
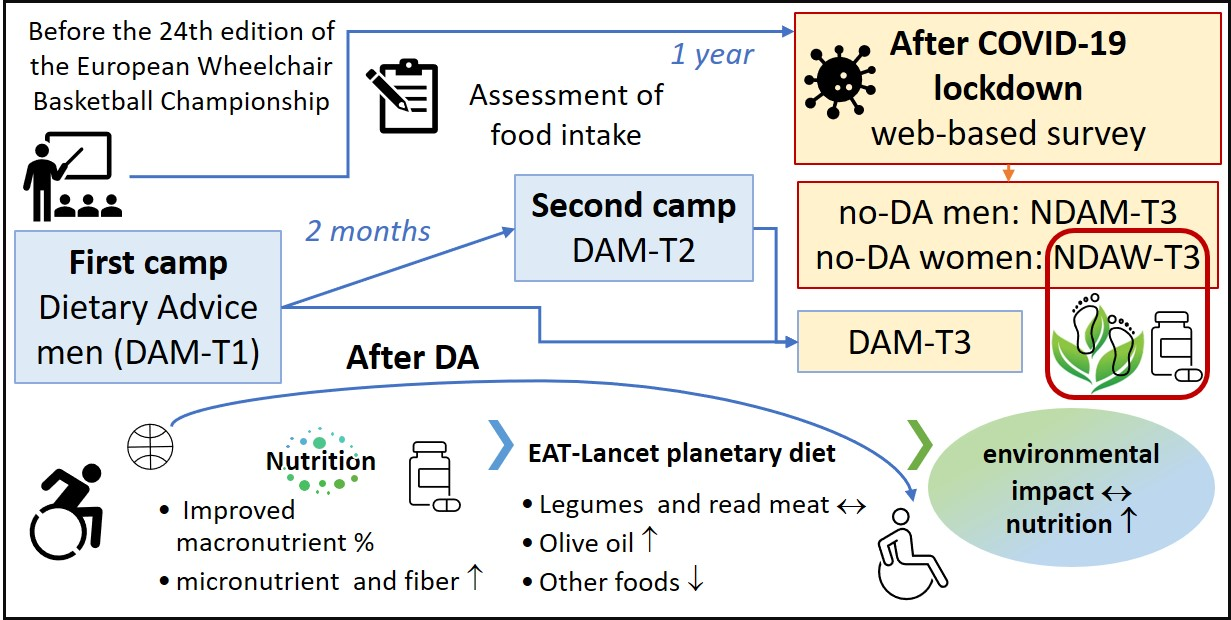
Longitudinal Effects of Dietary Advice on Wheelchair Basketball Athletes: Nutritional and Environmental Aspects

 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Methods
2.1. Recruitment and Study Design
2.2. Data Collection and Analysis
2.3. Statistics
3. Results
3.1. Characteristics and Post-LD Survey
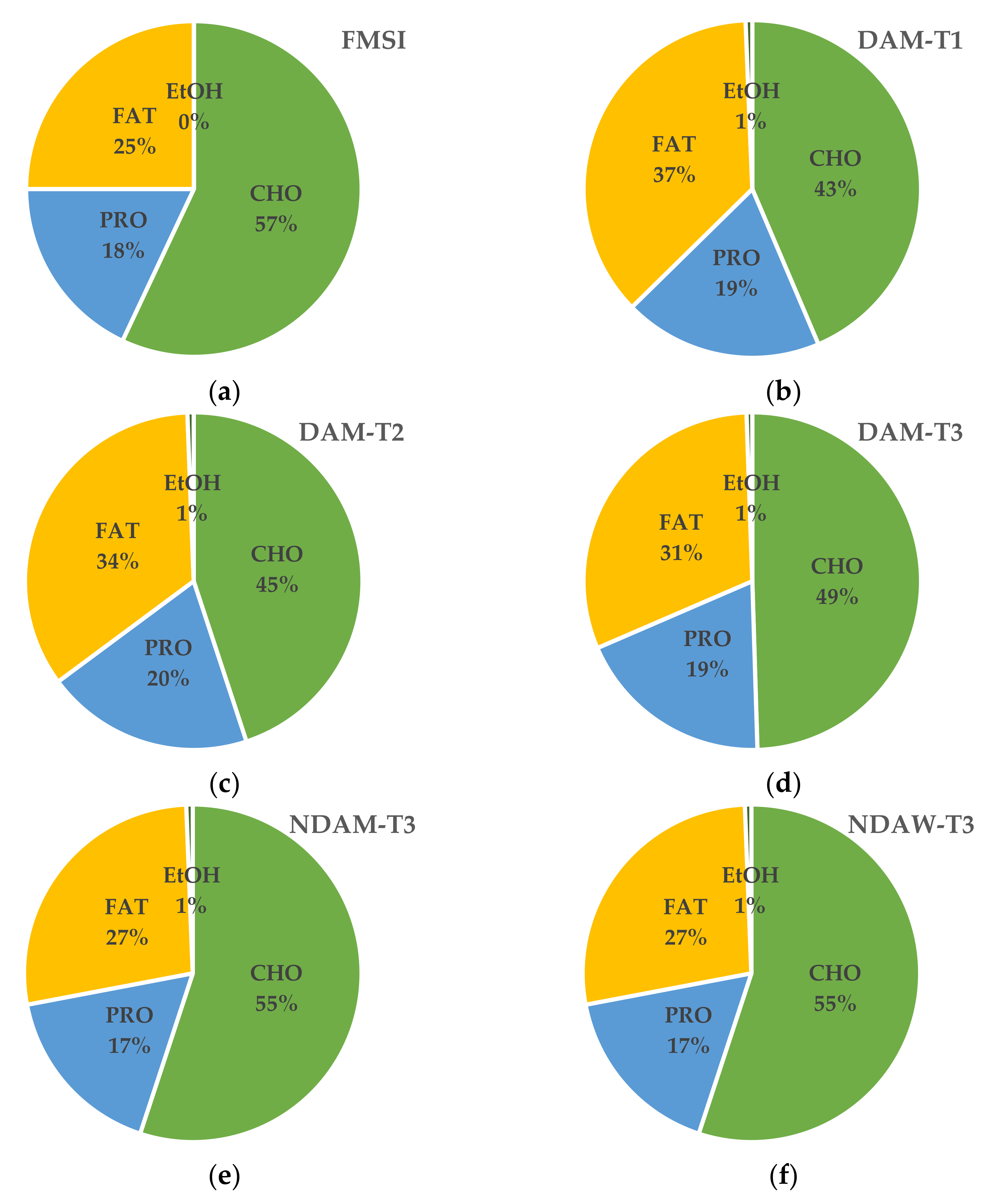
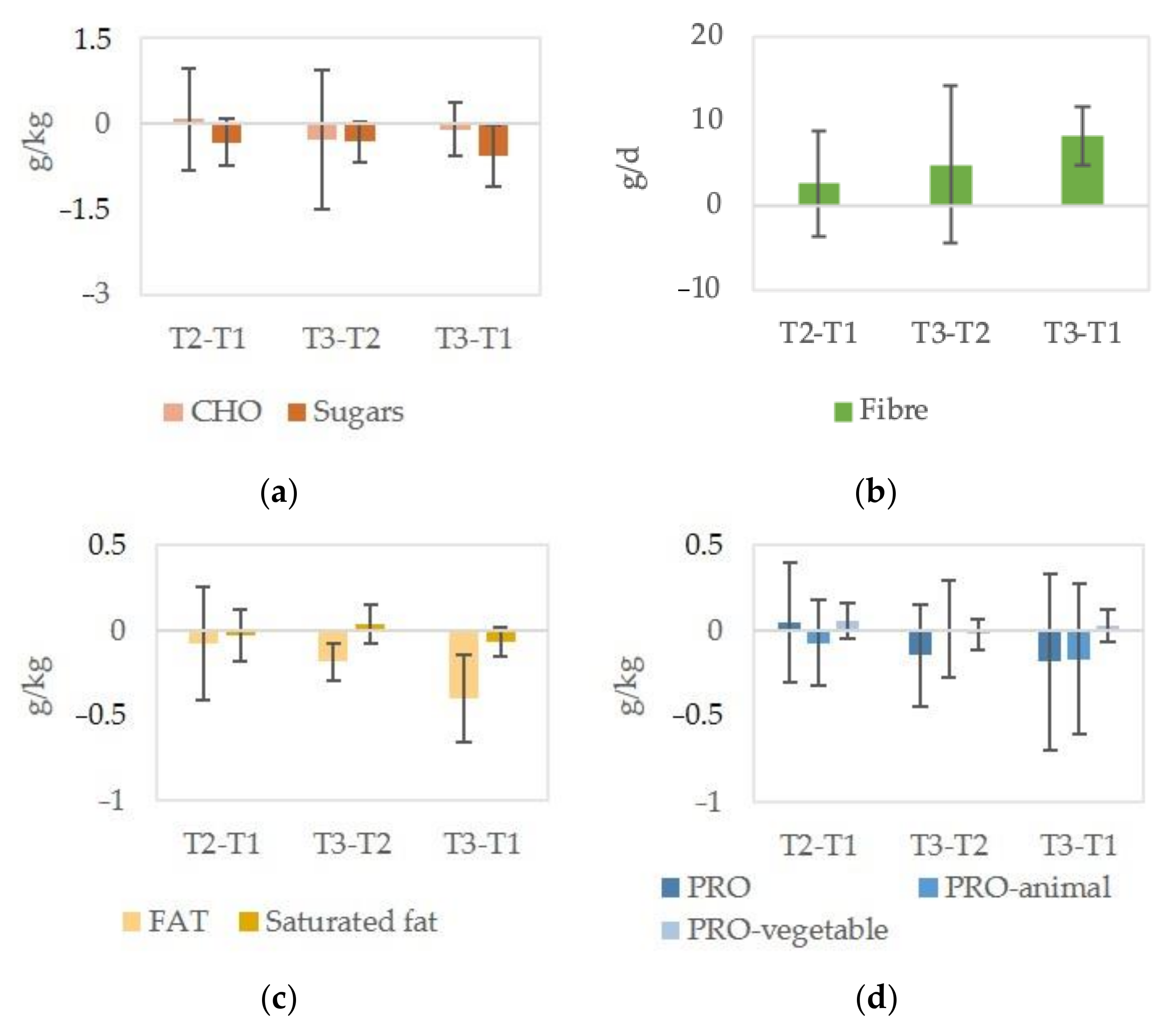
3.2. Dietary Intakes
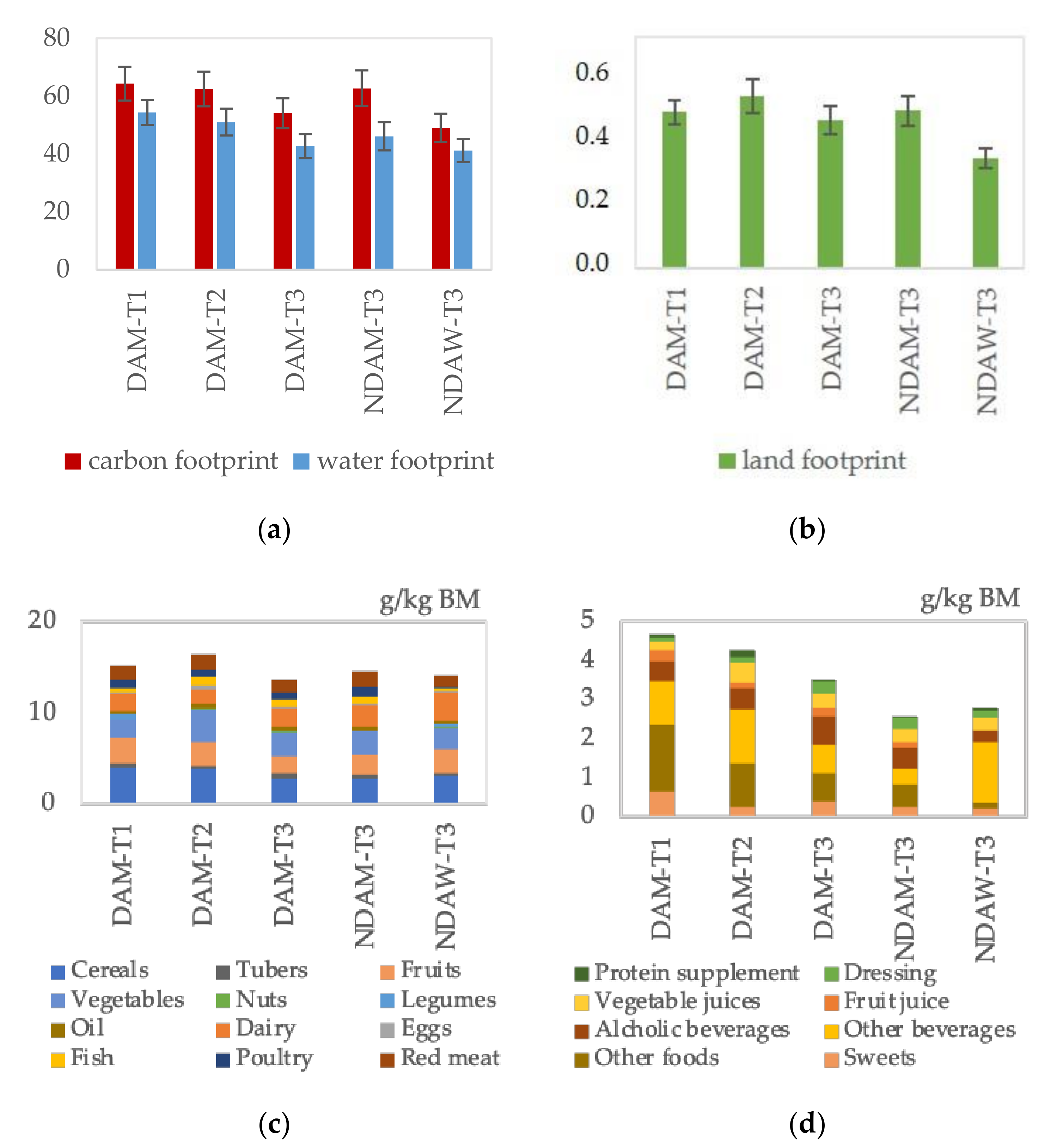
3.3. Diet Sustainability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Willett, W.J.; Rockstrom, B.; Loken, M.; Springmann, T.; Lang, S.; Vermeulen, T.; Garnett, D.; Tilman, F.; DeClerck, A.; Wood, M.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Grosso, G.A.; Mateo, N.; Rangelov, T.; Buzeti, T.; Birt, C. Nutrition in the context of the Sustainable Development Goals. Eur. J. Public Health 2020, 30 (Suppl. S1), i19–i23. [Google Scholar] [CrossRef]
- Serafini, M.; Toti, E. Unsustainability of Obesity: Metabolic Food Waste. Front. Nutr. 2016, 3, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolland, B.; Haesebaert, F.; Zante, E.; Benyamina, A.; Haesebaert, J.; Franck, N. Global Changes and Factors of Increase in Caloric/Salty Food Intake, Screen Use, and Substance Use During the Early COVID-19 Containment Phase in the General Population in France: Survey Study. JMIR Public Health Surveill 2020, 6, e19630. [Google Scholar] [CrossRef] [PubMed]
- Buckland, N.J.; Swinnerton, L.F.; Ng, K.; Price, M.; Wilkinson, L.L.; Myers, A.; Dalton, M. Susceptibility to increased high energy dense sweet and savoury food intake in response to the COVID-19 lockdown: The role of craving control and acceptance coping strategies. Appetite 2021, 158, 105017. [Google Scholar] [CrossRef]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Hardman, C.A. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Franco, I.; Bianco, A.; Bonfiglio, C.; Sorino, P.; Mirizzi, A.; Campanella, A.; Buongiorno, C.; Liuzzi, R.; Osella, A.R. Decreased levels of physical activity: Results from a cross-sectional study in southern Italy during the COVID-19 lockdown. J. Sports Med. Phys. Fit. 2021, 61, 294–300. [Google Scholar] [CrossRef]
