
Increase in Suicide Rates by Hanging in the Population of Tabasco, Mexico between 2003 and 2012

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
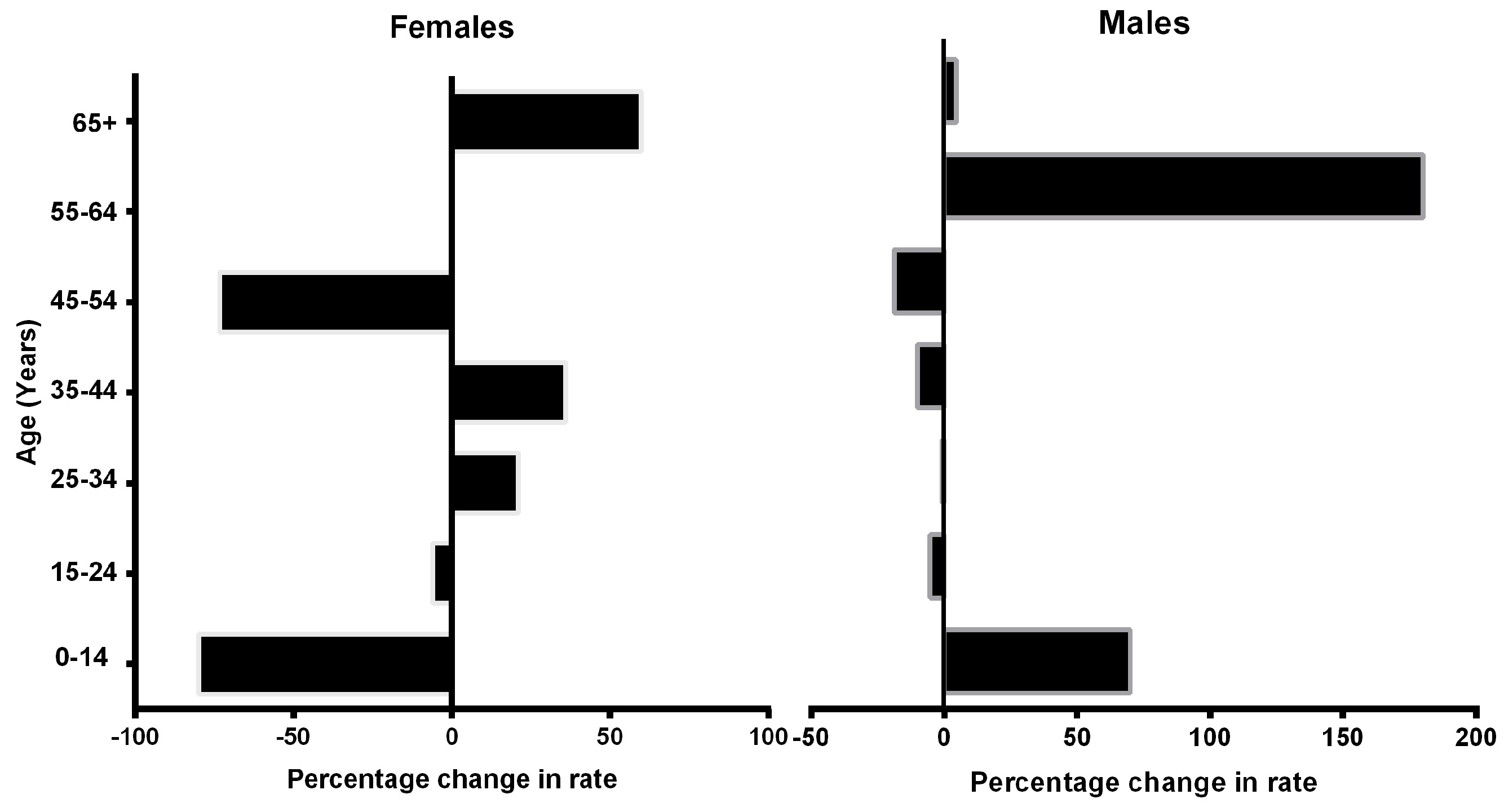
3.1. Suicide and Age Group
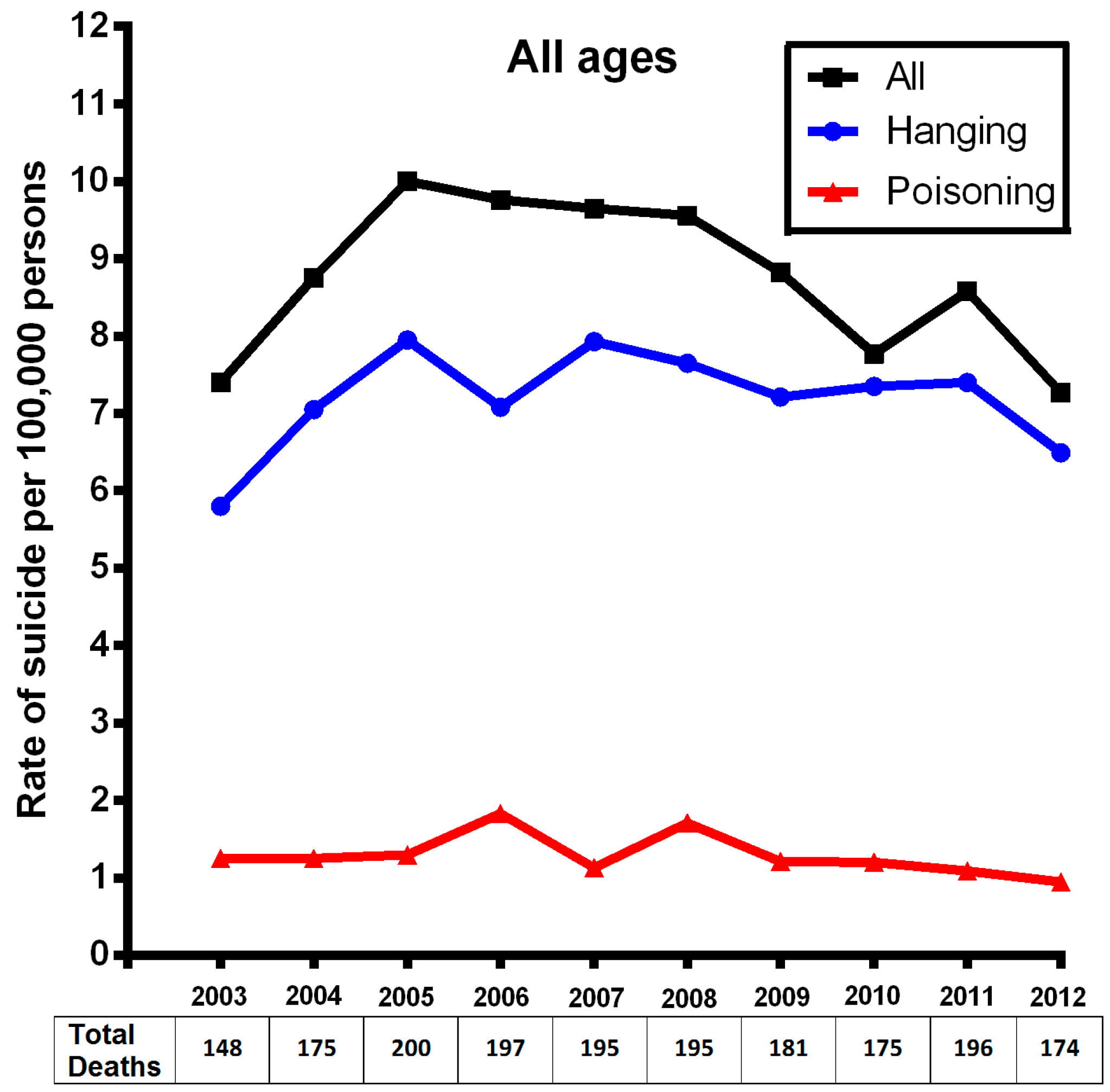
3.2. Suicide and Suicide Method
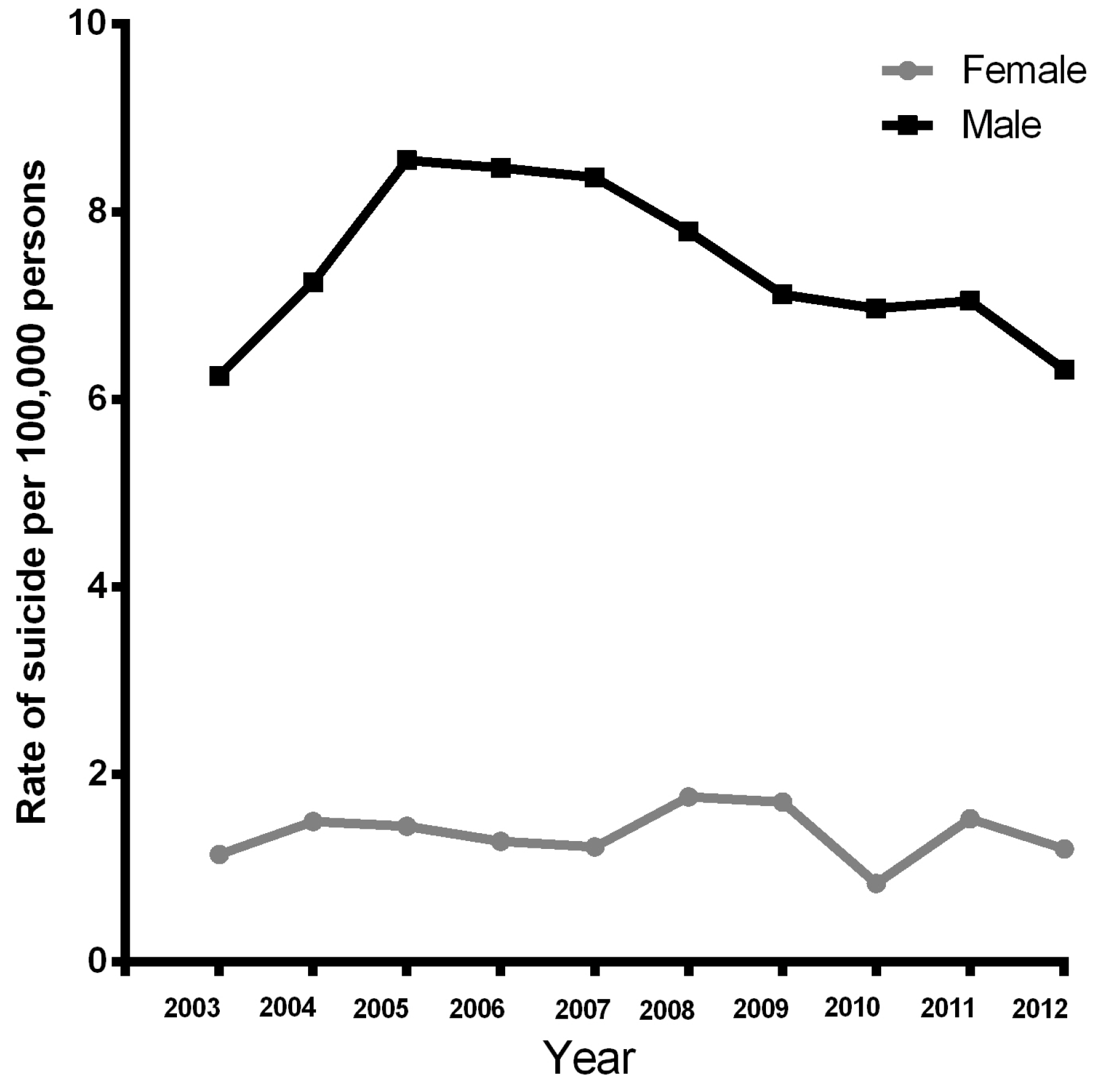
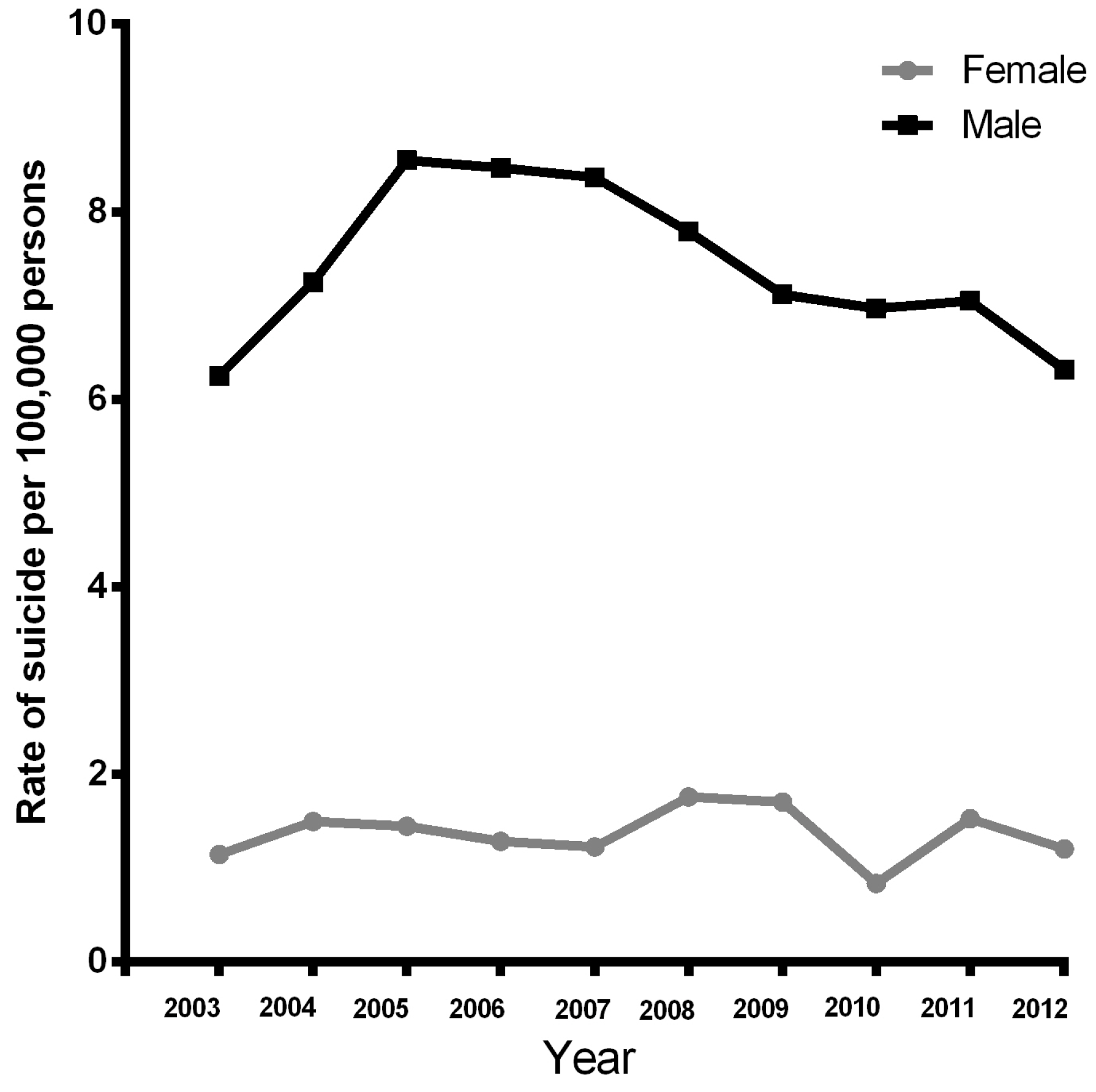
3.3. Suicide by Gender
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ICD | International Classification of Diseases and Related Health Problems |
| WISQARS | Web-Based Injury Statics Query and Reporting System |
| INEGI | National Institute of Statistics and Geography in Spanish |
| CONAPO | National Council of Population in Spanish |
References
- Gonzalez-Castro, T.B.; Juarez-Rojop, I.; Lopez-Narvaez, M.L.; Tovilla-Zarate, C.A. Association of TPH-1 and TPH-2 gene polymorphisms with suicidal behavior: A systematic review and meta-analysis. BMC Psychiatry 2014, 14, 196. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Castro, T.B.; Tovilla-Zarate, C.; Juarez-Rojop, I.; Pool Garcia, S.; Velazquez-Sanchez, M.P.; Genis, A.; Nicolini, H.; Lopez Narvaez, L. Association of the 5HTR2A gene with suicidal behavior: Case-control study and updated meta-analysis. BMC Psychiatry 2013, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, Z.; Sun, L.; Wu, H.; Sun, Y. Risk and risk factors of suicide attempt after first onset of suicide ideation: Findings from medical students in grades 1 and 2. Wei Sheng Yan Jiu 2014, 43, 47–53. [Google Scholar] [PubMed]
