Tri-Ponderal Mass Index: A Screening Tool for Risk of Central Fat Accumulation in Brazilian Preschool Children

 and
and
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar]
- Organización de lasNaciones Unidas para laAlimentación y la Agricultura. Panorama de Laseguridad Alimentaria y Nutricional: Sistemas Alimentariossostenibles para Ponerfin al Hambre y Lamalnutrición; Organización de lasNaciones Unidas para laAlimentación y la Agricultura y laOrganizaciónPanamericana de laSalud: Santiago, Chile, 2017. [Google Scholar]
- World Health Organization. Obesity and Overweight; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Sant’Anna, M.S.L.; Priore, S.E.; Franceschini, S.C. Metodos de avaliação da composição corporal em crianças. Rev. Paul. Pediatr. 2009, 27, 315–321. [Google Scholar] [CrossRef]
- Weber, D.R.; Leonard, M.B.; Zemel, B.S. Body composition analysis in the pediatric population. Pediatr. Endocrinol. Rev. 2012, 10, 130–139. [Google Scholar] [PubMed]
- Vanderwall1, C.; Clark, R.R.; Eickhoff, J.; Carrel, A.L. BMI is a poor predictor of adiposity in young overweight and obese children. BMC Pediatr. 2017, 17, 135. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, A.; Shai, I.; Afek, A.; Dubnov-Raz, G.; Ayalon, N.; Gordon, B.; Derazne, E.; Tzur, D.; Shamis, A.; Vinker, S.; et al. Adolescent BMI trajectory and risk of diabetes versus coronary disease. N. Engl. J. Med. 2011, 364, 1315–1325. [Google Scholar] [CrossRef] [PubMed]
- Ashwell, M.; Lejeune, S.; McPherson, K. Ratio of waist circumference to height may be better indicator of need for weight management. Br. Med. J. 1996, 312, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.M.; Su, H.; Thomas, D.M.; Heo, M.; Golnabi, A.H.; Pietrobelli, A.; Heymsfield, S.B. Tri-Ponderal Mass Index vs. Body Mass Index in Estimating Body Fat During Adolescence. JAMA Pediatr. 2017, 171, 629–636. [Google Scholar] [CrossRef]
- Ramirez-Velez, R.; Correa-Bautista, J.E.; Carrillo, H.A.; González-Jiménez, E.; Schmidt-RioValle, J.; Correa-Rodríguez, M.; García-Hermoso, A.; González-Ruíz, K. Tri-Ponderal Mass Index VS. Fat Mass/Height3 as a screening tool for metabolic syndrome prediction in Colombiam children and young people. Nutrients 2018, 10, 412. [Google Scholar] [CrossRef]
