Incinerator Pollution and Child Development in the Taiwan Birth Cohort Study

Abstract
:1. Introduction

2. Experimental Section
2.1. Participants
2.2. Materials
2.2.1. Taiwan Birth Cohort Study-Developmental Instrument (TBCS-DI)
2.2.2. Parental Concern Checklist (PCC)
2.3. Statistical Analysis
3. Results and Discussion
3.1. Results
3.1.1. Demographic Information
3.1.2. Parent-Perceived Children’s Developmental Condition and Parental Concern regarding Children’s Development

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lives near an incinerator (n = 953) | Does not live near an incinerator (n = 20,295) | ||||
|---|---|---|---|---|---|
| n (%) | n (%) | χ2 | p | ||
| Boys | 524 (55.0) | 10,621 (52.3) | 2.57 | 0.058 | |
| Twins | 534 (2.6) | 926 (2.6) | 0.14 | 0.391 | |
| Breastfed at six months | 230 (24.1) | 4,348 (21.4) | 10.86 | 0.026 | |
| Children’s health: | |||||
| Received vaccination | 950 (99.7) | 20,272 (99.9) | 3.02 | 0.109 | |
| Has had gastrointestinal illness | 182 (19.1) | 4,054 (20.0) | 0.44 | 0.267 | |
| Has been hospitalized | 127 (13.3) | 2,658 (13.1) | 0.04 | 0.438 | |
| Lives in the city | 503 (52.8) | 9,605 (47.3) | 10.86 | 0.001 | |
| Has moved | 26 (2.7) | 509 (2.5) | 0.18 | 0.375 | |
| Maternal education: | |||||
| Illiterate | 0 (0.0) | 18 (0.1) | |||
| Elementary school | 54 (5.7) | 774 (3.8) | |||
| Junior high | 103 (10.8) | 2,200 (10.8) | |||
| High school | 364 (38.2) | 8,134 (40.1) | |||
| University/college | 393 (41.2) | 8,467 (41.7) | |||
| Graduate school | 39 (4.1) | 702 (3.5) | |||
| Paternal education: | |||||
