
The Effect of Pringle Maneuver Applied during Living Donor Hepatectomy on the Ischemia-Reperfusion Injury Observed in the Donors and Recipients
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Technique for LDH Procedure
2.2. Study Parameters
2.3. Histologic Evaluation
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the LLDs
3.2. Evaluation of the LLDS with and without the Pringle Maneuver
3.3. Demographic and Clinical Characteristics of the Recipients
3.4. Evaluation of the Recipients That Received Liver Grafts with or without Pringle Maneuver
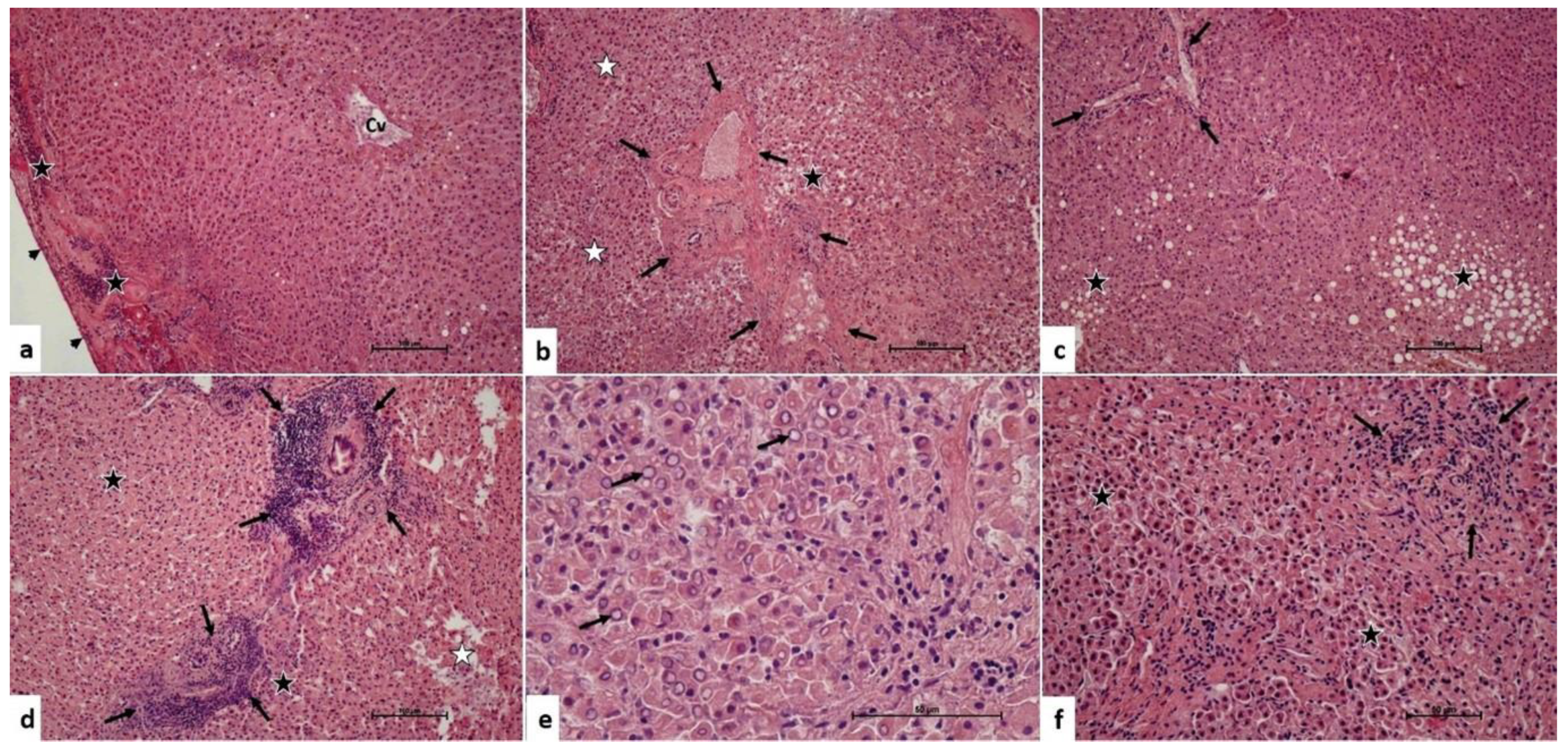
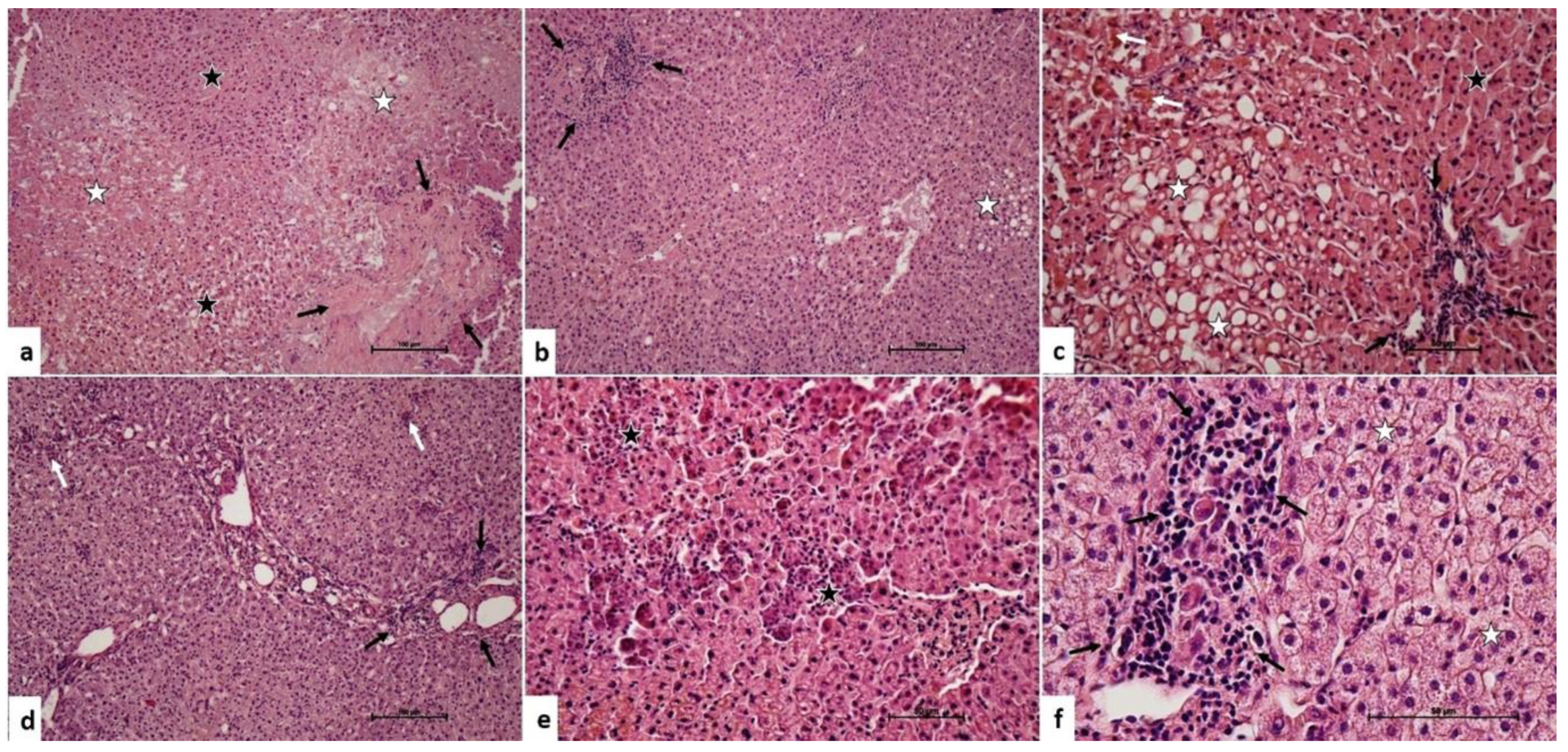
3.5. Microscopic Effects of the Pringle Maneuver
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akbulut, S.; Yilmaz, S. Liver transplantation in Turkey: Historical review and future perspectives. Transplant. Rev. 2015, 29, 161–167. [Google Scholar] [CrossRef]
- Olson, J.C.; Subramanian, R.; Karvellas, C.J. Intensive care management of liver transplant recipients. Curr. Opin. Crit. Care 2022, 28, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Starzl, T.E.; Groth, C.G.; Brettschneider, L.; Penn, I.; Fulginiti, V.A.; Moon, J.B.; Blanchard, H.; Martin, A.J., Jr.; Porter, K.A. Orthotopic homotransplantation of the human liver. Ann. Surg. 1968, 168, 392–415. [Google Scholar] [CrossRef] [PubMed]
- Starzl, T.E.; Marchioro, T.L.; Vonkaulla, K.N.; Hermann, G.; Brittain, R.S.; Waddell, W.R. Homotransplantation of the liver in humans. Surg. Gynecol. Obstet. 1963, 117, 659–676. [Google Scholar] [PubMed]
- Durand, F.; Renz, J.F.; Alkofer, B.; Burra, P.; Clavien, P.A.; Porte, R.J.; Freeman, R.B.; Belghiti, J. Report of the Paris consensus meeting on expanded criteria donors in liver transplantation. Liver Transpl. 2008, 14, 1694–1707. [Google Scholar] [CrossRef] [PubMed]
- Broering, D.C.; Sterneck, M.; Rogiers, X. Living donor liver transplantation. J. Hepatol. 2003, 38 (Suppl. S1), S119–S135. [Google Scholar] [CrossRef] [PubMed]
- Burra, P.; Zanetto, A.; Russo, F.P.; Germani, G. Organ Preservation in Liver Transplantation. Semin. Liver Dis. 2018, 38, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Howard, T.K.; Klintmalm, G.B.; Cofer, J.B.; Husberg, B.S.; Goldstein, R.M.; Gonwa, T.A. The influence of preservation injury on rejection in the hepatic transplant recipient. Transplantation 1990, 49, 103–107. [Google Scholar] [CrossRef]
- Dar, W.A.; Sullivan, E.; Bynon, J.S.; Eltzschig, H.; Ju, C. Ischaemia reperfusion injury in liver transplantation: Cellular and molecular mechanisms. Liver Int. 2019, 39, 788–801. [Google Scholar] [CrossRef]
