Oral Symptoms and Oral Health-Related Quality of Life in People with Rare Diseases in Germany: A Cross-Sectional Study

Abstract
:1. Introduction
2. Methods
2.1. Questionnaire
2.2. Participants
2.3. Data Source
2.4. Statistical Methods
3. Results
4. Discussion
4.1. Limitations
4.2. Interpretation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Regulation (EC) No 141/2000 of the European Parliament and of the Concil of 16 December 1999 on Orphan Medical Products. Available online: http://ec.europa.eu/health/files/eurdralex/vol.1/reg_2004141cons-2009-07/reg200141cons-2009-07en.pdf (accessed on 2 April 2018).
- European Commission on Rare Diseases. Available online: https://ec.europa.eu/health/rare_diseases/policy_en (accessed on 27 March 2018).
- Bundesministerium für Gesundheit. Prävention: Seltene Erkrankungen. 2013. Available online: http://www.bmg.bund.de/praevention/gesundheitsgefahren/selteneerkrankungen.html (accessed on 27 March 2018).
- Online Mendeline Inheritance of Man. Available online: https://www.omin.org (accessed on 2 April 2018).
- Jackowski, J.; Hanisch, M. Orofacial manifestations in 2006 rare diseases—A preliminary systematiy review of the literature. J. Ger. Soc. Dent. Oral Med. 2012, 67, D10. [Google Scholar]
- Hennekam, R.C.M.; Allanson, J.E.; Krantz, I.D.; Gorlin, R.J. Gorlin’s Syndromes of the Head and Neck, 5th ed.; Oxford University Press: New York, NY, USA, 2010. [Google Scholar]
- Hanisch, M.; Jung, S.; Kleinheinz, J. Oral Health-Related Quality of Life in Rare Diseases with Oral Manifestations. Gesundheitswesen 2018. [Google Scholar] [CrossRef]
- The Council of the European Union. Council Recommendation of 8 June 2009 on an Action in the Field of Rare Diseases (2009/C 151/02). Official Journal of the European Union. Available online: http://eur-lex.europe.eu/LEXUriServ.do?uri=OJ.C:2009:151:0007:0010:EN:PDF (accessed on 3 March 2018).
- Nationaler Aktionsplan für Menschen mit Seltenen Erkrankungen: Handlungsfelder, Empfehlungen und Maßnahmenvorschläge. BMG, BMBF, ACHSEe.V. 2013. Available online: http://www.namse.de/images/stories/Dokumente/Aktionsplan/national%20plan%20of %20action.pdf (accessed on 30 March 2018).
- Berglund, B.; Björck, E. Women with Ehlers-Danlos Syndrome Experience Low Oral Health-Related Quality of Life. J. Orofac. Pain 2012, 26, 307–314. [Google Scholar] [PubMed]
- Toupenay, S.; Razanamihaja, N.; Berdal, A.; Boy-Lefevre, M.L. Rare diseases with oral components: Care course and quality of life. Community Dent. Health 2013, 30, 10–14. [Google Scholar] [PubMed]
- Slade, G.D. Derivation and validation of a short-Form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef] [PubMed]
- John, M.T.; Micheelis, W. Mundgesundheitsbezogene Lebensqualität in der Bevölkerung: Grundlagen und Ergebnisse des OHIP aus einer repräsentativen Stichprobe in Deutschland. IDZ-Inf. 2003, 1, 1–28. [Google Scholar]
- Schmitt-Sausen, N. Tag der Seltenen Erkrankungen: Mehr Aufmerksamkeit für Waisenkinder der Medizin. Dtsch. Arztebl. 2010, 107, A-430/B-381/C-373. [Google Scholar]
- Hanisch, M.; Fröhlich, L.F.; Kleinheinz, J. Gingival hyperplasia as first sign of recurrence of granulomatosis with polyangiitis (Wegener´s granulomatosis): Case report and review of the literature. BMC Oral Health 2017, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- John, M.T.; Miglioretti, D.L.; LeResche, L.; Koepsell, T.D.; Hujoel, P.; Micheelis, W. German short forms of the Oral Health Impact Profile. Community Dent. Oral Epidemiol. 2006, 34, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Janssen, J.; Laatz, W. Statistische Analyse mit SPSS-Eine Anwendungsorientierte Einführung in das Basissystem und das Modul Exakte Tests; Springer: Berlin/Heidelberg, Germany, 2017; p. 281. ISBN 978-3-662-534779. [Google Scholar]
- List of Rare Diseases and Synonyms in Alphabetical Order. January 2018 Version. Available online: http://www.orpha.net/consor4.01/www/cgibin/Education_Home.php?lng=DE#REPORT_RARE_DISEASES (accessed on 28 March 2018).
