
Sensitization Rates for Various Allergens in Children with Allergic Rhinitis in Qingdao, China

Abstract
:1. Introduction
2. Methods
2.1. Study Subjects
2.2. Skin Prick Test (SPT)
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Population
3.2. Leading Allergens Causing AR

{kind=link}
| Allergens | Total Patients (N) | % | Age 3–5 years (N) | % | Age > 6 years (N) | % | Chis-Quare (χ2) | p Value | |
|---|---|---|---|---|---|---|---|---|---|
| Inhaled | Dermatophagoides farinae | 1887 | 66.4 | 634 | 62.5 | 1253 | 70.8 | 22.271 | <0.01 |
| Dermatophagoides pteronyssinus | 1978 | 69.6 | 688 | 67.5 | 1290 | 72.0 | 6.564 | <0.05 | |
| Mould type 1 (Penicillium notatum) | 1109 | 39 | 386 | 36.4 | 723 | 42.0 | 9.276 | <0.01 | |
| Mould type 2 (Aspergillus fumigatus) | 900 | 31.7 | 294 | 29.3 | 606 | 34.3 | 8.079 | <0.01 | |
| Late spring flower | 1076 | 37.9 | 371 | 36.3 | 705 | 39.6 | 3.206 | >0.05 | |
| Summer autumn flower | 544 | 19.1 | 207 | 20.6 | 337 | 17.5 | 4.327 | <0.05 | |
| Weeds | 686 | 24.1 | 235 | 23.1 | 451 | 25.3 | 1.781 | >0.05 | |
| Ragweed | 618 | 21.8 | 207 | 20.3 | 411 | 23.4 | 4.124 | <0.05 | |
| Latex | 690 | 24.3 | 217 | 20.7 | 473 | 28.3 | 21.817 | <0.01 | |
| Gramineae | 712 | 25.1 | 228 | 22.4 | 484 | 28.0 | 11.987 | <0.01 | |
| Ingested | Shrimp | 1030 | 36.3 | 385 | 34.5 | 645 | 38.6 | 5.3 | <0.05 |
| Mussels | 1113 | 39.2 | 432 | 40.0 | 681 | 38.7 | 0.477 | >0.05 | |
| Carp | 1038 | 36.5 | 386 | 34.7 | 654 | 39.0 | 5.724 | <0.05 | |
| Milk | 708 | 24.9 | 270 | 25.2 | 438 | 24.8 | 0.061 | >0.05 | |
| Egg | 616 | 21.7 | 231 | 21.5 | 385 | 22.1 | 0.120 | >0.05 | |
| Peanut | 643 | 22.6 | 241 | 22.4 | 402 | 23.1 | 0.201 | >0.05 | |
| Peach | 579 | 20.4 | 199 | 20.2 | 380 | 20.8 | 0.188 | >0.05 | |
| Eel | 198 | 6.97 | 94 | 8.1 | 104 | 5.7 | 6.237 | <0.05 | |
| Hemp | 169 | 5.95 | 56 | 6.5 | 113 | 5.4 | 1.296 | >0.05 | |
| Sea crab | 43 | 1.51 | 12 | 1.0 | 31 | 2.1 | 5.474 | <0.05 |
3.3. Comparison of Allergen Sensitizations between Groups with Different Ages
3.4. Comparison of Allergen Sensitization by Sex
