
The Effect of Systemic Parameters and Baseline Characteristics in Short-Term Response Analysis with Intravitreal Ranibizumab in Treatment-Naive Patients with Neovascular Age-Related Macular Degeneration

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Characteristics of the Study Group
2.2. Patient’s Criteria
2.3. Treatment Response Analysis
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Cohort Description
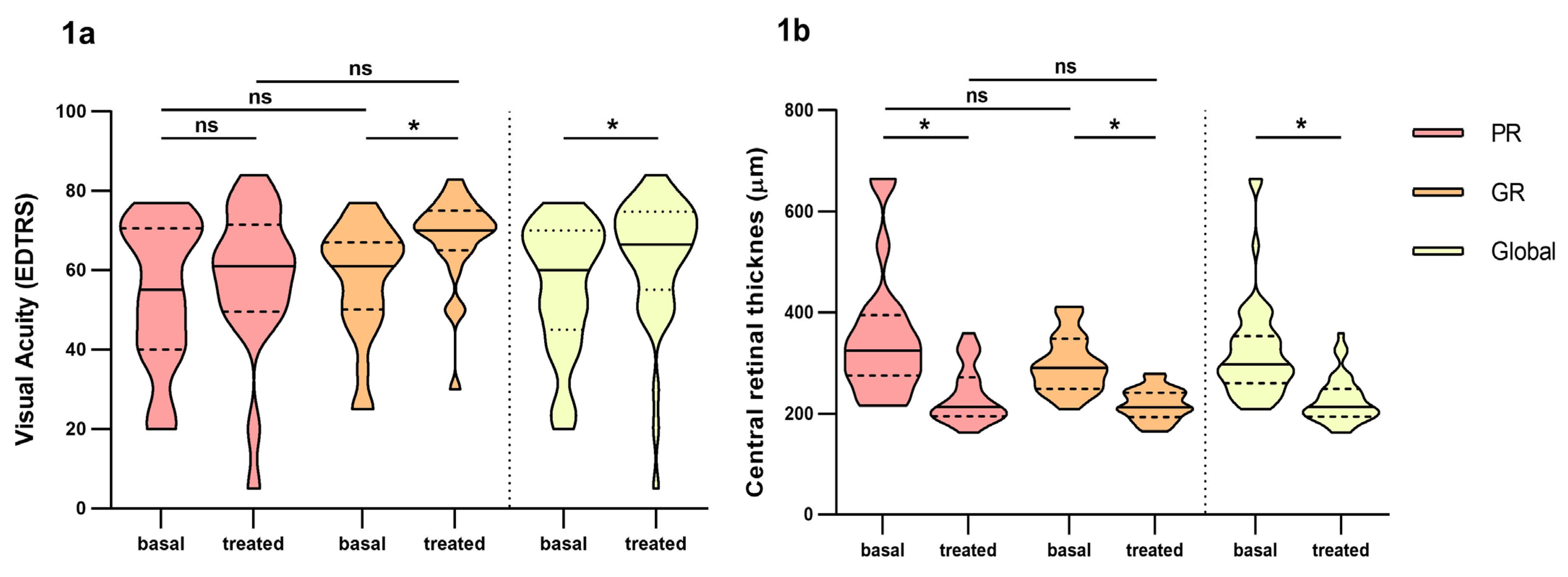
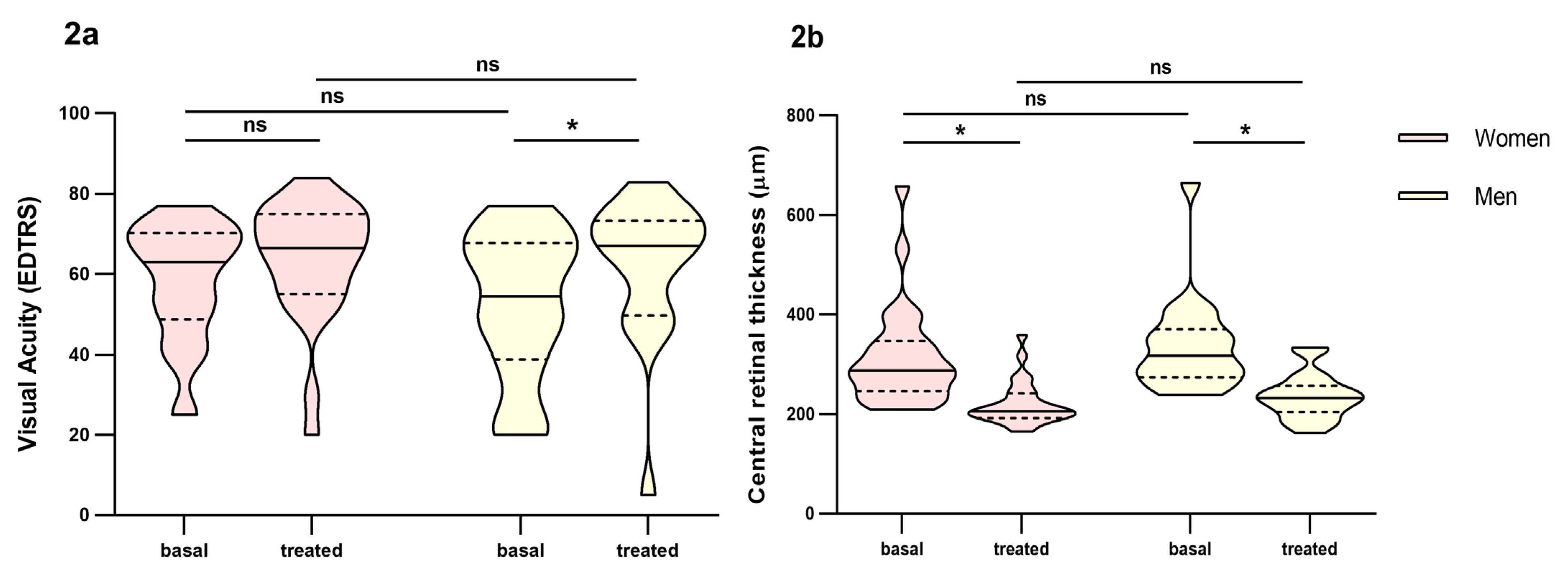
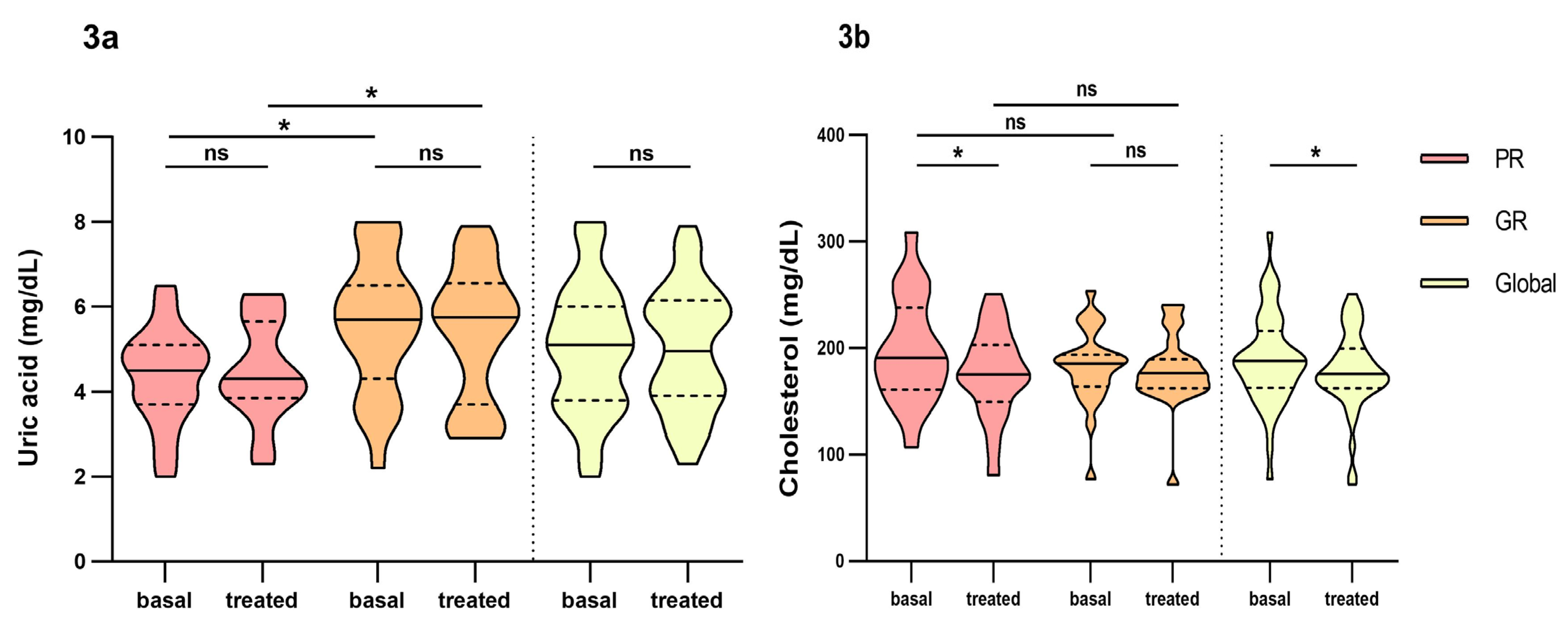
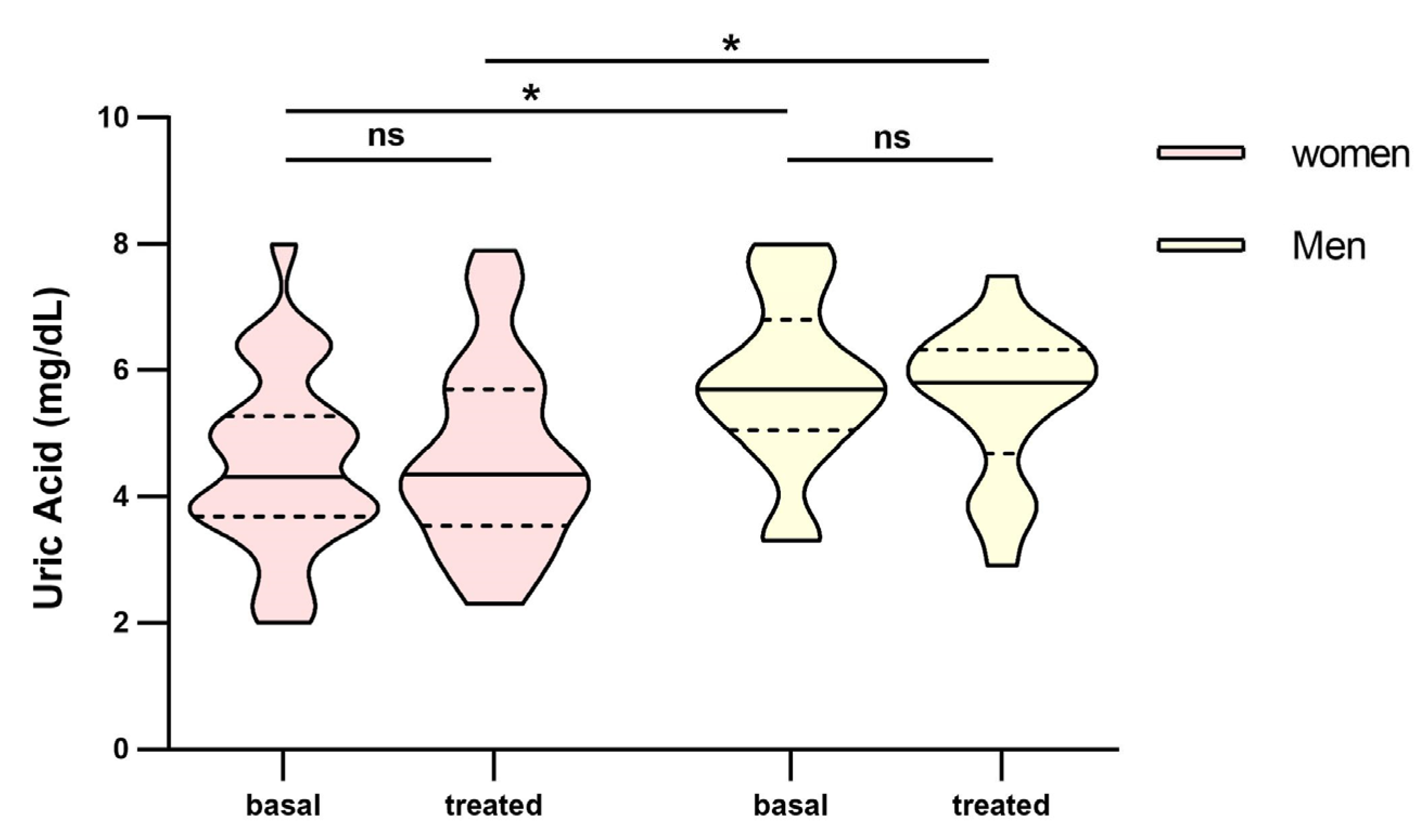
3.2. Biochemical and Inflammatory Parameter Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.-Y.; Wong, T.Y. Global Prevalence of Age-Related Macular Degeneration and Disease Burden Projection for 2020 and 2040: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [PubMed]
- Arrigo, A.; Saladino, A.; Aragona, E.; Mercuri, S.; Introini, U.; Bandello, F.; Parodi, M.B. Different Outcomes of Anti-VEGF Treatment for Neovascular AMD According to Neovascular Sutypes and Baseline Features: 2-Year Real-Life Clinical Outcomes. Biomed Res. Int. 2021, 2021, 5516981. [Google Scholar] [CrossRef] [PubMed]
- Joachim, N.; Mitchell, P.; Burlutsky, G.; Kifley, A.; Wang, J.J. The Incidence and Progression of Age-Related Macular Degeneration over 15 Years: The Blue Mountains Eye Study. Ophthalmology 2015, 122, 2482–2489. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.K.; Knudtson, M.D.; Meuer, S.M.; Swift, M.; Gangnon, R.E. Fifteen-Year Cumulative Incidence of Age-Related Macular Degeneration: The Beaver Dam Eye Study. Ophthalmology 2007, 114, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Maroñas, O.; García-Quintanilla, L.; Luaces-Rodríguez, A.; Fernández-Ferreiro, A.; Latorre-Pellicer, A.; Abraldes, M.J.; Lamas, M.J.; Carracedo, A. Anti-VEGF Treatment and Response in Age-Related Macular Degeneration: Disease’s Susceptibility, Pharmacogenetics and Pharmacokinetics. Curr. Med. Chem. 2020, 27, 549–569. [Google Scholar] [CrossRef]