- Zhang, W.C.; Jia, C.X.; Zhang, J.Y.; Wang, L.L.; Liu, X.C. Negative life events and attempted suicide in rural China. PLoS ONE 2015, 10, e0116634. [Google Scholar] [CrossRef] [PubMed]
- Bland, P. Identifying which patients are at risk of suicide. Practitioner 2014, 258, 7. [Google Scholar] [PubMed]
- Cardona, D.; Segura, A.M.; Espinosa, A.; Segura, A. Homicide and suicide in 15 to 24 year-old people in Colombia, 1998–2008. Biomed. Rev. Inst. Nac. Salud 2013, 33, 574–586. [Google Scholar]
- Wolodzko, T.; Kokoszka, A. Classification of persons attempting suicide. A review of cluster analysis research. Psychiatr. Pol. 2014, 48, 823–834. [Google Scholar] [PubMed]
- Alvarado-Esquivel, C.; Sanchez-Anguiano, L.F.; Arnaud-Gil, C.A.; Hernandez-Tinoco, J.; Molina-Espinoza, L.F.; Rabago-Sanchez, E. Socio-demographic, clinical and behavioral characteristics associated with a history of suicide attempts among psychiatric outpatients: A case control study in a northern Mexican city. Int. J. Biomed. Sci. 2014, 10, 61–68. [Google Scholar] [PubMed]
- Borges, G.; Orozco, R.; Benjet, C.; Medina-Mora, M.E. Suicide and suicidal behaviors in Mexico: Retrospective and current status. Salud Publ. Mex. 2010, 52, 292–304. [Google Scholar]
- Fazel, S.; Wolf, A.; Palm, C.; Lichtenstein, P. Violent crime, suicide, and premature mortality in patients with schizophrenia and related disorders: A 38-year total population study in Sweden. Lancet Psychiatry 2014, 1, 44–54. [Google Scholar] [CrossRef]