| Illiterate | 0 (0.0) | 3 (<0.1) | |||
| Elementary school | 16 (1.7) | 288 (1.4) | |||
| Junior high | 133 (14.0) | 2,503 (12.3) | |||
| High school | 369 (38.7) | 8,100 (39.9) | |||
| University/college | 362 (38.0) | 7,868 (38.8) | |||
| Graduate school | 1,533 (7.6) | 1,533 (7.6) | |||
| Variable (range) | Mean (SD) | Mean (SD) | t-test | p | |
| Parental education (years) | |||||
| Maternal education (0–18) | 12.56 (2.86) | 12.68 (2.69) | 2.89 | 0.089 | |
| Paternal education (0–19) | 12.92 (2.59) | 12.99 (2.51) | 1.50 | 0.221 | |
| Parental age (years) | |||||
| Mother’s age (14–49) | 29.57 (4.91) | 29.38 (4.89) | 0.09 | 0.762 | |
| Father’s age (17–80) | 33.43 (5.25) | 33.30 (5.46) | 1.55 | 0.214 | |
| Lives near an incinerator (n = 953) | Does not live near an incinerator (n = 20,295) | ||||
|---|---|---|---|---|---|
| TBCS-DI | Mean (SD) | Mean (SD) | t-test | p | |
| Six-month development | |||||
| Gross motor | 22.52 (3.38) | 22.62 (3.27) | 3.12 | 0.078 | |
| Fine motor | 16.24 (1.74) | 16.25 (1.73) | 0.35 | 0.553 | |
| Language | 20.87 (2.27) | 20.96 (2.37) | 2.74 | 0.098 | |
| Social | 5.79 (1.36) | 5.89 (1.42) | 1.99 | 0.158 | |
| 18-month development | |||||
| Gross motor | 13.81 (1.45) | 13.88 (1.40) | 2.64 | 0.104 | |
| Fine motor | 7.89 (1.23) | 7.92 (1.21) | 0.27 | 0.601 | |
| Language | 9.91 (2.07) | 10.01 (2.12) | 0.68 | 0.410 | |
| Social | 13.12 (1.80) | 13.16 (1.72) | 0.81 | 0.367 | |
| 36-month development | |||||
| Gross motor | 16.63 (1.85) | 16.77 (1.70) | 6.93 | 0.008 | |
| Fine motor | 10.00 (1.81) | 10.03 (1.73) | 2.74 | 0.098 | |