- Seddon, J.M.; Cote, J.; Davis, N.; Rosner, B. Progression of Age-Related Macular Degeneration: Association with Body Mass Index, Waist Circumference, and Waist-Hip Ratio. Arch. Ophthalmol. 2003, 121, 785–792. [Google Scholar] [CrossRef]
- Klein, R.; Klein, B.E.K.; Tomany, S.C.; Cruickshanks, K.J. The Association of Cardiovascular Disease with the Long-Term Incidence of Age-Related Maculopathy: The Beaver Dam Eye Study. Ophthalmology 2003, 110, 1273–1280. [Google Scholar] [CrossRef]
- AREDS2 Research Group; Chew, E.Y.; Clemons, T.; SanGiovanni, J.P.; Danis, R.; Domalpally, A.; McBee, W.; Sperduto, R.; Ferris, F.L. The Age-Related Eye Disease Study 2 (AREDS2): Study Design and Baseline Characteristics (AREDS2 Report Number 1). Ophthalmology 2012, 119, 2282–2289. [Google Scholar] [CrossRef]
- Kananen, F.; Strandberg, T.; Loukovaara, S.; Immonen, I. Early Middle Age Cholesterol Levels and the Association with Age-Related Macular Degeneration. Acta Ophthalmol. 2021, 99, e1063–e1069. [Google Scholar] [CrossRef]
- Rozing, M.P.; Durhuus, J.A.; Krogh Nielsen, M.; Subhi, Y.; Kirkwood, T.B.; Westendorp, R.G.; Sørensen, T.L. Age-Related Macular Degeneration: A Two-Level Model Hypothesis. Prog. Retin. Eye Res. 2020, 76, 100825. [Google Scholar] [CrossRef]
- Kersten, E.; Paun, C.C.; Schellevis, R.L.; Hoyng, C.B.; Delcourt, C.; Lengyel, I.; Peto, T.; Ueffing, M.; Klaver, C.C.W.; Dammeier, S.; et al. Systemic and Ocular Fluid Compounds as Potential Biomarkers in Age-Related Macular Degeneration. Surv. Ophthalmol. 2018, 63, 9–39. [Google Scholar] [CrossRef] [PubMed]
- Bobadilla, M.; Pariente, A.; Oca, A.I.; Peláez, R.; Pérez-Sala, Á.; Larráyoz, I.M. Biomarkers as Predictive Factors of Anti-VEGF Response. Biomedicines 2022, 10, 1003. [Google Scholar] [CrossRef] [PubMed]
- Pugazhendhi, A.; Hubbell, M.; Jairam, P.; Ambati, B. Neovascular Macular Degeneration: A Review of Etiology, Risk Factors, and Recent Advances in Research and Therapy. Int. J. Mol. Sci. 2021, 22, 1170. [Google Scholar] [CrossRef] [PubMed]