- Sinniah, A.; Maniam, T.; Oei, T.P.; Subramaniam, P. Suicide attempts in Malaysia from the year 1969 to 2011. Sci. World J. 2014, 2014, 718367. [Google Scholar] [CrossRef] [PubMed]
- Tahir, M.N.; Akbar, A.H.; Naseer, R.; Khan, Q.O.; Khan, F.; Yaqub, I. Suicide and attempted suicide trends in Mianwali, Pakistan: Social perspective. East. Mediterr. Health J. 2014, 19 (Suppl. S3), S111–S114. [Google Scholar] [PubMed]
- Bridge, J.A.; Greenhouse, J.B.; Sheftall, A.H.; Fabio, A.; Campo, J.V.; Kelleher, K.J. Changes in suicide rates by hanging and/or suffocation and firearms among young persons aged 10–24 years in the United States: 1992–2006. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2010, 46, 503–505. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.P.; Hu, G.; Wilcox, H.C.; Baker, T.D. Increase in suicide by hanging/suffocation in the U.S., 2000–2010. Am. J. Prev. Med. 2013, 44, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Fond, G.; Llorca, P.M.; Boucekine, M.; Zendjidjian, X.; Brunel, L.; Lancon, C.; Auquier, P.; Boyer, L. Disparities in suicide mortality trends between United States of America and 25 European countries: Retrospective analysis of who mortality database. Sci. Rep. 2016, 6, 20256. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Navarro, P.; Barrigon, M.L.; Lopez-Castroman, J.; Sanchez-Alonso, M.; Paramo, M.; Serrano, M.; Arrojo, M.; Baca-Garcia, E. Suicide mortality trends in Galicia, Spain and their relationship with economic indicators. Epidemiol. Psychiatr. Sci. 2015, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Ornelas, R.A.; Cardiel-Téllez, L. El suicidio y su tendencia social en México: 1990–2011. Pap. Poblac. 2013, 19, 205–229. [Google Scholar]
- Park, C.; Jee, Y.H.; Jung, K.J. Age-period-cohort analysis of the suicide rate in Korea. J. Affect. Disord. 2016, 194, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Nino, J.A.; Astudillo-Garcia, C.I.; Bojorquez-Chapela, I.; Morales-Carmona, E.; Montoya-Rodriguez, A.A.; Palacio-Mejia, L.S. The mexican cycle of suicide: A national analysis of seasonality, 2000–2013. PLoS ONE 2016, 11, e0146495. [Google Scholar] [CrossRef] [PubMed]
- Ajdacic-Gross, V.; Weiss, M.G.; Ring, M.; Hepp, U.; Bopp, M.; Gutzwiller, F.; Rossler, W. Methods of suicide: International suicide patterns derived from the WHO mortality database. Bull. World Health Organ. 2008, 86, 726–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loh, C.; Tai, B.C.; Ng, W.Y.; Chia, A.; Chia, B.H. Suicide in young Singaporeans aged 10–24 years between 2000 to 2004. Arch. Suicide Res. Off. J. Int. Acad. Suicide Res. 2012, 16, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Cervantes, F.S.; Serrano-González, R.E.; Márquez-Caraveo, M.E. Suicidios en menores de 20 años. México 1998–2011. Salud Ment. 2015, 38, 379–389. [Google Scholar] [CrossRef]
