
Synergistic Nanomedicine: Photodynamic, Photothermal and Photoimmune Therapy in Hepatocellular Carcinoma: Fulfilling the Myth of Prometheus?



Abstract
:1. Introduction
2. Photodynamic, Photothermal and Photoimmune Therapy in HCC—The Basics
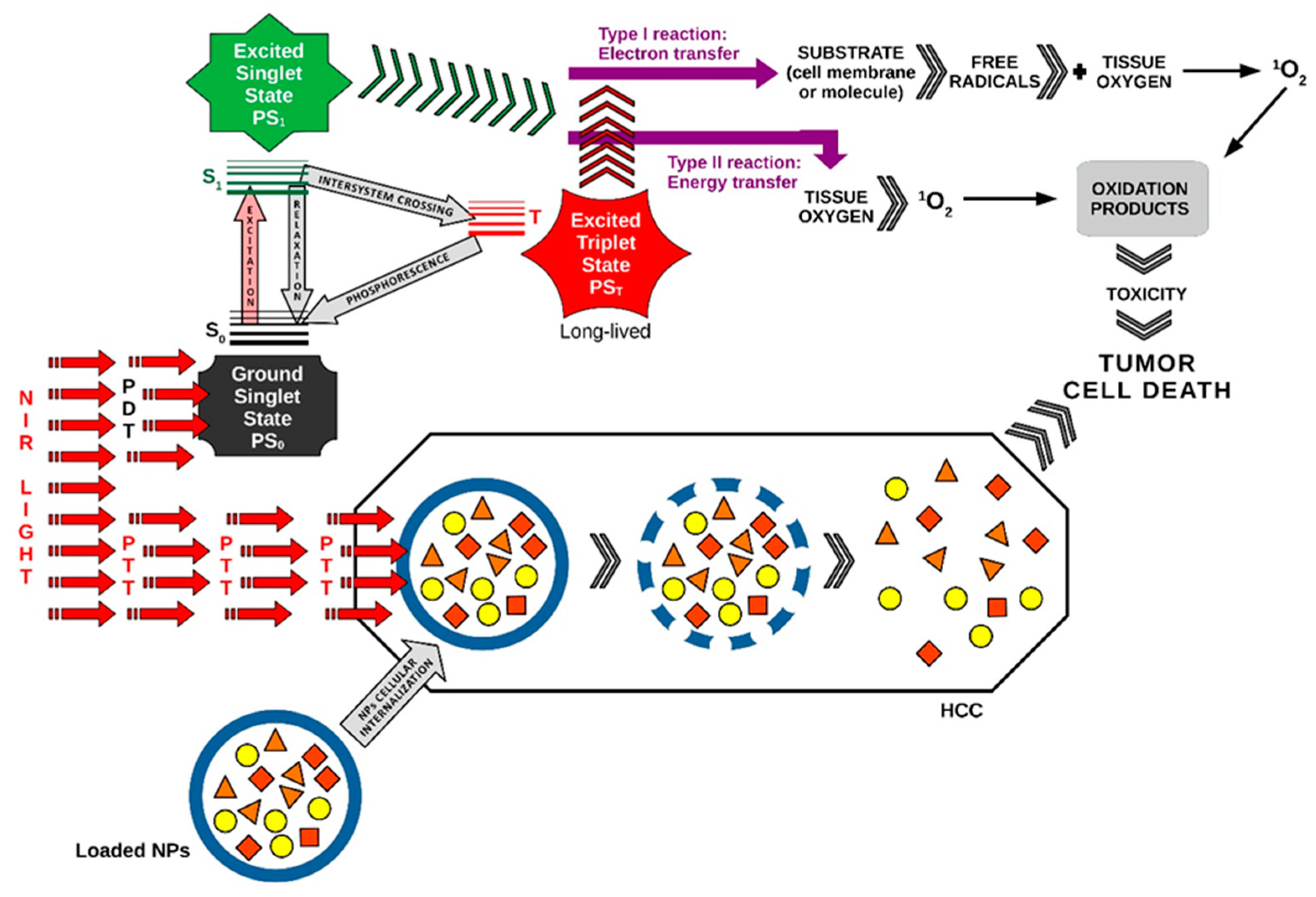
2.1. How Does PDT Work?
2.2. How Does PTT Work?
2.3. How Does PIT Work?
3. Investigational Studies Using Multifunctional Platforms for PTT in HCC
4. Experimental Applications of PDT and PTT in HCC
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Aggregation-induced emission-based luminogens | AIEgens |
| Alpha (Greek letter, lowercase alpha) | α |
| Alpha-fetoprotein | AFP |
| Antibody-photon absorber conjugate | APC |
| Asialoglycoprotein receptor | ASGPR |
| ATP-binding cassette | ABC |
| Barcelona Clinic Liver Cancer | BCLC |
| Bismuth, chemical element with atomic number 83 | Bi |
| CAR-T cell membrane-coated nanoparticles | CIMs |
| Cerium dioxide | CeO2 |
| Chemo-photodynamic therapy | chemo-PDT |
| Chimeric antigen receptor | CAR |
| Chimeric antigen receptors or chimeric T cell receptors | CAR-T |
| Chimeric antigen receptor (CAR) natural killer cell | CAR-NK |
| Chimeric antigen receptor T cell/NK cell | CAR-T/CAR-NK |
| Chlorin e6 | Ce6 |
| X-ray computed tomography | CT |
| Continuous wave | CW |
| Copper phthalocyanine 1 | PcC1 |
| Copper phthalocyanine 2 | PcC2 |
| Covalent organic polymers | COPs |
| Curcumin | Cur |
| Cyclic adenosine monophosphate | cAMP |
| Cytochrome c oxidase | CCO |
| Cytotoxic T lymphocyte-associated antigen-4 | CTLA-4 |
| C-X-C chemokine receptor type 4 | CXCR4 |
| Decrease | ↓ |
| Des-γ-carboxy-prothrombin | DCP |
| Diffuse correlation spectroscopy | DCS |
| Drug delivery | DD |
| Drug delivery systems | DDSs |
| Dulbecco’s Modified Eagle’s medium (EuroClone) | DMEM |
| Eastern Cooperative Oncology Group | ECOG |
| Electrochemiluminescence | ECL |
| Epidermal growth factor receptor | EGFR |
| Extracellular matrix | ECM |
| Fetal bovine serum | FBS |
| Fluorescence imaging | FLI |
| Fluorescence molecular imaging | FMI |
| Functional near-infrared spectroscopy | fNIRS |
| Gadolinium-diethylenetriamine pentaacetic acid | Gd-DTPA |
| Galactosylated amphiphilic graft copolymer | PHEA-g-BIB-pButMA-g-PEG-GAL |