- Duffy, J.P.; Hong, J.C.; Farmer, D.G.; Ghobrial, R.M.; Yersiz, H.; Hiatt, J.R.; Busuttil, R.W. Vascular complications of orthotopic liver transplantation: Experience in more than 4,200 patients. J. Am. Coll. Surg. 2009, 208, 896–903; discussion 903–905. [Google Scholar] [CrossRef]
- Kaltenmeier, C.; Wang, R.; Popp, B.; Geller, D.; Tohme, S.; Yazdani, H.O. Role of Immuno-Inflammatory Signals in Liver Ischemia-Reperfusion Injury. Cells 2022, 11, 2222. [Google Scholar] [CrossRef] [PubMed]
- Carini, R.; Autelli, R.; Bellomo, G.; Albano, E. Alterations of cell volume regulation in the development of hepatocyte necrosis. Exp. Cell Res. 1999, 248, 280–293. [Google Scholar] [CrossRef] [PubMed]
- St Peter, S.D.; Imber, C.J.; Friend, P.J. Liver and kidney preservation by perfusion. Lancet 2002, 359, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Yiang, G.T.; Liao, W.T.; Tsai, A.P.; Cheng, Y.L.; Cheng, P.W.; Li, C.Y.; Li, C.J. Current Mechanistic Concepts in Ischemia and Reperfusion Injury. Cell Physiol. Biochem. 2018, 46, 1650–1667. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Harvey, P.R.; Strasberg, S.M. Preservation and reperfusion injuries in liver allografts. An overview and synthesis of current studies. Transplantation 1992, 53, 957–978. [Google Scholar] [CrossRef]
- Kayyali, U.S.; Donaldson, C.; Huang, H.; Abdelnour, R.; Hassoun, P.M. Phosphorylation of xanthine dehydrogenase/oxidase in hypoxia. J. Biol. Chem. 2001, 276, 14359–14365. [Google Scholar] [CrossRef]
- Petrosillo, G.; Ruggiero, F.M.; Paradies, G. Role of reactive oxygen species and cardiolipin in the release of cytochrome c from mitochondria. FASEB J. 2003, 17, 2202–2208. [Google Scholar] [CrossRef] [PubMed]
- Vickneson, K.; George, J. Xanthine Oxidoreductase Inhibitors. Handb. Exp. Pharmacol. 2021, 264, 205–228. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, T.H.C.; Marques, P.E.; Proost, P.; Teixeira, M.M.M. Neutrophils: A cornerstone of liver ischemia and reperfusion injury. Lab. Investig. 2018, 98, 51–62. [Google Scholar] [CrossRef]
- Gandhi, C.R. Oxidative Stress and Hepatic Stellate Cells: A Paradoxical Relationship. Trends Cell Mol. Biol. 2012, 7, 1–10. [Google Scholar]
- Wang, M.; Zhang, J.; Gong, N. Role of the PI3K/Akt signaling pathway in liver ischemia reperfusion injury: A narrative review. Ann. Palliat. Med. 2022, 11, 806–817. [Google Scholar] [CrossRef] [PubMed]
- Aufhauser, D.D., Jr.; Foley, D.P. Beyond Ice and the Cooler: Machine Perfusion Strategies in Liver Transplantation. Clin. Liver Dis. 2021, 25, 179–194. [Google Scholar] [CrossRef]
