Properties of Experimental Dental Composites Containing Antibacterial Silver-Releasing Filler

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials Preparation
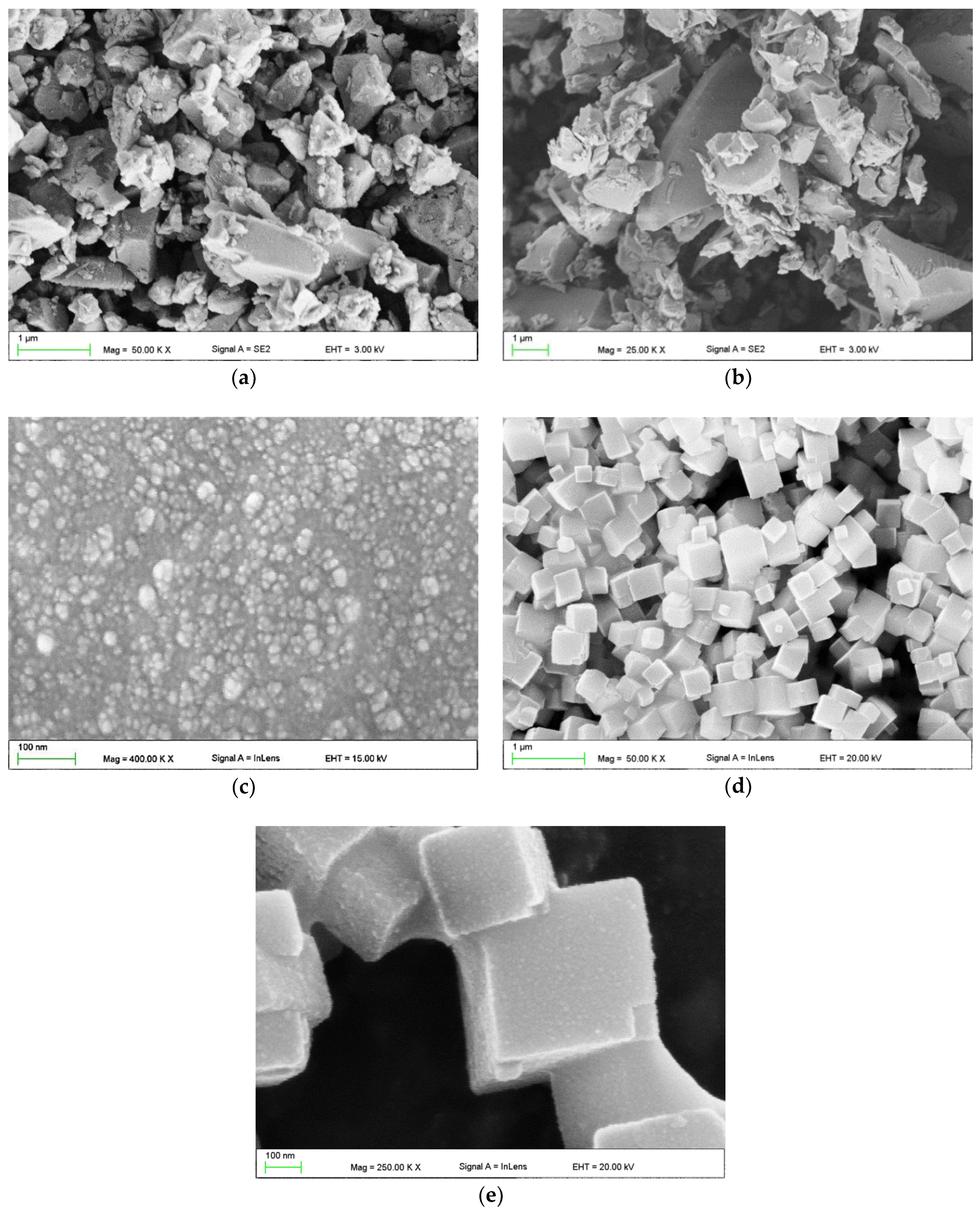
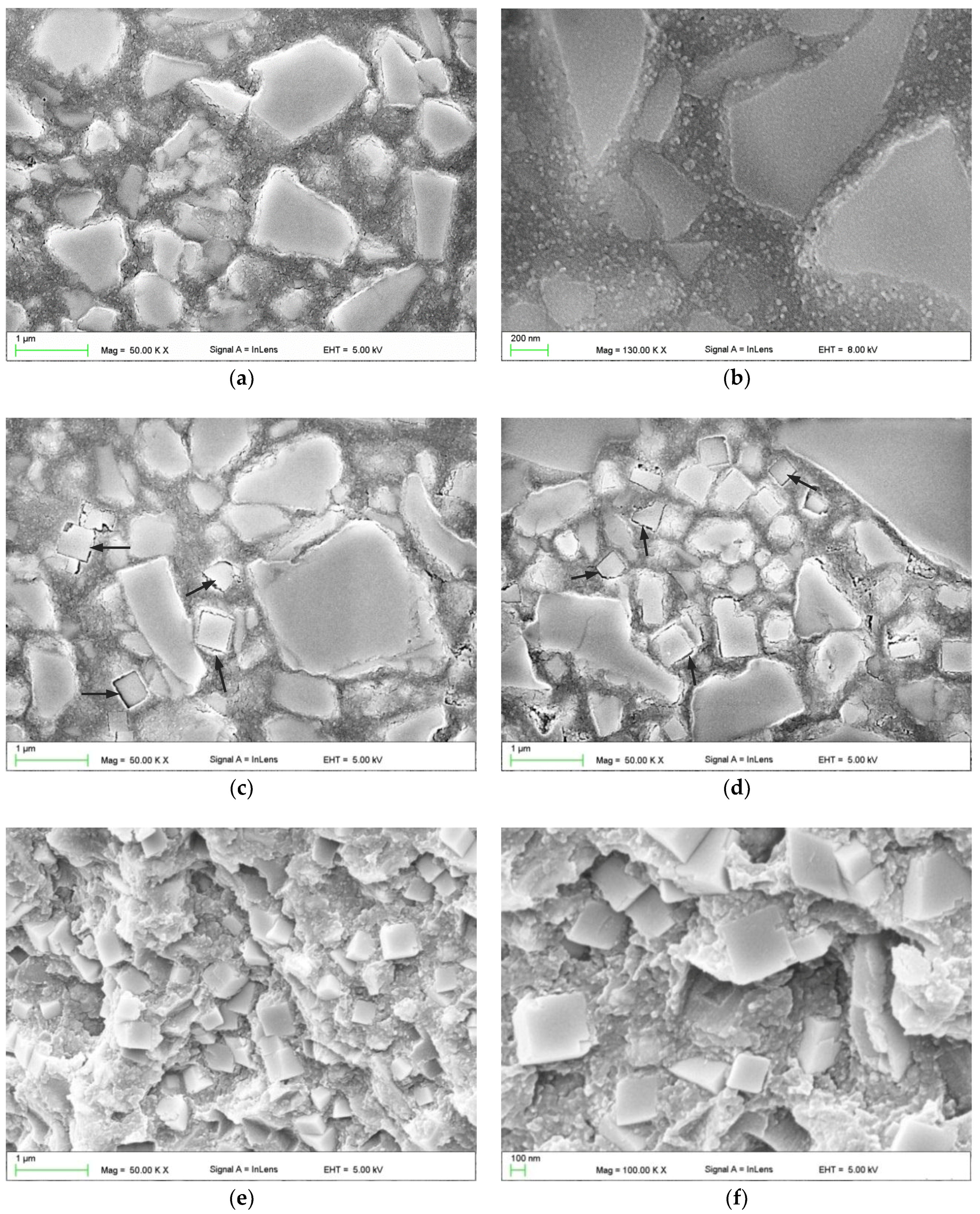
2.2. Scanning Electron Microscopy (SEM) Investigations
2.3. Antibacterial Test
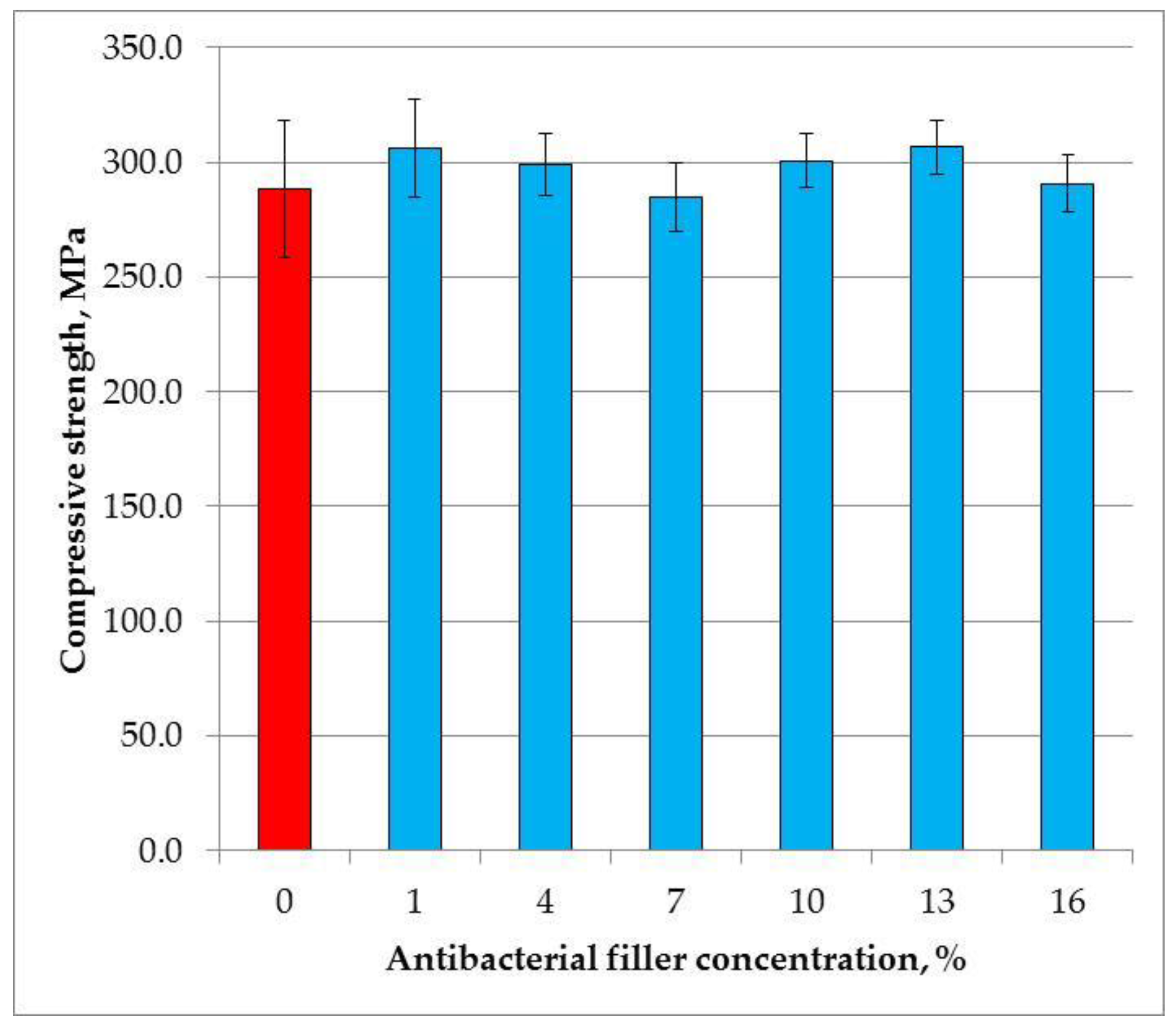
2.4. Compressive Strength
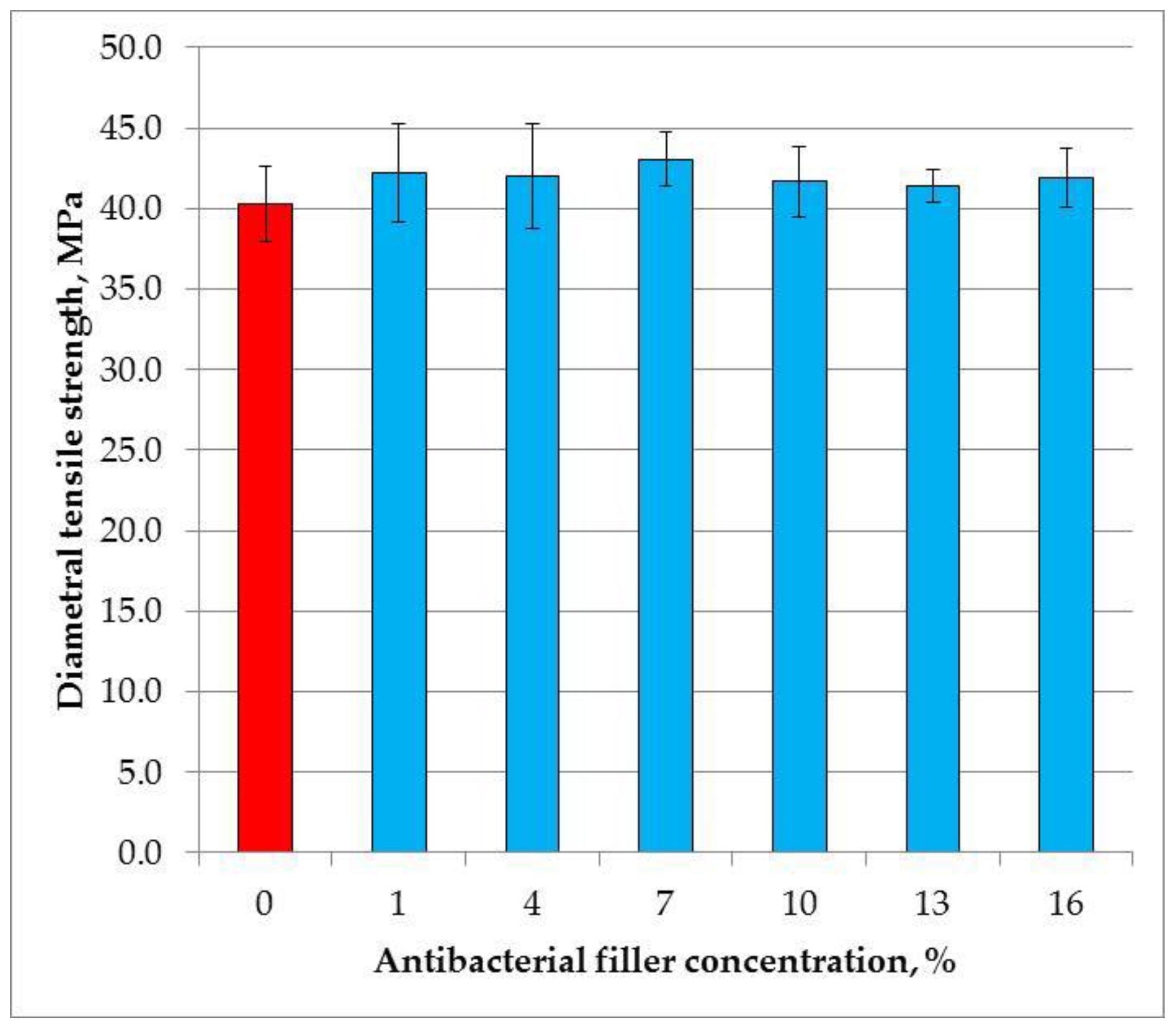
2.5. Diametral Tensile Strength
2.6. Flexural Strength
2.7. Vickers Hardness
2.8. Degree of Conversion
2.9. Sorption and Solubility
2.10. Color Change Measurement
2.11. Statistical Analysis
3. Results
3.1. Scanning Electron Microscopy Investigations
3.2. Antibacterial Test
3.3. Compressive Strength
3.4. Diametral Tensile Strength
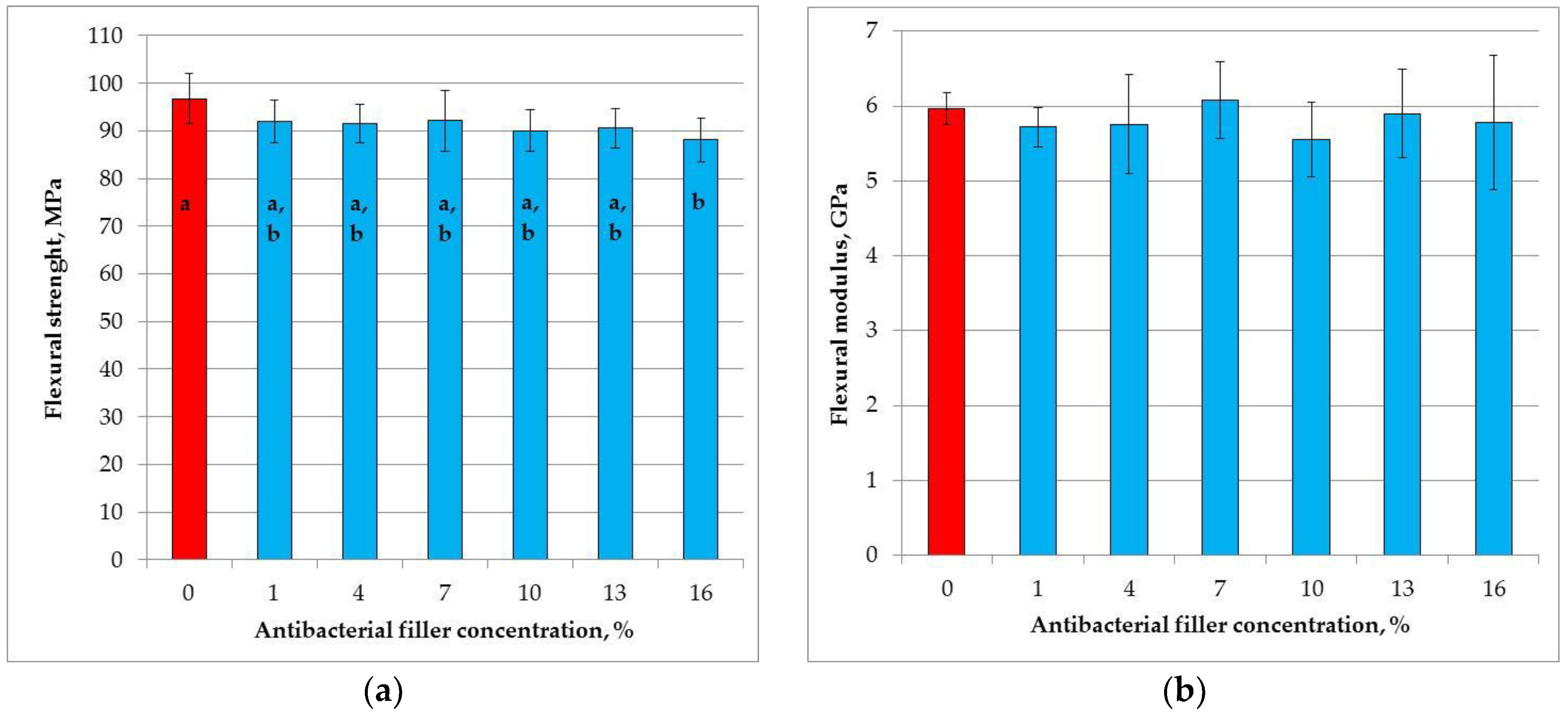
3.5. Flexural Strength
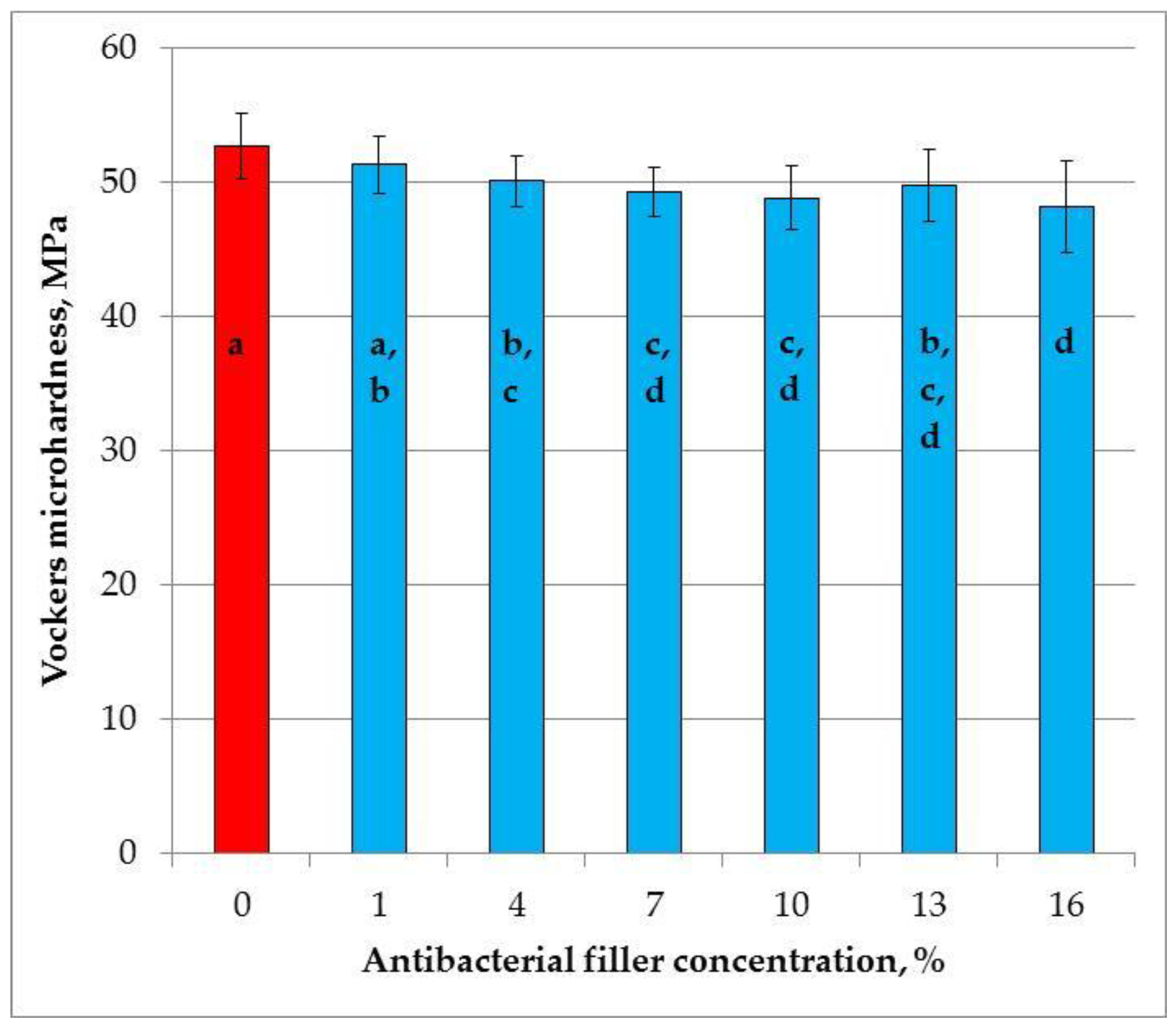
3.6. Vickers Hardness
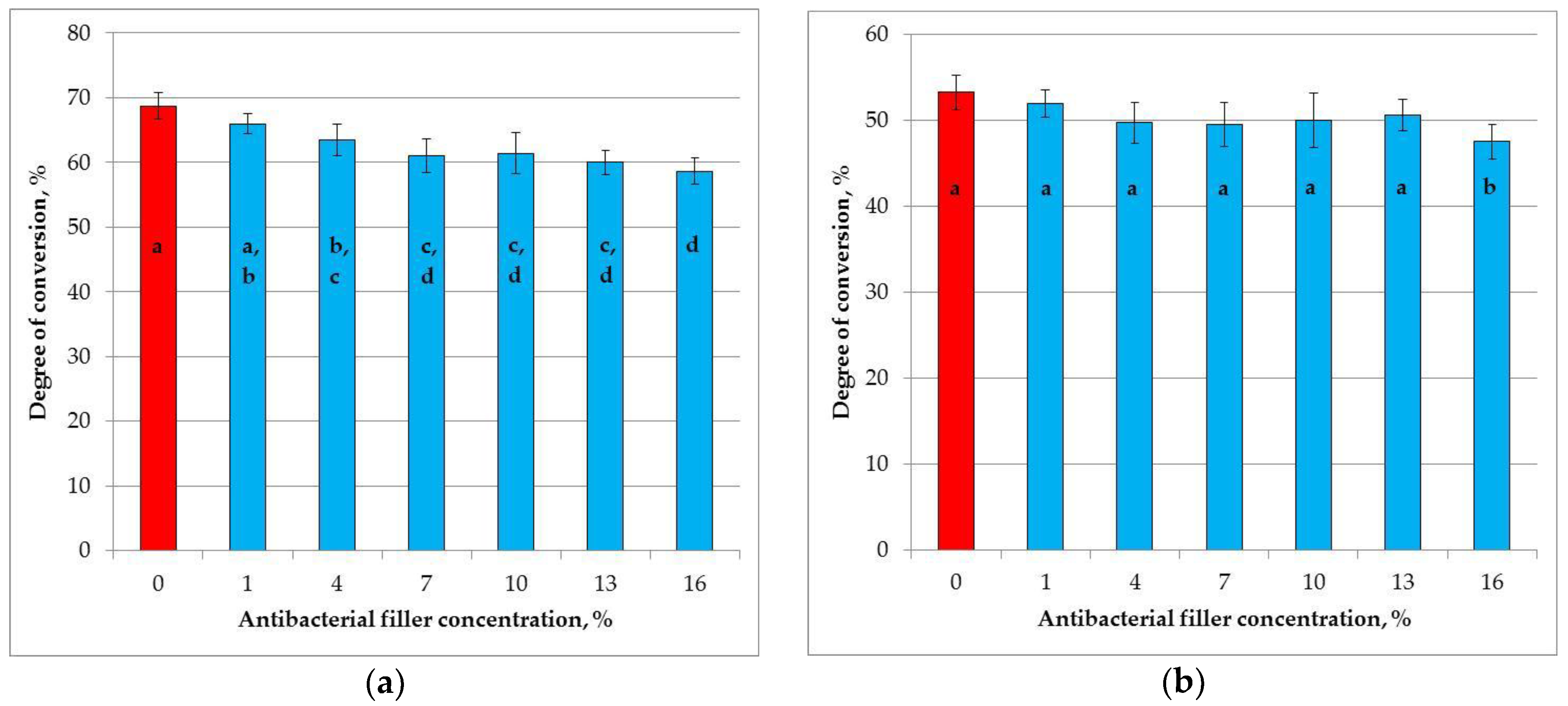
3.7. Degree of Conversion
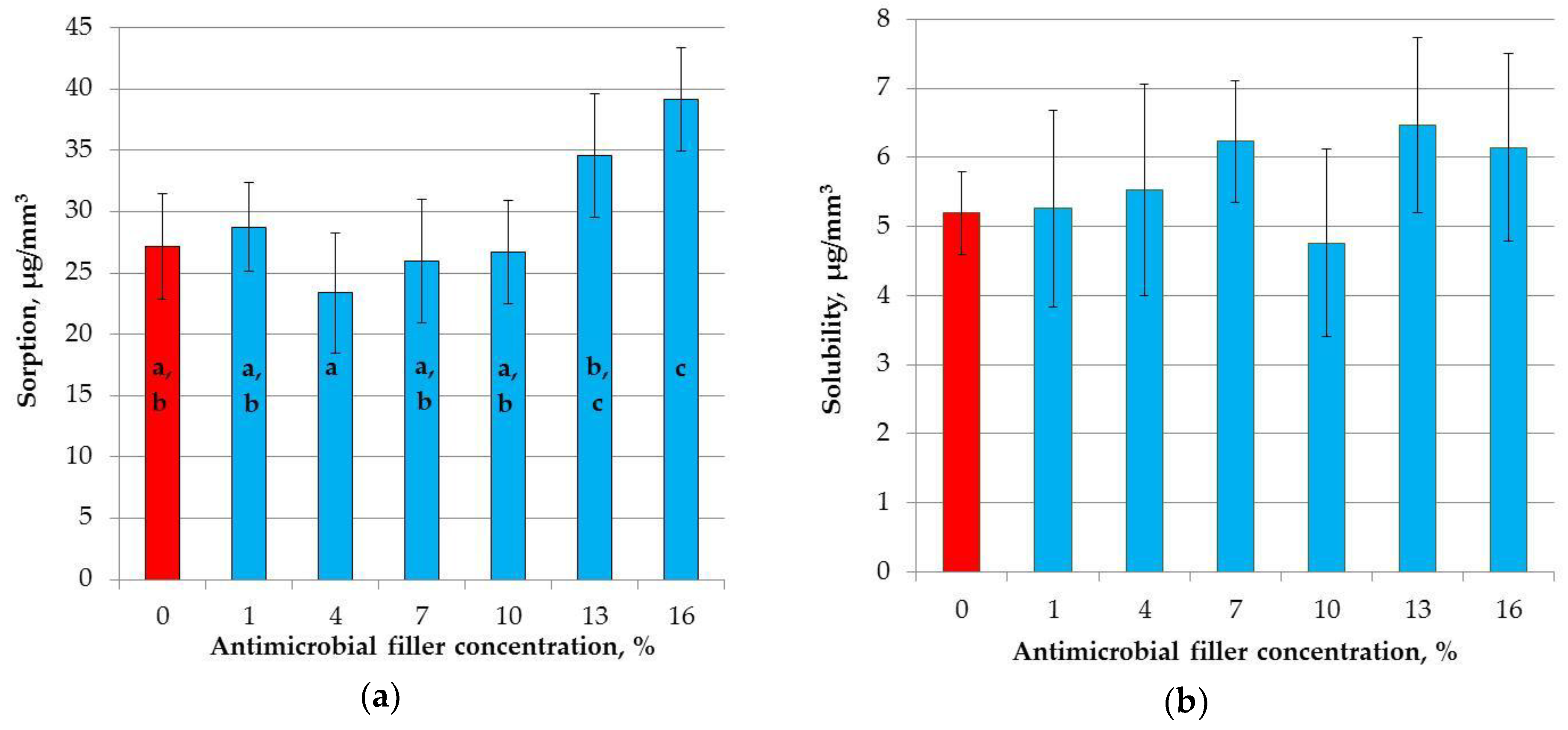
3.8. Sorption and Solubility
3.9. Color Measurement
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coggeshall, M.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Lond. Engl. 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- Polish Ministry of Health. Monitoring the Oral Health of the Polish Population in the Years 2016–2020; Polish Ministry of Health: Warsaw, Poland, 2015. (In Polish) [Google Scholar]
- Anusavice, K.; Shen, C.; Rawls, H.R. Phillips’ Science of Dental Materials—12th Edition, 12th ed.; Saunders: St. Louis, MO, USA, 2013; ISBN 978-0-32-324205-9. [Google Scholar]
- Jayanthi, N.; Vinod, V. Comparative evaluation of compressive strength and flexural strength of conventional core materials with nanohybrid composite resin core material an in vitro study. J. Indian Prosthodont. Soc. 2013, 13, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N.; Hickel, R. Resin composite restorative materials. Aust. Dent. J. 2011, 56 (Suppl. 1), 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ástvaldsdóttir, Á.; Dagerhamn, J.; van Dijken, J.W.V.; Naimi-Akbar, A.; Sandborgh-Englund, G.; Tranæus, S.; Nilsson, M. Longevity of posterior resin composite restorations in adults—A systematic review. J. Dent. 2015, 43, 934–954. [Google Scholar] [CrossRef] [PubMed]
- Alzraikat, H.; Burrow, M.; Maghaireh, G.; Taha, N. Nanofilled Resin Composite Properties and Clinical Performance: A Review. Oper. Dent. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Lambrechts, P.; Goovaerts, K.; Bharadwaj, D.; De Munck, J.; Bergmans, L.; Peumans, M.; Van Meerbeek, B. Degradation of tooth structure and restorative materials: A review. Wear 2006, 261, 980–986. [Google Scholar] [CrossRef]
- Chan, K.H.S.; Mai, Y.; Kim, H.; Tong, K.C.T.; Ng, D.; Hsiao, J.C.M. Review: Resin Composite Filling. Materials 2010, 3, 1228–1243. [Google Scholar] [CrossRef] [Green Version]