| Glycoprotein P | P-gp |
| Glypican-3 | GPC3 |
| Gold nanoparticles | AuNPs |
| Gold nanorods | AuNRs |
| Golgi protein 73 | GP73 |
| Heat shock proteins | HSPs |
| Hepatitis B virus | HBV |
| Hepatitis C virus | HCV |
| Hepatocellular carcinoma | HCC |
| Human dermal fibroblasts | NHDF |
| Human hepatocarcinoma cells | HepG2 |
| Hydrogen peroxide | H2O2 |
| Hydroxyl radical | •OH |
| Hypoxia-inducible factor 1 | HIF-1 |
| ICG/Pt@PDA-CXCR4 | IPP-c |
| Immune checkpoint blockade | ICB |
| Immunogenic cell death | ICD |
| Increase | ↑ |
| Indocyanine green | ICG |
| Insulin-like growth factors-1 | IGF-1 |
| Interferon-γ | IFN-γ |
| Interleukin 1-beta | IL-1β |
| Interleukin-10 | IL-10 |
| Interleukin-6 | IL-6 |
| International Agency for Research on Cancer | IARC |
| Interstitial fluid pressure | IFP |
| Interventional PTT | IPTT |
| Intra-arterial | IA |
| Intravenous | IV |
| Iron (III)-coordinated squaraine dye | SQ890 |
| IR780-loaded MSNs | IMs |
| Layered MoS2 hollow spheres | LMHSs |
| Lenvatinib | LEN |
| Light amplification by stimulated emission of radiation | LASER |
| Light-emitting diode | LED |
| Lipid droplets | LDs |
| Liposomes | LPs |
| Liver Imaging Reporting and Data System | LI-RADS |
| Localized surface plasmon resonance | LSPR |
| Magnetic particle imaging | MPI |
| Magnetic resonance | MR |
| Magnetic resonance elastogram/elastography | MRE |
| Magnetic resonance imaging | MRI |
| Maximum permissible exposure | MPE |
| Manganese dioxide | MnO2 |
| Mesoporous silica nanoparticles | MSNs |
| Methylene blue | MB |
| 3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide) assay | MTT |
| Mitochondria/mitochondrial | mt |
| Mitochondrial membrane potential | MMP |
| MnO2-SOR | MS |
| MnO2-SOR-Ce6 | MSC |
| MnO2-Ce6@PDA | MCP |
| MnO2-Ce6@PDA-PEG-FA | MCPF |
| MnO2-SOR-Ce6@PDA | MSCP |
| MnO2-SOR-Ce6@PDA- PEG-FA | MSCPF |
| Molybdenum disulfide | MoS2 |
| Monoclonal antibody | mAb |
| MR spectroscopy | MRS |
| Multidrug resistance | MDR |
| Multidrug resistance mutation 1 | MDR1 |
| Nanoemulsion | NE |
| Nanoparticle | NP |
| Nanoparticles | NPs |
| Natural killer | NK |
| Near-infrared | NIR |
| Near-infrared photoimmunotherapy | NIR-PIT |
| Negative control | NC |
| Oxaliplatin | Oxa |
| Paclitaxel | PTX |