- National Vital Statistics System, National Center for Health Statistics, CDC. 10 Leadings Causes of Death by Age Group, United States—2012. Available online: http://www.cdc.gov/injury/wisqars/pdf/leading_causes_of_death_by_age_group_2012-a.pdf (accessed on 10 February 2016).
- Kann, L.; Kinchen, S.; Shanklin, S.L.; Flint, K.H.; Kawkins, J.; Harris, W.A.; Lowry, R.; Olsen, E.O.; McManus, T.; Chyen, D.; et al. Youth risk behavior surveillance—United States, 2013. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2014, 63 (Suppl. S4), 1–168. [Google Scholar]
- Soor, G.S.; Vukin, I.; Bridgman-Acker, K.; Marble, R.; Barnfield, P.; Edwards, J.; Cooper, B.; Alfonsi, J.; Hunter, J.; Banayan, D.J.; et al. The effects of gender on adolescent suicide in Ontario, Canada. J. Can. Acad. Child Adolesc. Psychiatry 2012, 21, 179–185. [Google Scholar] [PubMed]
- Sinyor, M.; Schaffer, A.; Streiner, D.L. Characterizing suicide in Toronto: An observational study and cluster analysis. Can. J. Psychiatry 2014, 59, 26–33. [Google Scholar] [PubMed]
- Ilic, M.; Ilic, I. Suicide in Serbia. J. Affect. Disord. 2016, 193, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and suicidal behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Castro, T.B.; Hernandez-Diaz, Y.; Tovilla-Zarate, C.A.; Gonzalez-Gutierrez, K.P.; Fresan, A.; Juarez-Rojop, I.E.; Lopez-Narvaez, L.; Villar Soto, M.; Genis, A. Differences by gender in completed suicides in a Mexican population: A psychological autopsy study. J. Forensic Leg. Med. 2016, 38, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.V.; Lester, D. Suicide: Closing the Exits; Transaction Publishers: Piscataway, NJ, USA, 2013. [Google Scholar]