- Rasines Alcaraz, M.G.; Veitz-Keenan, A.; Sahrmann, P.; Schmidlin, P.R.; Davis, D.; Iheozor-Ejiofor, Z. Direct composite resin fillings versus amalgam fillings for permanent or adult posterior teeth. Cochrane Database Syst. Rev. 2014, 3, CD005620. [Google Scholar] [CrossRef] [PubMed]
- Hurst, D. Amalgam or composite fillings—Which material lasts longer? Evid. Based Dent. 2014, 15, 50–51. [Google Scholar] [CrossRef] [PubMed]
- Demarco, F.F.; Corrêa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J.M. Longevity of posterior composite restorations: Not only a matter of materials. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Opdam, N.J.M.; van de Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.; van Dijken, J.W. Longevity of posterior composite restorations: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Cenci, T.; Cenci, M.S.; Fedorowicz, Z.; Azevedo, M. Antibacterial agents in composite restorations for the prevention of dental caries. In The Cochrane Library; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2013. [Google Scholar] [Green Version]
- Lai, G.; Li, M. Secondary Caries. In Contemporary Approach to Dental Caries; InTech: Rijeka, Croatia, 2012; pp. 403–422. ISBN 978-9-53-510305-9. [Google Scholar]
- Mjör, I.A.; Toffenetti, F. Secondary caries: A literature review with case reports. Quintessence Int. Berl. Ger. 1985 2000, 31, 165–179. [Google Scholar]
- Shih, W.-Y. Microleakage in different primary tooth restorations. J. Chin. Med. Assoc. 2016, 79, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Gale, M.S.; Darvell, B.W. Thermal cycling procedures for laboratory testing of dental restorations. J. Dent. 1999, 27, 89–99. [Google Scholar] [CrossRef]
- Nedeljkovic, I.; Teughels, W.; De Munck, J.; Van Meerbeek, B.; Van Landuyt, K.L. Is secondary caries with composites a material-based problem? Dent. Mater. Off. Publ. Acad. Dent. Mater. 2015, 31, e247–e277. [Google Scholar] [CrossRef] [PubMed]
- Łukomska-Szymańska, M.; Zarzycka, B.; Grzegorczyk, J.; Sokołowski, K.; Półtorak, K.; Sokołowski, J.; Łapińska, B. Antibacterial Properties of Calcium Fluoride-Based Composite Materials: In VitroStudy. BioMed Res. Int. 2016, 2016, 1048320. [Google Scholar] [CrossRef] [PubMed]
- Chatzistavrou, X.; Lefkelidou, A.; Papadopoulou, L.; Pavlidou, E.; Paraskevopoulos, K.M.; Fenno, J.C.; Flannagan, S.; González-Cabezas, C.; Kotsanos, N.; Papagerakis, P. Bactericidal and Bioactive Dental Composites. Front. Physiol. 2018, 9, 103. [Google Scholar] [CrossRef] [PubMed]
- Imazato, S. Antibacterial properties of resin composites and dentin bonding systems. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2003, 19, 449–457. [Google Scholar] [CrossRef]
- Chen, L.; Shen, H.; Suh, B.I. Antibacterial dental restorative materials: A state-of-the-art review. Am. J. Dent. 2012, 25, 337–346. [Google Scholar] [PubMed]
