
Use of Reverse Shock Index Multiplied by Simplified Motor Score in a Five-Level Triage System: Identifying Trauma in Adult Patients at a High Risk of Mortality
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Cohort
2.2. TTAS System
2.3. Variable Measurements
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
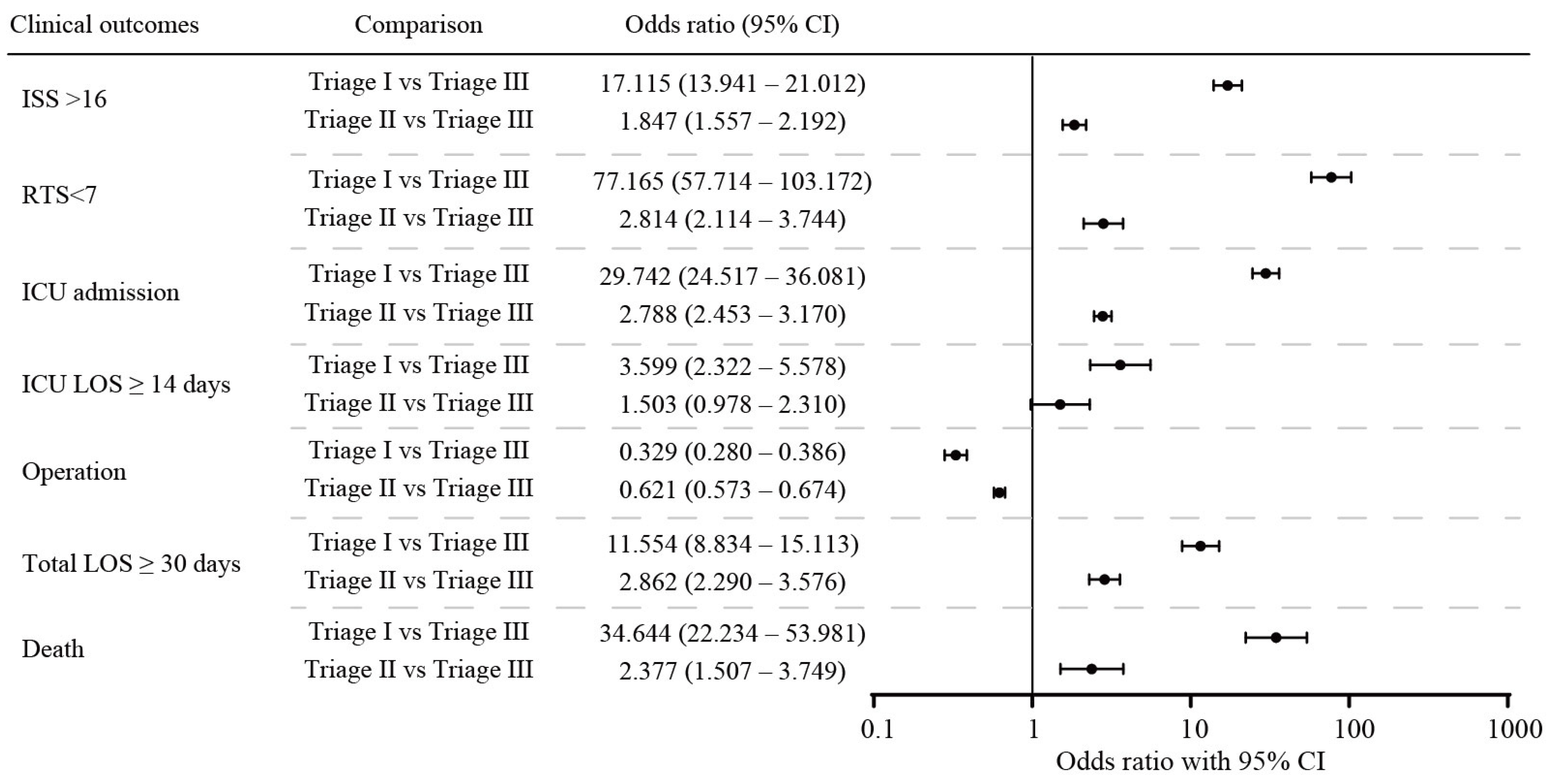
3.2. Prioritization Performance of Patients Using the TTAS System
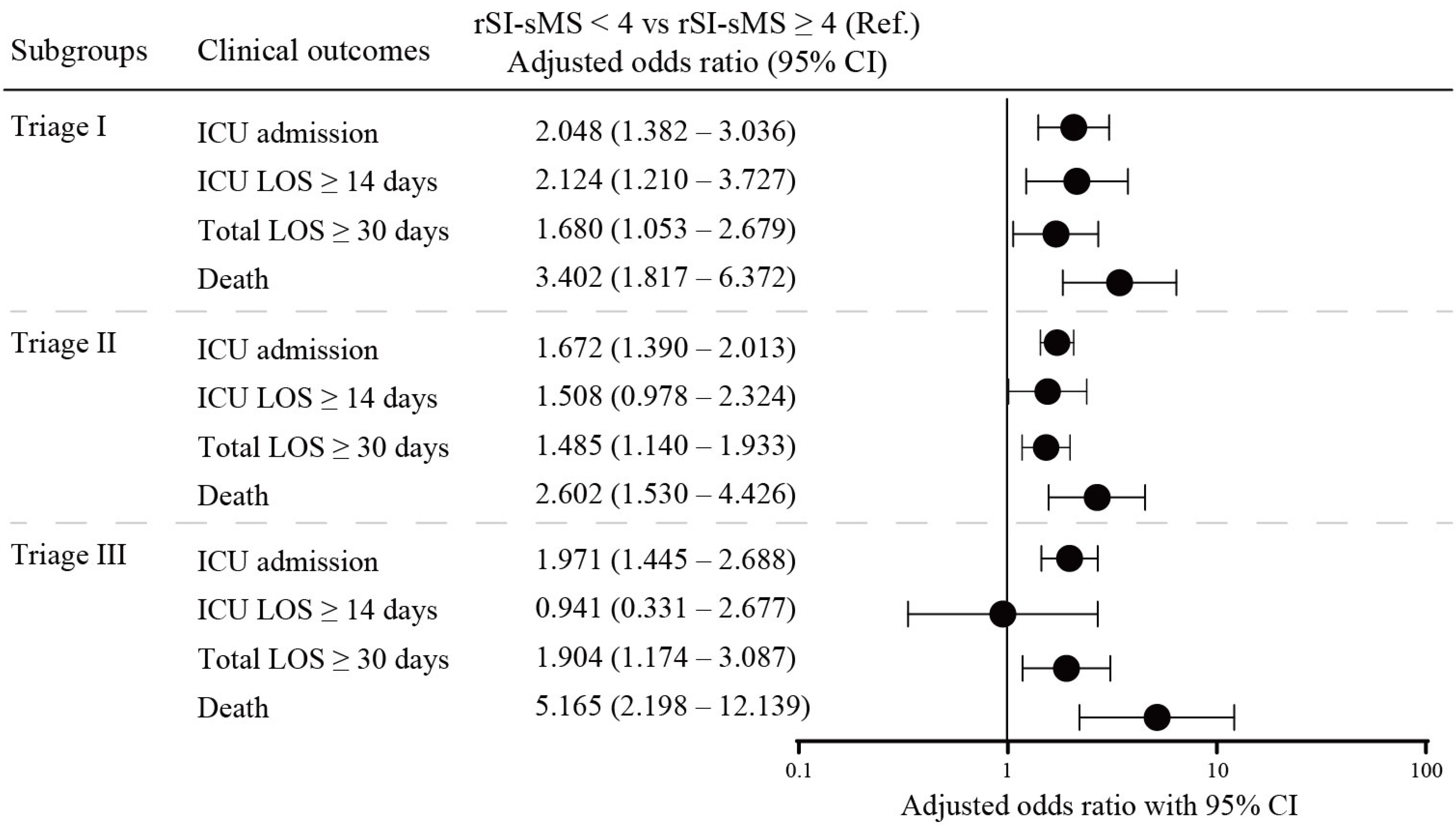
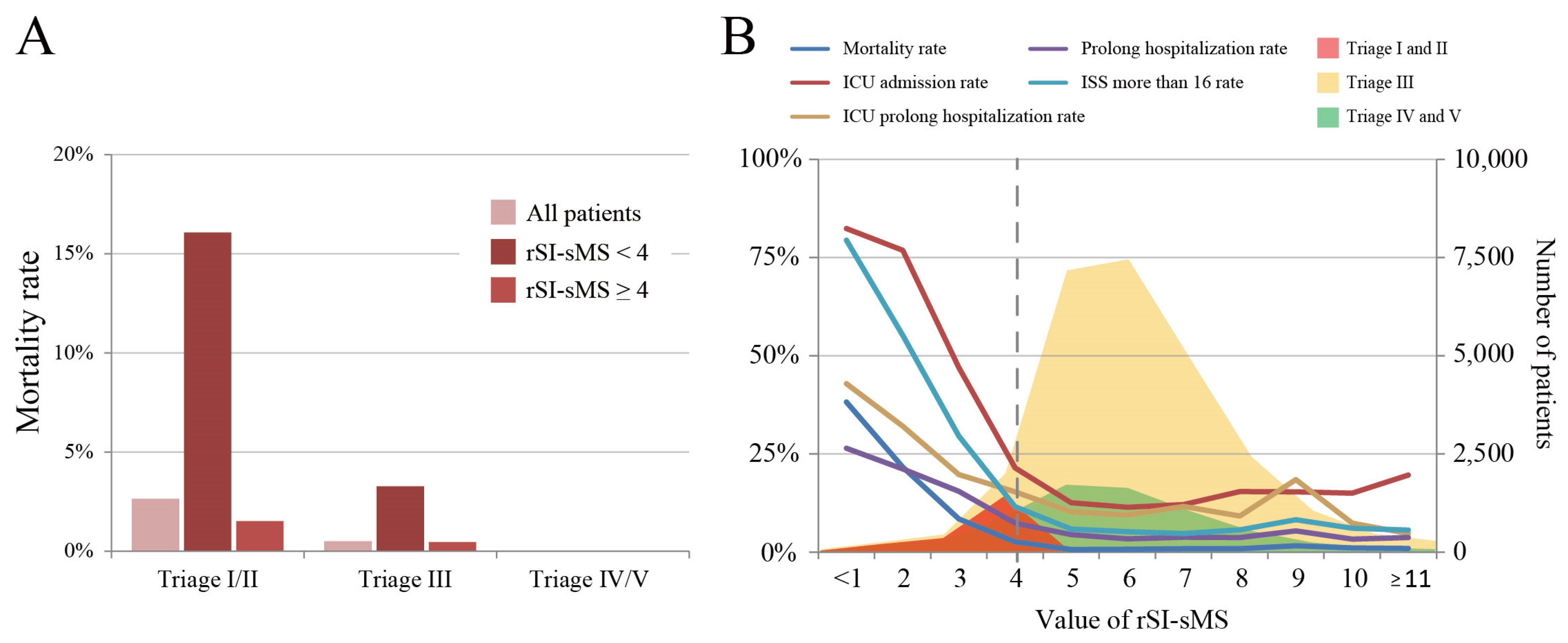
3.3. Risk Stratification Based on rSI-sMS < 4 in the TTAS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, M.-Y.; Lin, P.-C.; Liu, C.-Y.; Tzeng, I.-S.; Hsieh, T.-H.; Chang, C.-Y.; Hou, Y.-T.; Chen, Y.-L.; Chien, D.-S.; Yiang, G.-T. The impact of holiday season and weekend effect on traumatic injury mortality: Evidence from a 10-year analysis. Tzu Chi Med. J. 2023, 35, 69–77. [Google Scholar] [CrossRef]
- Dong, S.L.; Bullard, M.J.; Meurer, D.P.; Colman, I.; Blitz, S.; Holroyd, B.R.; Rowe, B.H. Emergency triage: Comparing a novel computer triage program with standard triage. Acad. Emerg. Med. 2005, 12, 502–507. [Google Scholar] [CrossRef]
- Wuerz, R.C.; Milne, L.W.; Eitel, D.R.; Travers, D.; Gilboy, N. Reliability and validity of a new five-level triage instrument. Acad. Emerg. Med. 2000, 7, 236–242. [Google Scholar] [CrossRef]
- Cronin, J. The introduction of the Manchester triage scale to an emergency department in the Republic of Ireland. Accid. Emerg. Nurs. 2003, 11, 121–125. [Google Scholar] [CrossRef]
- Ng, C.-J.; Yen, Z.-S.; Tsai, J.C.-H.; Chen, L.C.; Lin, S.J.; Sang, Y.Y.; Chen, J.-C. TTAS national working group Validation of the Taiwan triage and acuity scale: A new computerised five-level triage system. Emerg. Med. J. 2010, 28, 1026–1031. [Google Scholar] [CrossRef]