| Language | 11.83 (0.86) | 11.84 (0.76) | 1.75 | 0.186 | |
| Social | 13.78 (1.54) | 13.76 (1.49) | 0.03 | 0.864 | |
| PCC | n (%) | n (%) | χ2 | p | |
| 18-month mild U/DDD | 137 (14.4) | 2458 (21.2) | 4.35 | 0.037 | |
| 18-month moderate U/DDD | 20 (2.1) | 236 (1.2) | 6.70 | 0.010 | |
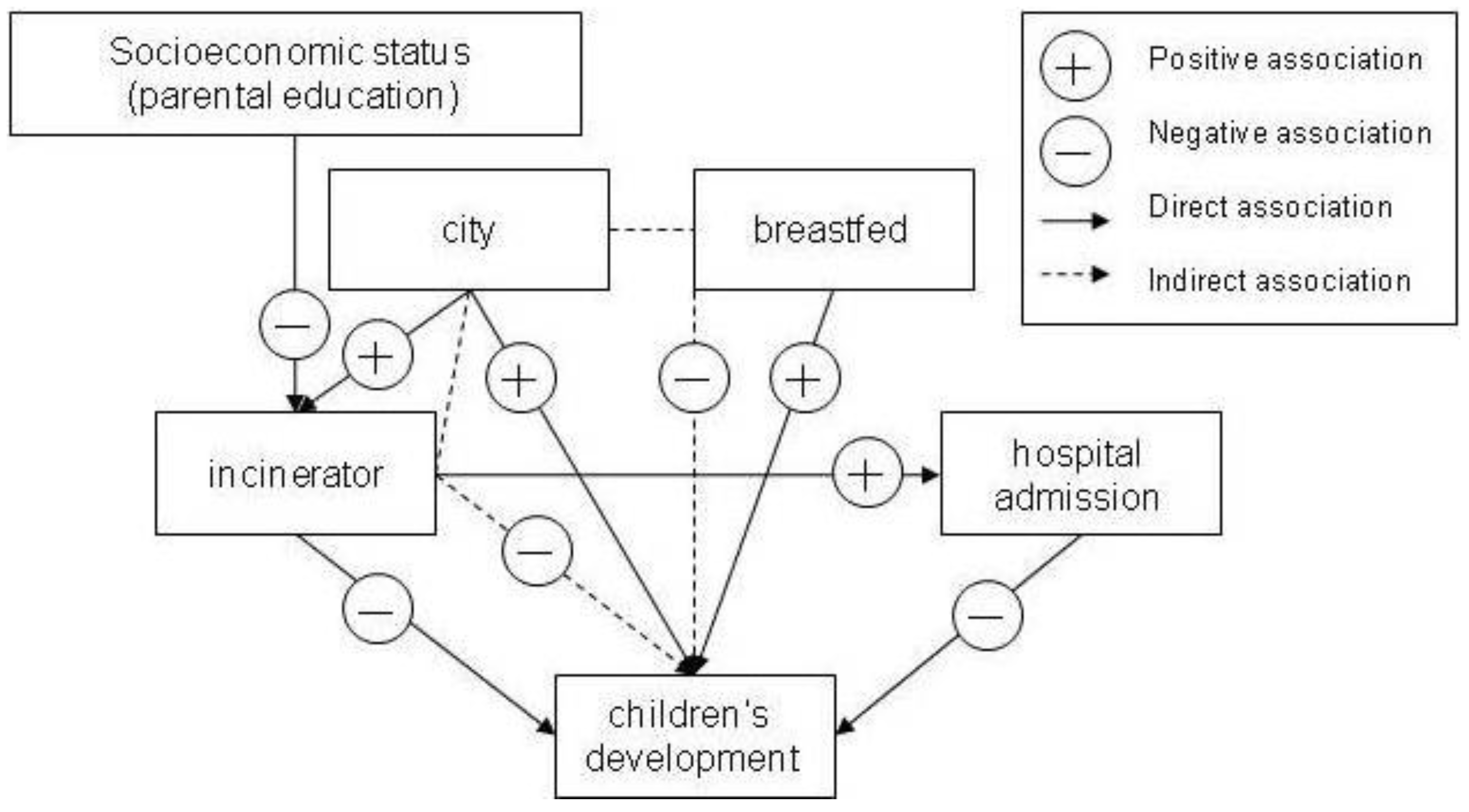
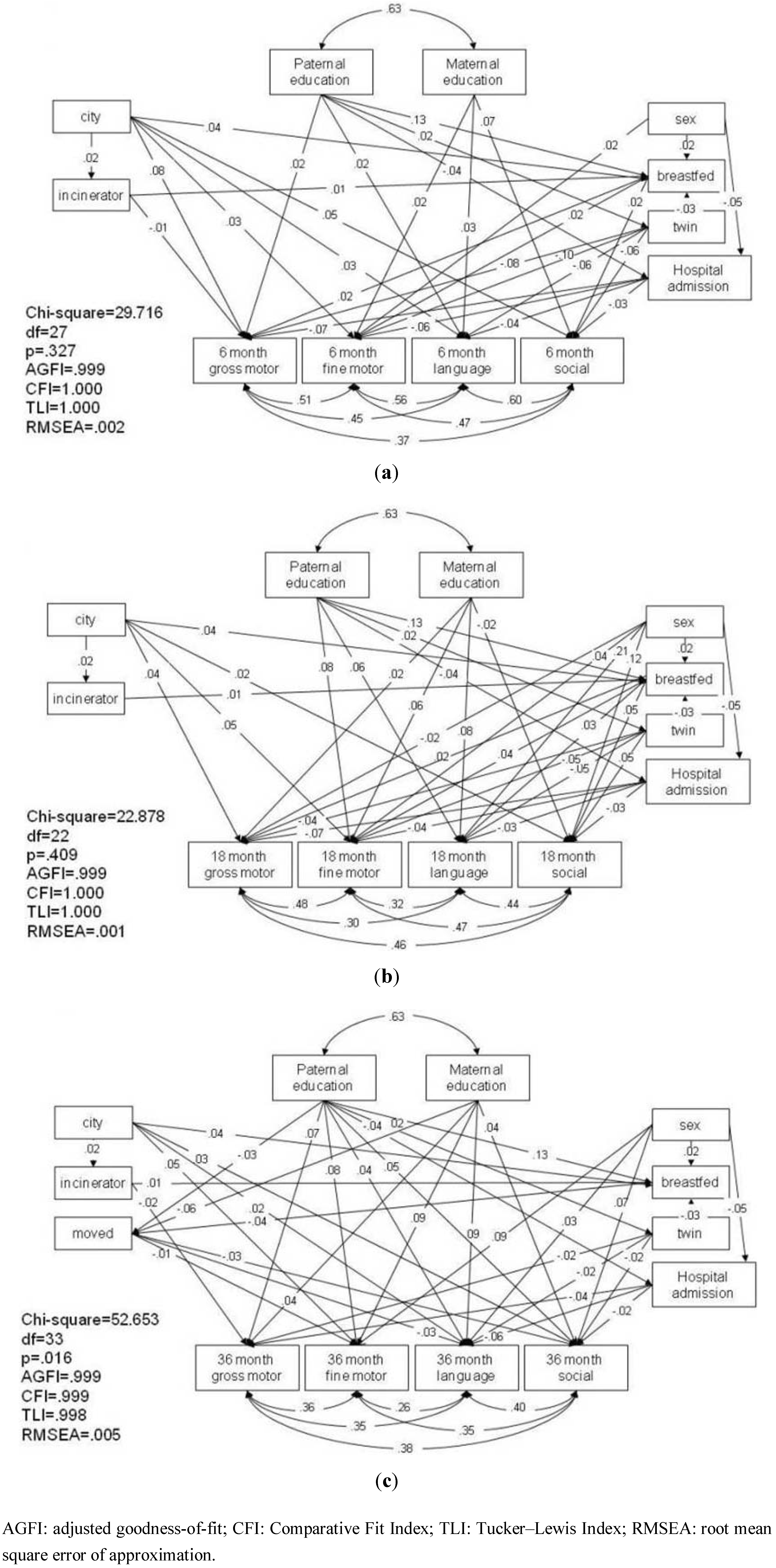
3.1.3. Pathway Analysis of Children’s Development at Six, 18, and 36 Months

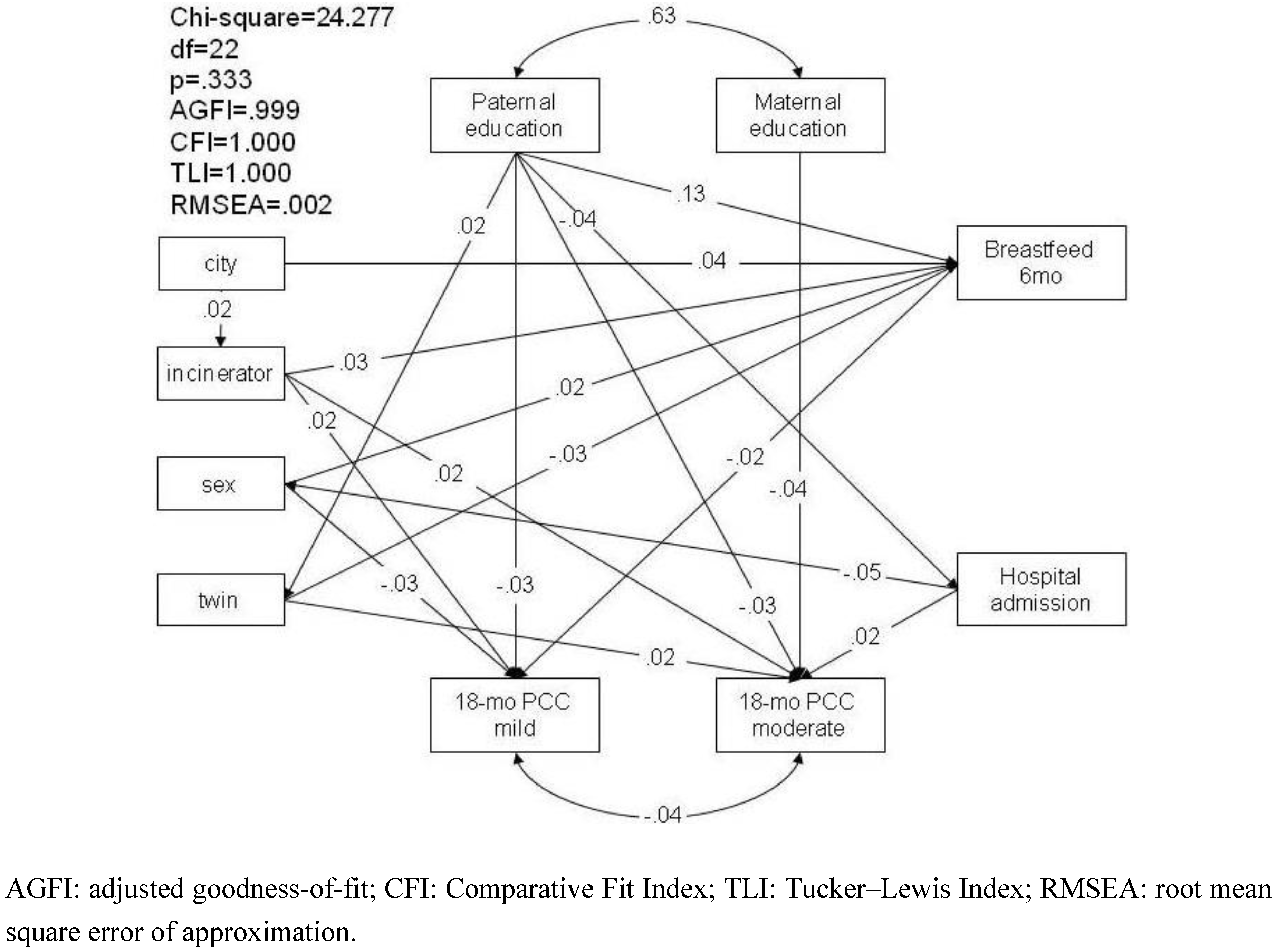
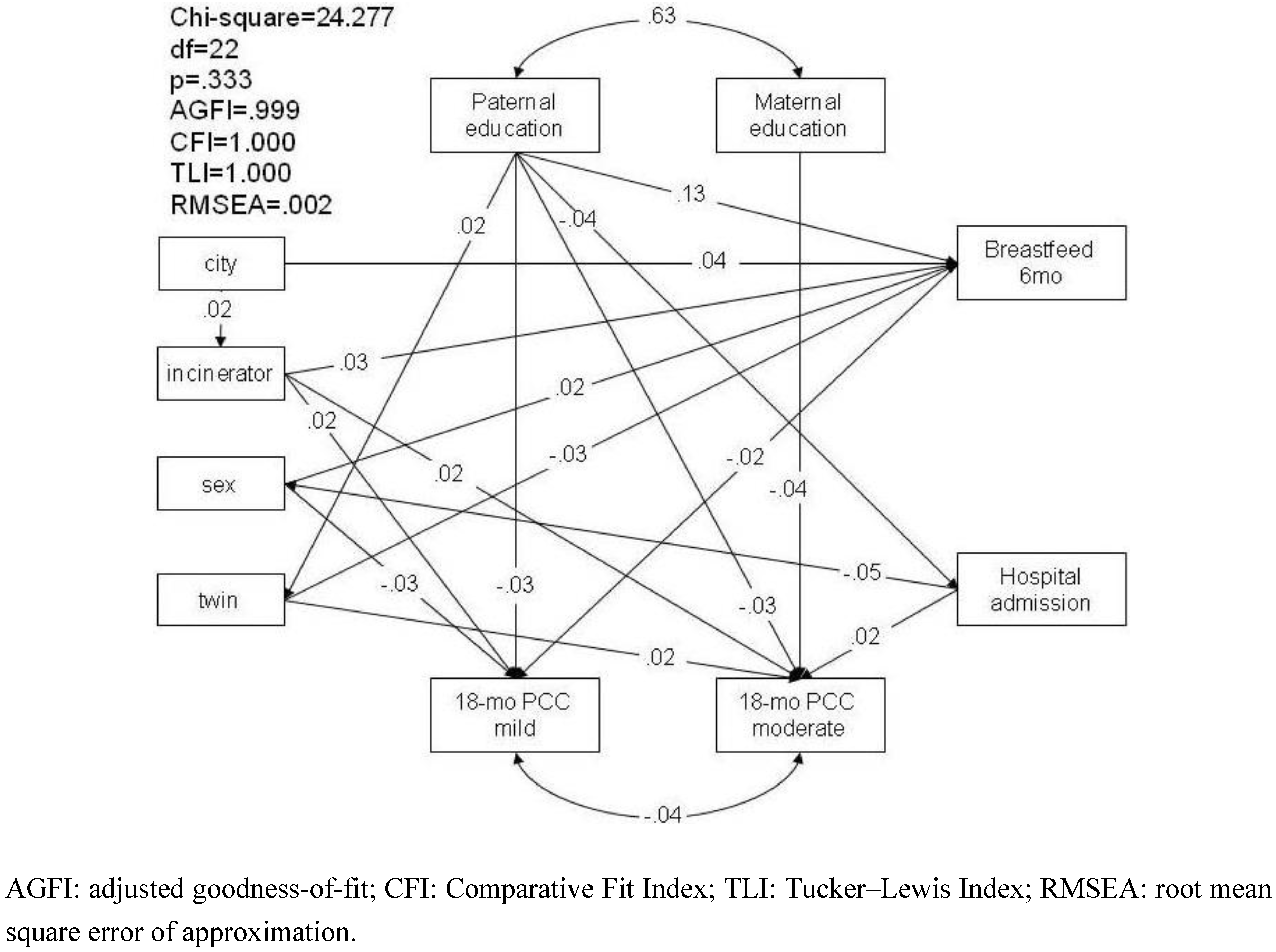
3.1.4. Pathway Analysis of Parental Concern regarding Children’s Development at 18 Months
3.2. Discussion
4. Conclusions
Acknowledgments
Conflict of Interest
References
- Allsopp, M.; Costner, P.; Johnston, P. Incineration and human health. Environ. Sci. Pollut. Res. 2001, 8, 141–145. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Carlson, J.E.; Bearer, C.F.; Cranmer, J.S.; Bullard, R.D.; Etzel, R.A.; Groopman, J.; McLachlan, J.A.; Perera, F.P.; Reigart, J.R.; et al. Children’s health and the environment: A new agenda for prevention research. Environ. Health Perspect. 1998, 106, 787–794. [Google Scholar]
- Liao, M.F.; Huang, J.L.; Chiang, L.C.; Wan, F.Y.; Chen, C.Y. Prevalence of asthma, rhinitis, and eczema from ISAAC survey of school children in central Taiwan. J. Asthma 2005, 42, 833–837. [Google Scholar] [CrossRef]
- Chandra, A.; Martinez, G.M.; Mosher, W.D.; Abma, J.C.; Jones, J. Fertility, family planning, and reproductive health of U.S. women: Data from the 2002 National Survey of Family Growth. National Center for Health Statistics. Vital Health Stat. 2005, 175, 1–160. [Google Scholar]