- Zangirolami-Raimundo, J.; Echeimberg, J.O.; Leone, C. Research methodology topics: Cross-sectional studies. J. Hum. Growth Dev. 2018, 28, 356–360. [Google Scholar] [CrossRef] [Green Version]
- Lohman, T.G.; Roche, A.F.; Matorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Publishers: Champaign, IL, USA, 1988. [Google Scholar]
- Zimmermann, M.B.; Gübeli, C.; Püntener, C.; Molinari, L. Detection of overweight and obesity in a national sample of 6-12-y-old Swiss children: Accuracy and validity of reference values for body mass index from the US Centers for Disease Control and Prevention and the International Obesity Task Force. Am. J. Clin. Nutr. 2004, 79, 838–843. [Google Scholar] [CrossRef]
- Mesa, M.S.; Marrodán, M.D.; Lomaglio, D.B.; López-Ejeda, N.; Moreno-Romero, S.; Bejarano, J.I.; Dipierri, J.E.; Pacheco, J.L. Anthropometric parameters in screening for excess of adiposity in Argentinian and Spanish adolescents: Evaluation using receiver operating characteristic (ROC) methodology. Ann. Hum. Biol. 2013, 40, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Ashwell, M.; Gunn, P.; Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes. Rev. 2012, 13, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Marrodán, M.D.; Álvarez, J.M.; de Espinosa, M.G.M.; Carmenate, M.M.; López-Ejeda, N.; Cabanas, M.D.; Pacheco, J.L.; Mesa, M.S.; Romero-Collazos, J.F.; Prado, C.; et al. Predicting percentage body fat through waist-to-height ratio (WtHR) in Spanish schoolchildren. Public Health Nutr. 2014, 17, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Sant’Anna, M.S.L.; Tinoco, A.L.A.; Rosado, L.E.F.P.L.; Sant’Ana, L.F.D.R.; Mello, A.D.C.; Brito, I.S.D.S.; Araújo, L.F.; Santos, T.F. Body fat assessment by bioelectrical impedance and its correlation with different anatomical sites used in the measurement of waist circumference in children. J. Pediatria 2009, 85, 61–66. [Google Scholar] [Green Version]
