Effects of Polyacrylic Acid Pre-Treatment on Bonded-Dentine Interfaces Created with a Modern Bioactive Resin-Modified Glass Ionomer Cement and Subjected to Cycling Mechanical Stress

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Preparation of Dentine Specimens
2.2. Micro-Tensile Bond Strength (MTBS) and Fracture Analysis (FE-SEM)
2.3. Ultramorphology of the Bonded-Dentine Interfaces: Confocal Microscopy Evaluation
3. Results
3.1. Micro-Tensile Bond Strength (MTBS) and Failure Mode Analysis
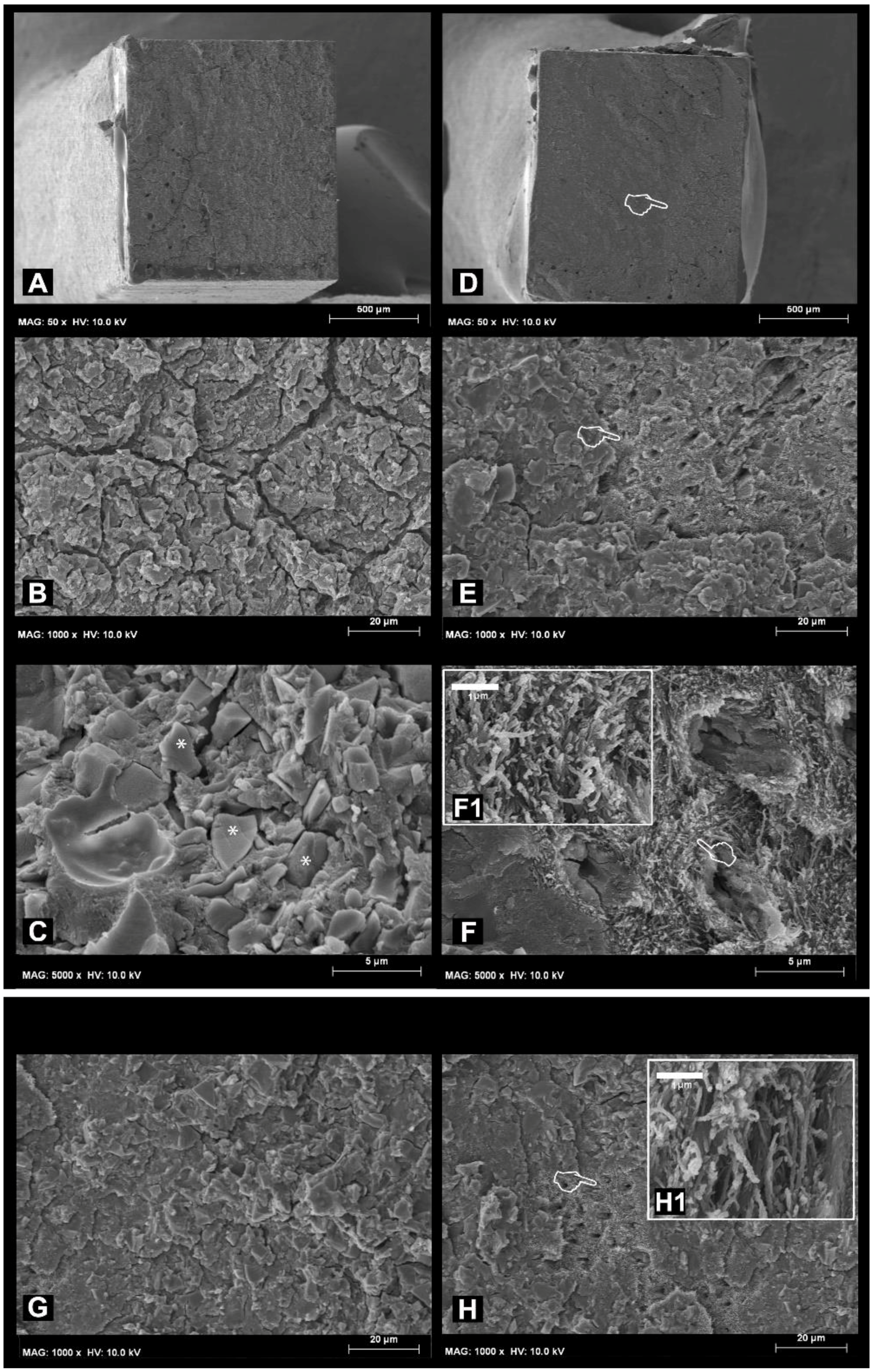
3.2. Failure and Fractographic FE-SEM Analysis
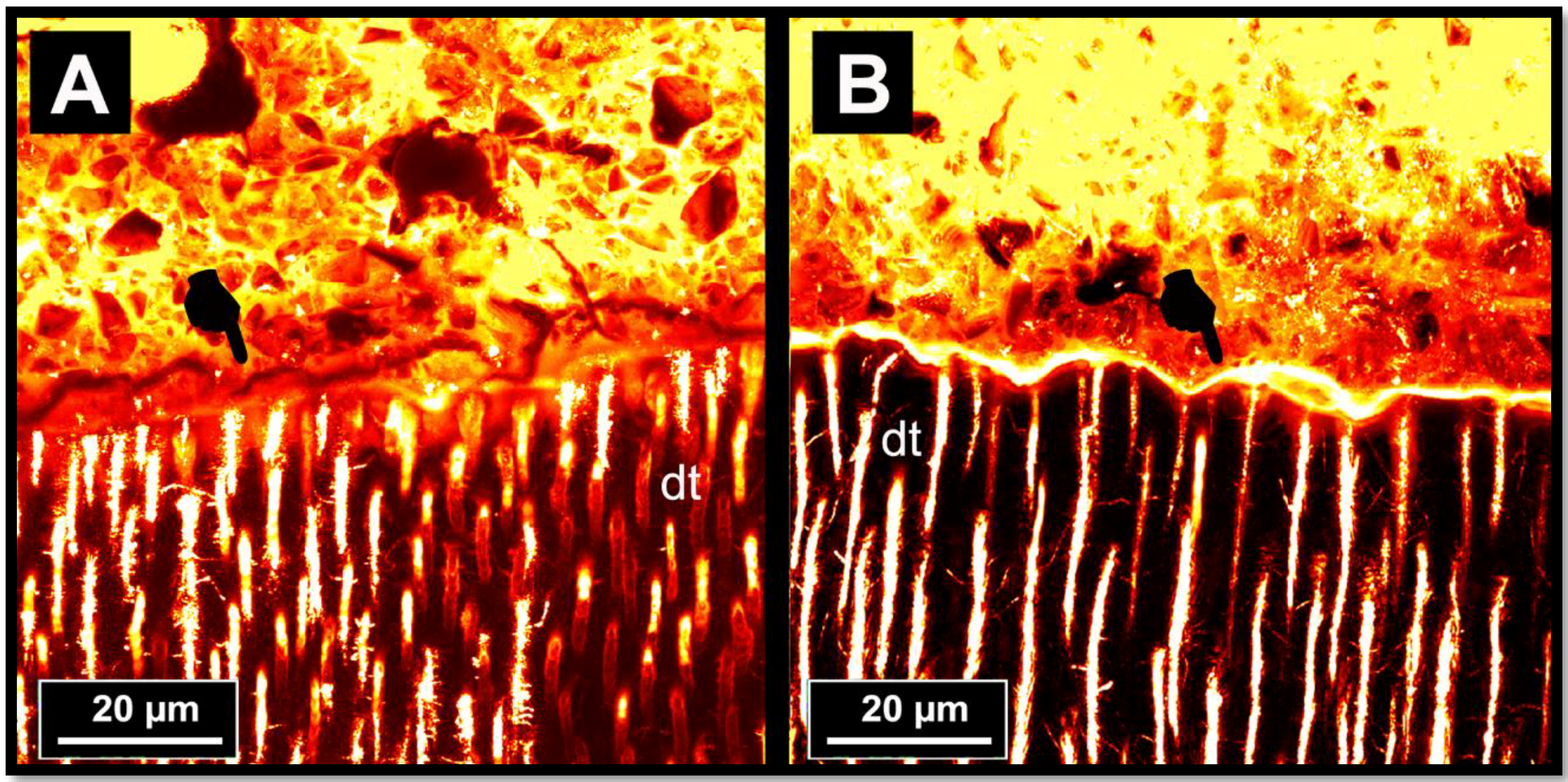
3.3. Ultramorphology of the Bonded-Dentine Interfaces: Confocal Microscopy Evaluation
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wilson, A.D.; Kent, B.E. The glass-ionomer cement, a new translucent dental filling material. J. Appl. Chem. Biotechnol. 1971, 21, 313. [Google Scholar] [CrossRef]
- Wilson, A.D.; Nicholson, J.W. Acid-Base Cements: Their Biomedical and Industrial Applications; Cambridge University Press: Cambridge, UK, July 2005; Volume 3. [Google Scholar]
- Prosser, H.J.; Powis, D.R.; Wilson, A.D. Glass-ionomer cements of improved flexural strength. J. Dent. Res. 1986, 65, 146–148. [Google Scholar] [CrossRef] [PubMed]
- Alhalawani, A.M.; Curran, D.J.; Boyd, D.; Towler, M.R. The role of poly(acrylic acid) in conventional glass polyalkenoate cements. J. Polym. Eng. 2016, 36, 221–237. [Google Scholar] [CrossRef]
- Guggenberger, R.; May, R.; Stefan, K.P. New trends in glass-ionomer chemistry. Biomaterials 1998, 19, 479–483. [Google Scholar] [CrossRef]
- McCabe, J.F.; Walls, A.W. (Eds.) Applied Dental Materials; John Wiley & Sons: Hoboken, NJ, USA, May 2013. [Google Scholar]
- Anusavice, K.J.; Shen, C.; Rawls, H.R. Phillips’ Science of Dental Materials; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Wilson, A.D. The chemistry of dental cements. Chem. Soc. Rev. 1978, 7, 265–296. [Google Scholar] [CrossRef]
- Nicholson, J.W. Chemistry of glass-ionomer cements: A review. Biomaterials 1998, 19, 485–494. [Google Scholar] [CrossRef]
- Zainuddin, N.; Karpukhina, N.; Hill, R.G.; Law, R.V. A long-term study on the setting reaction of glass ionomer cements by 27 Al MAS-NMR spectroscopy. Dent. Mater. 2009, 25, 290–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preston, A.J.; Higham, S.M.; Agalamanyi, E.A.; Mair, L.H. Fluoride recharge of aesthetic dental materials. J. Oral Rehabil. 1999, 26, 936–940. [Google Scholar] [CrossRef] [PubMed]
