
Effect of Different Downward Loads on Canal Centering Ability, Vertical Force, and Torque Generation during Nickel–Titanium Rotary Instrumentation


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Estimation
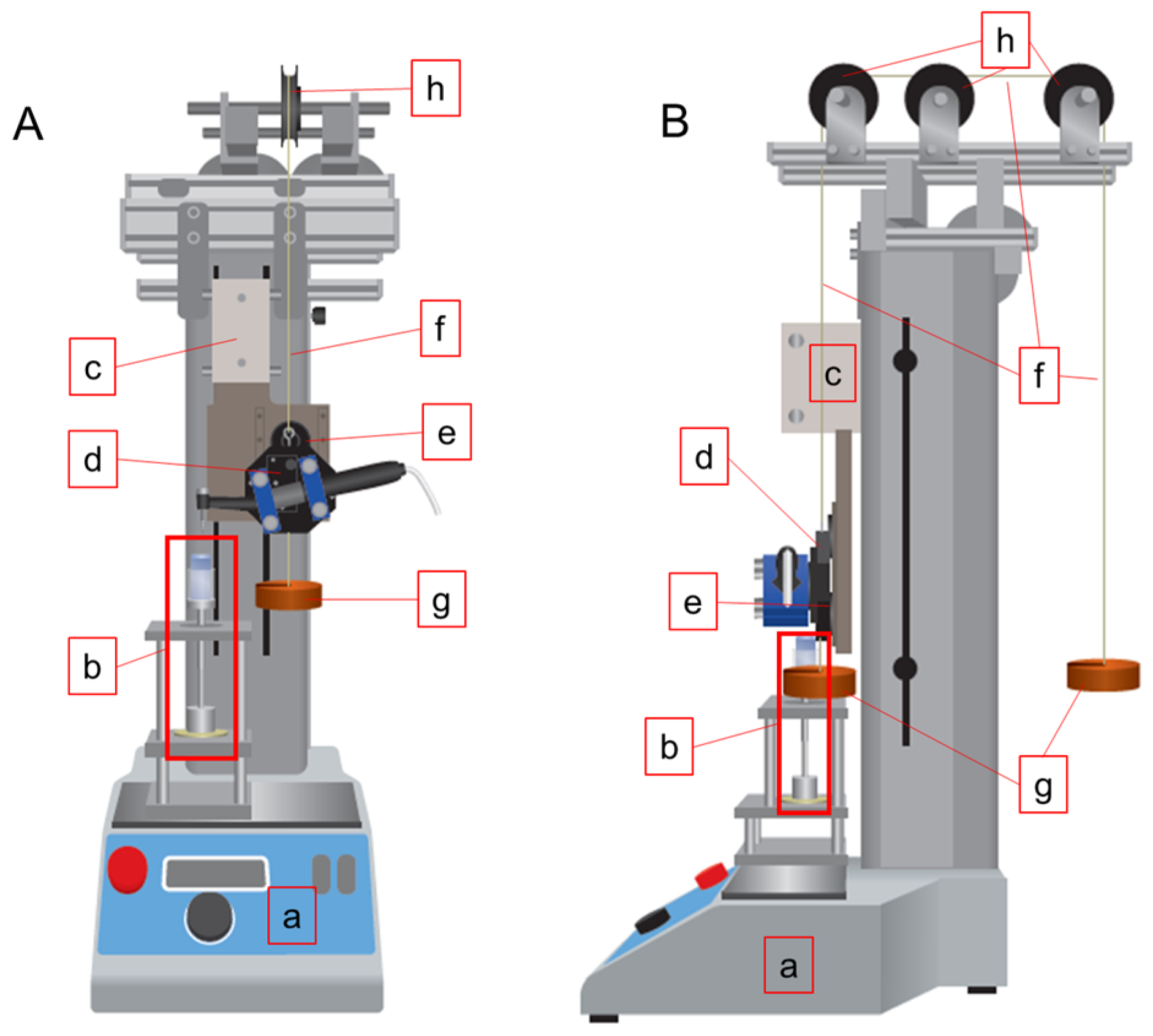
2.2. Downward Load-Controlled Root Canal Instrumentation and Torque/Force Measurement
2.3. Root Canal Instrumentation
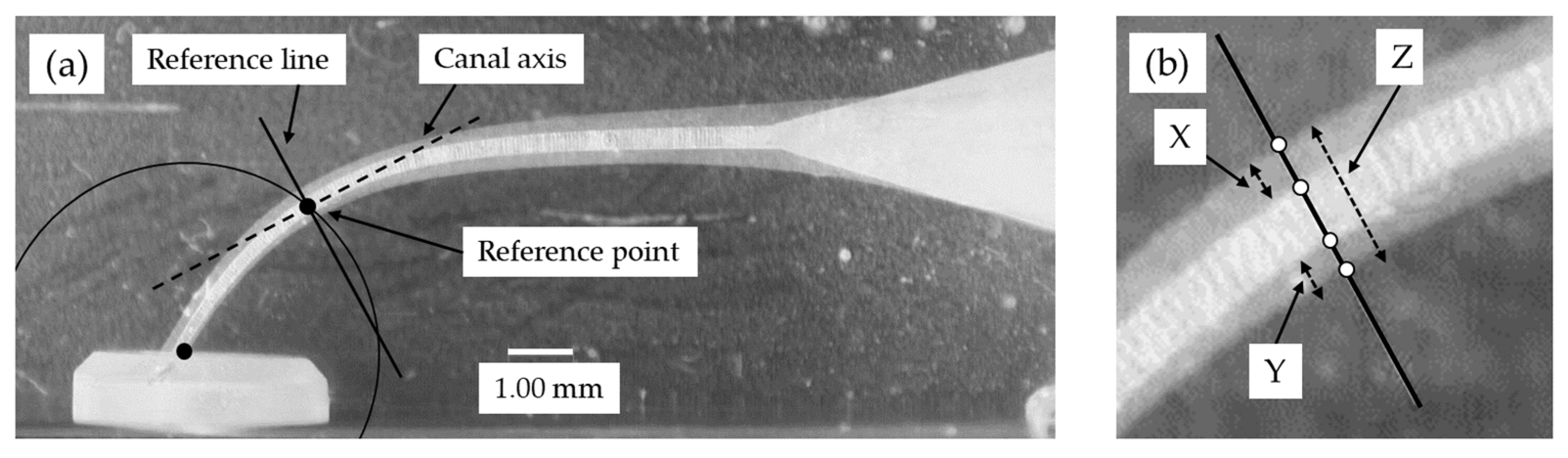
2.4. Evaluation of the Canal Centering Ratio and Instrumentation Time
- X = amount of material removed from the outer wall
- Y = amount of material removed from the inner wall
- Z = post-operative diameter of the canal.
2.5. Statistical Analysis
3. Results
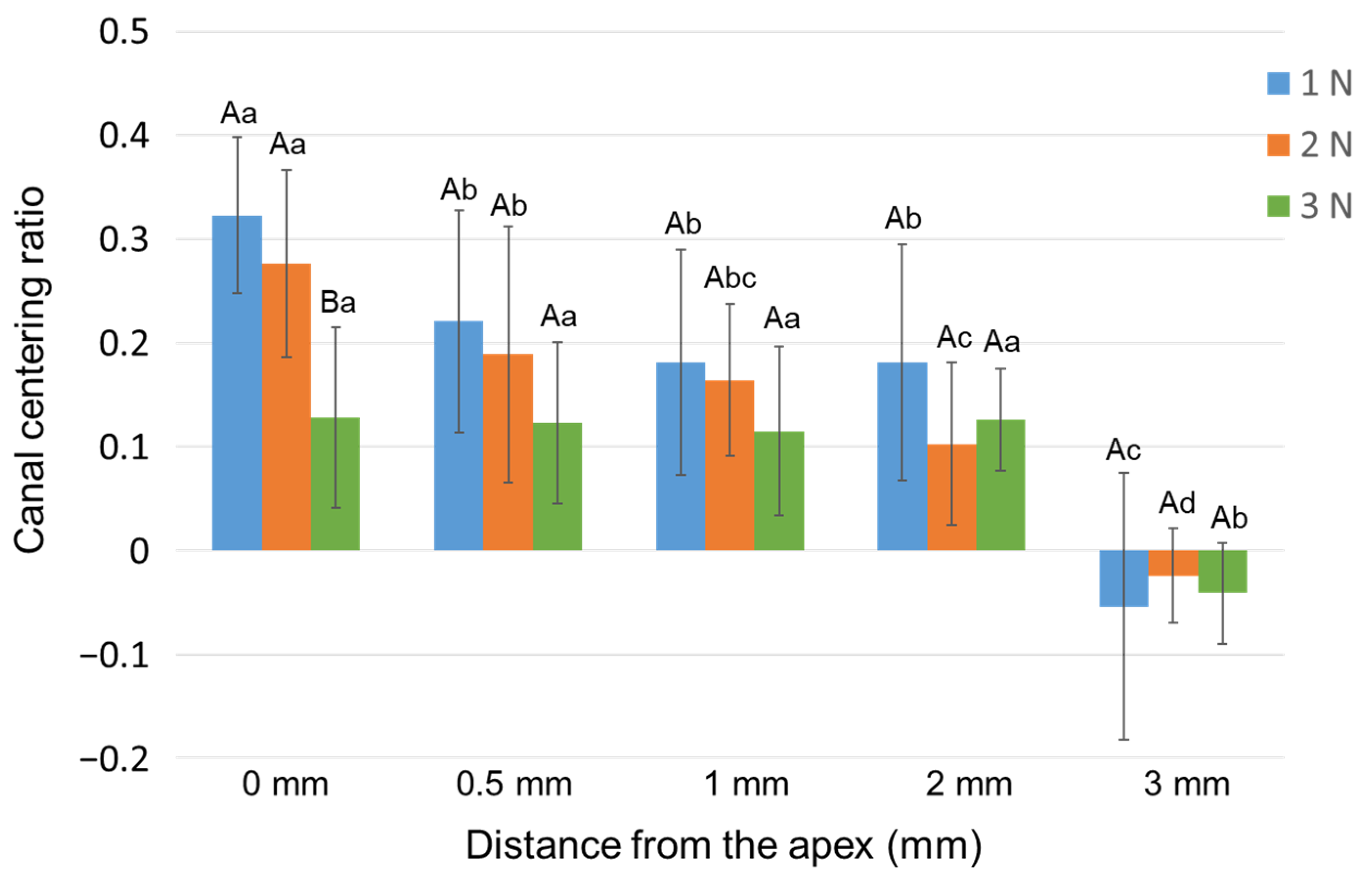
3.1. Canal Centering Ratio
3.2. Vertical Force and Clockwise Torque
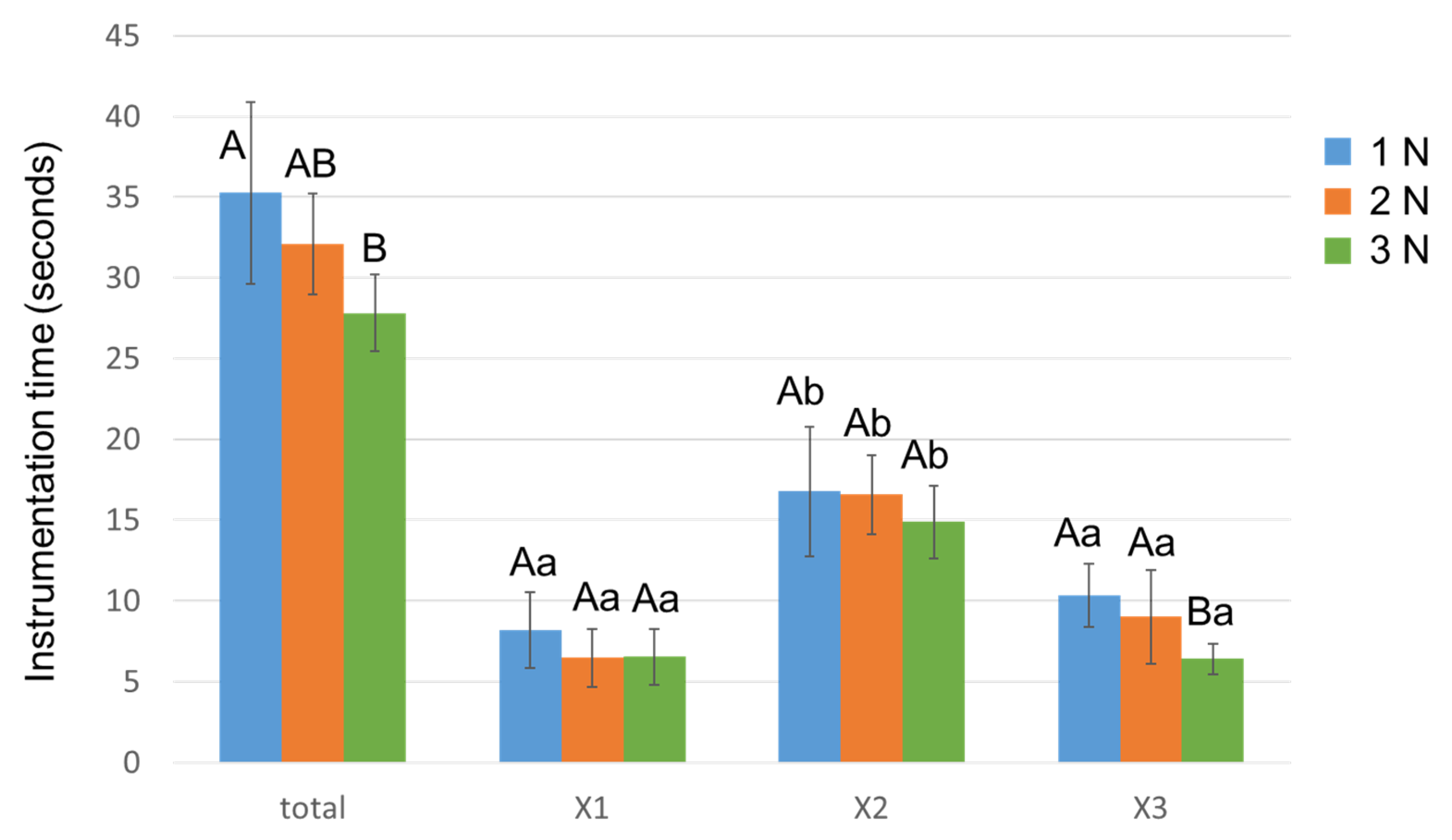
3.3. Instrumentation Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Metzger, Z.; Solomonov, M.; Kfir, A. The role of mechanical instrumentation in the cleaning of root canals. Endod. Top. 2013, 29, 87–109. [Google Scholar] [CrossRef]
- Gorni, F.G.; Gagliani, M.M. The outcome of endodontic retreatment: A 2-yr follow-up. J. Endod. 2004, 30, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Chevigny, C.; Dao, T.T.; Basrani, B.R.; Marquis, V.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment outcome in endodontics: The Toronto study–phase 4: Initial treatment. J. Endod. 2008, 34, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Ebihara, A.; Yahata, Y.; Miyara, K.; Nakano, K.; Hayashi, Y.; Suda, H. Heat treatment of nickel-titanium rotary endodontic instruments: Effects on bending properties and shaping abilities. Int. Endod. J. 2011, 44, 843–849. [Google Scholar] [CrossRef]