- John, M.T.; Micheelis, W.; Biffar, R. Norrmwerte Mundgesundheitsbezogener Lebensqualität für Kurzversionen des OHIP. Schweiz. Monatsschr. Zahnmed. 2004, 114, 784–791. [Google Scholar] [PubMed]
- Bogart, K.R.; Irvin, V.L. Health-realted quality of life among adults with diverse rare disorders. Orphanet J. Rare Dis. 2017, 12, 177. [Google Scholar] [CrossRef] [PubMed]
- Wetterauer, B.; Schuster, R. Seltene Krankheiten: Probleme, Stand und Entwicklung der nationalen und europäischen Forschungsförderung. Bundesgesundheitsblatt 2008, 51, 519. [Google Scholar] [CrossRef] [PubMed]
- Rare Diseases: Understanding this Public Health Priority. Available online: https://www.eurordis.org/IMG/pdf/princeps_document-EN.pdf (accessed on 29 March 2018).
- Reissmann, D.R.; Sierwald, I.; Heydecke, G.; John, M.T. Interpreting one oral health impact profile point. Health Qual. Life Outcomes 2013, 11, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabolli, S.; Bergamo, F.; Alessandroni, L.; Di Pietro, C.; Sampogna, F.; Abeni, D. Quality of Life and psychological problems of patients with oral mucosal disease in dermatological practice. Dermatology 2009, 218, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Fine, J.D. Inherited epidermolysis bullosa. Orphanet J. Rare Dis. 2010, 5, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faekonja, A. Prevalence of dental developmental anomalies of permanent teeth in children and their influence on esthetics. J. Esthet. Restor. Dent. 2017, 29, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Samorodnitzky-Naveh, G.R.; Geiger, S.B.; Levin, L. Patients satisfaction with dental esthetics. J. Dent. 2012, 40, 624–631. [Google Scholar] [CrossRef]
- Lundgren, G.P.; Karsten, A.; Dahllöf, G. Oral health-related quality of life beforeand after crown therapy in young patients with amelogenesis imperfect. Health Qual. Life Outcomes 2015, 13, 197. [Google Scholar] [CrossRef] [PubMed]
- Hausamen, J.E.; Machtens, E.; Reuther, J.F.; Eufinger, H.; Kübler, A.; Schliephake, H. Mund-Kiefer-Gesichtschirurgie-Operationslehre und Atlas, 4th ed.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 309–364. ISBN 978-3-642-17801-6. [Google Scholar]
- Sharma, G.; Nagpal, A. Oral health considerations in a patient with oligosymptomatic ectrodactyly-ectodermal dysplasia-cleft syndrome. Gen. Dent. 2017, 65, 66–69. [Google Scholar] [PubMed]