- Chang, Y.-C.; Ng, C.-J.; Wu, C.-T.; Chen, L.-C.; Chen, J.-C.; Hsu, K.-H. Effectiveness of a five-level Paediatric Triage System: An analysis of resource utilisation in the emergency department in Taiwan. Emerg. Med. J. 2012, 30, 735–739. [Google Scholar] [CrossRef]
- Jelinek, G.A.; Little, M. Inter-rater reliability of the National Triage Scale over 11,500 simulated occasions of triage. Emerg. Med. 1996, 8, 226–230. [Google Scholar] [CrossRef]
- Shelton, R. The emergency severity index 5-level triage system. Dimens. Crit. Care Nurs. 2009, 28, 9–12. [Google Scholar] [CrossRef]
- Levin, S.; Toerper, M.; Hamrock, E.; Hinson, J.S.; Barnes, S.; Gardner, H.; Dugas, A.; Linton, B.; Kirsch, T.; Kelen, G. Machine-Learning-Based Electronic Triage More Accurately Differentiates Patients with Respect to Clinical Outcomes Compared With the Emergency Severity Index. Ann. Emerg. Med. 2018, 71, 565–574.e2. [Google Scholar] [CrossRef]
- Chmielewski, N.D.; Moretz, J.M. ESI Triage Distribution in U.S. Emergency Departments. Adv. Emerg. Nurs. J. 2022, 44, 46–53. [Google Scholar] [CrossRef]
- Mirhaghi, A.; Heydari, A.; Mazlom, R.; Hasanzadeh, F. Reliability of the Emergency Severity Index: Meta-analysis. Sultan Qaboos Univ. Med. J. 2015, 15, e71–e77. [Google Scholar] [PubMed]
- Ebrahimi, M.; Heydari, A.; Mazlom, R.; Mirhaghi, A. The reliability of the Australasian Triage Scale: A meta-analysis. World J. Emerg. Med. 2015, 6, 94–99. [Google Scholar] [CrossRef]
- Zachariasse, J.M.; Seiger, N.; Rood, P.P.M.; Alves, C.F.; Freitas, P.; Smit, F.J.; Roukema, G.R.; Moll, H.A. Validity of the Manchester Triage System in emergency care: A prospective observational study. PLoS ONE 2017, 12, e0170811. [Google Scholar] [CrossRef]
- Zakeri, H.; Saleh, L.A.; Niroumand, S.; Ziadi-Lotfabadi, M. Comparison the Emergency Severity Index and Manchester Triage System in Trauma Patients. Bull. Emerg. Trauma 2022, 10, 65–70. [Google Scholar] [CrossRef]