- García-Quintanilla, L.; Rodríguez-Martínez, L.; Bandín-Vilar, E.; Gil-Martínez, M.; González-Barcia, M.; Mondelo-García, C.; Fernández-Ferreiro, A.; Mateos, J. Recent Advances in Proteomics-Based Approaches to Studying Age-Related Macular Degeneration: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 14759. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.N.; Patel, P.A.; Land, M.R.; Bakerkhatib-Taha, I.; Ahmed, H.; Sheth, V. Targeting the Complement Cascade for Treatment of Dry Age-Related Macular Degeneration. Biomedicines 2022, 10, 1884. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y.; MARINA Study Group. Ranibizumab for Neovascular Age-Related Macular Degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Michels, M.; Kaiser, P.K.; Heier, J.S.; Sy, J.P.; Ianchulev, T.; ANCHOR Study Group. Ranibizumab versus Verteporfin Photodynamic Therapy for Neovascular Age-Related Macular Degeneration: Two-Year Results of the ANCHOR Study. Ophthalmology 2009, 116, 57–65.e5. [Google Scholar] [CrossRef] [PubMed]
- Rofagha, S.; Bhisitkul, R.B.; Boyer, D.S.; Sadda, S.R.; Zhang, K. SEVEN-UP Study Group Seven-Year Outcomes in Ranibizumab-Treated Patients in ANCHOR, MARINA, and HORIZON: A Multicenter Cohort Study (SEVEN-UP). Ophthalmology 2013, 120, 2292–2299. [Google Scholar] [CrossRef]
- Bressler, N.M.; Chang, T.S.; Suñer, I.J.; Fine, J.T.; Dolan, C.M.; Ward, J.; Ianchulev, T.; MARINA and ANCHOR Research Groups. Vision-Related Function after Ranibizumab Treatment by Better- or Worse-Seeing Eye: Clinical Trial Results from MARINA and ANCHOR. Ophthalmology 2010, 117, 747–756.e4. [Google Scholar] [CrossRef]
- Chaudhary, V.; Matonti, F.; Zarranz-Ventura, J.; Stewart, M.W. Impact of Fluid Compartments on Functional Outcomes for Patients with Neovascular Age-Related Macular Degeneration: A Systematic Literature Review. Retina 2022, 42, 589–606. [Google Scholar] [CrossRef]