- Cai, H.; Qi, S.; Yan, Q.; Ling, J.; Du, J.; Chen, L. Global proteome profiling of human livers upon ischemia/reperfusion treatment. Clin. Proteom. 2021, 18, 3. [Google Scholar] [CrossRef]
- Jing, L.; Yao, L.; Zhao, M.; Peng, L.P.; Liu, M. Organ preservation: From the past to the future. Acta Pharmacol. Sin. 2018, 39, 845–857. [Google Scholar] [CrossRef] [PubMed]
- Saidi, R.F.; Kenari, S.K. Liver ischemia/reperfusion injury: An overview. J. Investig. Surg. 2014, 27, 366–379. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, J.; Jiang, B.; Wang, J.; Liu, C.; Peng, C.; Tian, B. Relationship between ischemia/reperfusion injury and acute rejection of allogeneic liver transplant in rats. Transplant. Proc. 2014, 46, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Man, K.; Fan, S.T.; Ng, I.O.; Lo, C.M.; Liu, C.L.; Yu, W.C.; Wong, J. Tolerance of the liver to intermittent pringle maneuver in hepatectomy for liver tumors. Arch. Surg. 1999, 134, 533–539. [Google Scholar] [CrossRef]
- Pringle, J.H.V. Notes on the Arrest of Hepatic Hemorrhage Due to Trauma. Ann. Surg. 1908, 48, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.; Chen, C.L.; Lin, C.C.; Yang, C.H.; Wang, C.C.; Wang, S.H.; Liu, Y.W.; Yong, C.C.; Concejero, A.; Jawan, B.; et al. Intraoperative blood loss is a risk factor for complications in donors after living donor hepatectomy. Liver Transpl. 2006, 12, 950–957. [Google Scholar] [CrossRef]
- Katz, S.C.; Shia, J.; Liau, K.H.; Gonen, M.; Ruo, L.; Jarnagin, W.R.; Fong, Y.; D’Angelica, M.I.; Blumgart, L.H.; Dematteo, R.P. Operative blood loss independently predicts recurrence and survival after resection of hepatocellular carcinoma. Ann. Surg. 2009, 249, 617–623. [Google Scholar] [CrossRef]
- Clavien, P.A.; Yadav, S.; Sindram, D.; Bentley, R.C. Protective effects of ischemic preconditioning for liver resection performed under inflow occlusion in humans. Ann. Surg. 2000, 232, 155–162. [Google Scholar] [CrossRef]
- Imamura, H.; Takayama, T.; Sugawara, Y.; Kokudo, N.; Aoki, T.; Kaneko, J.; Matsuyama, Y.; Sano, K.; Maema, A.; Makuuchi, M. Pringle’s manoeuvre in living donors. Lancet 2002, 360, 2049–2050. [Google Scholar] [CrossRef]
- Murry, C.E.; Jennings, R.B.; Reimer, K.A. Preconditioning with ischemia: A delay of lethal cell injury in ischemic myocardium. Circulation 1986, 74, 1124–1136. [Google Scholar] [CrossRef] [PubMed]
- Winbladh, A.; Björnsson, B.; Trulsson, L.; Offenbartl, K.; Gullstrand, P.; Sandström, P. Ischemic preconditioning prior to intermittent Pringle maneuver in liver resections. J. Hepatobiliary Pancreat. Sci. 2012, 19, 159–170. [Google Scholar] [CrossRef]
