M.; Mahdavi, R.; Jadid, M.P. Effects of alpha lipoic acid supplementation on serum levels of IL-8 and TNF-alpha in patient with ESRD undergoing hemodialysis. Int. J. Nephrol. Urol. 2014, 46, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Marckmann, P.; Agerskov, H.; Thineshkumar, S.; Bladbjerg, E.M.; Sidelmann, J.J.; Jespersen, J.; Nybo, M.; Rasmussen, L.M.; Hansen, D.; Scholze, A. Randomized controlled trial of cholecalciferol supplementation in chronic kidney disease patients with hypovitaminosis D. Nephrol. Dial. Transplant. 2012, 27, 3523–3531. [Google Scholar] [CrossRef] [PubMed]
- Hung, A.M.; Sundell, M.B.; Plotnikova, N.E.; Bian, A.; Shintani, A.; Ellis, C.D.; Siew, E.D.; Ikizler, T.A. A pilot study of active vitamin D administration and insulin resistance in African American patients undergoing chronic hemodialysis. J. Ren. Nutr. 2013, 23, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Seibert, E.; Heine, G.H.; Ulrich, C.; Seiler, S.; Kohler, H.; Girndt, M. Influence of cholecalciferol supplementation in hemodialysis patients on monocyte subsets: A randomized, double-blind, placebo-controlled clinical trial. Nephron Clin. Pract. 2013, 123, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Miskulin, D.C.; Majchrzak, K.; Tighiouart, H.; Muther, R.S.; Kapoian, T.; Johnson, D.S.; Weiner, D.E. Ergocalciferol supplementation in hemodialysis patients with vitamin d deficiency: A randomized clinical trial. J. Am. Soc. Nephrol. 2016, 27, 1801–1810. [Google Scholar] [CrossRef] [PubMed]
- Sirich, T.L.; Plummer, N.S.; Gardner, C.D.; Hostetter, T.H.; Meyer, T.W. Effect of increasing dietary fiber on plasma levels of colon-derived solutes in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1603–1610. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, R.; Pechenyak, B.; Vyas, U.; Ranganathan, P.; Weinberg, A.; Liang, P.; Mallappallil, M.C.; Norin, A.J.; Friedman, E.A.; Saggi, S.J. Randomized controlled trial of strain-specific probiotic formulation (Renadyl) in dialysis patients. Biomed Res. Int. 2014, 2014, 568571. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.M.; Ge, Y.Y.; Huang, X.; Zhang, Y.Q.; Li, J.X. Effects of fermentable dietary fiber supplementation on oxidative and inflammatory status in hemodialysis patients. Int. J. Clin. Exp. Med. 2015, 8, 1363–1369. [Google Scholar] [PubMed]
- Soleimani, A.; Zarrati Mojarrad, M.; Bahmani, F.; Taghizadeh, M.; Ramezani, M.; Tajabadi-Ebrahimi, M.; Jafari, P.; Esmaillzadeh, A.; Asemi, Z. Probiotic supplementation in diabetic hemodialysis patients has beneficial metabolic effects. Kidney Int. 2017, 91, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Himmelfarb, J.; Phinney, S.; Ikizler, T.A.; Kane, J.; McMonagle, E.; Miller, G. Gamma-tocopherol and docosahexaenoic acid decrease inflammation in dialysis patients. J. Ren. Nutr. 2007, 17, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Kamgar, M.; Zaldivar, F.; Vaziri, N.D.; Pahl, M.V. Antioxidant therapy does not ameliorate oxidative stress and inflammation in patients with end-stage renal disease. J. Natl. Med. Assoc. 2009, 101, 336–344. [Google Scholar] [CrossRef]