- Huber, B.C.; Steffen, J.; Schlichtiger, J.; Brunner, S. Altered nutrition behavior during COVID-19 pandemic lockdown in young adults. Eur. J. Nutr. 2020, 1–10. [Google Scholar] [CrossRef]
- Ruiz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Rangel Bousquet Carrilho, T.; de Oliveira Cardoso, L.; et al. Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef]
- Batlle-Bayer, L.; Aldaco, R.; Bala, A.; Puig, R.; Laso, J.; Margallo, M.; Vázquez-Rowe, I.; Antó, J.M.; Fullana-I-Palmer, P. Environmental and nutritional impacts of dietary changes in Spain during the COVID-19 lockdown. Sci. Total Environ. 2020, 748, 141410. [Google Scholar] [CrossRef] [PubMed]
- Scarmozzino, F.; Visioli, F. Covid-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Scacchi, A.; Catozzi, D.; Boietti, E.; Bert, F.; Siliquini, R. COVID-19 Lockdown and Self-Perceived Changes of Food Choice, Waste, Impulse Buying and Their Determinants in Italy: QuarantEat, a Cross-Sectional Study. Foods 2021, 10, 306. [Google Scholar] [CrossRef] [PubMed]
- Attwood, S.; Hajat, C. How will the COVID-19 pandemic shape the future of meat consumption? Public Health Nutr. 2020, 23, 3116–3120. [Google Scholar] [CrossRef] [PubMed]
- Didinger, C.; Thompson, H. Motivating Pulse-Centric Eating Patterns to Benefit Human and Environmental Well-Being. Nutrients 2020, 12, 3500. [Google Scholar] [CrossRef] [PubMed]
- Marty, L.; de Lauzon-Guillain, B.; Labesse, M.; Nicklaus, S. Food choice motives and the nutritional quality of diet during the COVID-19 lockdown in France. Appetite 2021, 157, 105005. [Google Scholar] [CrossRef]
- Pérez-Rodrigo, C.; Citores, M.G.; Bárbara, G.H.; Ruiz-Litago, F.; Sáenz, L.C.; Arija, V.; López-Sobaler, A.; de Victoria, E.M.; Ortega, R.; Partearroyo, T.; et al. Patterns of Change in Dietary Habits and Physical Activity during Lockdown in Spain due to the COVID-19 Pandemic. Nutrients 2021, 13, 300. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Pugliese, G.; Framondi, L.; Di Matteo, R.; Laudisio, D.; Savastano, S.; Colao, A.; Muscogiuri, G. Does Sars-Cov-2 threaten our dreams? Effect of quarantine on sleep quality and body mass index. J. Transl. Med. 2020, 18, 1–11. [Google Scholar] [CrossRef]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef]
- Clemente-Suárez, V.J.; Fuentes-García, J.P.; Marcos, R.D.L.V.; Patiño, M.J.M. Modulators of the Personal and Professional Threat Perception of Olympic Athletes in the Actual COVID-19 Crisis. Front. Psychol. 2020, 11, 1985. [Google Scholar] [CrossRef]
- Figel, K.; Pritchett, K.; Pritchett, R.; Broad, E. Energy and Nutrient Issues in Athletes with Spinal Cord Injury: Are They at Risk for Low Energy Availability? Nutrients 2018, 10, 1078. [Google Scholar] [CrossRef] [Green Version]
- Goosey-Tolfrey, V.L.; Crosland, J. Nutritional Practices of Competitive British Wheelchair Games Players. Adapt. Phys. Act. Q. 2010, 27, 47–59. [Google Scholar] [CrossRef]
- Eskici, G.; Ersoy, G. An evaluation of wheelchair basketball players’ nutritional status and nutritional knowledge levels. J. Sports Med. Phys. Fit. 2014, 56, 259–268. [Google Scholar]
- Raguzzini, A.; Toti, E.; Bernardi, M.; Castellucci, F.; Cavedon, V.; Fedullo, A.L.; Milanese, C.; Sciarra, T.; Peluso, I. Post-Exercise Ketosis, Salivary Uric Acid and Interleukin-6 after a Simulated Wheelchair Basketball Match. Endocr. Metab. Immune Disord. Drug Targets 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Toti, E.; Cavedon, V.; Raguzzini, A.; Fedullo, A.L.; Milanese, C.; Bernardi, E.; Bellito, S.; Bernardi, M.; Sciarra, T.; Peluso, I. Dietary Intakes and Food Habits of Wheelchair Basketball Athletes compared to Gym Attendees and Individuals who do not Practice Sport Activity. Endocr. Metab. Immune Disord. Drug Targets 2021, 21, 1. [Google Scholar] [CrossRef] [PubMed]
- Grams, L.; Garrido, G.; Villacieros, J.; Ferro, A. Marginal Micronutrient Intake in High-Performance Male Wheelchair Basketball Players: A Dietary Evaluation and the Effects of Nutritional Advice. PLoS ONE 2016, 11, e0157931. [Google Scholar] [CrossRef] [Green Version]