- Park, J.B.; Joh, J.W.; Kim, S.J.; Kwon, C.H.; Chun, J.M.; Kim, J.M.; Moon, J.I.; Lee, S.K. Effect of intermittent hepatic inflow occlusion with the Pringle maneuver during donor hepatectomy in adult living donor liver transplantation with right hemiliver grafts: A prospective, randomized controlled study. Liver Transpl. 2012, 18, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Ozgor, D.; Dirican, A.; Ates, M.; Gönültas, F.; Ara, C.; Yilmaz, S. Donor complications among 500 living donor liver transplantations at a single center. Transplant. Proc. 2012, 44, 1604–1607. [Google Scholar] [CrossRef]
- Yilmaz, S.; Akbulut, S.; Usta, S.; Ozsay, O.; Sahin, T.T.; Sarici, K.B.; Karabulut, E.; Baskiran, A.; Gonultas, F.; Ozdemir, F.; et al. Diagnostic and therapeutic management algorithm for biliary complications in living liver donors. Transpl. Int. 2021, 34, 2226–2237. [Google Scholar] [CrossRef]
- Camargo, C.A., Jr.; Madden, J.F.; Gao, W.; Selvan, R.S.; Clavien, P.A. Interleukin-6 protects liver against warm ischemia/reperfusion injury and promotes hepatocyte proliferation in the rodent. Hepatology 1997, 26, 1513–1520. [Google Scholar] [CrossRef] [PubMed]
- Cursio, R.; Gugenheim, J. Ischemia-Reperfusion Injury and Ischemic-Type Biliary Lesions following Liver Transplantation. J. Transplant. 2012, 2012, 164329. [Google Scholar] [CrossRef]
- Calne, R.Y.; Rolles, K.; White, D.J.; Thiru, S.; Evans, D.B.; McMaster, P.; Dunn, D.C.; Craddock, G.N.; Henderson, R.G.; Aziz, S.; et al. Cyclosporin A initially as the only immunosuppressant in 34 recipients of cadaveric organs: 32 kidneys, 2 pancreases, and 2 livers. Lancet 1979, 2, 1033–1036. [Google Scholar] [CrossRef]
- Starzl, T.E.; Todo, S.; Fung, J.; Demetris, A.J.; Venkataramman, R.; Jain, A. FK 506 for liver, kidney, and pancreas transplantation. Lancet 1989, 2, 1000–1004. [Google Scholar] [CrossRef]
- Koc, S.; Akbulut, S.; Soyer, V.; Yilmaz, M.; Barut, B.; Kutlu, R.; Yilmaz, S. Hepatic Venous Outflow Obstruction After Living-Donor Liver Transplant: Single Center Experience. Exp. Clin. Transplant. 2021, 19, 832–841. [Google Scholar] [CrossRef]
- Onghena, L.; Develtere, W.; Poppe, C.; Geerts, A.; Troisi, R.; Vanlander, A.; Berrevoet, F.; Rogiers, X.; Van Vlierberghe, H.; Verhelst, X. Quality of life after liver transplantation: State of the art. World J. Hepatol. 2016, 8, 749–756. [Google Scholar] [CrossRef]
- Imamura, H.; Kokudo, N.; Sugawara, Y.; Sano, K.; Kaneko, J.; Takayama, T.; Makuuchi, M. Pringle’s maneuver and selective inflow occlusion in living donor liver hepatectomy. Liver Transpl. 2004, 10, 771–778. [Google Scholar] [CrossRef]
