Total Exenteration En Bloc with a Nephrectomy for Locally Advanced Cervical Cancer Invading a Pelvic Kidney—A Case Report and Literature Review


 ,
,
Abstract
:1. Introduction
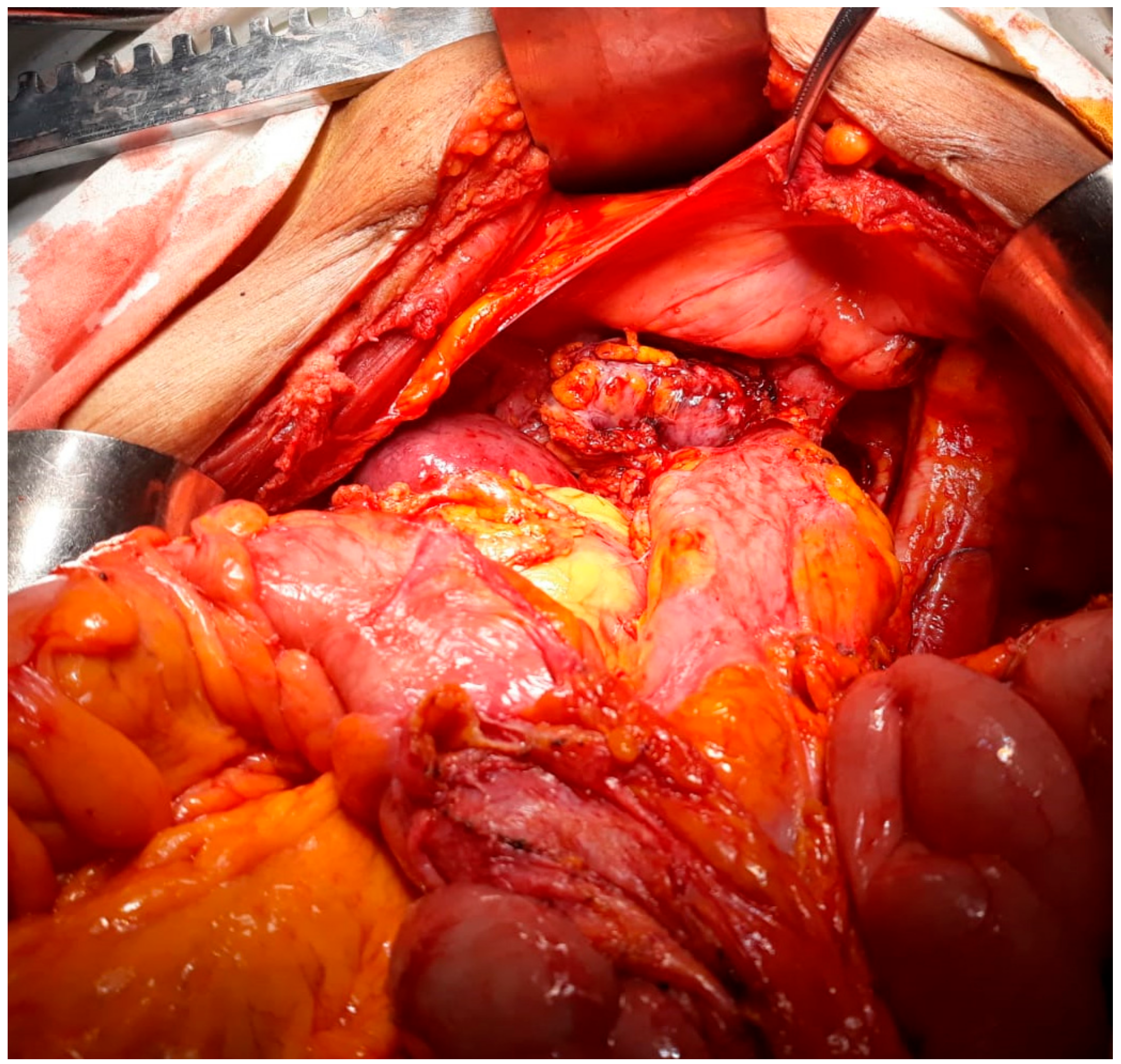
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bakri, Y.N.; Mansi, M.; Sundin, T. Stage IIB carcinoma of the cervix complicated by an ectopic pelvic kidney. Int. J. Gynaecol. Obstet. 1993, 42, 174–176. [Google Scholar] [CrossRef]
- Ramamurthy, R.; Muthusamy, V.; Hussain, S.A. Approach to carcinoma cervix with pelvic kidney. Indian J. Surg. Oncol. 2010, 1, 323–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dretler, S.P.; Olsson, C.; Pfister, R.C. The anatomic, radiologic and clinical characteristics of the pelvic kidney: An analysis of 86 cases. J. Urol. 1971, 105, 623–627. [Google Scholar] [CrossRef]
- Rosenshein, N.B.; Lichter, A.S.; Walsh, P.C. Cervical cancer complicated by a pelvic kidney. J. Urol. 1980, 123, 766–767. [Google Scholar] [CrossRef]
- Roth, T.M.; Woodring, C.T.; McGehee, R.P. Stage II-B carcinoma of the cervix complicated by bilateral pelvic kidneys. Gynecol. Oncol. 2004, 92, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Lataifeh, I.; Amarin, Z.; Jaradat, I. Stage IIB carcinoma of the cervix that is associated with pelvic kidney: A therapeutic dilemma. Am. J. Obstet. Gynecol. 2007, 197, e8–e10. [Google Scholar] [CrossRef] [PubMed]
- Ripley, D.; Levenback, C.; Eifel, P.; Lewis, R.M. Adenocarcinoma of the cervix in a renal transplant patient. Gynecol. Oncol. 1995, 59, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Abouna, G.M.; Micaily, B.; Lee, D.J.; Kumar, M.S.; Jahshan, A.E.; Lyons, P. Salvage of a kidney graft in a patient with advanced carcinoma of the cervix by reimplantation of the graft from the pelvis to the upper abdomen in preparation for radiation therapy. Transplantation 1994, 58, 520–522. [Google Scholar] [CrossRef] [PubMed]
- Kunkler, P.B.; Farr, R.F.; Luxton, R.W. The limit of renal tolerance to x-rays; an investigation into renal damage occurring following the treatment of tumours of the testis by abdominal baths. Br. J. Radiol. 1952, 25, 192–201. [Google Scholar] [PubMed]