- Jahnke, G.D.; Iannucci, A.R.; Scialli, A.R.; Shelby, M.D. Center for the evaluation of risks to human reproduction—The first five years. Birth Defects Res. B. Dev. Reprod. Toxicol. 2005, 74, 1–8. [Google Scholar] [CrossRef]
- Trasande, L.; Landrigan, P.J. The national children’s study: A critical national investment. Environ. Health Perspect. 2004, 112, A789–A790. [Google Scholar] [CrossRef]
- Calderón-Garcidueñas, L.; Torres-Jardón, R. Air pollution, socioeconomic status, and children’s cognition in megacities: The Mexico City scenario. Front. Psychol. 2012, 3, 217. [Google Scholar] [CrossRef]
- Herbert, M.R. Contributions of the environment and environmentally vulnerable physiology to autism spectrum disorders. Curr. Opin. Neurol. 2010, 23, 103–310. [Google Scholar] [CrossRef]
- Mutter, J.; Naumann, J.; Schneider, R.; Walach, H.; Haley, B. Mercury and autism: Accelerating evidence. Neuro. Endocrinol. Lett. 2005, 26, 439–446. [Google Scholar]
- Palmer, R.F.; Blanchard, S.; Wood, R. Proximity to point sources of environmental mercury release as a predictor of autism prevalence. Health Place 2009, 15, 18–24. [Google Scholar] [CrossRef]
- Brent, R.L. Environmental causes of human congenital malformations: The pediatrician’s role in dealing with these complex clinical problems caused by a multiplicity of environmental and genetic factors. Pediatrics 2004, 113, 957–968. [Google Scholar]
- Glynn, A.W.; Darnerud, P.O.; Aune, M.; Bjerselius, R.; Baumann, B.; Cnattingius, S. PCBs and dioxins in breast milk—Levels and trends in Sweden 1996–2001. Organohalogen. Compd. 2003, 64, 21–24. [Google Scholar]