- Jiménez-Castro, M.B.; Cornide-Petronio, M.E.; Gracia-Sancho, J.; Peralta, C. Inflammasome-Mediated Inflammation in Liver Ischemia-Reperfusion Injury. Cells 2019, 8, 1131. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; He, S.; Mao, X.; Zhang, Y.; Cai, Y.; Li, S. Effect of Hepatic Macrophage Polarization and Apoptosis on Liver Ischemia and Reperfusion Injury During Liver Transplantation. Front. Immunol. 2020, 11, 1193. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Chen, J.; Wei, Q.; Saeb-Parsy, K.; Xu, X. The Role of Ischemia/Reperfusion Injury in Early Hepatic Allograft Dysfunction. Liver Transpl. 2020, 26, 1034–1048. [Google Scholar] [CrossRef] [PubMed]
- Tokodai, K.; Lannsjö, C.; Kjaernet, F.; Romano, A.; Januszkiewicz, A.; Ericzon, B.G.; Nowak, G. Association of post-reperfusion syndrome and ischemia-reperfusion injury with acute kidney injury after liver transplantation. Acta Anaesthesiol. Scand. 2020, 64, 742–750. [Google Scholar] [CrossRef]
- Takatsuki, M.; Soyama, A.; Hidaka, M.; Kinoshita, A.; Adachi, T.; Kitasato, A.; Kuroki, T.; Eguchi, S. Prospective study of the safety and efficacy of intermittent inflow occlusion (Pringle maneuver) in living donor left hepatectomy. Hepatol. Res. 2015, 45, 856–862. [Google Scholar] [CrossRef]
- Khajeh, E.; Shafiei, S.; Al-Saegh, S.A.; Ramouz, A.; Hammad, A.; Ghamarnejad, O.; Al-Saeedi, M.; Rahbari, N.; Reissfelder, C.; Mehrabi, A.; et al. Meta-analysis of the effect of the pringle maneuver on long-term oncological outcomes following liver resection. Sci. Rep. 2021, 11, 3279. [Google Scholar] [CrossRef]
- Wei, X.; Zheng, W.; Yang, Z.; Liu, H.; Tang, T.; Li, X.; Liu, X. Effect of the intermittent Pringle maneuver on liver damage after hepatectomy: A retrospective cohort study. World J. Surg. Oncol. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed]
- Arab, H.A.; Sasani, F.; Rafiee, M.H.; Fatemi, A.; Javaheri, A. Histological and biochemical alterations in early-stage lobar ischemia-reperfusion in rat liver. World J. Gastroenterol. 2009, 15, 1951–1957. [Google Scholar] [CrossRef] [PubMed]
- De Lourdes Jorge, G.; Dos Reis Tártaro, R.; Fazzio Escanhoela, C.A.; Boin, I. Later Evaluation of Ischemia and Reperfusion by the Pringle Maneuver in Wistar Rats, Demonstrating That Hepatic Lesions Can Be Reversible. Transplant. Proc. 2017, 49, 898–901. [Google Scholar] [CrossRef] [PubMed]
- Qing, Z.S.; Zhang, X.S.; Gao, C.C.; Liu, W.D.; Xia, T.F.; Wu, K.; Pang, L.Q. Protective effect of ischemia preconditioning on ischemia-reperfusion injury in rat liver transplantation. Genet. Mol. Res. 2015, 14, 3018–3025. [Google Scholar] [CrossRef] [PubMed]