- Crummy, A.B., Jr.; Hellman, S.; Stansel, H.C., Jr.; Hukill, P.B. Renal hypertension secondary to unilateral radiation damage relieved by nephrectomy. Radiology 1965, 84, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, L.; Herlea, V.; Toma, L.; Orban, C. Association between chronic HCV hepatitis, membranoproliferative glomerulopathy and cutaneous sarcoidosis. J. Gastrointest. Liver Dis. 2015, 24, 8. [Google Scholar]
- Iliescu, L.; Mercan-Stanciu, A.; Toma, L.; Ioanitescu, E.S. A severe case of hyperglycemia in a kidney transplant recipient undergoing interferon-free therapy for chronic hepatitis C. Acta Endocrinol. Buchar 2018, 14, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, L.; Ioanitescu, S.; Toma, L.; Orban, C. Spontaneous portohepatic venous shunt: Ultrasonographic aspect. Ultrasound Q. 2015, 31, 141–144. [Google Scholar] [CrossRef]
- Koff, S.A.; Hayden, L.J.; Wise, H.A. Anomalies of the kidney. In Adult and Pediatric Urology; Doody, D.G., Gillenwater, J.Y., Eds.; Yearbook Medical Publishers: Chicago, IL, USA, 1987; Chapter 47; p. 1604. [Google Scholar]
- Bodean, O.; Bratu, O.; Munteanu, O.; Marcu, D.; Spinu, D.A.; Socea, B.; Diaconu, C.; Cirstoiu, M. Iatrogenic injury of the low urinary tract in women undergoing pelvic surgical interventions. Arch. Balk. Med. Union 2018, 53, 281–284. [Google Scholar] [CrossRef]
- Bumbu, A.; Nacer, K.; Bratu, O.; Berechet, M.; Bumbu, G.; Bumbu, B. Ureteral lesions in gynecological pathology. In Proceedings of the 14th National Congress of Urogynecology and the National Conference of the Romanian Asociation for the Study of Pain, Bucharest, Romania, 26–27 October 2017; pp. 82–89. [Google Scholar]
- Rusu, M.C.; Ilie, A.C.; Brezean, I. Human anatomic variations: Common, external iliac, origin of the obturator, inferior epigastric and medial circumflex femoral arteries and deep femoral artery course on the medial side of the femoral vessels. Surg. Radiol. Anat. 2017, 39, 1285–1288. [Google Scholar] [CrossRef]
- Brezean, I.; Aldoescu, S.; Catrina, E.; Valcu, M.; Ionut, I.; Predescu, G.; Degeratu, D.; Pantea, I. Pelvic and abdominal-wall actinomycotic infection by uterus gateway without genital lesions. Chirurgia 2010, 105, 123–125. [Google Scholar]