- Himmelfarb, J.; Ikizler, T.A.; Ellis, C.; Wu, P.; Shintani, A.; Dalal, S.; Kaplan, M.; Chonchol, M.; Hakim, R.M. Provision of antioxidant therapy in hemodialysis (PATH): A randomized clinical trial. J. Am. Soc. Nephrol. 2014, 25, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Viramontes-Horner, D.; Marquez-Sandoval, F.; Martin-del-Campo, F.; Vizmanos-Lamotte, B.; Sandoval-Rodriguez, A.; Armendariz-Borunda, J.; Garcia-Bejarano, H.; Renoirte-Lopez, K.; Garcia-Garcia, G. Effect of a symbiotic gel (lactobacillus acidophilus + bifidobacterium lactis + inulin) on presence and severity of gastrointestinal symptoms in hemodialysis patients. J. Ren. Nutr. 2015, 25, 284–291. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Li, M.S.; Lin, M.; Zhao, T.Y.; Gao, P. Effect of fish oil supplement in maintenance hemodialysis patients: A systematic review and meta-analysis of published randomized controlled trials. Eur. J. Clin. Pharmacol. 2016, 72, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Sun, Y.; Sun, W.; Yao, L.; Sun, L.; Liu, L.; Ma, J.; Wang, L. Effect of omega-3 fatty acid supplementation on serum lipids and vascular inflammation in patients with end-stage renal disease: A meta-analysis. Sci. Rep. 2016, 6, 39346. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Kelly, J.; Marshall, S.; Nakos, S.; Campbell, K.; Itsiopoulos, C. The effect of polyphenol-rich interventions on cardiovascular risk factors in haemodialysis: A systematic review and meta-analysis. Nutrients 2017, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Hussain, T.; Tan, B.; Yin, Y.; Blachier, F.; Tossou, M.C.; Rahu, N. Oxidative stress and inflammation: What polyphenols can do for us? Oxid. Med. Cell. Longev. 2016, 2016, 7432797. [Google Scholar] [CrossRef] [PubMed]
- Reiter, E.; Jiang, Q.; Christen, S. Anti-inflammatory properties of alpha- and gamma-tocopherol. Mol. Asp. Med. 2007, 28, 668–691. [Google Scholar] [CrossRef] [PubMed]
- Bowie, A.G.; O’Neill, L.A. Vitamin C inhibits NF-kappa B activation by TNF via the activation of p38 mitogen-activated protein kinase. J. Immunol. 2000, 165, 7180–7188. [Google Scholar] [CrossRef] [PubMed]
- Shay, K.P.; Moreau, R.F.; Smith, E.J.; Smith, A.R.; Hagen, T.M. Alpha-lipoic acid as a dietary supplement: Molecular mechanisms and therapeutic potential. Biochim. Biophys. Acta 2009, 1790, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Duntas, L.H. Selenium and inflammation: Underlying anti-inflammatory mechanisms. Horm. Metab. Res. 2009, 41, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Mechanisms of action of (n-3) fatty acids. J. Nutr. 2012, 142, 592s–599s. [Google Scholar] [CrossRef] [PubMed]
- Kaileh, M.; Sen, R. Role of nf-kappab in the anti-inflammatory effects of tocotrienols. J. Am. Coll. Nutr. 2010, 29, 334s–339s. [Google Scholar] [CrossRef] [PubMed]