- Zachariasse, J.M.; van der Hagen, V.; Seiger, N.; Mackway-Jones, K.; van Veen, M.; Moll, H.A. Performance of triage systems in emergency care: A systematic review and meta-analysis. BMJ Open 2019, 9, e026471. [Google Scholar] [CrossRef]
- Chien, D.-S.; Yiang, G.-T.; Liu, C.-Y.; Tzeng, I.-S.; Chang, C.-Y.; Hou, Y.-T.; Chen, Y.-L.; Lin, P.-C.; Wu, M.-Y. Association of In-Hospital Mortality and Trauma Team Activation: A 10-Year Study. Diagnostics 2022, 12, 2334. [Google Scholar] [CrossRef]
- Ng, C.-J.; Hsu, K.-H.; Kuan, J.-T.; Chiu, T.-F.; Chen, W.-K.; Lin, H.-J.; Bullard, M.J.; Chen, J.-C. Comparison Between Canadian Triage and Acuity Scale and Taiwan Triage System in Emergency Departments. J. Formos. Med. Assoc. 2010, 109, 828–837. [Google Scholar] [CrossRef]
- Xiang, H.; Wheeler, K.K.; Groner, J.I.; Shi, J.; Haley, K.J. Undertriage of major trauma patients in the US emergency departments. Am. J. Emerg. Med. 2014, 32, 997–1004. [Google Scholar] [CrossRef]
- Newgard, C.D.M.; Fischer, P.E.; Gestring, M.; Michaels, H.N.; Jurkovich, G.J.M.; Lerner, E.B.P.; Fallat, M.E.; Delbridge, T.R.; Brown, J.B.M.; Bulger, E.M.; et al. National guideline for the field triage of injured patients: Recommendations of the National Expert Panel on Field Triage, 2021. J. Trauma Acute Care Surg. 2022, 93, e49–e60. [Google Scholar] [CrossRef]
- Kuo, S.C.H.; Kuo, P.-J.; Hsu, S.-Y.; Rau, C.-S.; Chen, Y.-C.; Hsieh, H.-Y.; Hsieh, C.-H. The use of the reverse shock index to identify high-risk trauma patients in addition to the criteria for trauma team activation: A cross-sectional study based on a trauma registry system. BMJ Open 2016, 6, e011072. [Google Scholar] [CrossRef]