- Maas, M.S.; Alania, Y.; Natale, L.C.; Rodrigues, M.C.; Watts, D.C.; Braga, R.R. Trends in restorative composites research: What is in the future? Braz. Oral Res. 2017, 31, e55. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Zhang, K.; Zhou, C.-C.; Weir, M.D.; Zhou, X.-D.; Xu, H.H.K. One-year water-ageing of calcium phosphate composite containing nano-silver and quaternary ammonium to inhibit biofilms. Int. J. Oral Sci. 2016, 8, 172–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imazato, S.; Torii, M.; Tsuchitani, Y.; McCabe, J.F.; Russell, R.R. Incorporation of bacterial inhibitor into resin composite. J. Dent. Res. 1994, 73, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Li, F.; Imazato, S.; Cheng, L.; Liu, H.; Arola, D.D.; Bai, Y.; Xu, H.H.K. Dual antibacterial agents of nano-silver and 12-methacryloyloxydodecylpyridinium bromide in dental adhesive to inhibit caries. J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 929–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherchali, F.Z.; Mouzali, M.; Tommasino, J.B.; Decoret, D.; Attik, N.; Aboulleil, H.; Seux, D.; Grosgogeat, B. Effectiveness of the DHMAI monomer in the development of an antibacterial dental composite. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2017, 33, 1381–1391. [Google Scholar] [CrossRef] [PubMed]
- Rego, G.F.; Vidal, M.L.; Viana, G.M.; Cabral, L.M.; Schneider, L.F.J.; Portela, M.B.; Cavalcante, L.M. Antibiofilm properties of model composites containing quaternary ammonium methacrylates after surface texture modification. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2017, 33, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Beyth, N.; Yudovin-Farber, I.; Bahir, R.; Domb, A.J.; Weiss, E.I. Antibacterial activity of dental composites containing quaternary ammonium polyethylenimine nanoparticles against Streptococcus mutans. Biomaterials 2006, 27, 3995–4002. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.F.; Wu, R.; Fan, Y.; Liao, S.; Wang, Y.; Wen, Z.T.; Xu, X. Antibacterial dental composites with chlorhexidine and mesoporous silica. J. Dent. Res. 2014, 93, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.; Spratt, D.A.; Pratten, J.; Gulabivala, K.; Mordan, N.J.; Young, A.M. Chlorhexidine-releasing methacrylate dental composite materials. Biomaterials 2005, 26, 7145–7153. [Google Scholar] [CrossRef] [PubMed]
- Rathke, A.; Staude, R.; Muche, R.; Haller, B. Antibacterial activity of a triclosan-containing resin composite matrix against three common oral bacteria. J. Mater. Sci. Mater. Med. 2010, 21, 2971–2977. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Sangi, L.; Kumar, N. Exploring antibacterial activity and hydrolytic stability of resin dental composite restorative materials containing chitosan. Technol. Health Care Off. J. Eur. Soc. Eng. Med. 2017, 25, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Dong, X.; Yu, Q.; Baker, S.N.; Li, H.; Larm, N.E.; Baker, G.A.; Chen, L.; Tan, J.; Chen, M. Incorporation of antibacterial agent derived deep eutectic solvent into an active dental composite. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2017, 33, 1445–1455. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli Hojati, S.; Alaghemand, H.; Hamze, F.; Ahmadian Babaki, F.; Rajab-Nia, R.; Rezvani, M.B.; Kaviani, M.; Atai, M. Antibacterial, physical and mechanical properties of flowable resin composites containing zinc oxide nanoparticles. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2013, 29, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Kasraei, S.; Sami, L.; Hendi, S.; AliKhani, M.-Y.; Rezaei-Soufi, L.; Khamverdi, Z. Antibacterial properties of composite resins incorporating silver and zinc oxide nanoparticles on Streptococcus mutans and Lactobacillus. Restor. Dent. Endod. 2014, 39, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Aydin Sevinç, B.; Hanley, L. Antibacterial activity of dental composites containing zinc oxide nanoparticles. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 94, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Khvostenko, D.; Hilton, T.J.; Ferracane, J.L.; Mitchell, J.C.; Kruzic, J.J. Bioactive glass fillers reduce bacterial penetration into marginal gaps for composite restorations. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2016, 32, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sodagar, A.; Akhoundi, M.S.A.; Bahador, A.; Jalali, Y.F.; Behzadi, Z.; Elhaminejad, F.; Mirhashemi, A.H. Effect of TiO2 nanoparticles incorporation on antibacterial properties and shear bond strength of dental composite used in Orthodontics. Dent. Press J. Orthod. 2017, 22, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Niu, L.N.; Fang, M.; Jiao, K.; Tang, L.H.; Xiao, Y.H.; Shen, L.J.; Chen, J.H. Tetrapod-like zinc oxide whisker enhancement of resin composite. J. Dent. Res. 2010, 89, 746–750. [Google Scholar] [CrossRef] [PubMed]
- Chatzistavrou, X.; Velamakanni, S.; DiRenzo, K.; Lefkelidou, A.; Fenno, J.C.; Kasuga, T.; Boccaccini, A.R.; Papagerakis, P. Designing dental composites with bioactive and bactericidal properties. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 52, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Ai, M.; Du, Z.; Zhu, S.; Geng, H.; Zhang, X.; Cai, Q.; Yang, X. Composite resin reinforced with silver nanoparticles-laden hydroxyapatite nanowires for dental application. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2017, 33, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Łukomska-Szymańska, M.M.; Kleczewska, J.; Bieliński, D.M.; Jakubowski, W.; Sokołowski, J. Bactericidal properties of experimental dental composites based on dimethacrylate resins reinforced by nanoparticles. Eur. J. Chem. 2014, 5, 419–423. [Google Scholar] [CrossRef]