- Mauschitz, M.M.; Verzijden, T.; Schuster, A.K.; Elbaz, H.; Pfeiffer, N.; Khawaja, A.; Luben, R.N.; Foster, P.J.; Rauscher, F.G.; Wirkner, K.; et al. Association of Lipid-Lowering Drugs and Antidiabetic Drugs with Age-Related Macular Degeneration: A Meta-Analysis in Europeans. Br. J. Ophthalmol. 2022, 107, 1880–1886. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Jeon, H.L.; Park, S.J.; Shin, J.Y. Effect of Statins, Metformin, Angiotensin-Converting Enzyme Inhibitors, and Angiotensin II Receptor Blockers on Age-Related Macular Degeneration. Yonsei Med. J. 2019, 60, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, A.V.; Pineda, M.D.; Venkata, K.C.N. Comprehension of Top 200 Prescribed Drugs in the US as a Resource for Pharmacy Teaching, Training and Practice. Pharmacy 2018, 6, 43. [Google Scholar] [CrossRef]
- Moisseiev, E.; Tsai, Y.-L.; Herzenstein, M. Treatment of Neovascular Age-Related Macular Degeneration: An Economic Cost-Risk Analysis of Anti-Vascular Endothelial Growth Factor Agents. Ophthalmol. Retin. 2021, 6, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Amoaku, W.M.; Chakravarthy, U.; Gale, R.; Gavin, M.; Ghanchi, F.; Gibson, J.; Harding, S.; Johnston, R.L.; Kelly, S.P.; Lotery, A.; et al. Defining Response to Anti-VEGF Therapies in Neovascular AMD. Eye 2015, 29, 1397–1398. [Google Scholar] [CrossRef]
- Colijn, J.M.; Buitendijk, G.H.S.; Prokofyeva, E.; Alves, D.; Cachulo, M.L.; Khawaja, A.P.; Cougnard-Gregoire, A.; Merle, B.M.J.; Korb, C.; Erke, M.G.; et al. Prevalence of Age-Related Macular Degeneration in Europe: The Past and the Future. Ophthalmology 2017, 124, 1753–1763. [Google Scholar] [CrossRef] [PubMed]
- Westergaard, D.; Moseley, P.; Sørup, F.K.H.; Baldi, P.; Brunak, S. Population-Wide Analysis of Differences in Disease Progression Patterns in Men and Women. Nat. Commun. 2019, 10, 666. [Google Scholar] [CrossRef]
- Bek, T.; Klug, S.E. Age, Sex, and Type of Medication Predict the Effect of Anti-VEGF Treatment on Central Retinal Thickness in Wet Age-Related Macular Degeneration. Clin. Ophthalmol. 2018, 12, 473–479. [Google Scholar] [CrossRef]