- Chang, W.; Liu, H.-E.; Goopy, S.; Chen, L.-C.; Chen, H.-J.; Han, C.-Y. Using the Five-Level Taiwan Triage and Acuity Scale Computerized System: Factors in Decision Making by Emergency Department Triage Nurses. Clin. Nurs. Res. 2016, 26, 651–666. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-K.; Niu, K.-Y.; Seak, C.-J.; Weng, Y.-M.; Wang, J.-H.; Lai, P.-F. Comparison between simple triage and rapid treatment and Taiwan Triage and Acuity Scale for the emergency department triage of victims following an earthquake-related mass casualty incident: A retrospective cohort study. World J. Emerg. Surg. 2020, 15, 20. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.-Y.; Hou, Y.-T.; Chung, J.-Y.; Yiang, G.-T. Reverse shock index multiplied by simplified motor score as a predictor of clinical outcomes for patients with COVID-19. BMC Emerg. Med. 2024, 24, 26. [Google Scholar] [CrossRef] [PubMed]
- Dallaire, C.; Poitras, J.; Aubin, K.; Lavoie, A.; Moore, L. Emergency department triage: Do experienced nurses agree on triage scores? J. Emerg. Med. 2012, 42, 736–740. [Google Scholar] [CrossRef]
- Chuang, J.-F.; Rau, C.-S.; Wu, S.-C.; Liu, H.-T.; Hsu, S.-Y.; Hsieh, H.-Y.; Chen, Y.-C.; Hsieh, C.-H. Use of the reverse shock index for identifying high-risk patients in a five-level triage system. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 12. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Triage I | Triage II | Triage III | Triage IV/V | p-Value |
|---|---|---|---|---|---|
| Patient number | 711 (6.0%) | 6080 (51.7%) | 4914 (41.8%) | 55 (0.5%) | |
| Age (years) | 56 (39–74) | 59 (43–77) | 63 (47–77) | 52 (36–62) | <0.001 |
| Age < 65 ys | 438 (61.6%) | 3562 (58.6%) | 2642 (53.8%) | 43 (78.2%) | <0.001 |
| Age ≥ 65 ys | 273 (38.4%) | 2518 (41.4%) | 2272 (46.2%) | 12 (21.8%) | |
| Sex, n (%) | <0.001 | ||||
| Female | 257 (36.1%) | 2772 (45.6%) | 2577 (52.4%) | 25 (45.5%) | |
| Male | 454 (63.9%) | 3308 (54.4%) | 2337 (47.6%) | 30 (54.5%) | |
| Vital sign | |||||
| SBP | 143 (115–170) | 147 (127–169) | 148 (129–165) | 141 (122–154) | <0.001 |
| DBP | 81.5 (68–96) | 85 (74–97) | 85 (76–95) | 81 (73–93) | <0.001 |