- Radojkovic, M.; Stojanovic, M.; Stanojevic, G.; Radojkovic, D.; Gligorijevic, J.; Ilic, I.; Stojanovic, N. Ischemic preconditioning vs adenosine vs prostaglandin E1 for protection against liver ischemia/reperfusion injury. Braz. J. Med. Biol. Res. 2017, 50, e6185. [Google Scholar] [CrossRef]
- Tártaro, R.D.; Jorge, G.D.; Leonardi, M.I.; Escanhoela, C.A.; Leonardi, L.S.; Boin, I.F. No protective function found in Wistar rats submitted to long ischemia time and reperfusion after intermittent clamping of the total hepatic pedicle. Transplant. Proc. 2015, 47, 1038–1041. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Donor Characteristics | Pringle Maneuver Applied (n = 27) | Pringle Maneuver Not Applied (n = 27) | p |
|---|---|---|---|
| Age | 29 (15) | 28 (14) | 0.165 |
| BMI | 24.5 (5.6) | 23.8 (6.1) | 0.716 |
| Future Remnant Liver Volume (%) | 32 (3) | 30 (2) | 0.319 |
| Gender [n (%)] | |||
| Male | 18 (67) | 16 (59) | |
| Female | 9 (33) | 11 (41) | |
| Liver graft [n (%)] | |||
| Right lobe | 23 (85.2) | 24 (88.8) | |
| Left lob | 4 (14.8) | 3 (11.1) | |
| WBC (PreOP) | 7.4 (2.1) | 7.4 (1.8) | 0.653 |
| WBC (POD5) | 7 (3.1) | 7.3 (2.4) | 0.489 |
| HB (PreOP) | 15.4 (3.1) | 14.9 (2.7) | 0.574 |
| HB (POD5) | 12.1 (3.1) | 11.9 (2.1) | 0.640 |
| PLT (PreOP) | 272 (106) | 265 (75) | 0.959 |
| PLT (POD5) | 206 (96) | 225 (44) | 0.299 |
| INR (PreOP) | 0.9 (0.1) | 0.9 (0.09) | 0.748 |
| INR (POD5) | 1 (0.1) | 1.1 (0.1) | 0.373 |
| Albumin (PreOP) | 4.5 (0.3) | 4.5 (0.5) | 0.689 |
| Albumin (POD5) | 3.3 (0.2) | 3.4 (0.4) | 0.274 |
| T. Bilirubin (PreOP) | 0.5 (0.2) | 0.5 (0.3) | 0.800 |
| T. Bilirubin (POD5) | 1.1 (0.8) | 1 (0.7) | 0.267 |
| D. Bilirubin (PreOP) | 0.1 (0.07) | 0.1 (0.09) | 0.869 |
| D. Bilirubin (POD5) | 0.3 (0.3) | 0.3 (0.3) | 0.710 |
| AST (PreOP) | 18 (6) | 19 (8) | 0.482 |
| AST (POD5) | 59 (26) | 63 (36) | 0.986 |
| ALT (PreOP) | 16 (7) | 16 (9) | 0.537 |
| ALT (POD5) | 106 (78) | 115 (57) | 0.809 |
| ALP PreOP | 70 (27) | 67 (30) | 0.842 |
| ALP (POD5) | 81 (51) | 89 (40) | 0.993 |
| GGT (PreOP) | 13 (36) | 17 (8) | 0.222 |
| GGT (POD5) | 44 (72) | 50 (69) | 0.406 |
| LDH (PreOP) | 184 (30) | 171 (49) | 0.287 |
| LDH (POD5) | 242 (75) | 295 (119) | 0.213 |
| Donor Characteristics [Median (IQR)] | Pringle Maneuver Applied (n = 27) | Pringle Maneuver Not Applied (n = 27) | p |
|---|---|---|---|
| IL-1 (PreOP) | 42 (135) | 40 (89) | 0.424 |
| IL-1 (POD0) | 42 (134) | 51 (74) | 0.735 |
| IL-1 (POD1) | 43 (136) | 46 (92) | 0.531 |
| IL-1 (POD2) | 47 (132) | 46 (66) | 0.788 |
| IL-1 (POD3) | 52 (132) | 48 (73) | 0.309 |