| Allergens | Males (N) | % | Females (N) | % | Chi-Square (χ2) | p Value | |
|---|---|---|---|---|---|---|---|
| Inhaled | Dermatophagoides farinae | 1205 | 67.6 | 682 | 64.4 | 3.088 | >0.05 |
| Dermatophagoides pteronyssinus | 1263 | 70.9 | 715 | 67.5 | 3.543 | >0.05 | |
| Mould type 1 (Penicillium notatum) | 724 | 40.6 | 385 | 36.4 | 5.097 | <0.05 | |
| Mould type 2 (Aspergillus fumigatus) | 584 | 32.8 | 316 | 29.8 | 2.640 | >0.05 | |
| Late spring flower | 681 | 18.5 | 395 | 37.3 | 0.237 | >0.05 | |
| Summer autumn flower | 338 | 38.2 | 206 | 19.5 | 0.101 | >0.05 | |
| Weeds | 445 | 25.0 | 241 | 22.8 | 1.779 | >0.05 | |
| Ragweed | 410 | 23.0 | 208 | 19.6 | 4.423 | <0.05 | |
| Latex | 461 | 25.9 | 229 | 21.6 | 6.511 | <0.05 | |
| Gramineae | 439 | 24.6 | 273 | 25.8 | 0.463 | >0.05 | |
| Ingested | Shrimp | 655 | 36.8 | 375 | 35.4 | 0.520 | >0.05 |
| Mussels | 692 | 38.8 | 421 | 39.8 | 0.237 | >0.05 | |
| Carp | 642 | 36.0 | 396 | 37.4 | 0.535 | >0.05 | |
| Milk | 398 | 22.3 | 310 | 29.3 | 17.091 | <0.01 | |
| Egg | 388 | 21.8 | 228 | 21.5 | 0.023 | >0.05 | |
| Peanut | 408 | 22.9 | 235 | 22.2 | 0.188 | >0.05 | |
| Peach | 363 | 20.4 | 216 | 20.4 | 0 | >0.05 | |
| Eel | 120 | 6.7 | 78 | 9.5 | 1.788 | >0.05 | |
| Hemp | 105 | 5.9 | 64 | 6.0 | 0.027 | >0.05 | |
| Sea crab | 26 | 1.5 | 17 | 7.4 | 0.408 | >0.05 |
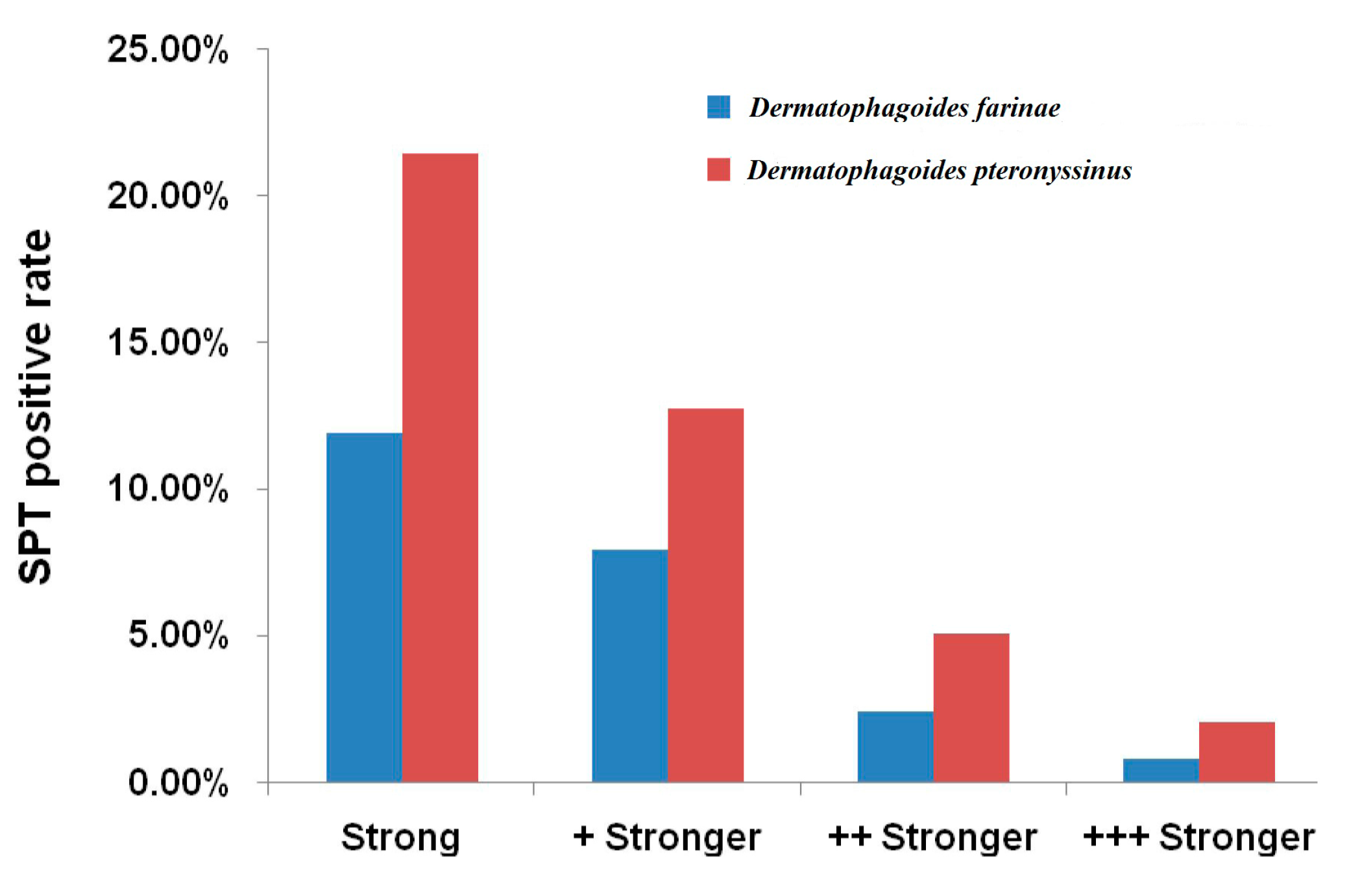
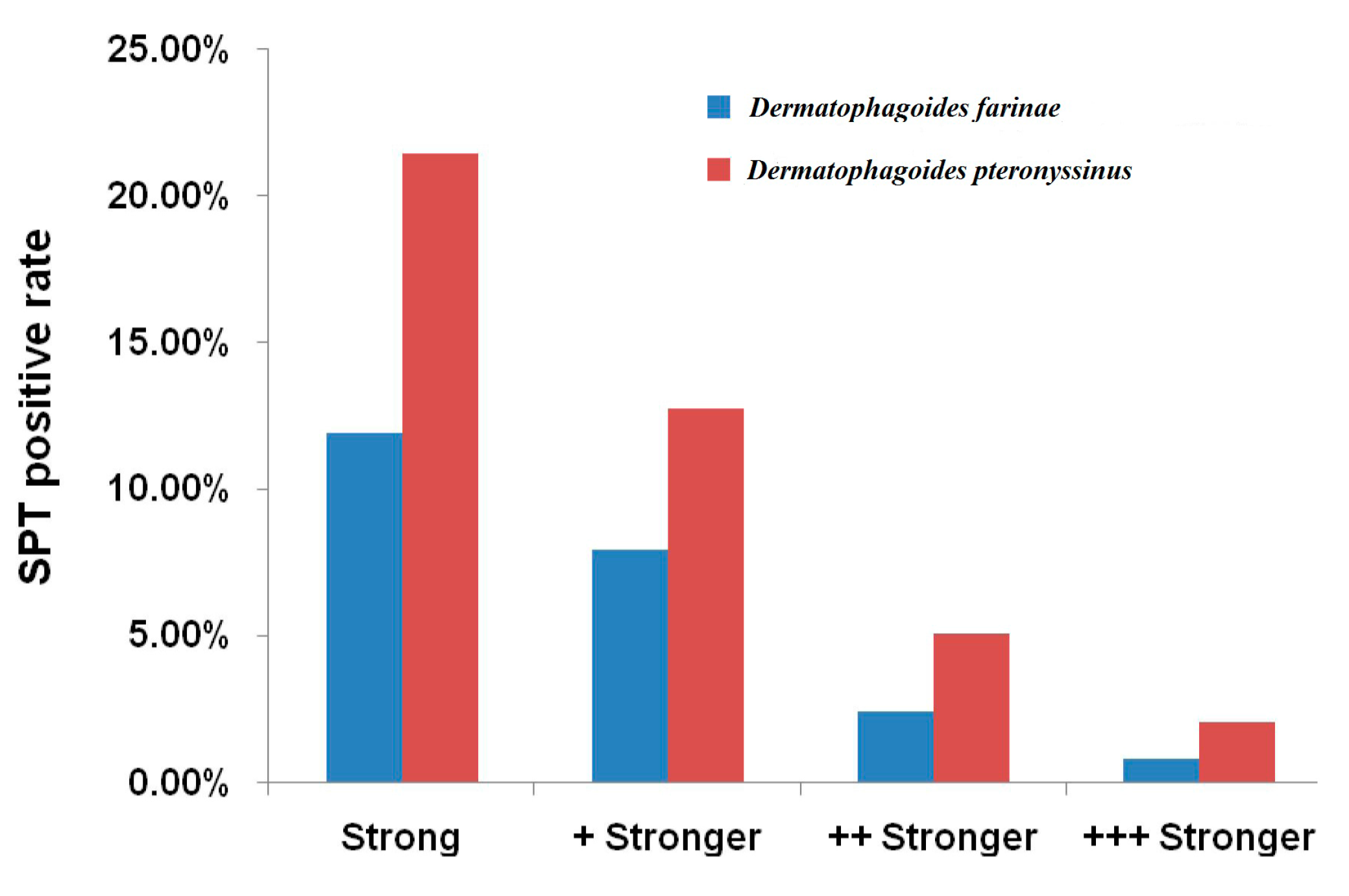
3.5. Comparison of the Intensity of Sensitization to Mite Allergen
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Seidman, M.D.; Gurgel, R.K.; Lin, S.Y.; Schwartz, S.R.; Baroody, F.M.; Bonner, J.R.; Dawson, D.E.; Dykewicz, M.S.; Hackell, J.M.; Han, J.K.; et al. Clinical practice guideline: Allergic rhinitis executive summary. Otolaryngol. Head Neck Surg. 2015, 152, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Meadows, A.; Kaambwa, B.; Novielli, N.; Huissoon, A.; Fry-Smith, A.; Meads, C.; Barton, P.; Dretzke, J. A systematic review and economic evaluation of subcutaneous and sublingual allergen immunotherapy in adults and children with seasonal allergic rhinitis. Health Technol. Assess. 2013, 17. [Google Scholar] [CrossRef] [PubMed]