- Savva, S.C.; Tornaritis, M.; Savva, M.E.; Kourides, Y.; Panagi, A.; Silikiotou, N.; Georgiou, C.; Kafatos, A. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1453–1458. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Ford, E.S.; Mokdad, A.H.; Cook, S. Recent trends in waist circumference and waist-height ratio among US children and adolescents. Pediatrics 2006, 118, 1390–1398. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.D.; Yoshinaga, H.; Muto, T. Waist-to-height ratio, a simple and practical index for assessing central fat distribution and metabolic risk in Japanese men and women. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 610–616. [Google Scholar] [CrossRef] [Green Version]
- Lehingue, Y.; Remontet, L.; Munoz, F.; Mamelle, N. Birth ponderal index and body mass index reference curves in a large population. Am. J. Hum. Biol. 1998, 10, 327–340. [Google Scholar] [CrossRef]
- Khoury, M.J.; Berg, C.J.; Calle, E.E. The ponderal index in term newborn siblings. Am. J. Epidemiol. 1990, 132, 576–583. [Google Scholar] [CrossRef]
- Seeds, J.W. Impaired fetal growth: Ultrasonic evaluation and clinical management. Obstet. Gynecol. 1984, 64, 577–584. [Google Scholar]
- Ashley-Martin, J.; Ensenauer, R.; Maguire, B.; Kuhle, S. Predicting cardiometabolic markers in children using tri-ponderal mass index: A cross-sectional study. Arch. Dis. Child. 2019. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Romano, L.; Di Renzo, L.; Gualtieri, P.; Salimei, C.; Carrano, E.; Rampello, T.; de Miranda, R.C. Tri-ponderal mass índex rather than body mass índex: An indicator of high adiposity in Italian children and adolescents. Nutrition 2018, 60, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Carrascosa, A.; Yeste, D.; Moreno-Galdo, A.; Gussinyé, M.; Ferrández, Á.; Clemente, M.; Fernández-Cancio, M. Indice de masa corporal e índice de masatriponderal de 1453 ninos no obesos ni malnutridos de La generacion del milênio. Estudio longitudinal de Barcelona. Anales de Pediatría 2018, 89, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Sims, E.D.; Wang, K.W.; Fleming, A.; Johnston, D.L.; Zelcer, S.M.; Rassekh, S.R.; Burrow, S.; Thabane, L.; Samaan, M.C. Tri-ponderal mass índex in survivors of childhood brain tumors: A cross-sectional study. Sci. Rep. 2018, 8, 16336. [Google Scholar] [CrossRef] [PubMed]