- Ferro, A.; Garrido, G.; Villacieros, J.; Pérez, J.; Grams, L. Nutritional Habits and Performance in Male Elite Wheelchair Basketball Players During a Precompetitive Period. Adapt. Phys. Act. Q. 2017, 34, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Silva, I.; Azevedo, J.; Rodrigues, S.; Seixas, A.; Jorge, M. Predicting musculoskeletal symptoms in workers of a manufacturing company. Int. J. Occup. Saf. Ergon. 2020, 1–9. [Google Scholar] [CrossRef]
- Gobba, F.; Gherisi, R.; Martinelli, S.; Richeldi, A.; Clerici, P.; Grazioli, P. Traduzione in lingua italiana e validazione del questionario standardizzato Nordic IRSST per la rilevazione di disturbi muscoloscheletrici. Med. Lav. 2008, 99, 424–443. [Google Scholar] [PubMed]
- Willett, W. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Bernardi, M.; Fedullo, A.L.; Bernardi, E.; Munzi, D.; Peluso, I.; Myers, J.; Lista, F.R.; Sciarra, T. Diet in neurogenic bowel management: A viewpoint on spinal cord injury. World J. Gastroenterol. 2020, 26, 2479–2497. [Google Scholar] [CrossRef]
- Berardy, A.; Costello, C.; Seager, T. Life Cycle Assessment of Soy Protein Isolate. In Proceedings of the International Symposium on Sustainable Systems and Technologies, Dearborn, MI, USA, 18–20 May 2015. [Google Scholar] [CrossRef]
- Bacenetti, J.; Bava, L.; Schievano, A.; Zucali, M. Whey protein concentrate (WPC) production: Environmental impact assessment. J. Food Eng. 2018, 224, 139–147. [Google Scholar] [CrossRef]
- Cancello, R.; Soranna, D.; Zambra, G.; Zambon, A.; Invitti, C. Determinants of the Lifestyle Changes during COVID-19 Pandemic in the Residents of Northern Italy. Int. J. Environ. Res. Public Health 2020, 17, 6287. [Google Scholar] [CrossRef] [PubMed]
- Tornaghi, M.; Lovecchio, N.; Vandoni, M.; Chirico, A.; Codella, R. Physical activity levels across COVID-19 outbreak in youngsters of Northwestern Lombardy. J. Sports Med. Phys. Fit. 2020. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Shimizu, Y.; Mutsuzaki, H.; Tachibana, K.; Hotta, K.; Wadano, Y. Investigation of the Female Athlete Triad in Japanese Elite Wheelchair Basketball Players. Medicina 2019, 56, 10. [Google Scholar] [CrossRef] [Green Version]