- Forsten, L. Resin-modified glass ionomer cements: Fluoride release and uptake. Acta Odontol. Scand. 1995, 53, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Forss, H.; Jokinen, J.; Spets-Happonen, S.; Seppä, L.; Luoma, H. Fluoride and mutans streptococci in plaque grown on glass ionomer and composite. Caries Res. 1991, 25, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Preston, A.J.; Mair, L.H.; Agalamanyi, E.A.; Higham, S.M. Fluoride release from aesthetic dental materials. J. Oral Rehabil. 1999, 26, 123–129. [Google Scholar] [CrossRef] [PubMed]
- De Amorim, R.G.; Leal, S.C.; Frencken, J.E. Survival of atraumatic restorative treatment (ART) sealants and restorations: A meta-analysis. Clin. Oral Investig. 2012, 16, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Van Dijken, J.W. 3-Year clinical evaluation of a compomer, a resin-modified glass ionomer and a resin composite in class III restorations. Am. J. Dent. 1996, 9, 195–198. [Google Scholar] [PubMed]
- Abdalla, A.I.; Alhadainy, H.A.; Garcia-Godoy, F. Clinical evaluation of glass ionomers and compomers in class V carious lesions. Am. J. Dent. 1997, 10, 18–20. [Google Scholar] [PubMed]
- Leevailoj, C.; Platt, J.A.; Cochran, M.A.; Moore, B.K. In vitro study of fracture incidence and compressive fracture load of all-ceramic crowns cemented with resin-modified glass ionomer and other luting agents. J. Prosthet. Dent. 1998, 80, 699–707. [Google Scholar] [CrossRef]
- Pascotto, R.C.; de Lima Navarro, M.F.; Capelozza Filho, L.; Cury, J.A. In vivo effect of a resin-modified glass ionomer cement on enamel demineralization around orthodontic brackets. Am. J. Orthod. Dentofac. 2004, 125, 36–41. [Google Scholar] [CrossRef]
- Jokstad, A.; Mjör, I.A. Ten years’ clinical evaluation of three luting cements. J. Dent. 1996, 24, 309–315. [Google Scholar] [CrossRef]
- Murdoch-Kinch, C.A.; McLean, M.E. Minimally invasive dentistry. J. Am. Dent. Assoc. 2003, 134, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Peumans, M.; de Munck, J.; Mine, A.; van Meerbeek, B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent. Mater. 2014, 30, 1089–1103. [Google Scholar] [CrossRef] [PubMed]
- Terata, R.; Nakashima, K.; Kubota, M. Effect of temporary materials on bond strength of resin-modified glass-ionomer luting cements to teeth. Am. J. Dent. 2000, 13, 209–211. [Google Scholar] [PubMed]