| HR | 88 (76–105) | 84 (74–96) | 82 (72–93) | 85 (72–97) | <0.001 |
| RR | 19 (18–20) | 18 (18–20) | 18 (18–20) | 18 (18–20) | <0.001 |
| GCS score | 14 (7–15) | 15 (15–15) | 15 (15–15) | 15 (15–15) | |
| Injury score systems | |||||
| rSIsms | 3.5 (2.0–5.0) | 5.2 (4.3–6.3) | 5.4 (4.5–6.3) | 4.8 (4.1–5.8) | <0.001 |
| rSIsms < 4 | 425 (59.8%) | 1069 (17.6%) | 625 (12.7%) | 13 (23.6%) | <0.001 |
| rSIsms ≥ 4 | 286 (40.2%) | 5011 (82.4%) | 4289 (87.3%) | 42 (76.4%) | |
| Injury severity | |||||
| RTS | 7.1 (6.0–7.8) | 7.8 (7.8–7.8) | 7.8 (7.8–7.8) | 7.8 (7.8–7.8) | <0.001 |
| RTS < 7 | 353 (49.6%) | 211 (3.5%) | 62 (1.3%) | 0 (0.0%) | <0.001 |
| ISS | 11 (9–20) | 9 (4–9) | 9 (4–9) | 4 (4–9) | <0.001 |
| ISS ≥ 16 | 300 (42.2%) | 444 (7.3%) | 201 (4.1%) | 2 (3.6%) | <0.001 |
| Isolated head injury * | 281 (39.5%) | 1080 (17.8%) | 500 (10.2%) | 10 (18.2%) | <0.001 |
| Injury type | <0.001 | ||||
| Penetration | 57 (8.0%) | 366 (6.0%) | 142 (2.9%) | 1 (1.8%) | |
| Non-penetration | 654 (92.0%) | 5714 (94.0%) | 4772 (97.1%) | 54 (98.2%) | |
| Mechanism of injury | <0.001 | ||||
| Road transport | 333 (46.8%) | 2255 (37.1%) | 1691 (34.4%) | 20 (36.4%) | |
| Low fall | 142 (20.0%) | 2298 (37.8%) | 2264 (46.1%) | 19 (34.5%) | |
| High fall | 129 (18.1%) | 789 (13.0%) | 556 (11.3%) | 5 (9.1%) | |
| Others | 107 (15.0%) | 738 (12.1%) | 403 (8.2%) | 11 (20.0%) | |
| Comorbidity | |||||
| CNS diseases | 48 (6.8%) | 405 (6.7%) | 283 (5.8%) | 0 (0.0%) | 0.052 |
| CVD | 142 (20.0%) | 1791 (29.5%) | 1626 (33.1%) | 9 (16.4%) | <0.001 |
| Respiratory diseases | 13 (1.8%) | 155 (2.5%) | 109 (2.2%) | 1 (1.8%) | 0.510 |
| CKD | 19 (2.7%) | 206 (3.4%) | 150 (3.1%) | 1 (1.8%) | 0.568 |
| Diabetes mellitus | 63 (8.9%) | 770 (12.7%) | 683 (13.9%) | 3 (5.5%) | 0.001 |
| ICU care | |||||
| ICU admission | 491 (69.1%) | 1052 (17.3%) | 343 (7.0%) | 5 (9.1%) | <0.001 |