- Petchkrua, W.; Little, J.W.; Burns, S.P.; Stiens, S.A.; James, J.J. Vitamin B12 deficiency in spinal cord injury: A retrospective study. J. Spinal Cord Med. 2003, 26, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.Z.; Liu, Y.P.; Liu, S.; Yan, M.; Hu, S.J.; Song, X.J. Systematic administration of B vitamins attenuates neuropathic hyperalgesia and reduces spinal neuron injury following temporary spinal cord ischaemia in rats. Eur. J. Pain 2014, 18, 76–85. [Google Scholar] [CrossRef]
- Riffel, A.; Santos, M.; De Souza, J.; Scheid, T.; Horst, A.; Kolberg, C.; Bello-Klein, A.; Partata, W. Treatment with ascorbic acid and α-tocopherol modulates oxidative-stress markers in the spinal cord of rats with neuropathic pain. Braz. J. Med. Biol. Res. 2018, 51, 7097. [Google Scholar] [CrossRef] [Green Version]
- Matossian-Motley, D.L.; Drake, D.A.; Samimi, J.S.; Camargo, C.A., Jr.; Quraishi, S.A. Association Between Serum 25(OH)D Level and Nonspecific Musculoskeletal Pain in Acute Rehabilitation Unit Patients. JPEN J. Parenter. Enteral. Nutr. 2016, 40, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Williams, T.G.; Ehsanian, R.; Shem, K.L.; Wright, J.; Isaac, L.; Crew, J. The Effect of Vitamin D Supplementation on Pain, Mood, Depression, and Strength in Patients with Spinal Cord Injury. PM&R 2016, 8, S153. [Google Scholar] [CrossRef]
- Madden, R.F.; Shearer, J.; Legg, D.; Parnell, J.A. Evaluation of Dietary Supplement Use in Wheelchair Rugby Athletes. Nutrients 2018, 10, 1958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaabouni, M.; Feki, W.; Chaabouni, K.; Kammoun, S. Vitamin D supplementation to prevent COVID-19 in patients with COPD: A research perspective. Adv. Respir. Med. 2020, 88, 364–365. [Google Scholar] [CrossRef]
- COVID-19 Rapid Guideline: Vitamin D. London, 2020. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33378143 (accessed on 14 February 2021).