| IL-2 (PreOP) | 290 (1016) | 330 (651) | 0.780 |
| IL-2 (POD0) | 281 (1045) | 334 (448) | 0.754 |
| IL-2 (POD1) | 286 (939) | 338 (637) | 0.842 |
| IL-2 (POD2) | 289 (1009) | 300 (556) | 0.910 |
| IL-2 (POD3) | 304 (1018) | 318 (564) | 0.689 |
| IL-6 (PreOP) | 92 (262) | 100 (194) | 0.682 |
| IL-6 (POD0) | 111 (251) | 104 (183) | 0.429 |
| IL-6 (POD1) | 102 (261) | 106 (176) | 0.828 |
| IL-6 (POD2) | 95 (235) | 104 (178) | 0.958 |
| IL-6 (POD3) | 98 (254) | 100 (115) | 0.544 |
| TNF-α (PreOP) | 132 (323) | 107 (255) | 0.677 |
| TNF-α (POD0) | 116 (352) | 120 (197) | 0.795 |
| TNF-α (POD1) | 127 (258) | 116 (221) | 0.965 |
| TNF-α (POD2) | 135 (333) | 123 (256) | 0.795 |
| TNF-α (POD3) | 122 (413) | 123 (170) | 0.476 |
| B-gal (PreOP) | 132 (404) | 162 (399) | 0.806 |
| B-gal (POD0) | 136 (387) | 176 (286) | 0.965 |
| B-gal (POD1) | 174 (389) | 159 (213) | 0.965 |
| B-gal (POD2) | 165 (375) | 168 (323) | 0.917 |
| B-gal (POD3) | 152 (383) | 154 (229) | 0.896 |
| Recipient Characteristics [Median (IQR)] | Pringle Maneuver Applied (n = 27) | Pringle Maneuver Not Applied (n = 27) | p |
|---|---|---|---|
| Age | 54 (23) | 53 (23) | 0.959 |
| BMI | 27.1 (6) | 25.1 (5.5) | 0.545 |
| Gender [n (%)] | 0.259 | ||
| Male | 15 (56) | 19 (70) | |
| Female | 12 (44) | 8 (30) | |
| MELD | 20 (7) | 18 (7) | 0.631 |
| Graft weight (gr) | 700 (270) | 760 (178) | 0.736 |
| Cold ischemia time (min) | 93 (40) | 95 (49) | 0.634 |
| Warm ischemia time (min) | 47 (25) | 54 (20) | 0.121 |
| WBC PreOP | 3.9 (2.1) | 5 (2.4) | 0.054 |
| WBC POD5 | 5.4 (5.6) | 6.8 (4.2) | 0.528 |
| Hb PreOP | 9.9 (2.4) | 11.1 (4.4) | 0.100 |
| Hb POD5 | 8.8 (1.2) | 8.8 (1.5) | 0.729 |
| Plt PreOP | 86 (72) | 103 (73) | 0.104 |
| Plt POD5 | 52 (49) | 56 (42) | 0.279 |
| INR PreOP | 1.5 (0.4) | 1.4 (0.3) | 0.775 |
| INR POD5 | 1.4 (0.4) | 1.3 (0.3) | 0.337 |
| Alb PreOP | 3 (1.5) | 2.8 (0.9) | 0.430 |
| Alb POD5 | 3.2 (0.5) | 3.3 (0.6) | 0.238 |
| T. Bilirubin PreOP | 2.1 (4.1) | 2.3 (5.5) | 0.171 |
| T. Bilirubin POD5 | 3.9 (3.6) | 3.1 (4.3) | 0.421 |
| D. Bilirubin PreOP | 0.6 (2.3) | 0.8 (2.9) | 0.177 |
| D. Bilirubin POD5 | 1.8 (3) | 1.7 (2.9) | 0.324 |
| AST PreOP | 42 (35) | 71 (86) | 0.059 |
| AST POD5 | 64 (25) | 52 (47) | 0.368 |
| ALT PreOP | 29 (25) | 39 (31) | 0.019 |
| ALT POD5 | 161 (146) | 136 (75) | 0.137 |
| ALP PreOP | 124 (77) | 141 (101) | 0.406 |
| ALP POD5 | 76 (50) | 72 (40) | 0.672 |
| GGT PreOP | 47 (84) | 85 (71) | 0.113 |
| GGT POD5 | 104 (156) | 104 (136) | 0.742 |
| LDH PreOP | 220 (95) | 258 (105) | 0.071 |
| LDH POD5 | 217 (109) | 221 (94) | 0.789 |
| Ammonia PreOP | 160 | 171 | 0.513 |