- Balescu, I.; Bacalbasa, N.; Vilcu, M.; Brasoveanu, V.; Brezean, I. Sentinel lymph node in early stage ovarian cancer; a literature review. J. Mind Med. Sci. 2018, 5, 184–188. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name, Year | Age of the Patient (Years) | Presumed FIGO Stage—Preoperatively | Histopathological Type | Therapeutic Strategy | Follow-up |
|---|---|---|---|---|---|
| Bakri, 1993 [1] | 65 | IIB | Squamous cell carcinoma | Per primam surgery—radical abdominal hysterectomy en bloc with left parametrectomy, left ureteral resection and reimplantation into the urinary bladder using a Boari flap technique Followed by adjuvant chemotherapy—Cisplatinum 100 mg/m2 3 weeks, 3 courses | Alive without recurrence at 6 years after surgery |
| Roth, 2003 [5] | 48 | IIB | Squamous cell carcinoma | Per primam surgery—anterior exenteration without vaginal reconstruction and distal ileal conduit | No evidence of disease at 14 months follow-up |
| Lataifeh,2007 [6] | 50 | IIB | Adenocarcinoma | Definitive radio-chemotherapy—4500 cGy and cisplatin with curative intent for 9 weeks | Disease free at two years follow-up, normal renal function |
| Ripley, 1995 [7] | NR | IB | Adenocarcinoma of the cervix in a previously kidney transplanted patient | Definitive external radiotherapy—4000 cGy and intracavitary radiotherapy with curative intent for 6.5 weeks | NR |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bacalbasa, N.; Balescu, I.; Vilcu, M.; Dima, S.; Diaconu, C.; Iliescu, L.; Filipescu, A.; Brezean, I. Total Exenteration En Bloc with a Nephrectomy for Locally Advanced Cervical Cancer Invading a Pelvic Kidney—A Case Report and Literature Review. Medicina 2020, 56, 33. https://doi.org/10.3390/medicina56010033
Bacalbasa N, Balescu I, Vilcu M, Dima S, Diaconu C, Iliescu L, Filipescu A, Brezean I. Total Exenteration En Bloc with a Nephrectomy for Locally Advanced Cervical Cancer Invading a Pelvic Kidney—A Case Report and Literature Review. Medicina. 2020; 56(1):33. https://doi.org/10.3390/medicina56010033
Chicago/Turabian StyleBacalbasa, Nicolae, Irina Balescu, Mihaela Vilcu, Simona Dima, Camelia Diaconu, Laura Iliescu, Alexandru Filipescu, and Iulian Brezean. 2020. "Total Exenteration En Bloc with a Nephrectomy for Locally Advanced Cervical Cancer Invading a Pelvic Kidney—A Case Report and Literature Review" Medicina 56, no. 1: 33. https://doi.org/10.3390/medicina56010033