- Schuhmacher, M.; Domingo, J.L.; Kiviranta, H.; Vartiainen, T. Monitoring dioxins and furans in a population living near a hazardous waste incinerator: Levels in breast milk. Chemosphere 2004, 57, 43–49. [Google Scholar] [CrossRef]
- Koopman-Esseboom, C.; Huisman, M.; Weisglas-Kuperus, N.; Van der Paauw, C.G.; Th.Tuinstra, L.G.M.; Boersma, E.R.; Sauer, P.J.J. PCB and dioxin levels in plasma and human milk of 418 Dutch women and their infants: Predictive value of PCB congener levels in maternal plasma for fetal and infant’s exposure to PCBs and dioxins. Chemosphere 1994, 28, 1721–1732. [Google Scholar] [CrossRef] [Green Version]
- Patandin, S.; Dagnelie, P.C.; Mulder, P.G.; Op de Coul, E.; van der Veen, J.E.; Weisglas-Kuperus, N.; Sauer, P.J. Dietary exposure to polychlorinated biphenyls and dioxins from infancy until adulthood: A comparison between breast-feeding, toddler, and long-term exposure. Environ. Health Perspect. 1999, 107, 45–51. [Google Scholar] [CrossRef]
- Neuberger, M.; Grossgut, R.; Gyimothy, J.; Leibetseder, J. Dioxin contamination of feed and food. Lancet 2000, 355, 1883. [Google Scholar] [CrossRef]
- Hu, S.W.; Shy, C.M. Health effects of waste incineration: A review of epidemiologic studies. J. Air Waste Manag. Assoc. 2001, 51, 1100–1109. [Google Scholar] [CrossRef]
- Lin, C.M.; Li, C.Y.; Mao, I.F. Birth outcomes of infants born in areas with elevated ambient exposure to incinerator generated PCDD/Fs. Environ. Int. 2006, 32, 624–629. [Google Scholar] [CrossRef]
