Prognostic Impact of Canonical TGF-? Signaling in Urothelial Bladder Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Histopathologic Analysis
2.2. Immunohistochemical Analysis
2.3. Statistical Analyses
3. Results
3.1. Expression of TGF-β1, Smad2, and Smad4 in Relation to Clinicopathologic Characteristics
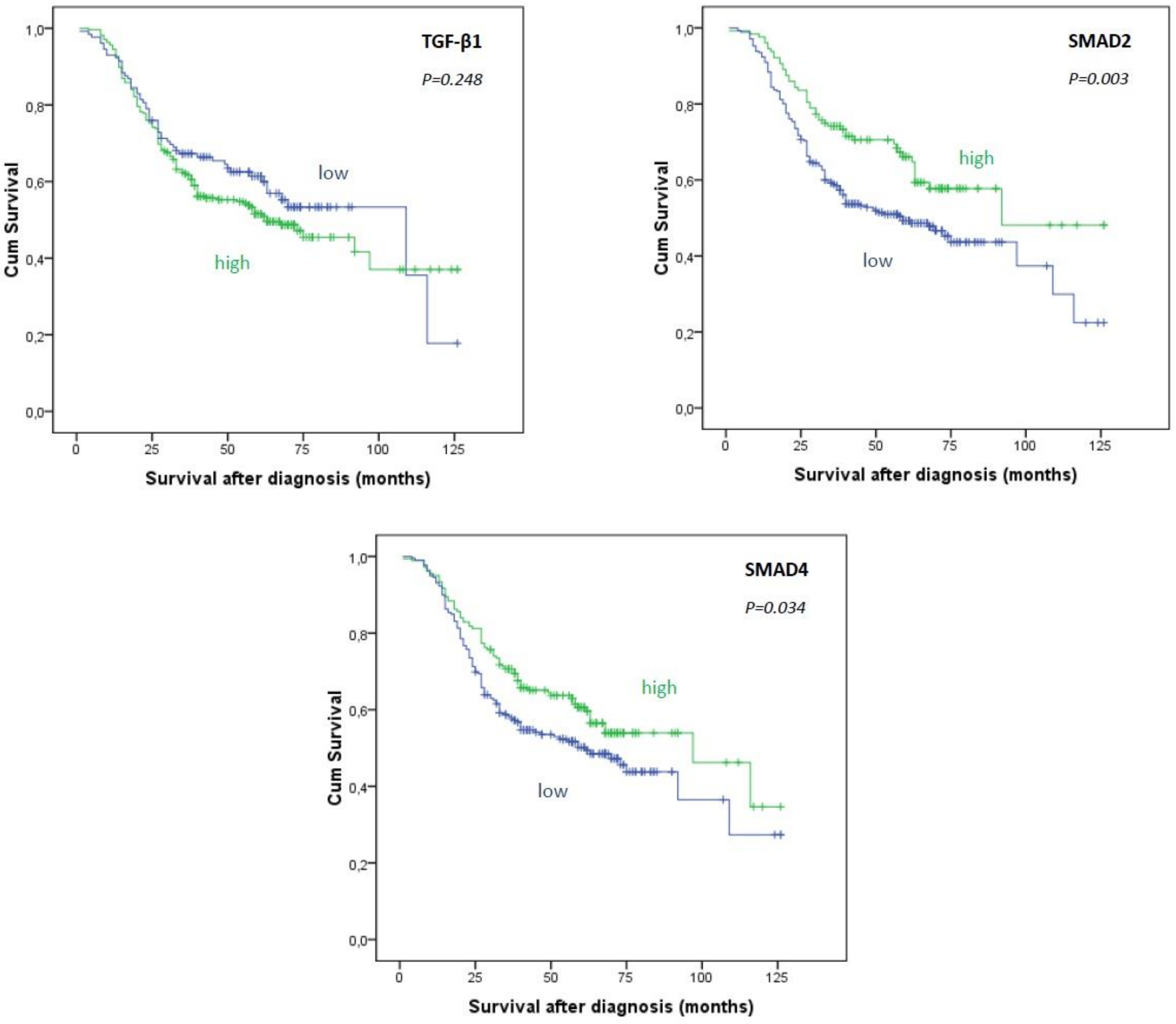
3.2. Association of TGF-β1and Smads Expression and Overall and Recurrence-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Fung, F.D.H.; Leung, C.; Cheung, W.W.L.; Goggins, W.B.; Ng, C.F. The global epidemiology of bladder cancer: A joinpoint regression analysis of its incidence and mortality trends and projection. Sci. Rep. 2018, 8, 1129. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 2014, 507, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Akbani, R.; Creighton, C.J.; Lerner, S.P.; Weinstein, J.N.; Getz, G.; Kwiatkowski, D.J. Invasive Bladder Cancer: Genomic Insights and Therapeutic Promise. Clin. Cancer Res. 2015, 21, 4514–4524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massagué, J. TGFβ in Cancer. Cell 2008, 134, 215–230. [Google Scholar] [CrossRef]
- Kitisin, K.; Saha, T.; Blake, T.; Golestaneh, N.; Deng, M.; Kim, C.; Tang, Y.; Shetty, K.; Mishra, B.; Mishra, L. Tgf-Beta signaling in development. Sci. STKE 2007, 2007, 1. [Google Scholar] [CrossRef] [PubMed]
- Brabletz, T.; Kalluri, R.; Nieto, M.A.; Weinberg, R.A. EMT in cancer. Nat. Rev. Cancer 2018, 18, 128–134. [Google Scholar] [CrossRef] [PubMed]
- McConkey, D.J.; Lee, S.; Choi, W.; Tran, M.; Majewski, T.; Lee, S.; Siefker-Radtke, A.; Dinney, C.; Czerniak, B. Molecular genetics of bladder cancer: Emerging mechanisms of tumor initiation and progression. Urol. Oncol. Semin. Orig. Investig. 2010, 28, 429–440. [Google Scholar] [CrossRef] [Green Version]
- Slaton, J.W.; Millikan, R.; Inoue, K.; Karashima, T.; Czerniak, B.; Shen, Y.; Yang, Y.; Benedict, W.F.; Dinney, C.P. Correlation of Metastasis Related Gene Expression and Relapse-Free Survival in Patients With Locally Advanced Bladder Cancer Treated with Cystectomy and Chemotherapy. J. Urol. 2004, 171, 570–574. [Google Scholar] [CrossRef]
- Liu, J.; Cao, J.; Zhao, X. miR-221 facilitates the TGFbeta1-induced epithelial-mesenchymal transition in human bladder cancer cells by targeting STMN1. BMC Urol. 2015, 15, 12. [Google Scholar] [CrossRef]
- Shi, Y.; Massagué, J. Mechanisms of TGF-beta signaling from cell membrane to the nucleus. Cell 2003, 113, 685–700. [Google Scholar] [CrossRef]