- Azarsina, M.; Kasraei, S.; Yousef-Mashouf, R.; Dehghani, N.; Shirinzad, M. The antibacterial properties of composite resin containing nanosilver against Streptococcus mutans and Lactobacillus. J. Contemp. Dent. Pract. 2013, 14, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Tanagawa, M.; Matsumoto, S.; Yamada, T.; Atsuta, M. Antibacterial activity of resin composites with silver-containing materials. Eur. J. Oral Sci. 1999, 107, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Sodagar, A.; Akhavan, A.; Hashemi, E.; Arab, S.; Pourhajibagher, M.; Sodagar, K.; Kharrazifard, M.J.; Bahador, A. Evaluation of the antibacterial activity of a conventional orthodontic composite containing silver/hydroxyapatite nanoparticles. Prog. Orthod. 2016, 17, 40. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Weir, M.D.; Xu, H.H.K.; Antonucci, J.M.; Kraigsley, A.M.; Lin, N.J.; Lin-Gibson, S.; Zhou, X. Antibacterial amorphous calcium phosphate nanocomposites with a quaternary ammonium dimethacrylate and silver nanoparticles. Dent. Mater. 2012, 28, 561–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, C.; Chu, L.; Rawls, H.R.; Norling, B.K.; Cardenas, H.L.; Whang, K. Development of an antimicrobial resin—A pilot study. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2011, 27, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Chladek, G.; Basa, K.; Mertas, A.; Pakieła, W.; Żmudzki, J.; Bobela, E.; Król, W. Effect of Storage in Distilled Water for Three Months on the Antimicrobial Properties of Poly(methyl methacrylate) Denture Base Material Doped with Inorganic Filler. Materials 2016, 9, 328. [Google Scholar] [CrossRef] [PubMed]
- Jabłońska-Stencel, E.; Pakieła, W.; Mertas, A.; Bobela, E.; Kasperski, J.; Chladek, G. Effect of Silver-Emitting Filler on Antimicrobial and Mechanical Properties of Soft Denture Lining Material. Materials 2018, 11, 318. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y. Silver-containing alginate fibres and dressings. Int. Wound J. 2005, 2, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Zhu, C. Antimicrobial Properties of Silver-Containing Chitosan Fibers. In Medical and Healthcare Textiles; Woodhead Publishing Series in Textiles; Woodhead Publishing: Sawston, UK, 2010; pp. 7–13. ISBN 978-1-84-569224-7. [Google Scholar]
- Ågren, M. Wound Healing Biomaterials—Volume 2: Functional Biomaterials; Woodhead Publishing: Sawston, UK, 2016; ISBN 978-0-08-100606-1. [Google Scholar]
- Qin, Y. Antimicrobial dressings for the management of wound infection. In Medical Textile Materials; Woodhead Publishing Series in Textiles; Woodhead Publishing: Sawston, UK, 2016; pp. 145–160. ISBN 978-0-08-100618-4. [Google Scholar]
- National Industrial Chemicals Notification and Assessment Scheme (Nicnas)-Silver Sodium Hydrogen Zirconium Phosphate. Available online: https://www.pharosproject.net/uploads/files/sources/1185/alphasan-std1081fr.pdf (accessed on 11 March 2004).