- Ollila, T.; Silvennoinen, J.; Joshi, A.; Liu, J.; Kulathinal, S.; Immonen, I. Analysing Subgroups and Treatment Discontinuation in a Finnish Cohort of Patients with Neovascular AMD. Ophthalmologica 2022, 245, 358–367. [Google Scholar] [CrossRef]
- Tsai, C.-Y.; Wu, C.-L.; Cheng, C.-K.; Shen, Y.-D.; Wu, W.-C.; Wu, P.-C.; Tsai, A.; Chen, J.-T. Baseline Characteristics and Treatment Response Predictive of nAMD Outcomes with Ranibizumab Therapy in Treatment-Naive Patients: The RACER Subgroup Analysis. BMC Ophthalmol. 2023, 23, 39. [Google Scholar] [CrossRef]
- Montero, J.A.; Ruiz-Moreno, J.M.; Sanchis-Merino, E.; Perez-Martin, S. Systemic Beta-Blockers May Reduce the Need for Repeated Intravitreal Injections in Patients with Wet Age-Related Macular Degeneration Treated by Bevacizumab. Retina 2013, 33, 508–512. [Google Scholar] [CrossRef]
- Al-Janabi, A.; Lightman, S.; Tomkins-Netzer, O. Statins in Retinal Disease. Eye 2018, 32, 981–991. [Google Scholar] [CrossRef] [PubMed]
- Tian, B.; Al-Moujahed, A.; Bouzika, P.; Hu, Y.; Notomi, S.; Tsoka, P.; Miller, J.W.; Lin, H.; Vavvas, D.G. Atorvastatin Promotes Phagocytosis and Attenuates Pro-Inflammatory Response in Human Retinal Pigment Epithelial Cells. Sci. Rep. 2017, 7, 2329. [Google Scholar] [CrossRef] [PubMed]
- Medina, R.J.; O’Neill, C.L.; Devine, A.B.; Gardiner, T.A.; Stitt, A.W. The Pleiotropic Effects of Simvastatin on Retinal Microvascular Endothelium Has Important Implications for Ischaemic Retinopathies. PLoS ONE 2008, 3, e2584. [Google Scholar] [CrossRef] [PubMed]
- Manresa, N.; Mulero, J.; Losada, M.; Zafrilla, P. Influence of Anti-VEGF about Cardiovascular Biomarkers in Age Related Macular Degeneration. J. Nutr. Health Aging 2015, 19, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Erdem, B.; Gok, M. Evaluation of the Effects of Intravitreal Aflibercept and Ranibizumab on Systemic Inflammatory and Cardiovascular Biomarkers in Patients with Neovascular Age-Related Macular Degeneration. Curr. Eye Res. 2021, 46, 1387–1392. [Google Scholar] [CrossRef] [PubMed]