- McLean, J.W.; Powis, D.R.; Prosser, H.J.; Wilson, A.D. The use of glass-ionomer cements in bonding composite resins to dentine. Br. Dent. J. 1985, 158, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Andersson-Wenckert, I.E.; Kieri, C. Durability of extensive class II open-sandwich restorations with a resin-modified glass ionomer cement after 6 years. Am. J. Dent. 2004, 17, 43–50. [Google Scholar] [PubMed]
- Yamaga, R.; Nishino, M.; Yoshida, S.; Yokomizo, I. Diammine silver fluoride and its clinical application. J. Osaka Univ. Dent. Sch. 1972, 12, 1–20. [Google Scholar] [PubMed]
- Sauro, S.; Osorio, R.; Watson, T.F.; Toledano, M. Influence of phosphoproteins’ biomimetic analogs on remineralization of mineral-depleted resin–dentin interfaces created with ion-releasing resin-based systems. Dent. Mater. 2015, 31, 759–777. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Brantley, W.A.; Culbertson, B.M.; Wang, G. Mechanical properties and microstructures of glass-ionomer cements. Dent. Mater. 2000, 16, 129–138. [Google Scholar] [CrossRef]
- Peutzfeldt, A.; Garcia-Godoy, F.; Asmussen, E. Surface hardness and wear of glass ionomers and compomers. Am. J. Dent. 1997, 10, 15–17. [Google Scholar] [PubMed]
- Ahmed, N.; Zafar, M.S. Effects of wear on hardness and stiffness of restorative dental materials. Life Sci. J. 2014, 11, 11–18. [Google Scholar]
- Um, C.M.; Øilo, G. The effect of early water contact on glass-ionomer cements. Quintessence Int. 1992, 1, 23. [Google Scholar]
- Moshaverinia, A.; Roohpour, N.; Chee, W.W.L.; Schricker, S.R. A review of powder modifications in conventional glass-ionomer dental cements. J. Mater. Chem. 2011, 21, 1319–1328. [Google Scholar] [CrossRef]
- Moshaverinia, A.; Ansari, S.; Moshaverinia, M.; Roohpour, N.; Darr, J.A.; Rehman, I. Effects of incorporation of hydroxyapatite and fluoroapatite nanobioceramics into conventional glass ionomer cements (GIC). Acta Biomater. 2008, 4, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Moshaverinia, A.; Ansari, S.; Movasaghi, Z.; Billington, R.W.; Darr, J.A.; Rehman, I.U. Modification of conventional glass-ionomer cements with N-vinylpyrrolidone containing polyacids, nano-hydroxy and fluorapatite to improve mechanical properties. Dent. Mater. 2008, 24, 1381–1390. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Resin-modified glass-ionomer cements. Int. J. Prosthodont. 1989, 3, 425–429. [Google Scholar]