- Terheyden, H.; Wüsthoff, F. Occlusal rehabilitation in patients with congenitally missing teeth-dental implants, conventional prosthetics, tooth autotransplants, and preservation of deciduous teeth-a systematic review. Int. J. Implant Dent. 2015, 1, 30. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.R.; Lindner, I.; Fickl, S. Implant treatment in periodontally compromised subjety-quality of life and patient satisfaction. Clin. Oral Investig. 2016, 20, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Filius, M.A.; Vissink, A.; Cune, M.S.; Raghoebar, G.M.; Visser, A. Long-term implant performance and patients’ satisfaction in oligodontia. J. Dent. 2018, 71, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Hashem, A.; Kelly, A.; O’Connell, B.; O’Sullivan, M. Impact of moderate and severe hypodontia and amelogenesis imperfecta on quality of life and self-esteem of adult patients. J. Dent. 2013, 41, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Stelzle, F.; Rohde, M.; Oetter, N.; Krug, K.; Riemann, M.; Adler, W.; Neukam, F.W.; Knipfer, C. Gingival esthetics and oral health-related quality of life in patients with cleft lip and palate. Int. J. Oral Maxillofac. Surg. 2017, 46, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Shueb, S.S.; Nixdorf, D.R.; John, M.T.; Alonso, B.F.; Durham, J. What is the impact of acute and chronic orofacial pain on quality of life? J. Dent. 2015, 43, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Lemos, G.A.; Paulino, M.R.; Forte, F.D.S.; Beltrão, R.T.S.; Batista, A.U.D. Influence of temporomandibular disorder presence an severity on oral- health- related Quality of Life. Rev. Dor 2015, 16, 10–14. [Google Scholar] [CrossRef]
- Niklander, S.; Veas, L.; Barrera, C.; Fuentes, F.; Chiappini, G. Marshall, M. Risk factors, hyposalivation and impact of xerostomia on oral health-related quality of life. Braz. Oral Res. 2017, 31, e14. [Google Scholar] [CrossRef] [PubMed]
- Xin, W.; Leung, K.C.M.; Lo, E.C.M.; Mok, M.Y.; Leung, M.H. A randomized, double-blind, placebo-controlled clinical trial of fluoride varnish in preventing dental caries of Sjögren’s syndrome patients. BMC Oral Health 2016, 16, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, L.; Wong, H.M.; McGrath, C.P.; Sun, L.; Wong, H.M. Relationship between the Severity of Malocclusion and Oral Health Related Quality of Life: A Systematic Review and Meta-analysis. Oral Health Prev. Dent. 2017, 15, 503–517. [Google Scholar] [PubMed]
- Drążewski, D.; Grzymisławska, M.; Korybalska, K.; Czepulis, N.; Grzymisławski, M.; Witowski, J.; Surdacka, A. Oral Health Status of Patients with Lysosomal Storage Diseases in Poland. Int. J. Environ. Res. Public Health 2017, 14, 281. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Name of Disease | OMIM Number | Number of Individuals |