- Lung, F.W.; Chiang, T.L.; Lin, S.J.; Shu, B.C.; Lee, M.C. Developing and refining the Taiwan Birth Cohort Study (TBCS): Five years of experience. Res. Dev. Disabil. 2011, 32, 2697–2703. [Google Scholar] [CrossRef]
- Lung, F.W.; Shu, B.C.; Chiang, T.L.; Lin, S.J. Efficient developmental screening instrument for 6- and 18-month-old children in the Taiwan Birth Cohort Pilot Study. Acta Paediatr. 2008, 98, 1093–1098. [Google Scholar]
- Lung, F.W.; Shu, B.C.; Chiang, T.L.; Lin, S.J. Parental concerns based general developmental screening tool and autism risk: The Taiwan National Birth Cohort Study. Pediatr. Res. 2010, 67, 226–231. [Google Scholar] [CrossRef]
- Lung, F.W.; Chiang, T.L.; Lin, S.J.; Feng, J.Y.; Chen, P.F.; Shu, B.C. Gender differences of children’s developmental trajectory from six to sixty months in the Taiwan Birth Cohort Pilot Study. Res. Dev. Disabil. 2011, 32, 100–106. [Google Scholar] [CrossRef]
- Glascoe, F.P. Parents’ Evaluations of Developmental Status: A Method for Detecting and Addressing Developmental and Behavioral Problems in Children; Ellsworth & Vandermeer Press: Nashville, TN, USA, 2006. [Google Scholar]
- Glascoe, F.P.; Macias, M.M.; Wegner, L.M.; Robertshaw, N.S. Can a broadband developmental-behavioral screening test identify children likely to have autism spectrum disorder? Clin. Pediatr. (Phila.) 2007, 46, 801–805. [Google Scholar] [CrossRef]
- Sram, R.J.; Binkova, B.; Dostal, M.; Merkerova-Dostalova, M.; Libalova, H.; Milcova, A.; Rossner, P., Jr.; Rossnerova, A.; Schmuczerova, J.; Svecova, V.; Topinka, J.; Votavova, H. Health impact of air pollution to children. Int. J. Hyg. Environ. Health 2013. [Google Scholar] [CrossRef]