- Vunta, H.; Davis, F.; Palempalli, U.D.; Bhat, D.; Arner, R.J.; Thompson, J.T.; Peterson, D.G.; Reddy, C.C.; Prabhu, K.S. The anti-inflammatory effects of selenium are mediated through 15-deoxy-delta12,14-prostaglandin J2 in macrophages. J. Biol. Chem. 2007, 282, 17964–17973. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.Q.; Khan, R.; Rehman, M.U.; Lateef, A.; Tahir, M.; Ali, F.; Sultana, S. Soy isoflavones (daidzein & genistein) inhibit 12-O-tetradecanoylphorbol-13-acetate (TPA)-induced cutaneous inflammation via modulation of COX-2 and NF-kappaB in swiss albino mice. Toxicology 2012, 302, 266–274. [Google Scholar] [PubMed]
- Yam, M.L.; Abdul Hafid, S.R.; Cheng, H.M.; Nesaretnam, K. Tocotrienols suppress proinflammatory markers and cyclooxygenase-2 expression in raw264.7 macrophages. Lipids 2009, 44, 787–797. [Google Scholar] [CrossRef] [PubMed]
- Meijer, K.; de Vos, P.; Priebe, M.G. Butyrate and other short-chain fatty acids as modulators of immunity: What relevance for health? Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Manach, C.; Scalbert, A.; Morand, C.; Remesy, C.; Jimenez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [PubMed]
- Chun, O.K.; Chung, S.J.; Claycombe, K.J.; Song, W.O. Serum C-reactive protein concentrations are inversely associated with dietary flavonoid intake in U.S. Adults. J. Nutr. 2008, 138, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Fanti, P.; Stephenson, T.J.; Kaariainen, I.M.; Rezkalla, B.; Tsukamoto, Y.; Morishita, T.; Nomura, M.; Kitiyakara, C.; Custer, L.J.; Franke, A.A. Serum isoflavones and soya food intake in japanese, thai and american end-stage renal disease patients on chronic haemodialysis. Nephrol. Dial. Transplant. 2003, 18, 1862–1868. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.A.; Beilin, L.J. Omega-3 fatty acids and inflammation. Curr. Atheroscler. Rep. 2004, 6, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Svensson, M.; Schmidt, E.B.; Jorgensen, K.A.; Christensen, J.H. N-3 fatty acids as secondary prevention against cardiovascular events in patients who undergo chronic hemodialysis: A randomized, placebo-controlled intervention trial. Clin. J. Am. Soc. Nephrol. 2006, 1, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Kutner, N.G.; Clow, P.W.; Zhang, R.; Aviles, X. Association of fish intake and survival in a cohort of incident dialysis patients. Am. J. Kidney Dis. 2002, 39, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S. Alpha-linolenic acid: A gift from the land? Circulation 2005, 111, 2872–2874. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Chung, S.H. Anti-inflammatory effect of alpha-linolenic acid and its mode of action through the inhibition of nitric oxide production and inducible nitric oxide synthase gene expression via NF-kappa B and mitogen-activated protein kinase pathways. J. Agric. Food Chem. 2007, 55, 5073–5080. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Liu, R.; Chang, M.; Huang, J.; Jin, Q.; Wang, X. Effect of dietary alpha-linolenic acid on blood inflammatory markers: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Nutr. 2018, 57, 277–891. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Liu, L.; Cheng, X.; Dong, J.; Geng, Q.; Zuo, L. Low levels of vitamin C in dialysis patients is associated with decreased prealbumin and increased C-reactive protein. BMC Nephrol. 2011, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Deved, V.; Poyah, P.; James, M.T.; Tonelli, M.; Manns, B.J.; Walsh, M.; Hemmelgarn, B.R. Ascorbic acid for anemia management in hemodialysis patients: A systematic review and meta-analysis. Am. J. Kidney Dis. 2009, 54, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K.; Khanna, S.; Roy, S. Tocotrienols: Vitamin E beyond tocopherols. Life Sci. 2006, 78, 2088–2098. [Google Scholar] [CrossRef] [PubMed]
- Heng, E.C.; Karsani, S.A.; Abdul Rahman, M.; Abdul Hamid, N.A.; Hamid, Z.; Wan Ngah, W.Z. Supplementation with tocotrienol-rich fraction alters the plasma levels of Apolipoprotein A-I precursor, Apolipoprotein E precursor, and C-reactive protein precursor from young and old individuals. Eur. J. Nutr. 2013, 52, 1811–1820. [Google Scholar] [CrossRef] [PubMed]
- Saboori, S.; Shab-Bidar, S.; Speakman, J.R.; Yousefi Rad, E.; Djafarian, K. Effect of vitamin E supplementation on serum C-reactive protein level: A meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2015, 69, 867–873. [Google Scholar] [CrossRef] [PubMed]
- D’Arrigo, G.; Baggetta, R.; Tripepi, G.; Galli, F.; Bolignano, D. Effects of vitamin E-coated versus conventional membranes in chronic hemodialysis patients: A systematic review and meta-analysis. Blood Purif. 2017, 43, 101–122. [Google Scholar] [CrossRef] [PubMed]
- Boaz, M.; Smetana, S.; Weinstein, T.; Matas, Z.; Gafter, U.; Iaina, A.; Knecht, A.; Weissgarten, Y.; Brunner, D.; Fainaru, M.; et al. Secondary prevention with antioxidants of cardiovascular disease in endstage renal disease (SPACE): Randomised placebo-controlled trial. Lancet 2000, 356, 1213–1218. [Google Scholar] [CrossRef]
- Tonelli, M.; Wiebe, N.; Hemmelgarn, B.; Klarenbach, S.; Field, C.; Manns, B.; Thadhani, R.; Gill, J. Trace elements in hemodialysis patients: A systematic review and meta-analysis. BMC Med. 2009, 7, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujishima, Y.; Ohsawa, M.; Itai, K.; Kato, K.; Tanno, K.; Turin, T.C.; Onoda, T.; Endo, S.; Okayama, A.; Fujioka, T. Serum selenium levels in hemodialysis patients are significantly lower than those in healthy controls. Blood Purif. 2011, 32, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Zachara, B.A.; Koterska, D.; Manitius, J.; Sadowski, L.; Dziedziczko, A.; Salak, A.; Wasowicz, W. Selenium supplementation on plasma glutathione peroxidase activity in patients with end-stage chronic renal failure. Biol. Trace Elem. Res. 2004, 97, 15–30. [Google Scholar] [CrossRef]