| Re-admission ICU | 8 (1.1%) | 27 (0.4%) | 9 (0.2%) | 0 (0.0%) | 0.001 |
| ICU LOS, days | 6 (3–13) | 4 (3–7) | 4 (3–6) | 2 (2–3) | <0.001 |
| LOS < 14 days | 372 (75.8%) | 928 (88.2%) | 315 (91.8%) | 5 (100.0%) | <0.001 |
| LOS ≥ 14 days | 119 (24.2%) | 124 (11.8%) | 28 (8.2%) | 0 (0.0%) | |
| Surgical intervention | |||||
| Operation | 327 (46.0%) | 3748 (61.6%) | 3544 (72.1%) | 29 (52.7%) | <0.001 |
| Re-operation | 75 (10.5%) | 188 (3.1%) | 81 (1.6%) | 0 (0.0%) | <0.001 |
| Complications | 176 (24.8%) | 830 (13.7%) | 165 (3.4%) | 2 (3.6%) | <0.001 |
| Total LOS | 11 (5–25) | 6 (4–10) | 6 (4–8) | 5 (3–7) | <0.001 |
| <30 days | 570 (80.2%) | 5279 (94.2%) | 4811 (97.9%) | 54 (98.2%) | <0.001 |
| ≥30 days | 141 (19.8%) | 351 (5.8%) | 103 (2.1%) | 1 (1.8%) |
| Outcomes | Triage I | Triage II | Triage III | Triage IV/V | ||||
|---|---|---|---|---|---|---|---|---|
| rSI-sMS < 4 | rSI-sMS ≥ 4 | rSI-sMS < 4 | rSI-sMS ≥ 4 | rSI-sMS < 4 | rSI-sMS ≥ 4 | rSI-sMS < 4 | rSI-sMS ≥ 4 | |
| Patient number | 425 (59.8%) | 286 (40.2%) | 1069 (17.6%) | 5011 (82.4%) | 625 (12.7%) | 4289 (87.3%) | 13 (23.6%) | 42 (76.4%) |
| Injury severity | ||||||||
| ISS ≥ 16 | 241 (56.7%) *** | 59 (20.6%) *** | 134 (12.5%) *** | 310 (6.2%) *** | 40 (6.4%) ** | 161 (3.8%) ** | 0 (0.0%) | 2 (4.8%) |
| RTS < 7 | 315 (74.1%) *** | 38 (13.3%) *** | 147 (13.8%) *** | 64 (1.3%) *** | 39 (6.2%) *** | 23 (0.5%) *** | 0 (0.0%) | 0 (0.0%) |
| ICU care | ||||||||
| ICU admission | 334 (78.6%) *** | 157 (54.9%) *** | 267 (25.0%) *** | 785 (15.7%) *** | 70 (11.2%) *** | 273 (6.4%) *** | 1 (7.7%) | 4 (9.5%) |
| Re-admission ICU | 7 (1.6%) | 1 (0.3%) | 9 (0.8%) * | 18 (0.4%) * | 3 (0.5%) | 6 (0.1%) | 0 (0.0%) | 0 (0.0%) |
| ICU LOS ≥ 14 days | 98 (29.3%) *** | 21 (13.4%) *** | 39 (14.6%) | 85 (10.8%) | 5 (7.1%) | 23 (8.4%) | 0 (0.0%) | 0 (0.0%) |
| Surgical intervention | ||||||||