- Cougnard-Grégoire, A.; Delyfer, M.-N.; Korobelnik, J.-F.; Rougier, M.-B.; Le Goff, M.; Dartigues, J.-F.; Barberger-Gateau, P.; Delcourt, C. Elevated High-Density Lipoprotein Cholesterol and Age-Related Macular Degeneration: The Alienor Study. PLoS ONE 2014, 9, e90973. [Google Scholar] [CrossRef]
- Liu, Q.; Li, J.; Cheng, R.; Chen, Y.; Lee, K.; Hu, Y.; Yi, J.; Liu, Z.; Ma, J. Nitrosative Stress Plays an Important Role in Wnt Pathway Activation in Diabetic Retinopathy. Antioxid. Redox Signal. 2013, 18, 1141–1153. [Google Scholar] [CrossRef]
- Subramani, S.; Khor, S.E.; Livingstone, B.I.; Kulkarni, U.V. Serum Uric Acid Levels and Its Association with Age-Related Macular Degeneration (ARMD). Med. J. Malays. 2010, 65, 36–40. [Google Scholar]
- Pai, H.-L.; Hsieh, S.M.-T.; Su, Y.-S.; Sue, X.-Y.; Chang, H.-H.; Lin, D.P.-C. Short-Term Hyperuricemia Leads to Structural Retinal Changes That Can Be Reversed by Serum Uric Acid Lowering Agents in Mice. Investig. Ophthalmol. Vis. Sci. 2022, 63, 8. [Google Scholar] [CrossRef]
- Qin, Y.J.; Zhang, Y.L.; Zhang, Y.Q.; He, B.T.; Wang, S.; Yu, H.H.; Chan, S.O.; Zhang, H.Y. Elevated Level of Uric Acid, but Not Glucose, in Aqueous Humor as a Risk Factor for Diabetic Macular Edema in Patients with Type 2 Diabetes. Retina 2022, 42, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Horwath-Winter, J.; Kirchengast, S.; Meinitzer, A.; Wachswender, C.; Faschinger, C.; Schmut, O. Determination of Uric Acid Concentrations in Human Tear Fluid, Aqueous Humour and Serum. Acta Ophthalmol. 2009, 87, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Charchar, F.J. Establishment of Sex Difference in Circulating Uric Acid Is Associated with Higher Testosterone and Lower Sex Hormone-Binding Globulin in Adolescent Boys. Sci. Rep. 2021, 11, 17323. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.H.; Pierce, C.O.; De Salvo, G.; Griffiths, H.; Nelson, M.; Cree, A.J.; Menon, G.; Lotery, A.J. The Effect of Systemic Levels of TNF-Alpha and Complement Pathway Activity on Outcomes of VEGF Inhibition in Neovascular AMD. Eye 2022, 36, 2192–2199. [Google Scholar] [CrossRef]