- Aït-Khaled, N.; Pearce, N.; Anderson, H.R.; Ellwood, P.; Montefort, S.; Shah, J.; the ISAAC Phase Three Study Group. Global map of the prevalence of symptoms of rhinoconjunctivitis in children: The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three. Allergy 2009, 64, 123–148. [Google Scholar] [CrossRef] [PubMed]
- Tamay, Z.; Akcay, A.; Ergin, A.; Guler, N. Prevalence of allergic rhinitis and risk factors in 6- to 7-year-old children in Istanbul, Turkey. Turk. J. Pediatr. 2014, 56, 31–40. [Google Scholar] [PubMed]
- Sedaghat, A.R.; Phipatanakul, W.; Cunningham, M.J. Prevalence of and associations with allergic rhinitis in children with chronic rhinosinusitis. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.M.; Zhang, J.; Liu, S.L.; Zhang, X.; Yang, S.N.; Gao, J.; Zhao, J.; Chen, H.; Chen, X.X.; Sun, F.X.; et al. Prevalence and associated risk factors of allergic rhinitis in preschool children in Beijing. Laryngoscope 2013, 123, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Bedolla-Barajas, M.; Cuevas-Rios, G.; Garcia-Barboza, E.; Barrera-Zepeda, A.T.; Morales-Romero, J. Prevalence and associated factors to allergic rhinitis in school children of ciudad Guzman, Mexico. Rev. Invest. Clin. 2010, 62, 244–251. [Google Scholar] [PubMed]
- Volkov, A.G.; Chepurnaia, M.M.; Marugin, I.V. Allergic rhinitis in children as a risk factor of bronchial asthma. Vestn. Otorinolaringol. 2010, 4, 33–34. [Google Scholar] [PubMed]
- Bogacka, E.; Nittner-Marszalska, M.; Fal, A.M.; Kuzniar, J.; Nikiel, E.; Malolepszy, J. Allergy to mould allergens as a risk factor for bronchial asthma in patients suffering from allergic rhinitis. Pol. Merkur. Lekarski 2003, 14, 388–392. [Google Scholar] [PubMed]