- Melaiye, A.; Sun, Z.; Hindi, K.; Milsted, A.; Ely, D.; Reneker, D.H.; Tessier, C.A.; Youngs, W.J. Silver(I)-imidazole cyclophane gem-diol complexes encapsulated by electrospun tecophilic nanofibers: Formation of nanosilver particles and antimicrobial activity. J. Am. Chem. Soc. 2005, 127, 2285–2291. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Yang, Q.; Wang, Y.; Yu, H.; Chen, X.; Jing, X. Biodegradable electrospun poly(l-lactide) fibers containing antibacterial silver nanoparticles. Eur. Polym. J. 2006, 42, 2081–2087. [Google Scholar] [CrossRef]
- Mota, E.G.; Weiss, A.; Spohr, A.M.; Oshima, H.M.S.; de Carvalho, L.M.N. Relationship between filler content and selected mechanical properties of six microhybrid composites. Rev. Odonto Ciênc. 2011, 26, 151–155. [Google Scholar] [CrossRef] [Green Version]
- Galvão, M.R.; Caldas, S.G.F.R.; Calabrez-Filho, S.; Campos, E.A.; Bagnato, V.S.; Rastelli, A.N.S.; Andrade, M.F. Compressive strength of dental composites photo-activated with different light tips. Laser Phys. 2013, 23, 045604. [Google Scholar] [CrossRef] [Green Version]
- Penn, R.W.; Craig, R.G.; Tesk, J.A. Diametral tensile strength and dental composites. Dent. Mater. 1987, 3, 46–48. [Google Scholar] [CrossRef]
- International Organization for Standardization (ISO). EN ISO 4049:2009 Dentistry—Polymer-Based Restorative Materials; ISO: Geneva, Switzerland, 2009. [Google Scholar]
- Chladek, G.; Basa, K.; Żmudzki, J.; Malara, P.; Nowak, A.J.; Kasperski, J. Influence of aging solutions on wear resistance and hardness of selected resin-based dental composites. Acta Bioeng. Biomech. 2016, 18, 43–52. [Google Scholar] [PubMed]
- Atria, P.J.; Sampaio, C.S.; Cáceres, E.; Fernández, J.; Reis, A.F.; Giannini, M.; Coelho, P.G.; Hirata, R. Micro-computed tomography evaluation of volumetric polymerization shrinkage and degree of conversion of composites cured by various light power outputs. Dent. Mater. J. 2018, 37, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barszczewska-Rybarek, I.; Jurczyk, S. Comparative Study of Structure-Property Relationships in Polymer Networks Based on Bis-GMA, TEGDMA and Various Urethane-Dimethacrylates. Materials 2015, 8, 1230–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leal, J.P.; da Silva, D.J.; Leal, R.F.M.; Oliveira-Júnior, C.D.C.; Prado, V.L.G.; Vale, G.C. Effect of Mouthwashes on Solubility and Sorption of Restorative Composites. Int. J. Dent. 2017, 2017, 5865691. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.; Osorio, R.; Osorio, E.; Fuentes, V.; Prati, C.; Garcia-Godoy, F. Sorption and solubility of resin-based restorative dental materials. J. Dent. 2003, 31, 43–50. [Google Scholar] [CrossRef]
- Vichi, A.; Ferrari, M.; Davidson, C.L. Color and opacity variations in three different resin-based composite products after water aging. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2004, 20, 530–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swift, E.J.; Swift, E.J. Nanocomposites. J. Esthet. Restor. Dent. 2005, 17, 3–4. [Google Scholar] [CrossRef]
- Nuñez-Anita, R.E.; Acosta-Torres, L.S.; Vilar-Pineda, J.; Martínez-Espinosa, J.C.; de la Fuente-Hernández, J.; Castaño, V.M. Toxicology of antimicrobial nanoparticles for prosthetic devices. Int. J. Nanomed. 2014, 9, 3999–4006. [Google Scholar] [CrossRef]
- Scully, C. Oral and Maxillofacial Medicine—E-Book: The Basis of Diagnosis and Treatment, 3rd ed.; Churchill Livingstone Elsevier: Edinburgh, UK, 2013; ISBN 978-0-70-205205-7. [Google Scholar]
- Pinto, T.M.S.; Neves, A.C.C.; Leão, M.V.P.; Jorge, A.O.C. Vinegar as an antimicrobial agent for control of Candida spp. in complete denture wearers. J. Appl. Oral Sci. Rev. FOB 2008, 16, 385–390. [Google Scholar] [CrossRef]
- Gupta Effect of Comonomer of Methacrylic Acid on Flexural Strength and Adhesion of Staphylococcus aureus to Heat Polymerized Poly (Methyl Methacrylate) Resin: An in Vitro Study. Available online: http://www.j-ips.org/article.asp?issn=0972-4052;year=2017;volume=17;issue=2;spage=149;epage=155;aulast=Gupta#ref12 (accessed on 12 January 2018).
- Sumi, Y.; Miura, H.; Sunakawa, M.; Michiwaki, Y.; Sakagami, N. Colonization of denture plaque by respiratory pathogens in dependent elderly. Gerodontology 2002, 19, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.Z.; van der Mei, H.C.; van der Veen, M.H.; de Soet, J.J.; Huysmans, M.C. Bacterial composition and red fluorescence of plaque in relation to primary and secondary caries next to composite: An in situ study. Oral Microbiol. Immunol. 2008, 23, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Tanner, J.; Carlén, A.; Söderling, E.; Vallittu, P.K. Adsorption of parotid saliva proteins and adhesion of Streptococcus mutans ATCC 21752 to dental fiber-reinforced composites. J. Biomed. Mater. Res. B Appl. Biomater. 2003, 66, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Beyth, N.; Bahir, R.; Matalon, S.; Domb, A.J.; Weiss, E.I. Streptococcus mutans biofilm changes surface-topography of resin composites. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2008, 24, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Cazzaniga, G.; Ottobelli, M.; Ionescu, A.; Garcia-Godoy, F.; Brambilla, E. Surface properties of resin-based composite materials and biofilm formation: A review of the current literature. Am. J. Dent. 2015, 28, 311–320. [Google Scholar] [PubMed]
- Kampmann, Y.; De Clerck, E.; Kohn, S.; Patchala, D.K.; Langerock, R.; Kreyenschmidt, J. Study on the antimicrobial effect of silver-containing inner liners in refrigerators. J. Appl. Microbiol. 2008, 104, 1808–1814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahn, E. Clinical criteria for the successful curing of composite materials. Rev. Clín. Periodoncia Implantol. Rehabil. Oral 2013, 6, 148–153. [Google Scholar] [CrossRef]
- Yap, A.U.J.; Teoh, S.H. Comparison of flexural properties of composite restoratives using the ISO and mini-flexural tests. J. Oral Rehabil. 2003, 30, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Dennison, J.; Yaman, P. Physical property evaluation of four composite materials. Oper. Dent. 2013, 38, E144–E153. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, F.; Campos, L.M.P.; Rodrigues-Júnior, E.C.; Costa, F.V.; Marques, P.A.; Francci, C.E.; Braga, R.R.; Boaro, L.C.C. A comparative study of bulk-fill composites: Degree of conversion, post-gel shrinkage and cytotoxicity. Braz. Oral Res. 2018, 32, e17. [Google Scholar] [CrossRef] [PubMed]
- Monte Alto, R.V.; Guimarães, J.G.A.; Poskus, L.T.; da Silva, E.M. Depth of cure of dental composites submitted to different light-curing modes. J. Appl. Oral Sci. Rev. FOB 2006, 14, 71–76. [Google Scholar] [CrossRef]
- Koran, P.; Kürschner, R. Effect of sequential versus continuous irradiation of a light-cured resin composite on shrinkage, viscosity, adhesion, and degree of polymerization. Am. J. Dent. 1998, 11, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Catelan, A.; Mainardi, M.D.C.A.J.; Soares, G.P.; de Lima, A.F.; Ambrosano, G.M.B.; Lima, D.A.N.L.; Marchi, G.M.; Aguiar, F.H.B. Effect of light curing protocol on degree of conversion of composites. Acta Odontol. Scand. 2014, 72, 898–902. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Hanabusa, M.; Kimura, S.; Momoi, Y.; Hayakawa, T. Changes in polymerization stress and elastic modulus of bulk-fill resin composites for 24 hours after irradiation. Dent. Mater. J. 2018, 37, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Achilias, D.S. A Review of Modeling of Diffusion Controlled Polymerization Reactions. Macromol. Theory Simul. 2007, 16, 319–347. [Google Scholar] [CrossRef]