- Wiciński, M.; Seredyka-Burduk, M.; Liberski, S.; Marczak, D.; Pol, M.; Malinowski, B.; Pawlak-Osińska, K.; Kaluzny, B.J. Evaluation of Blood Coagulation Parameters and ADMA, NO, IL-6, and IL-18 Serum Levels in Patients with Neovascular AMD before, during, and after the Initial Loading Phase of Intravitreal Aflibercept. Life 2021, 11, 441. [Google Scholar] [CrossRef]
- García-Quintanilla, L.; Luaces-Rodríguez, A.; Gil-Martínez, M.; Mondelo-García, C.; Maroñas, O.; Mangas-Sanjuan, V.; González-Barcia, M.; Zarra-Ferro, I.; Aguiar, P.; Otero-Espinar, F.J.; et al. Pharmacokinetics of Intravitreal Anti-VEGF Drugs in Age-Related Macular Degeneration. Pharmaceutics 2019, 11, 365. [Google Scholar] [CrossRef]
- Xu, L.; Lu, T.; Tuomi, L.; Jumbe, N.; Lu, J.; Eppler, S.; Kuebler, P.; Damico-Beyer, L.A.; Joshi, A. Pharmacokinetics of Ranibizumab in Patients with Neovascular Age-Related Macular Degeneration: A Population Approach. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1616–1624. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Count N (%) (Total N = 44) | Poor Responders (N = 20) | Good Responders (N = 24) | p-Value * |
|---|---|---|---|---|
| Women | 26, 59.1 | 16, 80.0 | 10, 41.7 | 0.014 |
| Age; Median, IQR | 80, (74–86) | 80, (74–86) | 79, (75–86) | 0.850 |
| Co-morbidities | ||||
| Obesity (>30 kg/m2) | 17, 38.6 | 6, 30.0 | 11, 45.8 | 0.302 |
| Smoker | 14, 31.8 | 7, 35.0 | 7, 29.2 | 0.752 |
| Smoking status Non-smoker smoker Ex-smoker | 30, 68.2 3, 6.8 11, 25.0 | 13, 65.0 3, 15.0 4, 20.0 | 17, 70.8 0, 0.0 7, 29.2 | 0.134 |
| Cardiovascular | 30, 68.2 | 14, 70.0 | 16, 66.7 | 1.000 |
| Endocrine | 24, 54.5 | 14, 70.0 | 10, 41.7 | 0.076 |
| Concomitant medication | ||||
| Anti-inflammatories | 13, 29.5 | 7, 35.0 | 6, 25.0 | 0.522 |
| Anticoagulants | 9, 20.5 | 3, 15.0 | 6, 25.0 | 0.477 |
| Statins | 21, 47.7 | 13, 65.0 | 8, 33.0 | 0.068 |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| Variable | N | OR (IC95%) | p-Value | OR (IC95%) | p-Value |