- Zachara, B.A.; Gromadzinska, J.; Zbrog, Z.; Swiech, R.; Wasowicz, W.; Twardowska, E.; Jablonska, E.; Sobala, W. Selenium supplementation to chronic kidney disease patients on hemodialysis does not induce the synthesis of plasma glutathione peroxidase. Acta Biochim. Pol. 2009, 56, 183–187. [Google Scholar] [PubMed]
- Gomes, M.B.; Negrato, C.A. Alpha-lipoic acid as a pleiotropic compound with potential therapeutic use in diabetes and other chronic diseases. Diabetol. Metab. Syndr. 2014, 6, 80. [Google Scholar] [CrossRef] [PubMed]
- Bucharles, S.; Barberato, S.H.; Stinghen, A.E.; Gruber, B.; Meister, H.; Mehl, A.; Piekala, L.; Dambiski, A.C.; Souza, A.; Olandoski, M.; et al. Hypovitaminosis D is associated with systemic inflammation and concentric myocardial geometric pattern in hemodialysis patients with low iPTH levels. Nephron Clin. Pract. 2011, 118, c384–c391. [Google Scholar] [CrossRef] [PubMed]
- Matias, P.J.; Jorge, C.; Ferreira, C.; Borges, M.; Aires, I.; Amaral, T.; Gil, C.; Cortez, J.; Ferreira, A. Cholecalciferol supplementation in hemodialysis patients: Effects on mineral metabolism, inflammation, and cardiac dimension parameters. Clin J. Am. Soc. Nephrol. 2010, 5, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Griffith, J.A.; Chasan-Taber, L.; Olendzki, B.C.; Jackson, E.; Stanek, E.J., 3rd; Li, W.; Pagoto, S.L.; Hafner, A.R.; Ockene, I.S. Association between dietary fiber and serum C-reactive protein. Am. J. Clin. Nutr. 2006, 83, 760–766. [Google Scholar] [CrossRef] [PubMed]
- North, C.J.; Venter, C.S.; Jerling, J.C. The effects of dietary fibre on C-reactive protein, an inflammation marker predicting cardiovascular disease. Eur. J. Clin. Nutr. 2009, 63, 921–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Huang, X.; Riserus, U.; Krishnamurthy, V.M.; Cederholm, T.; Arnlov, J.; Lindholm, B.; Sjogren, P.; Carrero, J.J. Dietary fiber, kidney function, inflammation, and mortality risk. Clin. J. Am. Soc. Nephrol. 2014, 9, 2104–2110. [Google Scholar] [CrossRef] [PubMed]
- McLoughlin, R.F.; Berthon, B.S.; Jensen, M.E.; Baines, K.J.; Wood, L.G. Short-chain fatty acids, prebiotics, synbiotics, and systemic inflammation: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2017, 106, 930–945. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Kopple, J.D.; Deepak, S.; Block, D.; Block, G. Food intake characteristics of hemodialysis patients as obtained by food frequency questionnaire. J. Ren. Nutr. 2002, 12, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Ahluwalia, N.; Albers, R.; Bosco, N.; Bourdet-Sicard, R.; Haller, D.; Holgate, S.T.; Jönsson, L.S.; Latulippe, M.E.; Marcos, A.; Moreines, J. A consideration of biomarkers to be used for evaluation of inflammation in human nutritional studies. Br. J. Nutr. 2013, 109 (Suppl. S1), S1–S34. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Author, Year | Country | Intervention | Content | Control | Duration (Month) | n | Mean Age (Year) | Gender (M/F) | Dialysis Vintage (Month) | Outcomes | Jadad Score [21] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Polyphenols | ||||||||||||