- Kim, J.S.; Ouyang, F.; Pongracic, J.A.; Fang, Y.; Wang, B.; Liu, X.; Xing, H.; Caruso, D.; Liu, X.; Zhang, S.; et al. Dissociation between the prevalence of atopy and allergic disease in rural China among children and adults. J. Allergy Clin. Immunol. 2008, 122, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Feleszko, W.; Ruszczynski, M.; Jaworska, J.; Strzelak, A.; Zalewski, B.M.; Kulus, M. Environmental tobacco smoke exposure and risk of allergic sensitisation in children: A systematic review and meta-analysis. Arch. Dis. Child. 2014, 99, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.Q.; Chen, D.H.; Zheng, P.Y.; Huang, H.M.; Luo, W.T.; Zeng, G.Q.; Zhang, X.W. Allergy-related evidences in relation to serum ige: Data from the china state key laboratory of respiratory disease, 2008–2013. Biomed. Environ. Sci. 2014, 27, 495–505. [Google Scholar] [PubMed]
- Panzner, P.; Malkusova, I.; Vachova, M.; Liska, M.; Brodska, P.; Ruzickova, O.; Maly, M. Bronchial inflammation in seasonal allergic rhinitis with or without asthma in relation to natural exposure to pollen allergens. Allergol. Immunopathol. (Madr) 2015, 43, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Trebuchon, F.; Lheritier-Barrand, M.; David, M.; Demoly, P. Characteristics and management of sublingual allergen immunotherapy in children with allergic rhinitis and asthma induced by house dust mite allergens. Clin. Transl. Allergy 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Li, W.; Di, R.; Wang, J.; Hu, P.; Ji, P. Prevalence of sensitization to allergens in 1139 patients with allergic rhinitis in zhengzhou area. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi, 2014; 49, 858–860, (in Chinese). [Google Scholar] [PubMed]
- Kidon, M.I.; Chiang, W.C.; Liew, W.K.; Lim, S.H.; See, Y.; Goh, A.; Tan, J.P.; Chay, O.M.; Balakrishnan, A. Sensitization to dust mites in children with allergic rhinitis in singapore: Does it matter if you scratch while you sneeze? Clin. Exp. Allergy 2005, 35, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhao, Y.; Wang, C.S.; Wang, X.D.; Zhang, L. Prevalence of sensitization to aeroallergens in 10 030 patients with allergic rhinitis. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi, 2011; 46, 914–920, (in Chinese). [Google Scholar] [PubMed]