- Souza, M.F.C.; Gurgel, R.Q.; Barreto, I.D.C.; Saravanan, S. Neck circumference as screening measure for identifying adolescents with overweight and obesity. J. Hum. Growth Dev. 2016, 26, 260–266. [Google Scholar] [CrossRef] [Green Version]



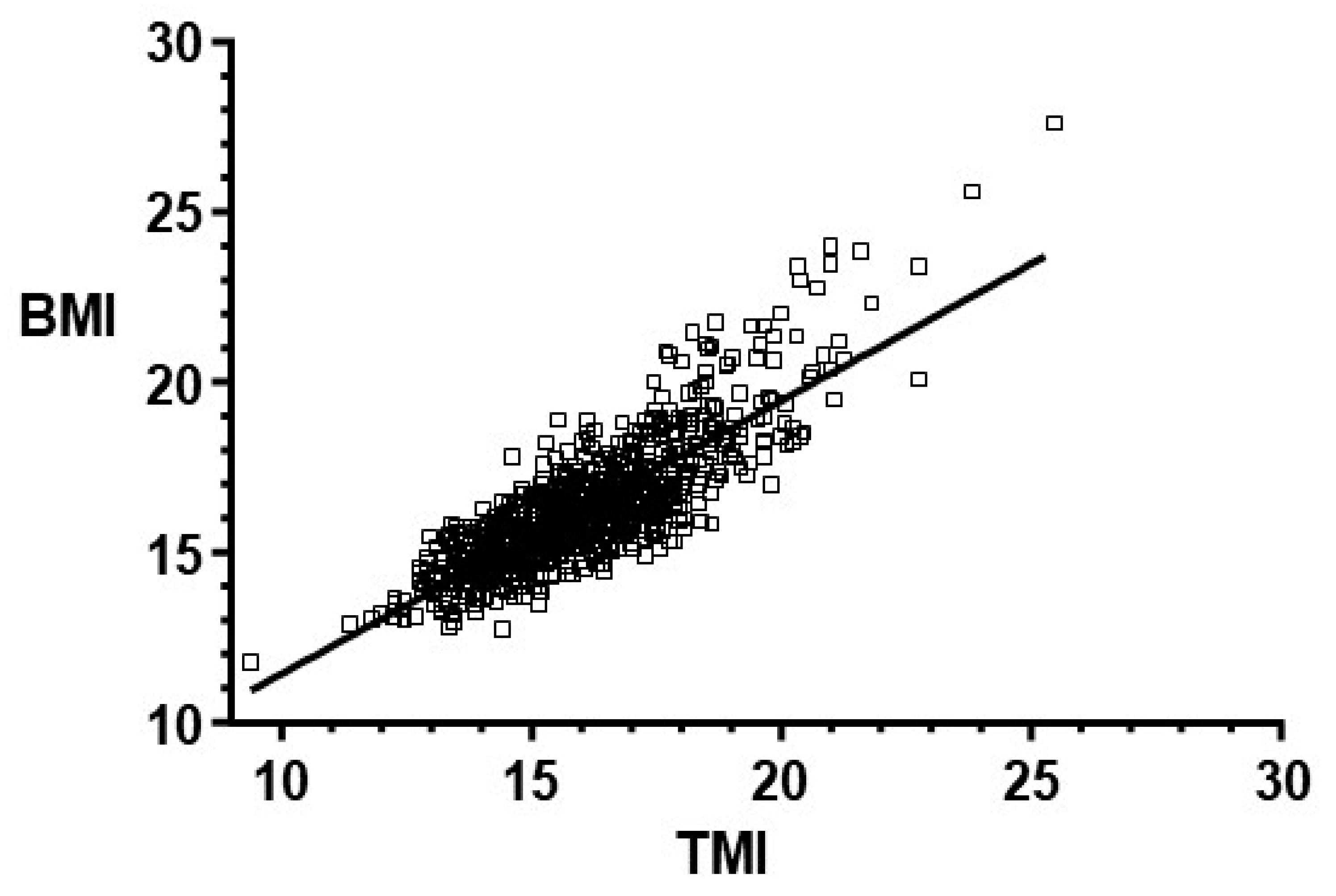{kind=link}
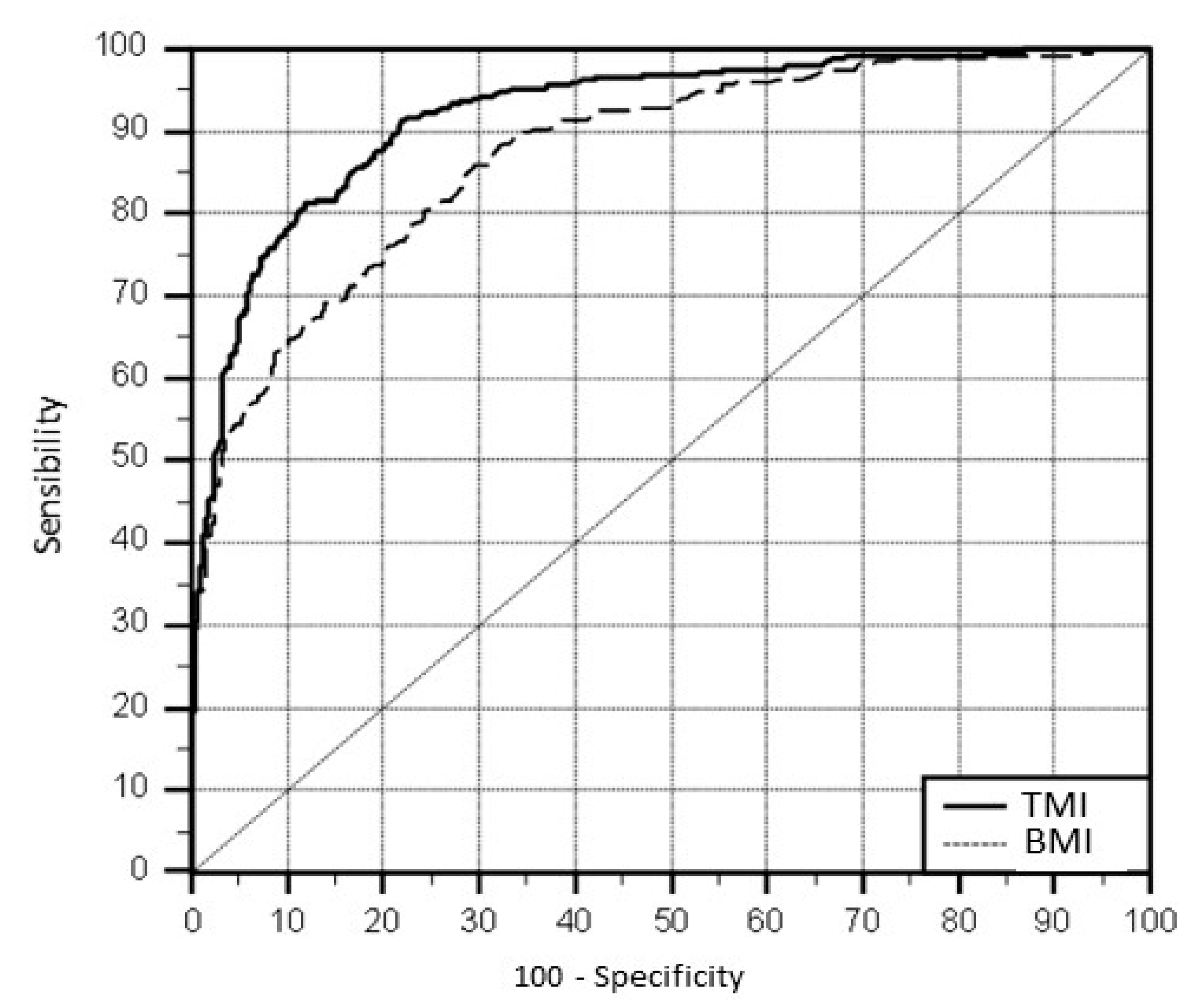{kind=link}
| Median | Mean | SD | |
|---|---|---|---|
| Weight (kg) | 16.4 | 16.9 | 3.2 |
| Height (cm) | 101.6 | 101.8 | 6.6 |
| BMI | 15.9 | 16.2 | 1.8 |
| WC (cm) | 51.5 | 52 | 5.1 |
| WHtR | 0.51 | 0.52 | 0.04 |
| TMI | 15.8 | 16 | 1.8 |
| Cutoff Point (kg/m3) | Sensibility (CI 95%) | Specificity (CI 95%) |
|---|---|---|
| 14 | 99.3 (97.6–99.9) | 18.5 (15.5–21.8) |
| 14.5 | 99.0 (97.1–99.8) | 32.7 (29.0–36.6) |
| 15 | 97.4 (94.8–98.8) | 46.2 (42.2–50.2) |
| 15.5 | 96.0 (93.2–97.9) | 60.0 (56.0–63.9) |
| 16 | 91.7 (88.0–94.6) | 76.2 (72.6–79.5) |
| 16.5 * | 81.5 (76.6–85.7) | 88.2 (84.8–90.2) |
| 17 | 68.2 (62.6–73.4) | 94.5 (92.4–96.5) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nascimento, V.G.; Bertoli, C.J.; Gallo, P.R.; Abreu, L.C.d.; Leone, C. Tri-Ponderal Mass Index: A Screening Tool for Risk of Central Fat Accumulation in Brazilian Preschool Children. Medicina 2019, 55, 577. https://doi.org/10.3390/medicina55090577
Nascimento VG, Bertoli CJ, Gallo PR, Abreu LCd, Leone C. Tri-Ponderal Mass Index: A Screening Tool for Risk of Central Fat Accumulation in Brazilian Preschool Children. Medicina. 2019; 55(9):577. https://doi.org/10.3390/medicina55090577
Chicago/Turabian StyleNascimento, Viviane Gabriela, Ciro João Bertoli, Paulo Rogerio Gallo, Luiz Carlos de Abreu, and Claudio Leone. 2019. "Tri-Ponderal Mass Index: A Screening Tool for Risk of Central Fat Accumulation in Brazilian Preschool Children" Medicina 55, no. 9: 577. https://doi.org/10.3390/medicina55090577