| Operation | 211 (49.6%) * | 116 (40.6%) * | 640 (59.9%) | 3108 (62.0%) | 425 (68.0%) * | 3119 (72.7%) * | 6 (46.2%) | 23 (54.8%) |
| Re-operation | 57 (13.4%) ** | 18 (6.3%) ** | 54 (5.1%) *** | 134 (2.7%) *** | 18 (2.9%) ** | 63 (1.5%) ** | 0 (0.0%) | 0 (0.0%) |
| Complications | 121 (28.5%) ** | 55 (19.2%) ** | 197 (18.4%) *** | 633 (12.6%) *** | 40 (6.4%) *** | 125 (2.9%) *** | 0 (0.0%) | 2 (4.8%) |
| Total LOS ≥ 30 days | 106 (24.9%) *** | 35 (12.2%) *** | 89 (8.3%) *** | 262 (5.2%) *** | 24 (3.8%) *** | 79 (1.8%) *** | 0 (0.0%) | 1 (2.4%) |
| Death | 91 (21.4%) *** | 16 (5.6%) *** | 25 (2.3%) *** | 48 (1.0%) *** | 9 (1.4%) *** | 16 (0.4%) *** | 0 (0.0%) | 0 (0.0%) |
| Scoring Systems | Mortality | ICU Admission | Prolong ICU Stay | Prolong Total Hospital Stay | ||||
|---|---|---|---|---|---|---|---|---|
| AUROC (95% CI) | p-Value | AUROC (95% CI) | p-Value | AUROC (95% CI) | p-Value | AUROC (95% CI) | p-Value | |
| SI | 0.505 (0.458–0.552) | 0.819 | 0.522 (0.506–0.537) | 0.003 | 0.527 (0.488–0.567) | 0.147 | 0.547 (0.522–0.573) | <0.001 |
| mSI | 0.541 (0.495–0.587) | 0.046 | 0.535 (0.519–0.550) | <0.001 | 0.545 (0.506–0.584) | 0.018 | 0.559 (0.534–0.584) | <0.001 |
| rSI-sMS | 0.733 (0.688–0.778) | <0.001 | 0.605 (0.590–0.621) | <0.001 | 0.623 (0.584–0.662) | <0.001 | 0.616 (0.591–0.642) | <0.001 |
| Triage | 0.780 (0.743–0.816) | <0.001 | 0.702 (0.689–0.715) | <0.001 | 0.621 (0.584–0.657) | <0.001 | 0.676 (0.654–0.699) | <0.001 |
| Triage + SI | 0.770 (0.733–0.807) | <0.001 | 0.699 (0.686–0.713) | <0.001 | 0.617 (0.579–0.655) | <0.001 | 0.689 (0.667–0.711) | <0.001 |
| Triage + mSI | 0.780 (0.744–0.816) | <0.001 | 0.703 (0.690–0.717) | <0.001 | 0.623 (0.585–0.660) | <0.001 | 0.692 (0.670–0.713) | <0.001 |
| Triage + rSI-sMS | 0.797 (0.759–0.835) | <0.001 | 0.714 (0.701–0.728) | <0.001 | 0.641 (0.603–0.679) | <0.001 | 0.699 (0.677–0.721) | <0.001 |