- Mansouri-Attia, N.; Tripurani, S.K.; Gokul, N.; Piard, H.; Anderson, M.L.; Eldin, K.; Pangas, S.A. TGFβ Signaling Promotes Juvenile Granulosa Cell Tumorigenesis by Suppressing Apoptosis. Mol. Endocrinol. 2014, 28, 1887–1898. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Kamat, A.M.; Aldousari, S.; Ye, Y.; Huang, M.; Dinney, C.P.; Wu, X. Genetic Variations in the Transforming Growth Factor Beta Pathway as Predictors of Bladder Cancer Risk. PLoS ONE 2012, 7, e51758. [Google Scholar] [CrossRef] [PubMed]
- Castillejo, A.; Rothman, N.; Murta-Nascimento, C.; Malats, N.; García-Closas, M.; Gómez-Martínez, A.; Lloreta, J.; Tardón, A.; Serra, C.; García-Closas, R.; et al. TGFB1andTGFBR1polymorphic variants in relationship to bladder cancer risk and prognosis. Int. J. Cancer 2009, 124, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Sjöblom, T.; Jones, S.; Wood, L.D.; Parsons, D.W.; Lin, J.; Barber, T.D.; Mandelker, D.; Leary, R.J.; Ptak, J.; Silliman, N.; et al. The Consensus Coding Sequences of Human Breast and Colorectal Cancers. Science 2006, 314, 268–274. [Google Scholar] [CrossRef]
- Schutte, M.; Hruban, R.H.; Hedrick, L.; Cho, K.R.; Nadasdy, G.M.; Weinstein, C.L.; Bova, G.S.; Isaacs, W.B.; Cairns, P.; Nawroz, H. DPC4 gene in various tumor types. Cancer Res. 1996, 56, 2527–2530. [Google Scholar] [PubMed]
- Wang, X.; Chen, E.; Tang, M.; Yang, X.; Wang, Y.; Quan, Z.; Wu, X.; Luo, C. The SMAD2/3 pathway is involved in hepaCAM-induced apoptosis by inhibiting the nuclear translocation of SMAD2/3 in bladder cancer cells. Tumor Boil. 2016, 37, 10731–10743. [Google Scholar] [CrossRef]
- Moch, H.; Humphrey, P.A.; Ulbright, T.M.; Reuter, V. WHO Classification of Tumours of the Urinary System and Male Genital Organs, 4th ed.; IARC: Lyon, France, 2016. [Google Scholar]
- Brierly, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Chichester, UK, 2017. [Google Scholar]
- Kim, J.H.; Shariat, S.F.; Kim, I.Y.; Menesses-Diaz, A.; Tokunaga, H.; Wheeler, T.M.; Lerner, S.P. Predictive value of expression of transforming growth factor-β1 and its receptors in transitional cell carcinoma of the urinary bladder. Cancer 2001, 92, 1475–1483. [Google Scholar] [CrossRef]
- Karam, J.A.; Lotan, Y.; Karakiewicz, P.I.; Ashfaq, R.; Sagalowsky, A.I.; Roehrborn, C.G.; Shariat, S.F. Use of combined apoptosis biomarkers for prediction of bladder cancer recurrence and mortality after radical cystectomy. Lancet Oncol. 2007, 8, 128–136. [Google Scholar] [CrossRef]
- Knowles, M.A.; Hurst, C.D. Molecular biology of bladder cancer: New insights into pathogenesis and clinical diversity. Nat. Rev. Cancer 2015, 15, 25–41. [Google Scholar] [CrossRef]