- Paleker, F.; van der Vyver, P.J. Comparison of canal transportation and centering ability of K-files, ProGlider File, and G-Files: A micro-computed tomography study of curved root canals. J. Endod. 2016, 42, 1105–1109. [Google Scholar] [CrossRef] [Green Version]
- Cheung, G.S.; Liu, C.S. A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. J. Endod. 2009, 35, 938–943. [Google Scholar] [CrossRef]
- Tokita, D.; Ebihara, A.; Miyara, K.; Okiji, T. Dynamic torsional and cyclic fracture behavior of ProFile rotary instruments at continuous or reciprocating rotation as visualized with high-speed digital video imaging. J. Endod. 2017, 43, 1337–1342. [Google Scholar] [CrossRef]
- McGuigan, M.B.; Louca, C.; Duncan, H.F. Endodontic instrument fracture: Causes and prevention. Br. Dent. J. 2013, 214, 341–348. [Google Scholar] [CrossRef]
- Ha, J.H.; Kwak, S.W.; Sigurdsson, A.; Cheng, S.W.; Kim, S.K.; Kim, H.C. Stress generation during pecking motion of rotary nickel-titanium instruments with different pecking depth. J. Endod. 2017, 43, 1688–1691. [Google Scholar] [CrossRef]
- Ahn, S.Y.; Kim, H.C.; Kim, E. Kinematic effects of nickel-titanium instruments with reciprocating or continuous rotation motion: A systematic review of in vitro studies. J. Endod. 2016, 42, 1009–1017. [Google Scholar] [CrossRef]
- Bardsley, S.; Peters, C.I.; Peters, O.A. The effect of three rotational speed settings on torque and apical force with vortex rotary instruments in vitro. J. Endod. 2011, 37, 860–864. [Google Scholar] [CrossRef] [PubMed]