- Korkut, E.; Torlak, E.; Altunsoy, M. Antimicrobial and mechanical properties of dental resin composite containing bioactive glass. J. Appl. Biomater. Funct. Mater. 2016, 14, e296–e301. [Google Scholar] [CrossRef] [PubMed]
- Chun, K.; Choi, H.; Lee, J. Comparison of mechanical property and role between enamel and dentin in the human teeth. J. Dent. Biomech. 2014, 5, 1758736014520809. [Google Scholar] [CrossRef] [PubMed]
- Moezzyzadeh, M. Evaluation of the Compressive Strength of Hybrid and Nanocomposites. Shahid Beheshti Univ. Dent. J. 2012, 30, 23–28. [Google Scholar]
- Xu, X.; Burgess, J.O. Compressive strength, fluoride release and recharge of fluoride-releasing materials. Biomaterials 2003, 24, 2451–2461. [Google Scholar] [CrossRef]
- Das Neves, P.B.A.; Agnelli, J.A.M.; Kurachi, C.; de Souza, C.W.O. Addition of silver nanoparticles to composite resin: Effect on physical and bactericidal properties in vitro. Braz. Dent. J. 2014, 25, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.D.; Smith, D.C. Measurement of the tensile strength of dental restorative materials by use of a diametral compression test. J. Dent. Res. 1971, 50, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.; Ciaramella, S.; Fabianelli, A.; Gloria, A.; Martorelli, M.; Lanzotti, A.; Watts, D.C. Mechanical behavior of bulk direct composite versus block composite and lithium disilicate indirect Class II restorations by CAD-FEM modeling. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2017, 33, 690–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dejak, B.; Młotkowski, A. A comparison of stresses in molar teeth restored with inlays and direct restorations, including polymerization shrinkage of composite resin and tooth loading during mastication. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2015, 31, e77–e87. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, R.; Powers, J. Craig’s Restorative Dental Materials, 13th ed.; Elsevier Mosby: Philadelphia, PA, USA, 2012; ISBN 978-0-32-308108-5. [Google Scholar]
- Casselli, D.S.M.; Worschech, C.C.; Paulillo, L.A.M.S.; Dias, C.T.D.S. Diametral tensile strength of composite resins submitted to different activation techniques. Braz. Oral Res. 2006, 20, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Della Bona, A.; Benetti, P.; Borba, M.; Cecchetti, D. Flexural and diametral tensile strength of composite resins. Braz. Oral Res. 2008, 22, 84–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, S.B.; Wu, D.; Holmes, B.N. An application of nanotechnology in advanced dental materials. J. Am. Dent. Assoc. 1939 2003, 134, 1382–1390. [Google Scholar] [CrossRef]
- Łukomska-Szymańska, M.; Kleczewska, J.; Nowak, J.; Pryliński, M.; Szczesio, A.; Podlewska, M.; Sokołowski, J.; Łapińska, B. Mechanical Properties of Calcium Fluoride-Based Composite Materials. BioMed Res. Int. 2016, 2016, 2752506. [Google Scholar] [CrossRef] [PubMed]
- Dias, H.B.; Bernardi, M.I.B.; Ramos, M.A.D.S.; Trevisan, T.C.; Bauab, T.M.; Hernandes, A.C.; de Souza Rastelli, A.N. Zinc oxide 3D microstructures as an antimicrobial filler content for composite resins. Microsc. Res. Tech. 2017, 80, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Sokołowski, J.; Szynkowska, M.I.; Kleczewska, J.; Kowalski, Z.; Sobczak-Kupiec, A.; Pawlaczyk, A.; Sokołowski, K.; Łukomska-Szymańska, M. Evaluation of resin composites modified with nanogold and nanosilver. Acta Bioeng. Biomech. 2014, 16, 51–61. [Google Scholar]
- Ferracane, J.L. Resin-based composite performance: Are there some things we can’t predict? Dent. Mater. Off. Publ. Acad. Dent. Mater. 2013, 29, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peutzfeldt, A.; Asmussen, E. Modulus of resilience as predictor for clinical wear of restorative resins. Dent. Mater. Off. Publ. Acad. Dent. Mater. 1992, 8, 146–148. [Google Scholar] [CrossRef]
- Feiz, A.; Samanian, N.; Davoudi, A.; Badrian, H. Effect of different bleaching regimens on the flexural strength of hybrid composite resin. J. Conserv. Dent. 2016, 19, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Pala, K.; Tekçe, N.; Tuncer, S.; Demirci, M.; Öznurhan, F.; Serim, M. Flexural strength and microhardness of anterior composites after accelerated aging. J. Clin. Exp. Dent. 2017, 9, e424–e430. [Google Scholar] [CrossRef] [PubMed]
- Kumar, G.; Shivrayan, A. Comparative study of mechanical properties of direct core build-up materials. Contemp. Clin. Dent. 2015, 6, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Randolph, L.D.; Palin, W.M.; Leloup, G.; Leprince, J.G. Filler characteristics of modern dental resin composites and their influence on physico-mechanical properties. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2016, 32, 1586–1599. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues Junior, S.A.; Zanchi, C.H.; de Carvalho, R.V.; Demarco, F.F. Flexural strength and modulus of elasticity of different types of resin-based composites. Braz. Oral Res. 2007, 21, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandão, N.L.; Portela, M.B.; Maia, L.C.; Antônio, A.; Silva, V.L.M.E.; Silva, E.M.D. Model resin composites incorporating ZnO-NP: Activity against S. mutans and physicochemical properties characterization. J. Appl. Oral Sci. Rev. FOB 2018, 26, e20170270. [Google Scholar] [CrossRef] [PubMed]
- Łapińska, B.; Łukomska-Szymańska, M.; Sokołowski, J.; Nowak, J. Experimental composite material modified with calcium fluoride—Three-point bending flexural test. J. Achiev. Mater. Manuf. Eng. 2016, 74, 72–77. [Google Scholar] [CrossRef]
- Azillah, M.A.; Anstice, H.M.; Pearson, G.J. Long-term flexural strength of three direct aesthetic restorative materials. J. Dent. 1998, 26, 177–182. [Google Scholar] [CrossRef]
- Poggio, C.; Lombardini, M.; Gaviati, S.; Chiesa, M. Evaluation of Vickers hardness and depth of cure of six composite resins photo-activated with different polymerization modes. J. Conserv. Dent. 2012, 15, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Abed, Y.A.; Sabry, H.A.; Alrobeigy, N.A. Degree of conversion and surface hardness of bulk-fill composite versus incremental-fill composite. Tanta Dent. J. 2015, 12, 71–80. [Google Scholar] [CrossRef]
- Roy, K.K.; Kumar, K.P.; John, G.; Sooraparaju, S.G.; Nujella, S.K.; Sowmya, K. A comparative evaluation of effect of modern-curing lights and curing modes on conventional and novel-resin monomers. J. Conserv. Dent. 2018, 21, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.; Ilie, N. The effect of aging on the mechanical properties of nanohybrid composites based on new monomer formulations. Clin. Oral Investig. 2013, 17, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Randolph, L.D.; Palin, W.M.; Bebelman, S.; Devaux, J.; Gallez, B.; Leloup, G.; Leprince, J.G. Ultra-fast light-curing resin composite with increased conversion and reduced monomer elution. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2014, 30, 594–604. [Google Scholar] [CrossRef] [PubMed]
- AlShaafi, M.M. Factors affecting polymerization of resin-based composites: A literature review. Saudi Dent. J. 2017, 29, 48–58. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, D.C.R.S.; de Menezes, L.R.; Gatti, A.; Correr Sobrinho, L.; Ferracane, J.L.; Sinhoreti, M.A.C. Effect of Nanofiller Loading on Cure Efficiency and Potential Color Change of Model Composites. J. Esthet. Restor. Dent. 2016, 28, 171–177. [Google Scholar] [CrossRef] [PubMed]