- Soncini, J.A.; Maserejian, N.N.; Trachtenberg, F.; Tavares, M.; Hayes, C. The Longevity of amalgam versus compomer/composite restorations in posterior primary and permanent teeth: Findings from the new england children’s amalgam trial. J. Am. Dent. Assoc. 2007, 138, 763–772. [Google Scholar] [CrossRef] [PubMed]
- McCabe, J.F. Resin-modified glass-ionomers. Biomaterials 1998, 19, 521–527. [Google Scholar] [CrossRef]
- Sauro, S.; Pashley, D. Strategies to stabilise dentine-bonded interfaces through remineralising operative approaches - State of The Art. Int. J. Adhes. Adhes. 2016, 69, 39–57. [Google Scholar] [CrossRef]
- Tyas, M.J.; Burrow, M.F. Adhesive restorative materials: A review. Aust. Dent. J. 2004, 49, 112–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, S.; Abe, Y.; Yoshida, Y.; De Munck, J.; Sano, H.; Suzuki, K.; Lambrechts, P.; Van Meerbeek, B. Effect of conditioner on bond strength of glass-ionomer adhesive to dentin/enamel with and without smear layer interposition. Oper. Dent. 2004, 29, 685–692. [Google Scholar] [PubMed]
- De Munck, J.; Van Meerbeek, B.; Yoshida, Y.; Inoue, S.; Suzuki, K.; Lambrechts, P. Four-year water degradation of a resin-modified glass-ionomer adhesive bonded to dentin. Eur. J. Oral Sci. 2004, 112, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.; Cabello, I.; Aguilera, F.S.; Osorio, E.; Osorio, R. Effect of in vitrochewing and bruxism events on remineralization, at the resin-dentin interface. J. Biomech. 2015, 48, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Sauro, S.; Watson, T.; Moscardó, A.P.; Luzi, A.; Feitosa, V.P.; Banerjee, A. The effect of dentine pre-treatment using bioglass and/or polyacrylic acid on the interfacial characteristics of resin-modified glass ionomer cements. J. Dent. 2018, 73, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Watson, T.F.; Atmeh, A.R.; Sajini, S.; Cook, R.J.; Festy, F. Present and future of glass ionomersand calcium-silicate cements as bioactive materials in dentistry: biophotonics-based interfacial analyses in health and disease. Dent. Mater. 2014, 30, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Van Meerbeek, B.; Abe, Y.; Yoshida, Y.; Lambrechts, P.; Vanherle, G.; Sano, H. Effect of remaining dentin thickness and the use of conditioner on micro-tensile bond strength of a glass-ionomer adhesive. Dent. Mater. 2001, 17, 445–455. [Google Scholar] [CrossRef]