- Grosso, G.; Fresán, U.; Bes-Rastrollo, M.; Marventano, S.; Galvano, F. Environmental Impact of Dietary Choices: Role of the Mediterranean and Other Dietary Patterns in an Italian Cohort. Int. J. Environ. Res. Public Health 2020, 17, 1468. [Google Scholar] [CrossRef] [Green Version]
- Menozzi, D.; Sogari, G.; Mora, C. Explaining Vegetable Consumption among Young Adults: An Application of the Theory of Planned Behaviour. Nutrients 2015, 7, 7633–7650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buscemi, S.; Mattina, A.; Rosafio, G.; Massenti, F.M.; Galvano, F.; Grosso, G.; Amodio, E.; Barile, A.M.; Maniaci, V.; Bonura, A.; et al. Habitual street food intake and subclinical carotid atherosclerosis. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2014, 19, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, S.; Barile, A.; Maniaci, V.; Batsis, J.A.; Mattina, A.; Verga, S. Characterization of street food consumption in palermo: Possible effects on health. Nutr. J. 2011, 10, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buscemi, S.; Maniaci, V.; Barile, A.M.; Rosafio, G.; Mattina, A.; Canino, B.; Verga, S.; Rini, G.B. Endothelial function and other biomarkers of cardiovascular risk in frequent consumers of street food. Clin. Nutr. 2012, 31, 934–939. [Google Scholar] [CrossRef]
- Fedullo, A.L.; Ciccotti, M.; Giannotta, P.; Alviti, F.; Bernardi, M.; Raguzzini, A.; Toti, E.; Sciarra, T.; Peluso, I. Hormetic Effects of Bioactive Compounds from Foods, Beverages, and Food Dressing: The Potential Role in Spinal Cord Injury. Oxidative Med. Cell. Longev. 2021, 2021, 6615752. [Google Scholar] [CrossRef]
- Polito, A.; Peluso, I. Effects of Olive Oil on TNF-α and IL-6 in Humans: Implication in Obesity and Frailty. Endocr. Metab. Immune Disord. Drug Targets 2017, 18, 63–74. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | DAM-T1 (n = 16) | DAM-T2 (n = 12) | DAM-T3 (n = 12) | NDAM-T3 (n = 12) | NDAW-T3 (n = 9) |
|---|---|---|---|---|---|
| Age (year) | 27 (24–31) a | 27 (25–31) a | 28 (25–30) a | 19 (18–21) b | 26 (19–30) a,b |
| National Team | 100% Senior | 100% Senior | 100% Senior | 47% Senior | 100% Women |
| IWBF class | 2.5 (1.5–4.0) | 3.0 (1.6–4.0) | 4.0 (2.5–4.2) | 2.5 (1.7–3.2) | 2.5 (1.2–3.2) |
| Health condition | 8 SCI/SB, 5 AMP, 3 OHC | 5 SCI/SB, 4 AMP, 3 OHC | 3 SCI/SB, 4 AMP, 5 OHC | 6 SCI/SB, 2 AMP, 4 OHC | 4 SCI/SB, 1 AMP, 4 OHC |
| BM (kg) | 74.2 ± 12.3 a | 76.4 ± 11.7 a | 72.8 ± 9.8 a | 57.2 ± 11.7 b | 61.0 ± 10.6 b |
| BM variation | measured difference (kg) T2–T1: −1.4 ± 2.5 | measured difference (kg) T3–T2: −1.3 ± 4.8 T3–T1: −2.2 ± 3.8 reported variation during LD 55% ↔ 9% ↓ (diet) 18% ↑ (training) 18% other/missing | reported variation during LD 50% ↔ 25% ↓ (diet) 25% ↑ (LD) | reported variation during LD 45% ↔ 22% ↓ (diet) 22% ↑ (LD) 11% missing | |
| BM difference between measured and reported | 0.1 (0.0–4.7) | 0.0 (−0.5–0.3) | −0.8 (−2.5–0.8) | −0.2 (−5.1–0.9) | 1.2 (−0.3–4.1) |
| Self-Reported Data | DAM-T3 (n = 12) | NDAM-T3 (n = 12) | NDAW-T3 (n = 9) |
|---|---|---|---|
| Test-COVID LD | 18% negative | not tested | not tested |