- AlShaafi, M.M. Effects of Different Temperatures and Storage Time on the Degree of Conversion and Microhardness of Resin-based Composites. J. Contemp. Dent. Pract. 2016, 17, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Catelan, A.; de Araújo, L.S.N.; da Silveira, B.C.M.; Kawano, Y.; Ambrosano, G.M.B.; Marchi, G.M.; Aguiar, F.H.B. Impact of the distance of light curing on the degree of conversion and microhardness of a composite resin. Acta Odontol. Scand. 2015, 73, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Bociong, K.; Szczesio, A.; Sokolowski, K.; Domarecka, M.; Sokolowski, J.; Krasowski, M.; Lukomska-Szymanska, M. The Influence of Water Sorption of Dental Light-Cured Composites on Shrinkage Stress. Materials 2017, 10, 1142. [Google Scholar] [CrossRef] [PubMed]
- Boaro, L.C.; Gonçalves, F.; Guimarães, T.C.; Ferracane, J.L.; Pfeifer, C.S.; Braga, R.R. Sorption, solubility, shrinkage and mechanical properties of “low-shrinkage” commercial resin composites. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2013, 29, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Mortier, E.; Gerdolle, D.A.; Jacquot, B.; Panighi, M.M. Importance of water sorption and solubility studies for couple bonding agent—Resin-based filling material. Oper. Dent. 2004, 29, 669–676. [Google Scholar] [PubMed]
- Sideridou, I.; Tserki, V.; Papanastasiou, G. Study of water sorption, solubility and modulus of elasticity of light-cured dimethacrylate-based dental resins. Biomaterials 2003, 24, 655–665. [Google Scholar] [CrossRef]
- Mokrzycki, W.S.; Tatol, M. Color difference ΔE: A survey. Mach. Graph. Vis. 2011, 20, 383–411. [Google Scholar]
- De Oliveira, D.C.R.S.; Ayres, A.P.A.; Rocha, M.G.; Giannini, M.; Puppin Rontani, R.M.; Ferracane, J.L.; Sinhoreti, M.A.C. Effect of Different In Vitro Aging Methods on Color Stability of a Dental Resin-Based Composite Using CIELAB and CIEDE2000 Color-Difference Formulas. J. Esthet. Restor. Dent. 2015, 27, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Jeong, T.-S.; Kang, H.-S.; Kim, S.-K.; Kim, S.; Kim, H.-I.; Kwon, Y.H. The effect of resin shades on microhardness, polymerization shrinkage, and color change of dental composite resins. Dent. Mater. J. 2009, 28, 438–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albuquerque, P.P.A.C.; Bertolo, M.L.; Cavalcante, L.M.A.; Pfeifer, C.; Schneider, L.F.S. Degree of conversion, depth of cure, and color stability of experimental dental composite formulated with camphorquinone and phenanthrenequinone photoinitiators. J. Esthet. Restor. Dent. 2015, 27 (Suppl. 1), S49–S57. [Google Scholar] [CrossRef] [PubMed]
- Fúcio, S.B.P.; Carvalho, F.G.; Sobrinho, L.C.; Sinhoreti, M.A.C.; Puppin-Rontani, R.M. The influence of 30-day-old Streptococcus mutans biofilm on the surface of esthetic restorative materials—An in vitro study. J. Dent. 2008, 36, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Melo, M.A.; Orrego, S.; Weir, M.D.; Xu, H.H.K.; Arola, D.D. Designing Multiagent Dental Materials for Enhanced Resistance to Biofilm Damage at the Bonded Interface. ACS Appl. Mater. Interfaces 2016, 8, 11779–11787. [Google Scholar] [CrossRef] [PubMed]
- Mutluay, M.M.; Zhang, K.; Ryou, H.; Yahyazadehfar, M.; Majd, H.; Xu, H.H.K.; Arola, D. On the fatigue behavior of resin-dentin bonds after degradation by biofilm. J. Mech. Behav. Biomed. Mater. 2013, 18, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Carrera, C.; Chen, R.; Li, J.; Lenton, P.; Rudney, J.D.; Jones, R.S.; Aparicio, C.; Fok, A. Degradation in the dentin-composite interface subjected to multi-species biofilm challenges. Acta Biomater. 2014, 10, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Drummond, J.L. Degradation, fatigue and failure of resin dental composite materials. J. Dent. Res. 2008, 87, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Lohbauer, U.; Belli, R.; Ferracane, J.L. Factors involved in mechanical fatigue degradation of dental resin composites. J. Dent. Res. 2013, 92, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Ravindranath, V.; Gosz, M.; De Santiago, E.; Drummond, J.L.; Mostovoy, S. Effect of cyclic loading and environmental aging on the fracture toughness of dental resin composite. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 80, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Mutluay, M.M.; Yahyazadefar, M.; Ryou, H.; Majd, H.; Do, D.; Arola, D. Fatigue of the Resin-Dentin Interface: A New Approach for Evaluating the Durability of Dentin Bonds. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2013, 29, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Yahyazadehfar, M.; Mutluay, M.M.; Majd, H.; Ryou, H.; Arola, D. Fatigue of the resin-enamel bonded interface and the mechanisms of failure. J. Mech. Behav. Biomed. Mater. 2013, 21, 121–132. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Code | Matrix, g | Matrix, % (w/w) | RF, g | RF, % (w/w) | SSHZP, g | SSHZP, % (w/w) | TF, % (w/w) |
|---|---|---|---|---|---|---|---|
| Control | 15.00 | 35.00 | 27.86 | 65.00 | 0 | 0 | 65.00 |
| AC 1 | 15.00 | 34.35 | 27.86 | 64.65 | 0.43 | 1 | 65.35 |
| AC 4 | 15.00 | 33.60 | 27.86 | 62.40 | 1.76 | 4 | 66.40 |
| AC 7 | 15.00 | 32.55 | 27.86 | 60.45 | 3.22 | 7 | 67.45 |
| AC 10 | 15.00 | 31.50 | 27.86 | 58.50 | 4.76 | 10 | 68.50 |
| AC 13 | 15.00 | 30.45 | 27.86 | 56.55 | 6.40 | 13 | 69.55 |
| AC 16 | 15.00 | 29.40 | 27.86 | 54.60 | 8.16 | 16 | 70.60 |
| cSSZHP, % | CFU/mL (Vt) ×104 | RB, % | ||||
|---|---|---|---|---|---|---|
| Med | Max | Min | Med | Max | Min | |
| 0 | 3.53 | 3.99 | 3.13 | 4.7 | 15.5 | −7.7 |
| 1 | 2.08 | 2.89 | 1.87 | 43.8 | 49.6 | 21.9 |
| 4 | 0.68 | 0.13 | 0.00 | 70.1 | 93.2 | 65.7 |
| 7 | 0.00 | 0.00 | 0.00 | 100.0 | 100.0 | 100.0 |
| 10 | 0.00 | 0.00 | 0.00 | 100.0 | 100.0 | 100.0 |
| 13 | 0.00 | 0.00 | 0.00 | 100.0 | 100.0 | 100.0 |
| 16 | 0.00 | 0.00 | 0.00 | 100.0 | 100.0 | 100.0 |
| cSSZHP, % | L* | a* | b* |
|---|---|---|---|
| 0 | 51.34 ± 0.36 a | 5.97 ± 0.08 a | 12.83 ± 0.26 a |
| 1 | 54.48 ± 0.47 b | 4.53 ± 0.20 b | 11.21 ± 0.38 b |
| 4 | 70.42 ± 0.21 c | 2.28 ± 0.21 c | 10.59 ± 0.35 c |
| 7 | 76.50 ± 0.18 d | 1.79 ± 0.15 d | 9.55 ± 0.22 d |
| 10 | 81.09 ± 0.09 e | 1.00 ± 0.04 e | 6.82 ± 0.18 e |
| 13 | 82.84 ± 0.16 f | 0.96 ± 0.07 e | 5.63 ± 0.10 f |
| 16 | 85.84 ± 0.16 g | 0.51 ± 0.11 f | 5.32 ± 0.19 f |
| cSSZHP, % | ΔL* | Δa* | Δb* | ΔE* |
|---|---|---|---|---|
| 0 | −0.88 ± 0.15 a | 0.37 ± 0.07 a | 0.61 ± 0.04 a | 1.14 ± 0.10 a |
| 1 | −0.95 ± 0.18 a,b | 0.41 ± 0.06 a | 0.64 ± 0.04 a | 1.22 ± 0.13 a |
| 4 | −1.10 ± 0.08 a,b | 0.47 ± 0.10 a,b | 0.60 ± 0.05 a | 1.34 ± 0.09 a |
| 7 | −1.13 ± 0.14 a,b | 0.44 ± 0.12 a | 0.64 ± 0.07 a | 1.38 ± 0.10 a |
| 10 | −0.98 ± 0.15 a,b | 0.43 ± 0.09 a | 0.70 ± 0.06 a | 1.29 ± 0.10 a |
| 13 | −1.21 ± 0.14 b | 0.64 ± 0.05 b | 1.11 ± 0.12 b | 1.77 ± 0.14 b |
| 16 | −1.88 ± 0.16 c | 1.10 ± 0.05 c | 1.41 ± 0.08 c | 2.60 ± 0.11 c |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stencel, R.; Kasperski, J.; Pakieła, W.; Mertas, A.; Bobela, E.; Barszczewska-Rybarek, I.; Chladek, G. Properties of Experimental Dental Composites Containing Antibacterial Silver-Releasing Filler. Materials 2018, 11, 1031. https://doi.org/10.3390/ma11061031
Stencel R, Kasperski J, Pakieła W, Mertas A, Bobela E, Barszczewska-Rybarek I, Chladek G. Properties of Experimental Dental Composites Containing Antibacterial Silver-Releasing Filler. Materials. 2018; 11(6):1031. https://doi.org/10.3390/ma11061031
Chicago/Turabian StyleStencel, Robert, Jacek Kasperski, Wojciech Pakieła, Anna Mertas, Elżbieta Bobela, Izabela Barszczewska-Rybarek, and Grzegorz Chladek. 2018. "Properties of Experimental Dental Composites Containing Antibacterial Silver-Releasing Filler" Materials 11, no. 6: 1031. https://doi.org/10.3390/ma11061031