- Kosky, R.J.; Dundas, P. Death by hanging: implications for prevention of an important method of youth suicide. Aust. N. Z. J. Psychiatry 2000, 34, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.T.; Hawton, K.; Lee, C.T.; Chen, T.H. The influence of media reporting of the suicide of a celebrity on suicide rates: A population-based study. Int. J. Epidemiol. 2007, 36, 1229–1234. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Method | 2003 n = 148 | 2012 n = 174 | Percentage Change in Rate |
|---|---|---|---|---|
| All | All | 7.40 | 7.53 | 1.75 |
| Hanging | 5.80 | 6.49 | 11.89 | |
| Poisoning | 1.25 | 0.95 | −24 | |
| Firearm | 0.25 | 0.08 | −68 | |
| 0–14 | All | 0.3 | 0.21 | −30 |
| Hanging | 0.25 | 0.21 | −16 | |
| Poisoning | 0.05 | 0 | −100 | |
| Firearm | 0 | 0 | 0 | |
| 15–24 | All | 2.6 | 2.46 | −5.38 |
| Hanging | 2.15 | 2.20 | 2.32 | |
| Poisoning | 0.3 | 0.25 | −16.6 | |
| Firearm | 0.1 | 0.0 | −100 | |
| 25–34 | All | 1.3 | 1.51 | 15.26 |
| Hanging | 1.1 | 1.47 | 33.63 | |
| Poisoning | 0.15 | 0.04 | −73.3 | |
| Firearm | 0 | 0 | 0 | |
| 35–44 | All | 1.45 | 1.42 | −2.06 |
| Hanging | 1.0 | 1.08 | 8 | |
| Poisoning | 0.45 | 0.30 | −33.33 | |
| Firearm | 0 | 0.04 | ||
| 45–54 | All | 1.05 | 0.77 | −30 |
| Hanging | 0.7 | 0.64 | −14.2 | |
| Poisoning | 0.2 | 0.12 | −50 | |