| Fever LD | 18% | 8% | 11% |
| Cough LD | 9% | 17% | 22% |
| Fatigue LD | 9% | 0% | 22% |
| Reported pain: neck shoulders dorsal lumbar | LD–no before LD 27–0% 45–0% 18–0% 36–0% | LD–no before LD 25–0% 33–17% 33–8% 17–8% | LD–no before LD 44–0% 33–0% 11–0% 22–0% |
| Reported cause of pain | training 80% ↓ physiotherapy 20% | training 44% ↑ sedentary 22% | training 17% ↓ physiotherapy 17% |
| Exercise LD | ↓ 73%–↑ 18% | ↓ 92%–↑ 8% | ↓ 44%–↑ 22% |
| Sedentary LD | ↑ 73% | ↑ 83% | ↑ 33% |
| Eating LD | ↓ 36%–↑ 9% | ↓ 42%–↑ 25% | ↓ 11%–↑ 11% |
| Energy and Macronutrients | DAM-T1 (n = 16) | DAM-T2 (n = 12) | DAM-T3 (n = 12) | NDAM-T3 (n = 12) | NDAW-T3 (n = 9) |
|---|---|---|---|---|---|
| En (kcal/kg BM) | 32.9 ± 10.4 | 30.1 ± 6.1 | 29.4 ± 4.8 | 32.4 ± 8.8 | 26.8 ± 5.1 |
| CHO (g/kg) T1/T2: >5 g/kg T3: 3–5g/kg [31] Sugars (%En) 15 %En (LARN) Fiber (g/d) 25 g/d (LARN) for AMP/OHC and 15–30 g/d for SCI/SB [31] | 3.6 ± 1.2 | 3.4 ± 0.9 | 3.6 ± 0.7 | 4.5 ± 1.5 | 3.7 ± 0.9 |
| <87% | <92% | 0% * | >15% | >11% | |
| 15.2 ± 4.6 a | 10.2 ± 2.6 b | 10.5 ± 4.3 b | 8.6 ± 3.2 b | 10.4 ± 4.2 b | |
| >50% | 0% * | >11% | 0% | >22% | |
| 17 (14–22) a | 18 (14–24) a,b | 23 (21–25) b | 19 (16–21) a,b | 18 (13–20) a | |
| <69% (>12% SCI/SB) | <67% | <44% | <61% | <78% | |
| FAT (g/kg) Saturated fat (%En) 10 %En (LARN) | 1.3 ± 0.4 a | 1.1 ± 0.2 a,b | 1.0 ± 0.2 b | 1.0 ± 0.3 b | 0.9 ± 0.2 b |
| 11 (9–12) a | 10 (8–11) a | 12 (10–13) a,b | 13 (12–14) b | 14 (12–16) b | |
| >56% | >58% | >67% | >100% * | >100% * | |
| PRO-animal (g/kg) PRO-vegetable (g/kg) PRO-supplement use PRO (g/kg) range 1.2–1.7 g/kg BM [31] 0.9 g/kg BM (LARN) | 0.9 (0.7–1.1) a | 0.9 (0.9–1.0) a | 0.8 (0.7–0.9) a | 0.9 (0.7–1.1) a | 0.5 (0.4–0.6) b |
| 0.5 ± 0.2 | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.4 ± 0.2 | 0.4 ± 0.2 | |
| 37% | 67% * | 11% | 8% | 11% | |
| 1.5 (1.1–2.0) a | 1.5 (1.2_1.8) (a) | 1.3 (1.2_1.4) (a,b) | 1.3 (1.1_1.4) (a,b) | 1.0 (0.8_1.0) (b) | |
| <37%–>37% <12% | <33% _ > 42 % 0% | < 22 % _ > 11 % 0% | < 46 % _ > 15 % 0% | < 89 % _ > 11 % <44% * |
| Micronutrients | DAM-T1 (n = 16) | DAM-T2 (n = 12) | DAM-T3 (n = 12) | NDAM-T3 (n = 12) | NDAW-T3 (n = 9) |
|---|---|---|---|---|---|
| Vitamin B1 mg 1.2 (M) and 1.1 (W) LARN | 1.1 (0.8–1.8) | 1.0 (0.9–1.7) | 1.1 (1.0–1.2) | 1.0 (0.9–1.1) | 0.9 (0.8–1.2) |
| <50% | <58% | <92% | <20% | <67% | |
| Vitamin B2 mg 1.6 (M) and 1.3 (W) LARN | 1.6 (1.1–2.9) | 1.8 (1.4–2.4) | 1.7 (1.4–1.9) | 1.2 (1.1–1.4) | 1.1 (0.9–1.3) |
| <44% | <42% | <22% | <85% | <55% | |
| Vitamin B3 mg 18.0 LARN | 23.4 ± 5.1 a | 20.5 ± 4.8 a | 22.3 ± 3.7 a | 15.9 ± 3.9 b | 10.8 ± 4.1 c |
| <6% | <17% | <3% * | <15% | <13% | |
| Vitamin B6 mg 1.3 LARN | 2.4 ± 0.7 a | 2.4 ± 0.6 a | 2.4 ± 0.3 a | 1.7 ± 0.5 b | 1.3 ± 0.7 b |
| 0% | 0% | 0% | <15% | <67% * | |
| Vitamin B12 µg 2.4 LARN | 2.2 ± 0.4 a | 3.0 ± 0.5 b | 2.7 ± 0.1 c | 2.3 ± 0.1 a | 1.9 ± 0.3 a |
| <80% | 0% | 0% | <61% | <100% * | |
| Folic acid µg 400.0 LARN | 318.6 ± 133.2 a,b | 364.2 ± 128.1 a | 329.3 ± 77.5 a,b | 233.1 ± 92.2 b | 200.0 ± 89.3 b |
| <75% | <75% | <78% | <92% | <100% | |