| Age | 44 | 1.051 (0.971–1.137) | 0.218 | ||
| women | 44 | 0.179 (0.046–0.698) | 0.013 | 0.153, (0.026–0.901) | 0.038 |
| Body Mass Index | 44 | 1.039 (0.901–1.176) | 0.669 | ||
| Smoker | 44 | 0.765 (0.214–2.730) | 0.679 | ||
| Statins | 44 | 0.269 (0.077–0.940) | 0.040 | 0.159, (0.032–0.794) | 0.025 |
| Uric Acid basal | 43 | 1.894, (1.142–3.142) | 0.013 | 1.595, (0.906–2.807) | 0.105 |
| Creatinine basal | 43 | 42.387, (1.543–1164.734) | 0.027 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Quintanilla, L.; Almuiña-Varela, P.; Rodríguez-Cid, M.J.; Gil-Martínez, M.; Abraldes, M.J.; Gómez-Ulla, F.; González-Barcia, M.; Mondelo-García, C.; Estany-Gestal, A.; Otero-Espinar, F.J.; et al. The Effect of Systemic Parameters and Baseline Characteristics in Short-Term Response Analysis with Intravitreal Ranibizumab in Treatment-Naive Patients with Neovascular Age-Related Macular Degeneration. Pharmaceutics 2024, 16, 105. https://doi.org/10.3390/pharmaceutics16010105
García-Quintanilla L, Almuiña-Varela P, Rodríguez-Cid MJ, Gil-Martínez M, Abraldes MJ, Gómez-Ulla F, González-Barcia M, Mondelo-García C, Estany-Gestal A, Otero-Espinar FJ, et al. The Effect of Systemic Parameters and Baseline Characteristics in Short-Term Response Analysis with Intravitreal Ranibizumab in Treatment-Naive Patients with Neovascular Age-Related Macular Degeneration. Pharmaceutics. 2024; 16(1):105. https://doi.org/10.3390/pharmaceutics16010105
Chicago/Turabian StyleGarcía-Quintanilla, Laura, Pablo Almuiña-Varela, María José Rodríguez-Cid, María Gil-Martínez, Maximino J. Abraldes, Francisco Gómez-Ulla, Miguel González-Barcia, Cristina Mondelo-García, Ana Estany-Gestal, Francisco J. Otero-Espinar, and et al. 2024. "The Effect of Systemic Parameters and Baseline Characteristics in Short-Term Response Analysis with Intravitreal Ranibizumab in Treatment-Naive Patients with Neovascular Age-Related Macular Degeneration" Pharmaceutics 16, no. 1: 105. https://doi.org/10.3390/pharmaceutics16010105