- Yoshida, Y.; Van Meerbeek, B.; Nakayama, Y.; Snauwaert, J.; Hellemans, L.; Lambrechts, P.; Vanherle, G.; Wakasa, K. Evidence of chemical bonding at biomaterial–hard tissue interfaces. J. Dent. Res. 2000, 79, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Van Meerbeek, B.; Vargas, M.; Inoue, S.; Yoshida, Y.; Peumans, M.; Lambrechts, P.; Vanherle, G. Adhesives and cements topromote preservation dentistry. Oper. Dent. 2001, 26, 119–144. [Google Scholar]
- Van Meerbeek, B.; Inoue, S.; Perdigao, J.; Lambrechts, P.; Vanherle, G. Enamel and Dentin Adhesion; Summitt, J.B., Robbins, J.W., Schwartz, R.S, Eds.; Quintessence Publishing Co.: Chicago, IL, USA, 2001; pp. 178–235. [Google Scholar]
- Lin, A.; McIntyre, N.; Davidson, R. Studies on the adhesion of glass ionomer cements to dentin. J. Dent. Res. 1992, 71, 1836–1841. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.; Osorio, R.; Osorio, E.; Cabello, I.; Toledano-Osorio, M.; Aguilera, F.S. In vitro mechanical stimulation facilitates stress dissipation and sealing ability at the conventional glass ionomer cement-dentin interface. J. Dent. 2018, 73, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Yiu, C.K.; Kim, J.R.; Gu, L.; Kim, S.K.; Weller, R.N.; Pashley, D.H.; Tay, F.R. Failureof a glass ionomer to remineralise apatite-depleted dentin. J. Dent. Res. 2010, 89, 230–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, L.S.; Kim, J.; Kim, Y.K.; Liu, Y.; Dickens, S.H.; Pashley, D.H.; Ling, J.Q.; Tay, F.R. Achemical phosphorylation-inspired design for Type I collagen biomimeticremineralization. Dent. Mater. 2010, 26, 1077–1089. [Google Scholar] [CrossRef] [PubMed]
- Nishitani, Y.; Yoshiyama, M.; Wadgaonkar, B.; Breschi, L.; Mannello, F.; Mazzoni, A.; Carvalho, R.M.; Tjäderhane, L.; Tay, F.R.; Pashley, D.H. Activation of gelatinolytic/collagenolytic activity in dentin by self-etching adhesives. Eur. J. Oral Sci. 2006, 114, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Es-Souni, M.; Fischer-Brandies, H.; Zaporojshenko, V.; Es-Souni, M. On the interactionof polyacrylic acid as a conditionning agent with bovine enamel. Biomaterials 2002, 23, 2871–2878. [Google Scholar] [CrossRef]
- Sidhu, S.K.; Watson, T.F. Interfacial characteristics of resin-modified glass-ionomermaterials: A study on fluid permeability using confocal fluorescence microscopy. J. Dent. Res. 1998, 77, 1749–1759. [Google Scholar] [CrossRef] [PubMed]