| Vitamin C mg 105 (M) and 85 (W) LARN | 89.5 (71.7–154.3) | 94.8 (49.8–164.2) | 128.2 (76.4–133.3) | 78.9 (44.1–96.7) | 55.7 (48.5–73.1) |
| <62% | <50% | <44% | <93% | <89% | |
| Vitamin A (RE) µg 700 (M) and 600 (W) LARN | 664 (530–1266) | 812 (673–1437) | 826 (533–1211) | 722 (350–832) | 456 (326–693) |
| <56% | <25% | <44% | <46% | <67% | |
| Beta-caroteneµg | 2703 (1924–4021) | 3307 (1877–6936) | 3884 (2426–6343) | 3484 (1348–4482) | 2009 (1436–2844) |
| Vitamin E mg 13.0 (M) and 12.0 (W) LARN | 14.9 (13.1–17.5) a | 14.0 (12.7–16.3) a | 11.6 (9.2–14.6) a.b | 9.3 (7.6–11.0) b | 8.1 (5.0–10.5) b |
| <25% | <17% | <56% | <92% | <100% * | |
| Vitamin D µg 15.0 LARN | 1.9 (1.7–3.5) a | 1.7 (1.2–2.2) a | 6.5 (2.3–11.5) b | 2.1 (1.9–3.7) a,b | 2.2 (1.7–2.9) a,b |
| <100% | <100% | <100% | <100% | <100% | |
| Calcium g 1.00 LARN | 0.77 (0.46–10) | 0.61 (0.50–0.78) | 0.86 (0.84-0.95) | 0.85 (0. 73-0.98) | 0.74 (0.62-0.83) |
| <75% | <92% | <89% | <85% | <100% | |
| Phosphorus g 0.7 LARN | 1.35 (1.10–1.60) a | 1.30 (1.18–1.39) a | 1.25 (1.12–1.34) a,b | 0.91 (0.89–1.03) b | 0.75 (0.60–1.09) b |
| 0% | 0% | 0% | 0% | <44% * | |
| Sodium g in the range 1.5–2.0 LARN | 1.99 (0.98–2.48) | 1.39 (1.01–2.63) | 1.15 (0.79–1.95) | 1.04 (0.74–1.69) | 1.53 (1.09–1.63) |
| 12% | 17% | 11% | 23% | 44% | |
| Potassium g 3.9 LARN | 3.05 (2.73–4.01) a | 3.01 (2.51–3.63) a,b | 2.98 (2.26–3.32) a,b | 2.14 (1.80–2.57) b | 1.58 (1.12–2.95) b |
| <69% | <92% | <100% | <85% | <79% | |
| Iron mg 10.0 (M) and 18.0 (W) LARN HEME iron non-HEME iron | 11.2 (9.9–14.6) a | 11.0 (9.1–14.2) a | 11.9 (9.4–13.4) a | 8.0 (7.2–11.0) a,b | 5.9 (5.7–8.0) b |
| <25% | <33% | <33% | <69% | <100% | |
| 3.6 ± 1.3 a | 3.6 ± 1.1 a | 3.5 ±1.0 a | 3.6 ± 1.5 a | 1.7 ± 0.3 b | |
| 8.6 (6.8–10.5) a | 8.4 (6.1–10.8) a,b | 8.1 (6.1–11.0) a,b | 5.3 (4.2–6.5) b | 4.4 (3.1–7.4) b | |
| Zinc mg 12.0 (M) and 9.0 (W) LARN | 13.7 ± 3.7 a | 14.0 ± 2.6 a | 11.9 ± 2.3 a,b | 10.0 ± 3.4 b,c | 8.2 ± 3.1 c |
| <37% | <25% | <44% | <77% | <67% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toti, E.; Raguzzini, A.; Fedullo, A.L.; Cavedon, V.; Milanese, C.; Bernardi, M.; Mariani, B.M.; Massaro, L.; Mellara, F.; Sciarra, T.; et al. Longitudinal Effects of Dietary Advice on Wheelchair Basketball Athletes: Nutritional and Environmental Aspects. Sustainability 2021, 13, 5244. https://doi.org/10.3390/su13095244
Toti E, Raguzzini A, Fedullo AL, Cavedon V, Milanese C, Bernardi M, Mariani BM, Massaro L, Mellara F, Sciarra T, et al. Longitudinal Effects of Dietary Advice on Wheelchair Basketball Athletes: Nutritional and Environmental Aspects. Sustainability. 2021; 13(9):5244. https://doi.org/10.3390/su13095244
Chicago/Turabian StyleToti, Elisabetta, Anna Raguzzini, Anna Lucia Fedullo, Valentina Cavedon, Chiara Milanese, Marco Bernardi, Bianca Maria Mariani, Luca Massaro, Francesco Mellara, Tommaso Sciarra, and et al. 2021. "Longitudinal Effects of Dietary Advice on Wheelchair Basketball Athletes: Nutritional and Environmental Aspects" Sustainability 13, no. 9: 5244. https://doi.org/10.3390/su13095244