| Ammonia POD 5 | 87 (48) | 89 (65) | 0.606 |
| Recipient Characteristics [Median (IQR)] | Pringle Maneuver Applied (n = 27) | Pringle Maneuver Not Applied (n = 27) | p |
|---|---|---|---|
| IL-1 PreOP | 39 (63) | 39 (58) | 0.577 |
| IL-1 POD0 | 56 (123) | 48 (45) | 0.112 |
| IL-1 POD1 | 60 (123) | 53 (34) | 0.152 |
| IL-1 POD2 | 68 (125) | 57 (44) | 0.339 |
| IL-1 POD3 | 65 (126) | 55 (36) | 0.249 |
| IL-2 PreOP | 280 (307) | 245 (503) | 0.573 |
| IL-2 POD0 | 376 (992) | 366 (502) | 0.340 |
| IL-2 POD1 | 368 (958) | 384 (319) | 0.331 |
| IL-2 POD2 | 498 (932) | 447 (508) | 0.434 |
| IL-2 POD3 | 480 (984) | 380 (386) | 0.657 |
| IL-6 PreOP | 93 (84) | 79 (100) | 0.331 |
| IL-6 POD0 | 112 (249) | 101 (88) | 0.224 |
| IL-6 POD1 | 114 (245) | 98 (77) | 0.129 |
| IL-6 POD2 | 119 (247) | 103 (96) | 0.384 |
| IL-6 POD3 | 116 (248) | 109 (76) | 0.440 |
| TNF-a PreOP | 106 (170) | 94 (138) | 0.390 |
| TNF-a POD0 | 169 (408) | 111 (191) | 0.132 |
| TNF-a POD1 | 158 (394) | 128 (101) | 0.087 |
| TNF-a POD2 | 170 (396) | 158 (135) | 0.708 |
| TNF-a POD3 | 193 (402) | 135 (140) | 0.215 |
| B-gal PreOP | 140 (174) | 118 (135) | 0.242 |
| B-gal POD0 | 199 (382) | 144 (231) | 0.138 |
| B-gal POD1 | 206 (373) | 164 (173) | 0.150 |
| B-gal POD2 | 185 (370) | 203 (207) | 0.348 |
| B-gal POD3 | 245 (388) | 196 (132) | 0.366 |
| Histopathological Scores [Ortanca (IQR)] | Pringle Maneuver Applied (n = 25) | Pringle Maneuver Not Applied (n = 26) | p |
|---|---|---|---|
| Inflammatory cell infiltration | 1 (0) | 1 (0) | 0.334 |
| Hepatocyte damage | 2 (1) | 1 (1) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalda, Y.; Akbulut, S.; Sahin, T.T.; Tuncer, A.; Ogut, Z.; Satilmis, B.; Dalda, O.; Gul, M.; Yilmaz, S. The Effect of Pringle Maneuver Applied during Living Donor Hepatectomy on the Ischemia-Reperfusion Injury Observed in the Donors and Recipients. Medicina 2024, 60, 649. https://doi.org/10.3390/medicina60040649
Dalda Y, Akbulut S, Sahin TT, Tuncer A, Ogut Z, Satilmis B, Dalda O, Gul M, Yilmaz S. The Effect of Pringle Maneuver Applied during Living Donor Hepatectomy on the Ischemia-Reperfusion Injury Observed in the Donors and Recipients. Medicina. 2024; 60(4):649. https://doi.org/10.3390/medicina60040649
Chicago/Turabian StyleDalda, Yasin, Sami Akbulut, Tevfik Tolga Sahin, Adem Tuncer, Zeki Ogut, Basri Satilmis, Ozlem Dalda, Mehmet Gul, and Sezai Yilmaz. 2024. "The Effect of Pringle Maneuver Applied during Living Donor Hepatectomy on the Ischemia-Reperfusion Injury Observed in the Donors and Recipients" Medicina 60, no. 4: 649. https://doi.org/10.3390/medicina60040649