| Outcomes. | Triage I/II | Triage III | Triage IV/V | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sens. | Spec. | PLR | NLR | Sens. | Spec. | PLR | NLR | Sens. | Spec. | PLR | NLR | |
| ISS ≥ 16 | 50.40% | 81.49% | 2.72 | 0.61 | 19.9% | 87.6% | 1.60 | 0.91 | ---- | ---- | ---- | ---- |
| ICU admission | 39.0% | 83.0% | 2.29 | 0.73 | 20.4% | 87.9% | 1.68 | 0.91 | 20.0% | 76.0% | 0.83 | 1.05 |
| ICU LOS ≥ 14 days | 56.4% | 64.3% | 1.58 | 0.68 | 17.9% | 79.4% | 0.86 | 1.03 | ---- | ---- | ---- | ---- |
| Operation | 20.9% | 76.3% | 0.88 | 1.04 | 12.0% | 85.4% | 0.82 | 1.03 | 20.7% | 73.1% | 0.77 | 1.08 |
| Total LOS ≥ 30 days | 39.6% | 79.4% | 1.92 | 0.76 | 23.3% | 87.5% | 1.86 | 0.88 | ---- | ---- | ---- | ---- |
| Death | 64.4% | 79.2% | 3.10 | 0.45 | 36.0% | 87.4% | 2.86 | 0.73 | ---- | ---- | ---- | ---- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, P.-C.; Wu, M.-Y.; Chien, D.-S.; Chung, J.-Y.; Liu, C.-Y.; Tzeng, I.-S.; Hou, Y.-T.; Chen, Y.-L.; Yiang, G.-T. Use of Reverse Shock Index Multiplied by Simplified Motor Score in a Five-Level Triage System: Identifying Trauma in Adult Patients at a High Risk of Mortality. Medicina 2024, 60, 647. https://doi.org/10.3390/medicina60040647
Lin P-C, Wu M-Y, Chien D-S, Chung J-Y, Liu C-Y, Tzeng I-S, Hou Y-T, Chen Y-L, Yiang G-T. Use of Reverse Shock Index Multiplied by Simplified Motor Score in a Five-Level Triage System: Identifying Trauma in Adult Patients at a High Risk of Mortality. Medicina. 2024; 60(4):647. https://doi.org/10.3390/medicina60040647
Chicago/Turabian StyleLin, Po-Chen, Meng-Yu Wu, Da-Sen Chien, Jui-Yuan Chung, Chi-Yuan Liu, I-Shiang Tzeng, Yueh-Tseng Hou, Yu-Long Chen, and Giou-Teng Yiang. 2024. "Use of Reverse Shock Index Multiplied by Simplified Motor Score in a Five-Level Triage System: Identifying Trauma in Adult Patients at a High Risk of Mortality" Medicina 60, no. 4: 647. https://doi.org/10.3390/medicina60040647