| 1 | Fanti et al., 2006 [22] | USA | Soy protein | Isoflavones (26–54 mg) | Milk protein | 2 | 25 | 61.0 | 15/10 | ≥3 months | ↔ CRP, ↔ IL-6, ↔TNF-α | 3 |
| 2 | Siefker et al., 2006 [23] | USA | Soy protein | Isoflavones (52 mg) | Whey protein | 1 | 17 | 50.3 | 7/10 | 13.0 | ↔ CRP, ↔TNF-α | 1 |
| 3 | Tomayko et al., 2014 [24] | USA | Soy isolate | Isoflavones (40 mg) | Whey protein | 6 a | 27 | 52.9 | 17/10 | ≥3 months | ↔ CRP, ↓ IL-6 | 2 |
| 4 | Shema-didi et al., 2012 [25] | Israel | Pomegranate juice | Polyphenol (0.7 mmol) | Placebo juice | 12 | 101 | 65.9 | 55/46 | 27.6 | ↓ IL-6, ↓ TNF-α | 4 |
| 5 | Wu, 2015 [26] | USA | Pomegranate extract | Gallic acid (600–755 mg) | Placebo | 6 | 27 | 54.3 | 17/10 | 75.5 | ↔ CRP, ↔ IL-6 | 4 |
| 6 | Rassaf et al., 2016 [27] | Germany | Cocoa flavanols | Flavanols (900 mg) | Placebo drink | 1 | 52 | 65.5 | 38/14 | 43 b | ↔ CRP, ↔ IL-6 | 5 |
| 7 | Janiques et al., 2014 [28] | Brazil | Grape jelly + grape powder | Polyphenol (12–500 mg) | Grape jelly | 1.15 | 32 | 52.9 | 18/14 | 111 | ↔ CRP | 4 |
| 8 | Pakferat et al., 2014 [29] | Iran | Tumeric | Curcumin 66.3 mg | Placebo | 8 | 100 | 53.3 | 60/40 | 5.0 | ↓ CRP | 4 |
| Omega-3 Fatty Acids | ||||||||||||
| 9 | Saifullah et al., 2007 [30] ‡ | USA | Omega 3 Fatty Acid | EPA 854 mg, DHA 488 mg | Soybean/corn oil | 3 | 23 | 57.5 | 18/5 | N/A | ↓ CRP | 5 |
| 10 | Bowden et al., 2009 [31] | USA | Omega 3 Fatty Acid | EPA 960 mg, DHA 600 mg | Corn oil | 6 | 33 | 60.8 | 19/14 | N/A | ↓ CRP | 5 |
| 11 | Kooshki et al., 2011 [32] ‡ | Iran | Omega 3 Fatty acid | EPA 1240 mg, DHA 760 mg | MCT | 2.5 | 34 | 50.0 | 21/13 | 24.5 | ↔ CRP, ↔ IL-6, ↔ TNF-α | 4 |
| 12 | Poulia et al., 2011 [33] ‡ | Greece | Omega 3 fatty acid | EPA 1840 mg, DHA 760 mg, α-TP 8 mg | α-TP | 1 | 25 | 51.0 | 16/9 | 112.8 | ↔ CRP | 3 |
| 13 | Daud et al., 2012 [34] ‡ | USA | Omega 3 Fatty Acid | EPA 1800 mg, DHA 600 mg | Olive oil | 6 a | 55 | 58.5 | 32/31 | 41.4 | ↔ CRP | 4 |
| 14 | Gharekhani et al., 2014 [35] ‡ | Iran | Omega 3 Fatty acid | EPA 1080 mg, DHA 720 mg | Paraffin oil | 4 | 45 | 57.0 | 25/20 | 65.9 | ↔ CRP, ↔ IL-6, ↔ TNF-α | 3 |
| 15 | Hung et al., 2014 [36] ‡ | USA | Omega 3 Fatty acid | EPA 1933 mg, DHA 967 mg | Placebo | 3 | 34 | 52.0 b | 27/7 | 47 b | ↔ CRP, ↔ IL-6, ↔ TNF-α | 4 |
| 16 | Lee, 2015 [37] ‡ | Korea | Omega 3 Fatty Acid | EPA 1104 mg, DHA 912 mg | Olive oil | 3 | 15 | 62. | 5/10 | ≥6 months | ↔ CRP | 5 |
| 17 | Harving et al., 2015 [38] ‡ | Denmark | Omega 3 Fatty Acid | EPA 765 mg, DHA 638 mg | Olive oil | 3 | 162 | 66.7 | 96/56 | 45.6 | ↔ CRP | 5 |
| 18 | Asemi, 2016 [39] ‡ | Iran | Omega 3 Fatty Acid | EPA 600 mg, DHA 300 mg and 300 mg other omega-3 fatty acids | Placebo | 3 | 60 | 57.6 | 40/20 | 42.0 | ↔ CRP | 5 |