- Kyaw, M.S.; Ebihara, A.; Kasuga, Y.; Maki, K.; Kimura, S.; Htun, P.H.; Nakatsukasa, T.; Okiji, T. Influence of rotational speed on torque/force generation and shaping ability during root canal instrumentation with continuous rotation and optimum torque reverse motion. Int. Endod. J. 2021, 54, 1614–1622. [Google Scholar] [CrossRef] [PubMed]
- Maki, K.; Ebihara, A.; Kimura, S.; Nishijo, M.; Tokita, D.; Okiji, T. Effect of different speeds of up-and-down motion on canal centering ability and vertical force and torque generation of nickel-titanium rotary instruments. J. Endod. 2019, 45, 68–72.e1. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.W.; Shen, Y.; Liu, H.; Kim, H.C.; Haapasalo, M. Torque generation of the endodontic instruments: A narrative review. Materials 2022, 15, 664. [Google Scholar] [CrossRef]
- Tokita, D.; Ebihara, A.; Nishijo, M.; Miyara, K.; Okiji, T. Dynamic torque and vertical force analysis during nickel-titanium rotary root canal preparation with different modes of reciprocal rotation. J. Endod. 2017, 43, 1706–1710. [Google Scholar] [CrossRef]
- Maki, K.; Ebihara, A.; Kimura, S.; Nishijo, M.; Tokita, D.; Miyara, K.; Okiji, T. Enhanced root canal-centering ability and reduced screw-in force generation of reciprocating nickel-titanium instruments with a post-machining thermal treatment. Dent. Mater. J. 2020, 39, 251–255. [Google Scholar] [CrossRef] [Green Version]
- Thu, M.; Ebihara, A.; Adel, S.; Okiji, T. Analysis of torque and force induced by rotary nickel-titanium instruments during root canal preparation: A systematic review. Appl. Sci. 2021, 11, 3079. [Google Scholar] [CrossRef]