- Gupta, S.; Hau, A.M.; Al-Ahmadie, H.A.; Harwalkar, J.; Shoskes, A.C.; Elson, P.; Beach, J.R.; Hussey, G.S.; Schiemann, W.P.; Egelhoff, T.T.; et al. Transforming Growth Factor-β Is an Upstream Regulator of Mammalian Target of Rapamycin Complex 2–Dependent Bladder Cancer Cell Migration and Invasion. Am. J. Pathol. 2016, 186, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, H.; Kubota, Y.; Shuin, T.; Torigoe, S.; Dobashi, Y.; Hosaka, M. Expression of transforming growth factor-β1 in human bladder cancer. Cancer 1995, 75, 2565–2570. [Google Scholar] [CrossRef]
- Hahn, S.A.; Schutte, M.; Hoque, A.T.M.S.; Moskaluk, C.A.; Da Costa, L.T.; Rozenblum, E.; Weinstein, C.L.; Fischer, A.; Yeo, C.J.; Hruban, R.H.; et al. DPC4, A Candidate Tumor Suppressor Gene at Human Chromosome 18q21.1. Science 1996, 271, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Brosens, L.A.; Langeveld, D.; Van Hattem, W.A.; Giardiello, F.M.; Offerhaus, G.J.; Brosens, L.A. Juvenile polyposis syndrome. World J. Gastroenterol. 2011, 17, 4839–4844. [Google Scholar] [CrossRef] [PubMed]
- Kong, C.; Zhang, X.; Takenaka, I. Apoptotic cell death and Smad4 expression in transitional cell carcinoma of the renal pelvis and ureter. Int. J. Urol. 2001, 8, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witjes, J.A.; Lebret, T.; Compérat, E.M.; Cowan, N.C.; De Santis, M.; Bruins, H.M.; Hernández, V.; Espinós, E.L.; Dunn, J.; Rouanne, M.; et al. Updated 2016 EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer. Eur. Urol. 2017, 71, 462–475. [Google Scholar] [CrossRef] [PubMed]
- Neuzillet, C.; Tijeras-Raballand, A.; Cohen, R.; Cros, J.; Faivre, S.; Raymond, E.; De Gramont, A. Targeting the TGFβ pathway for cancer therapy. Pharmacol. Ther. 2015, 147, 22–31. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| TGF-β1 | Smad2 | Smad4 | |||||
|---|---|---|---|---|---|---|---|
| Characteristics | High | p value | High | p value | High | p value | |
| Total (n (%)) | 404 (100) | 275 (68.1) | 128 (31.7) | 181 (45.2) | |||
| Gender | |||||||
| Female | 92 (22.8) | 70 (25.5) | 0.038 | 27 (21.1) | 0.340 | 45 (24.9) | 0.246 |
| Male | 312 (77.2) | 205 (74.5) | 101 (78.9) | 136 (75.1) | |||
| Tumor grade | |||||||
| Low | 148 (36.6) | 81 (29.5) | <0.001 | 60 (46.9) | 0.003 | 75 (41.4) | 0.048 |
| High | 256 (63.4) | 194 (70.5) | 68 (53.1) | 106 (58.6) | |||
| Pathologic stage | |||||||
| pTa | 97 (24.0) | 44 (16.0) | <0.001 | 43 (33.6) | <0.001 | 51 (28.2) | 0.003 |
| pT1 | 195 (48.3) | 144 (52.4) | 71 (55.5) | 95 (52.5) | |||
| pT2 | 112 (27.7) | 87 (31.6) | 14 (10.9) | 35 (19.3) | |||
| Carcinoma in situ | |||||||
| Yes | 33 (8.2) | 25 (9.1) | 0.216 | 11 (8.6) | 0.485 | 11 (6.1) | 0.104 |
| No | 371 (91.8) | 250 (90.9) | 117 (91.4) | 170 (93.9) | |||
| Variant differentiation | |||||||
| Negative | 338 (83.7) | 228 (82.9) | 0.328 | 115 (89.8) | 0.014 | 155 (85.6) | 0.214 |
| Positive | 66 (16.3) | 47 (17.1) | 13 (10.2) | 26 (14. 4) | |||