- Hao, B.; Ma, L.; Qiao, X. Identification of broad-spectrum antagonistic strain B96-II and GFP tagging. Acta Agr. Boreali-Sinica 2009, 24, 188–191. (in Chinese). [Google Scholar]
- Fereidouni, M.; Hossini, R.F.; Azad, F.J.; Assarehzadegan, M.A.; Varasteh, A. Skin prick test reactivity to common aeroallergens among allergic rhinitis patients in Iran. Allergol. Immunopathol. (Madr) 2009, 37, 73–79. [Google Scholar] [CrossRef]
- Demore, J.P.; Leo, H.L. Cat, dog and house dust mite allergen levels on children’s soft toys. Pediatrics 2014, 134 Supplemen 3, S143–S144. [Google Scholar] [CrossRef] [PubMed]
- Xiang, L.; Fu, Y.; Wang, J.; Wang, Q. Distribution Characteristics and environmental influencing factors of house dust mite allergens’ content in household dust from house dust mite-allergic asthmatic children. Chin. J. Allergy Clin. Immunol. 2013, 7, 314–321. (in Chinese). [Google Scholar]
- Zhong, N.; Ye, J.; Zhang, J.; Liu, Y.; Yi, H. Analysis of aeroallergen spectrum in patients with allergic rhinitis in nanchang area. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi, 2014; 49, 505–508, (in Chinese). [Google Scholar] [PubMed]
- Xiang, L.; Fu, Y.; Wang, J.; Wang, Q. The correlation between the seasonal variation of house dust mite allergens exposure level in household and the level of asthma control in asthmatic children. Zhonghua Er Ke Za Zhi, 2014; 52, 177–183, (in Chinese). [Google Scholar] [PubMed]
- Chen, D.; Sun, B.; Lin, Y.; Pan, X.; Zhong, G.; Chen, Q.; Chen, F.; Li, J.; Zhong, N. Prevalence analysis of common allergies in respiratory allergic diseases of children in Guangzhou urban districts. Int. J. Respir. Dis. 2009, 29, 385–388. [Google Scholar]
- Wu, Y.; Ai, T.; Luo, R.; Wang, C.; Lu, Z. Analysis of the allergic skin prick test results in 827 children with asthma in chengdu. Chongqing Med. 2010, 39, 2362–2363. (in Chinese). [Google Scholar]