- Pereira, G.; Cook, A.G.; Haggar, F.; Bower, C.; Nassar, N. Locally derived traffic-related air pollution and fetal growth restriction: A retrospective cohort study. Occup. Environ. Med. 2012, 69, 815–822. [Google Scholar] [CrossRef]
- Foroushani, A.R.; Mohammad, K.; Mahmoodi, M.; Siassi, F. Effect of breastfeeding on cognitive performance in a British birth cohort. East. Mediterr. Health J. 2010, 16, 202–208. [Google Scholar]
- Kull, I.; Melen, E.; Alm, J.; Hallberg, J.; Svartengren, M.; van Hage, M.; Pershagen, G.; Wickman, M.; Bergström, A. Breast-feeding in relation to asthma, lunch function, and sensitization in young schoolchildren. J. Allergy Clin. Immunol. 2010, 125, 1013–1019. [Google Scholar] [CrossRef]
- Holme, A.; MacArthur, C.; Lanceshire, R. The effects of breastfeeding on cognitive and neurological development of children at 9 years. Child. Care Health Dev. 2010, 36, 583–590. [Google Scholar] [CrossRef]
- Forastiere, F.; Badaloni, C.; de Hoogh, K.; von Kraus, M.K.; Martuzzi, M.; Mitis, F.; Palkovicova, L.; Porta, D.; Preiss, P.; Ranzi, A.; et al. Health impact assessment of waste management facilities in three European countries. Environ. Health 2011, 10, 53. [Google Scholar] [CrossRef]
- Chinese Breastfeeding Infants Growth and Development Study Group. A longitudinal study of urban-rural growth differences among infants fed with breast milk in six economically better areas in China. Chin. J. Pediatr. 2012, 50, 484–492.