|---|---|---|
| Marfan Syndrome | 154700 | 51 |
| Ectodermal Dysplasia | 305100 | 46 |
| Achalasia | 231550 | 44 |
| Sarcoidosis | 181000 | 36 |
| Ehlers–Danlos Syndrome | 120180 | 32 |
| Lymphangioleiomyomatosis | 606690 | 17 |
| Alpha-1-Antitrypsin Deficiency | 613490 | 15 |
| Syringomyelia | 118420 | 13 |
| X-linked Hypophosphatemia | 307800 | 13 |
| Symptoms | Prevalence (%) |
|---|---|
| Anomalies of the Tooth Formation | 24.4 |
| Dysgnathia | 18.4 |
| Changes in Number of the Teeth | 13.6 |
| Malocclusion | 12.4 |
| Oral Mucosa Disease | 9.5 |
| Mineralization Disorders of the Hard Tissue of the Teeth | 9.3 |
| Temperomandibular Dysfunction | 5.4 |
| Disease of the Periodontium | 5.4 |
| Vegetative Disorders | 3.1 |
| Neurological Disease | 2.1 |
| Cleft Lip and Palate | 1.7 |
| Microstomia | 1.2 |
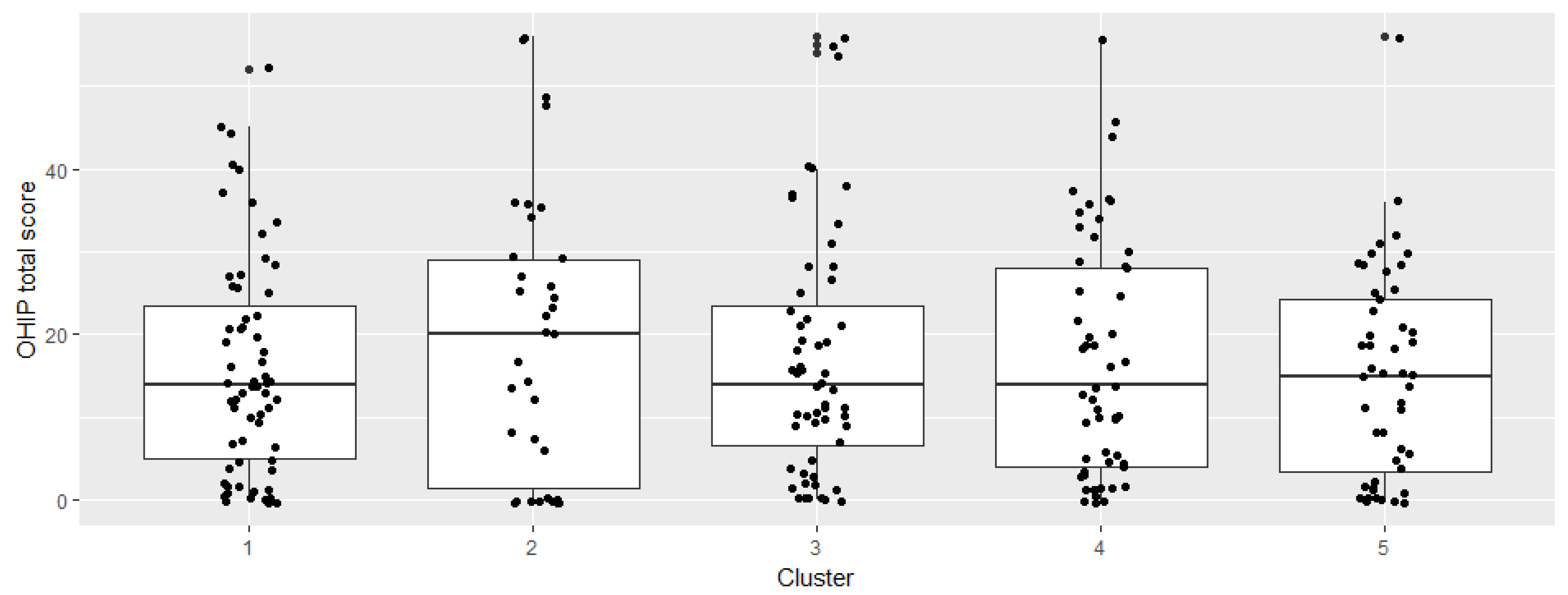
| Clusters | Symptom Prevalence in Each Cluster (%) | Number of Individuals in Each Cluster | OHIP Mean (Minimum; Maximum) | OHIP Standard Deviation |
|---|---|---|---|---|
| Cluster 1 | Anomalies of the Tooth Formation: 98% Mineralization Disorders of the Hard Tissue of the Teeth: 70% | 63 | 15.9 (0;52) | 13.1 |
| Cluster 2 | Oral Mucosa Disease: 83% Disease of the Periodontium: 34% Microstomia: 14% | 35 | 19.7 (0;56) | 17.1 |
| Cluster 3 | Changes in the Number of the Teeth: 100% Anomalies of the Tooth Formation: 96% Cleft Lip/Palate: 7% | 56 | 16.9 (0;56) | 14.5 |
| Cluster 4 | Temporomandibular Dysfunctions: 31% Vegetative Disorders: 16% Neurological Diseases: 15% | 55 | 16.9 (0;56) | 14.3 |
| Cluster 5 | Dysgnathia: 100% Malocclusion: 54% | 48 | 15.1 (0;56) | 12.4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiemann, S.; Frenzel Baudisch, N.; Jordan, R.A.; Kleinheinz, J.; Hanisch, M. Oral Symptoms and Oral Health-Related Quality of Life in People with Rare Diseases in Germany: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1493. https://doi.org/10.3390/ijerph15071493
Wiemann S, Frenzel Baudisch N, Jordan RA, Kleinheinz J, Hanisch M. Oral Symptoms and Oral Health-Related Quality of Life in People with Rare Diseases in Germany: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2018; 15(7):1493. https://doi.org/10.3390/ijerph15071493
Chicago/Turabian StyleWiemann, Sabrina, Nicolas Frenzel Baudisch, Rainer A. Jordan, Johannes Kleinheinz, and Marcel Hanisch. 2018. "Oral Symptoms and Oral Health-Related Quality of Life in People with Rare Diseases in Germany: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 15, no. 7: 1493. https://doi.org/10.3390/ijerph15071493