- Nakatsukasa, T.; Ebihara, A.; Kimura, S.; Maki, K.; Nishijo, M.; Tokita, D.; Okiji, T. Comparative evaluation of mechanical properties and shaping performance of heat-treated nickel titanium rotary instruments used in the single-length technique. Dent. Mater. J. 2021, 40, 743–749. [Google Scholar] [CrossRef]
- Ha, J.H.; Cheung, G.S.; Versluis, A.; Lee, C.J.; Kwak, S.W.; Kim, H.C. ‘Screw-in’ tendency of rotary nickel-titanium files due to design geometry. Int. Endod. J. 2015, 48, 666–672. [Google Scholar] [CrossRef]
- Peters, O.A.; Barbakow, F. Dynamic torque and apical forces of ProFile. 04 rotary instruments during preparation of curved canals. Int. Endod J. 2002, 35, 379–389. [Google Scholar] [CrossRef]
- Diop, A.; Maurel, N.; Oiknine, M.; Patoor, E.; Machtou, P. A novel platform for in vitro analysis of torque, forces, and three-dimensional file displacements during root canal preparations: Application to ProTaper rotary files. J. Endod. 2009, 35, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Calberson, F.L.; Deroose, C.A.; Hommez, G.M.; de Moor, R.J.G. Shaping ability of ProTaper nickel-titanium files in simulated resin root canals. Int. Endod. J. 2004, 37, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Luo, H.X.; Zhou, X.D.; Tan, H.; Huang, D.M. The shaping effect of the combination of two rotary nickel-titanium instruments in simulated S-shaped canals. J. Endod. 2008, 34, 456–458. [Google Scholar] [CrossRef] [PubMed]
- Ba-Hattab, R.; Prohl, A.K.; Lang, H.; Pahncke, D. Comparison of the shaping ability of GT® Series X, Twisted Files and AlphaKite rotary nickel-titanium systems in simulated canals. BMC Oral Health 2013, 13, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, K.C.; Webber, J. The validity of simulated root canals for the investigation of the prepared root canal shape. Int. Endod. J. 1985, 18, 240–246. [Google Scholar] [CrossRef]