- Chen, X.; Li, D. Parental encouragement of initiative-taking and adjustment in Chinese children from rural, urban, and urbanized families. J. Fam. Psychol. 2012, 26, 927–936. [Google Scholar] [CrossRef]
- Miller, P.; Votruba-Drzal, E.; Setodji, C.M. Family income and early achievement across the urban-rural continuum. Dev. Psychol. 2012. [Google Scholar] [CrossRef]
- Lung, F.W.; Shu, B.C.; Chiang, T.L.; Lin, S.J. Parental mental health, education, age at childbirth and child development from six to 18 months. Acta Paediatr. 2009, 98, 834–841. [Google Scholar] [CrossRef]
- Lung, F.W.; Shu, B.C.; Chiang, T.L.; Lin, S.J. Parental mental health and child developmental from six to thirty-six months in a birth cohort study in Taiwan. J. Perinat. Med. 2009, 37, 397–402. [Google Scholar]
- Filipek, P.A.; Accardo, P.J.; Ashwal, S.; Baranek, G.T.; Cook, E.H., Jr.; Dawson, G.; Gordon, B.; Gravel, J.S.; Johnson, C.P.; Kallen, R.J.; et al. Practice parameter: Screening and diagnosis of autism: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Child Neurology Society. Neurology 2000, 55, 468–479. [Google Scholar] [CrossRef]
- Glascoe, F.P.; Foster, E.M.; Wolraich, M.L. An economic analysis of developmental detection methods. Pediatrics 1997, 99, 830–837. [Google Scholar] [CrossRef]
- Lim, Y.; Yang, J.; Kim, Y.; Chang, Y.; Shin, D. Assessment of human health risk of dioxin in Korea. Environ. Monit. Assess. 2004, 92, 221–228. [Google Scholar]
- Wang, M.S.; Chen, S.J.; Huang, K.L.; Lai, Y.C.; Chang-Chien, G.P.; Tsai, J.H.; Lin, W.Y.; Chang, K.C.; Lee, J.T. Determination of levels of persistent organic pollutants (PCDD/Fs, PBDD/Fs, PBDEs, PCBs, and PBBs) in atmosphere near a municipal solid waste incinerator. Chemosphere 2010, 80, 1220–1226. [Google Scholar] [CrossRef]
- Hayakawa, K.; Takatsuki, H.; Watanabe, I.; Sakai, S.I. Polybrominated diphenyl ethers (PBDEs), polybrominated dibenzo-p-dioxins/dibenzofurans (PBDD/Fs) and monobromo-polychlorinated dibenzo-p-dioxins/dibenzofurans (MoBPXDD/Fs) in the atmosphere and bulk deposition in Kyoto, Japan. Chemosphere 2004, 57, 343–356. [Google Scholar] [CrossRef]
- Kurttio, P.; Perkanen, J.; Alfthan, G.; Paunio, M.; Jaakkola, J.J.K.; Heinonen, O.P. Increased mercury exposure in inhabitants living in the vicinity of a hazardous waste incinerator: A 10-year follow-up. Arch. Environ. Health 1998, 53, 129–137. [Google Scholar] [CrossRef]
- Center for Longitudinal Studies. Available online: www.cls.ioe.ac.uk/default.aspx (accessed on 19 April 2013).
Supplemental Materials

© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lung, F.-W.; Chiang, T.-L.; Lin, S.-J.; Shu, B.-C. Incinerator Pollution and Child Development in the Taiwan Birth Cohort Study. Int. J. Environ. Res. Public Health 2013, 10, 2241-2257. https://doi.org/10.3390/ijerph10062241
Lung F-W, Chiang T-L, Lin S-J, Shu B-C. Incinerator Pollution and Child Development in the Taiwan Birth Cohort Study. International Journal of Environmental Research and Public Health. 2013; 10(6):2241-2257. https://doi.org/10.3390/ijerph10062241
Chicago/Turabian StyleLung, For-Wey, Tung-Liang Chiang, Shio-Jean Lin, and Bih-Ching Shu. 2013. "Incinerator Pollution and Child Development in the Taiwan Birth Cohort Study" International Journal of Environmental Research and Public Health 10, no. 6: 2241-2257. https://doi.org/10.3390/ijerph10062241