- Sauro, S.; Watson, T.F.; Thompson, I.; Toledano, M.; Nucci, C.; Banerjee, A. Influence of air-abrasion executed with PAA-bioglass 45S5 on the bonding performance of a resin-modified glass ionomer cement. Eur. J. Oral Sci. 2012, 120, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Brackett, M.G.; Agee, K.A.; Brackett, W.W.; Key, W.O.; Sabatini, C.; Kato, M.T.; Buzalaf, M.A.; Tjäderhane, L.; Pashley, D.H. Effect of sodium fluoride on theendogenous MMP activity of dentin matrices. J. Nat. Sci. 2015, 1, e118. [Google Scholar] [PubMed]
- Tezvergil-Mutluay, A.; Seseogullari-Dirihan, R.; Feitosa, V.P.; Cama, G.; Brauer, D.S.; Sauro, S. Effects of Composites Containing Bioactive Glasses on Demineralized Dentin. J. Dent. Res. 2017, 96, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Makowski, G.S.; Ramsby, M.L. Differential effect of calcium phosphate andcalcium pyrophosphate on binding of matrix metalloproteinases to fibrin: comparison to a fibrin-binding protease from inflammatory joint fluids. Clin. Exp. Immunol. 2004, 136, 176–187. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Main Groups Dentine Etching (10% PAA gel) | 24 h AS (CTR) | Load Cycling in AS (LC) | Load Cycling and 8-Month in AS (LC-AS) |
|---|---|---|---|
| No PAA (95/5) | 16.3 ± 5.9 (A1) | 16.4 ± 4.1 (A1) | 13.1 ± 4.6 (A1) |
| (5/25/70) | (2/10/88) | (10 */55 */35 *) | |
| Yes PAA (100/0) | 21.5 ± 4.8 (A1) | 21.1 ± 5.5 (A1) | 14.2 ± 5.2 (A2) |
| (0/15/85) | (3/17/80) | (13 */65 */22 *) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sauro, S.; Faus-Matoses, V.; Makeeva, I.; Nuñez Martí, J.M.; Gonzalez Martínez, R.; García Bautista, J.A.; Faus-Llácer, V. Effects of Polyacrylic Acid Pre-Treatment on Bonded-Dentine Interfaces Created with a Modern Bioactive Resin-Modified Glass Ionomer Cement and Subjected to Cycling Mechanical Stress. Materials 2018, 11, 1884. https://doi.org/10.3390/ma11101884
Sauro S, Faus-Matoses V, Makeeva I, Nuñez Martí JM, Gonzalez Martínez R, García Bautista JA, Faus-Llácer V. Effects of Polyacrylic Acid Pre-Treatment on Bonded-Dentine Interfaces Created with a Modern Bioactive Resin-Modified Glass Ionomer Cement and Subjected to Cycling Mechanical Stress. Materials. 2018; 11(10):1884. https://doi.org/10.3390/ma11101884
Chicago/Turabian StyleSauro, Salvatore, Vicente Faus-Matoses, Irina Makeeva, Juan Manuel Nuñez Martí, Raquel Gonzalez Martínez, José Antonio García Bautista, and Vicente Faus-Llácer. 2018. "Effects of Polyacrylic Acid Pre-Treatment on Bonded-Dentine Interfaces Created with a Modern Bioactive Resin-Modified Glass Ionomer Cement and Subjected to Cycling Mechanical Stress" Materials 11, no. 10: 1884. https://doi.org/10.3390/ma11101884