- De-Deus, G.; Simões-Carvalho, M.; Belladonna, F.G.; Versiani, M.A.; Silva, E.J.N.L.; Cavalcante, D.M.; Souza, E.M.; Johnsen, G.F.; Haugen, H.J.; Paciornik, S. Creation of well-balanced experimental groups for comparative endodontic laboratory studies: A new proposal based on micro-CT and in silico methods. Int. Endod. J. 2020, 53, 974–985. [Google Scholar] [CrossRef]
- Elnaghy, A.M. Cyclic fatigue resistance of ProTaper Next nickel-titanium rotary files. Int. Endod. J. 2014, 47, 1034–1039. [Google Scholar] [CrossRef]
- Velozo, C.; Silva, S.; Almeida, A.; Romeiro, K.; Vieira, B.; Dantas, H.; Sousa, F.; de Albuquerque, D.S. Shaping ability of XP-endo Shaper and ProTaper Next in long oval-shaped canals: A micro-computed tomography study. Int. Endod. J. 2020, 53, 998–1006. [Google Scholar] [CrossRef]
- Pereira, E.S.J.; Gomes, R.O.; Leroy, A.M.; Singh, R.; Peters, O.A.; Bahia, M.G.A.; Buono, V.T. Mechanical behavior of M-Wire and conventional NiTi wire used to manufacture rotary endodontic instruments. Dent. Mater. 2013, 29, e318–e324. [Google Scholar] [CrossRef]
- Jamleh, A.; Alfouzan, K. Vertical load induced with Twisted File Adaptive System during canal shaping. J. Endod. 2016, 42, 1811–1814. [Google Scholar] [CrossRef]
- De Cristofaro Almeida, G.; Aun, D.P.; Resende, P.D.; Peixoto, I.F.D.C.; Viana, A.C.D.; Buono, V.T.L.; de Azevedo Bahia, M.G. Comparative analysis of torque and apical force to assess the cutting behaviour of ProTaper Next and ProTaper Universal endodontic instruments. Aust. Endod. J. 2020, 46, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kwak, S.W.; Ha, J.H.; Kim, H.C. Ex-Vivo comparison of torsional stress on nickel–titanium instruments activated by continuous rotation or adaptive motion. Materials 2020, 13, 1900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zupanc, J.; Vahdat-Pajouh, N.; Schäfer, E. New thermomechanically treated NiTi alloys—A review. Int. Endod. J. 2018, 51, 1088–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishijo, M.; Ebihara, A.; Tokita, D.; Doi, H.; Hanawa, T.; Okiji, T. Evaluation of selected mechanical properties of NiTi rotary glide path files manufactured from controlled memory wires. Dent. Mater. J. 2018, 37, 549–554. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maki, K.; Ebihara, A.; Unno, H.; Omori, S.; Nakatsukasa, T.; Kimura, S.; Okiji, T. Effect of Different Downward Loads on Canal Centering Ability, Vertical Force, and Torque Generation during Nickel–Titanium Rotary Instrumentation. Materials 2022, 15, 2724. https://doi.org/10.3390/ma15082724
Maki K, Ebihara A, Unno H, Omori S, Nakatsukasa T, Kimura S, Okiji T. Effect of Different Downward Loads on Canal Centering Ability, Vertical Force, and Torque Generation during Nickel–Titanium Rotary Instrumentation. Materials. 2022; 15(8):2724. https://doi.org/10.3390/ma15082724
Chicago/Turabian StyleMaki, Keiichiro, Arata Ebihara, Hayate Unno, Satoshi Omori, Taro Nakatsukasa, Shunsuke Kimura, and Takashi Okiji. 2022. "Effect of Different Downward Loads on Canal Centering Ability, Vertical Force, and Torque Generation during Nickel–Titanium Rotary Instrumentation" Materials 15, no. 8: 2724. https://doi.org/10.3390/ma15082724