| 19 | Lemos et al., 2012 [40] ‡ | Brazil | Flaxseed oil | 2 g | Mineral oil | 4 | 145 | 57.0 | 85/60 | ≥3 months | ↓ CRP | 4 |
| 20 | Khalatbari Soltani et al., 2012 [41] ‡ | Iran | Flaxseed | Fat 13.5 g, fiber 6.7 g | Control | 2 | 30 | 54.3 | 16/14 | 32.5 | ↓ CRP | 2 |
| 21 | Mirfatahi, 2016 [42] ‡ | Iran | Flaxseed oil | 6 g | MCT oil | 2 | 34 | 54.3 | 22/12 | 32.5 | ↓ CRP | 5 |
| Antioxidants | ||||||||||||
| 22 | Fumeron et al., 2005 [43] | France | Vitamin C | 250 mg | Control | 2a | 33 | 52.0 | 20/13 | 71.5 | ↔ CRP | 2 |
| 23 | Zhang et al., 2013 [44] | China | Vitamin C | 200 mg | Control | 3 | 100 | 64.4 | 47/53 | 48 b | ↓ CRP | 2 |
| 24 | Hodkova et al., 2006 [45] ‡ | Czech Republic | α-TP | 888 IU | Control | 1.15 | 29 | 61.6 | 10/19 | 32 | ↔ CRP | 2 |
| 25 | Coloma et al., 2011 [46] ‡ | Philippine | α-TP | 400 IU | Placebo | 2 | 50 | 59.7 | 36/14 | N/A | ↔ CRP | 4 |
| 26 | Ahmadi et al., 2013 [47] ‡ | Iran | α-TP | 400 IU | Placebo | 2 | 41 | 46.8 | 20/21 | 180 | ↔ CRP, ↓ IL-6 | 2 |
| 27 | Daud et al., 2013 [48] ‡ | USA | TT | 180 mg | Placebo | 4 | 81 | 58.5 | 43/38 | ≥3 months | ↔ CRP, ↔ IL-6 | 5 |
| 28 | Sohrabi et al., 2016 [49] ‡ | Iran | α-TP | 600 IU | Control | 2 | 69 | 56.3 | 37/32 | N/A | ↔ CRP, ↓ IL-6 | 3 |
| 29 | Asemi et al., 2016 [39] ‡ | Iran | α-TP | 400 IU | Placebo | 3 | 60 | 60.6 | 40/20 | 41.4 | ↔ CRP | 5 |
| 30 | Salehi et al., 2013 [50] | Iran | Selenium | 200 μg | Placebo | 3 | 80 | 52.5 | 36/44 | ≥3 months | ↔ CRP, ↓ IL-6 | 4 |
| 31 | Omrani et al., 2015 [51] | Iran | Selenium | 200 μg | Placebo | 3 | 64 | 58.4 | 30/34 | ≥6 months | ↔ CRP | 4 |
| 32 | Chang et al., 2007 [52] | Korea | α-lipoic acids | 600 mg | Control | 3 | 50 | 64.5 | 27/23 | N/A | ↔ CRP | 2 |
| 33 | Ahmadi et al., 2013 [47] | Iran | α-lipoic acids | 600 mg | Placebo | 2 | 44 | 48.9 | 23/21 | 18.1 | ↔ CRP, ↔ IL-6 | 2 |
| 34 | El-Nakib et al., 2013 [53] | Egypt | α-lipoic acids | 600 mg | Control | 3 | 44 | 47.7 | 24/20 | 92.4 | ↔ IL-6, ↔ TNF-α | 2 |
| 35 | Khabbazi et al., 2012 [54] | Iran | α-lipoic acids | 600 mg | Control | 2 | 52 | 53.9 | 34/18 | 55.3 | ↓ CRP | 2 |
| 36 | Safa et al., 2014 [55] | Iran | α-lipoic acids | 600 mg | Placebo | 2 | 61 | 57.2 | 42/19 | 79.6 | ↔ TNF-α | 3 |
| Vitamin D | ||||||||||||
| 37 | Marckmann et al., 2012 [56] | Denmark | Cholecalcife-rol | 40,000 IU | Placebo | 2 | 27 | N/A | N/A | N/A | ↔ CRP, ↔ IL-6 | 5 |
| 38 | Hung et al., 2013 [57] | USA | Paracalcitol | As per KDOQI guidelines | Cinacalcet | 2 | 10 | 48.5 | 6/4 | 40 b | ↔ CRP, ↔ IL-6 | 3 |
| 39 | Seibert et al., 2013 [58] | Germany | Cholecalcife-rol | 20,000 IU | Placebo | 3 | 33 | 67.2 | 18/15 | 25.2 | ↔ CRP, ↔ TNF-α | 5 |
| 40 | Miskulin et al., 2016 [59] | USA | Ergocalcife-rol | 50,000 IU | Placebo | 6 | 252 | 61.1 | N/A | 42 b | ↔ CRP | 5 |
| Fibers & Probiotics | ||||||||||||
| 41 | Sirich et al., 2014 [60] | USA | High amylose corn starch | 15 g | Waxy corn starch | 1.4 | 40 | 56.0 | 24/16 | 48.0 | ↔ CRP | 3 |