- El-Ghitany, E.M.; Abd El-Salam, M.M. Environmental intervention for house dust mite control in childhood bronchial asthma. Environ. Health Prev. Med. 2012, 17, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Saridomichelakis, M.N.; Marsella, R.; Lee, K.W.; Esch, R.E.; Farmaki, R.; Koutinas, A.F. Assessment of cross-reactivity among five species of house dust and storage mites. Vet. Dermatol. 2008, 19, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Z.; Ma, Y.; Wang, H.Y.; Wang, H.J.; Zhao, J.; Cao, L.; Li, S.; Wong, G.W.; Zhong, N.S.; Fok, T.F.; et al. Individual allergens as risk factors for asthma and bronchial hyperresponsiveness in chinese children. Zhonghua Er Ke Za Zhi, 2003; 41, 538–541, (in Chinese). [Google Scholar] [PubMed]
- Bousquet, P.J.; Hooper, R.; Kogevinas, M.; Jarvis, D.; Burney, P. Number of allergens to be tested to assess allergenic sensitization in epidemiologic studies: Results of the european community respiratory health survey I. Clin. Exp. Allergy 2007, 37, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Smits, W.L.; Letz, K.L.; Evans, T.S.; Giese, J.K. Evaluating the response of patients undergoing both allergy skin testing and in vitro allergy testing with the immunocap technology system. J. Am. Acad. Nurs. Pract. 2003, 15, 415–423. [Google Scholar] [CrossRef]
- Bousquet, P.J.; Chatzi, L.; Jarvis, D.; Burney, P. Assessing skin prick tests reliability in ECRHS-I. Allergy 2008, 63, 341–346. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.; Lin, R.; Li, N. Sensitization Rates for Various Allergens in Children with Allergic Rhinitis in Qingdao, China. Int. J. Environ. Res. Public Health 2015, 12, 10984-10994. https://doi.org/10.3390/ijerph120910984
Lin H, Lin R, Li N. Sensitization Rates for Various Allergens in Children with Allergic Rhinitis in Qingdao, China. International Journal of Environmental Research and Public Health. 2015; 12(9):10984-10994. https://doi.org/10.3390/ijerph120910984
Chicago/Turabian StyleLin, Hang, Rongjun Lin, and Na Li. 2015. "Sensitization Rates for Various Allergens in Children with Allergic Rhinitis in Qingdao, China" International Journal of Environmental Research and Public Health 12, no. 9: 10984-10994. https://doi.org/10.3390/ijerph120910984