| Recurrence | |||||||
| Yes | 150 (37.1) | 103 (37.5) | 0.467 | 49 (38.3) | 0.413 | 74 (40.9) | 0.103 |
| No | 254 (62.9) | 172 (62.5) | 79 (61.7) | 107 (59.1) | |||
| Cancer-specific death | |||||||
| Yes | 138 (34.2) | 102 (37.1) | 0.043 | 31 (24.2) | 0.003 | 52 (28.7) | 0.022 |
| Other cause | 53 (13.1) | 34 (12.4) | 17 (13.3) | 24 (13.3) | |||
| Alive | 213 (52.7) | 139 (50.5) | 80 (62.5) | 105 (58.0) | |||
| Treatment | |||||||
| TURBT ± mitomycin * | 67 (16.6) | 41 (14.9) | 24 (18.8) | 31 (17.1) | 0.069 | ||
| Intravesical BCG | 186 (46.0) | 119 (43.3) | 71 (55.4) | 0.007 b | 89 (49.2) | ||
| Cystectomy | 72 (17.8) | 53 (19.3) | 13 (10.2) | 0.004 c | 26 (14.4) | ||
| Chemo/radiotherapy | 79 (19.6) | 62 (22.5) | 0.017 a | 20 (15.6) | 35 (19.3) |
| Overall Survival | ||||||
|---|---|---|---|---|---|---|
| Parameter | B | SE | HR | 95%CI | p Value | |
| Lower | Upper | |||||
| Tumor grade (high) | 1.245 | 0.268 | 3.472 | 2.054 | 5.868 | <0.001 |
| Pathologic stage | ||||||
| pT1 | 0.844 | 0.325 | 2.326 | 1.230 | 4.401 | 0.009 |
| pT2 | 1.733 | 0.357 | 5.656 | 2.812 | 11.376 | <0.001 |
| Variant morphology (yes) | 0.106 | 0.192 | 1.112 | 0.764 | 1.620 | 0.580 |
| Carcinoma in situ (yes) | −0.163 | 0.242 | 0.850 | 0.529 | 1.365 | 0.501 |
| TGF-β1 (high) | 0.448 | 0.219 | 1.565 | 1.019 | 2.405 | 0.041 |
| Smad2 (high) | 0.052 | 0.204 | 1.053 | 0.705 | 1.572 | 0.800 |
| Smad4 (high) | −0.140 | 0.174 | 0.869 | 0.619 | 1.222 | 0.420 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojnev, S.; Krstić, M.; Čukuranović Kokoris, J.; Conić, I.; Petković, I.; Ilić, S.; Milosević-Stevanović, J.; Janković Veličković, L. Prognostic Impact of Canonical TGF-? Signaling in Urothelial Bladder Cancer. Medicina 2019, 55, 302. https://doi.org/10.3390/medicina55060302
Stojnev S, Krstić M, Čukuranović Kokoris J, Conić I, Petković I, Ilić S, Milosević-Stevanović J, Janković Veličković L. Prognostic Impact of Canonical TGF-? Signaling in Urothelial Bladder Cancer. Medicina. 2019; 55(6):302. https://doi.org/10.3390/medicina55060302
Chicago/Turabian StyleStojnev, Slavica, Miljan Krstić, Jovana Čukuranović Kokoris, Irena Conić, Ivan Petković, Sonja Ilić, Jelena Milosević-Stevanović, and Ljubinka Janković Veličković. 2019. "Prognostic Impact of Canonical TGF-? Signaling in Urothelial Bladder Cancer" Medicina 55, no. 6: 302. https://doi.org/10.3390/medicina55060302
APA StyleStojnev, S., Krstić, M., Čukuranović Kokoris, J., Conić, I., Petković, I., Ilić, S., Milosević-Stevanović, J., & Janković Veličković, L. (2019). Prognostic Impact of Canonical TGF-? Signaling in Urothelial Bladder Cancer. Medicina, 55(6), 302. https://doi.org/10.3390/medicina55060302