| 42 | Natarajan et al., 2014 [61] | USA | Probiotics | S. thermophilus KB 19, L. acidophilus KB 27, and B. longum KB 31 (3 × 109 CFU) | Cream of wheat and psyllium husk | 2 | 22 | 54 | 6/16 | N/A | ↔ CRP | 3 |
| 43 | Xie et al., 2015 [62] | China | Water soluble fiber | 10 g and 20 g | Placebo starch | 1.5 | 124 | 52.8 | 68/56 | 22.6 | ↓ CRP, ↓ IL-6, ↓ TNF-α | 2 |
| 44 | Soleimani et al., 2016 [63] | Iran | Probiotics | L. acidophilus, L. casei, and B. bifidum (2 × 109 CFU/g each) | Placebo | 3 | 60 | 56.7 | 40/20 | 42.6 | ↓ CRP | 5 |
| Nutrient Combinations | ||||||||||||
| 45 | Himmelfarb et al., 2007 [64] | USA | γ–TP + DHA | γ–TP (308 mg) and DHA (800 mg) | High Oleic Sunflower oil | 2 | 63 | 59.6 | 40/23 | 28.1 | ↔ CRP, ↓ IL-6 | 5 |
| 46 | Kamgar et al., 2009 [65] | USA | Antioxidants | Vitamin E (800 IU), vitamin C (250 mg), B6 (100 mg), B12 (250 μg), and folic acid (10 mg) | Placebo | 2 | 37 | 52.1 | 22/15 | 53.6 | ↔ CRP, ↔ IL-6 | 3 |
| 47 | Ahmadi et al, 2013 [47] | Iran | Vitamin E and α-lipoic acids | Vitamin E (400 IU) and α-lipoic acids (600 mg) | Placebo | 2 | 48 | 51.1 | 20/28 | 17.7 | ↔ CRP, ↓ IL-6 | 2 |
| 48 | Himmelfarb et al., 2014 [66] | USA | Mixed TP and α-lipoic acids | Mixed TP (666 IU) and α-lipoic acids (600 mg) | Placebo | 6 | 325 | 59.0 | 143/182 | 51.5 | ↔ CRP, ↔ IL-6 | 5 |
| 49 | Viramontes-Horner et al., 2015 [67] | Mexico | Synbiotic gel, omega-3 fatty acids, and vitamins | L. acidophilus NCFM and Bifidobacterium lactis Bi-07 (11 × 106 CFU); inulin (2.31 g) EPA and DHA (1.5 g); and vitamins (complex B, folic acid, ascorbic acid, and vitamin E). | Placebo | 2 | 42 | 39.8 | 32/10 | 60.3 | ↔ CRP, ↔ IL-6, ↔ TNF-α | 4 |
| 50 | Asemi et al., 2016 [39] | Iran | α-TP, EPA, and DHA | α-TP (400 IU), EPA (600 mg), and DHA (300 mg) | Placebo | 3 | 60 | 57.4 | 40/20 | 40.8 | ↔ CRP | 5 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khor, B.-H.; Narayanan, S.S.; Sahathevan, S.; Gafor, A.H.A.; Daud, Z.A.M.; Khosla, P.; Sabatino, A.; Fiaccadori, E.; Chinna, K.; Karupaiah, T. Efficacy of Nutritional Interventions on Inflammatory Markers in Haemodialysis Patients: A Systematic Review and Limited Meta-Analysis. Nutrients 2018, 10, 397. https://doi.org/10.3390/nu10040397
Khor B-H, Narayanan SS, Sahathevan S, Gafor AHA, Daud ZAM, Khosla P, Sabatino A, Fiaccadori E, Chinna K, Karupaiah T. Efficacy of Nutritional Interventions on Inflammatory Markers in Haemodialysis Patients: A Systematic Review and Limited Meta-Analysis. Nutrients. 2018; 10(4):397. https://doi.org/10.3390/nu10040397
Chicago/Turabian StyleKhor, Ban-Hock, Sreelakshmi Sankara Narayanan, Sharmela Sahathevan, Abdul Halim Abdul Gafor, Zulfitri Azuan Mat Daud, Pramod Khosla, Alice Sabatino, Enrico Fiaccadori, Karuthan Chinna, and Tilakavati Karupaiah. 2018. "Efficacy of Nutritional Interventions on Inflammatory Markers in Haemodialysis Patients: A Systematic Review and Limited Meta-Analysis" Nutrients 10, no. 4: 397. https://doi.org/10.3390/nu10040397