| Firearm | 0.1 | 0 | −100 | |
| 55–64 | All | 0.2 | 0.56 | 180 |
| Hanging | 0.15 | 0.43 | 186.66 | |
| Poisoning | 0.05 | 0.08 | 60 | |
| Firearm | 0 | 0.04 | ||
| ≥65 | All | 0.50 | 0.56 | 12 |
| Hanging | 0.40 | 0.40 | 0 | |
| Poisoning | 0.05 | 0.12 | 140 | |
| Firearm | 0 | 0 | 0 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Alvarado, M.M.; González-Castro, T.B.; Tovilla-Zárate, C.A.; Fresán, A.; Juárez-Rojop, I.E.; López-Narváez, M.L.; Villar-Soto, M.; Genis-Mendoza, A. Increase in Suicide Rates by Hanging in the Population of Tabasco, Mexico between 2003 and 2012. Int. J. Environ. Res. Public Health 2016, 13, 552. https://doi.org/10.3390/ijerph13060552
Hernández-Alvarado MM, González-Castro TB, Tovilla-Zárate CA, Fresán A, Juárez-Rojop IE, López-Narváez ML, Villar-Soto M, Genis-Mendoza A. Increase in Suicide Rates by Hanging in the Population of Tabasco, Mexico between 2003 and 2012. International Journal of Environmental Research and Public Health. 2016; 13(6):552. https://doi.org/10.3390/ijerph13060552
Chicago/Turabian StyleHernández-Alvarado, Mervyn Manuel, Thelma Beatriz González-Castro, Carlos Alfonso Tovilla-Zárate, Ana Fresán, Isela E. Juárez-Rojop, María Lilia López-Narváez, Mario Villar-Soto, and Alma Genis-Mendoza. 2016. "Increase in Suicide Rates by Hanging in the Population of Tabasco, Mexico between 2003 and 2012" International Journal of Environmental Research and Public Health 13, no. 6: 552. https://doi.org/10.3390/ijerph13060552