| P-glycoprotein | P-gp |
| Phosphate-buffered saline | PBS |
| Photoacoustic imaging | PAI |
| Photodynamic inactivation | PDI |
| Photodynamic therapy | PDT |
| Photoimmunoconjugate | PIC |
| Photoimmunotherapy | PIT |
| Photosensitizer | PS |
| Photosensitizers | PSs |
| Photothermal | PT |
| Photothermal agents | PTAs |
| Photothermal conversion | PTC |
| Photothermal conversion efficiency | PCE |
| Photothermal therapy | PTT |
| Phthalocyanine | Pc |
| Phthalocyanine amino-substituted A1 | PcA1 |
| Phthalocyanine amino-substituted A2 | PcA2 |
| Piperazine | PcB1 |
| Poly(ethyleneglycol)-folate | PEG-FA |
| Polydopamine | PDA |
| Positron emission tomography | PET |
| Programmed cell death 1 | PD-1 |
| Programmed cell death ligand 1 | PD-L1 |
| Protein-induced absence of vitamin K or antagonist-II | PIVKA-II |
| Radiopharmaceutical-excited fluorescence | REF |
| Reactive oxygen species | ROS |
| Recurrent head and neck squamous cell carcinoma | rHNSCC |
| Red | R |
| Second near-infrared light-activated photothermal therapy | NIR-II PTT |
| Silver nanoparticles | AgNPs |
| Singlet oxygen, dioxygen (singlet) or dioxidene | 1O2 |
| Small orthotopic hepatocellular carcinoma | SHCC |
| Sorafenib | SOR |
| Spatial harmonic imaging | SHI |
| Superoxide | •O−2 |
| Terminal transferase-mediated dUTP nick end-labeling | TUNEL |
| Theta (Greek letter, lowercase theta) | θ |
| Transarterial chemoembolization | TACE |
| Tumor inhibition rate | TIR |
| Tumor microenvironment | TME |
| Tumor necrosis factor alpha | TNF-α |
| 1-[2-hydroxyethyl]-4-[4-(1,2,2-triphenylvinyl)styryl]pyridinium bromide | TPE-Py-OH |
| U.S. Food and Drug Administration | FDA |
| Ultrasound scan (ultrasonography) | US |
| Ultraviolet | UV |
| Ultraviolet-visible | UV-Vis |
| Ultraviolet A | UVA |
| Ultraviolet B | UVB |
| Vascular endothelial growth factor | VEGF |
| World Health Organization | WHO |
References
- Centers for Disease Control and Prevention. An Update on Cancer Deaths in the United States. Available online: https://www.cdc.gov/cancer/dcpc/research/update-on-cancer-deaths/index.htm (accessed on 14 February 2023).
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer, World Health Organization. Liver Cancer. Global, Regional, and National Burden of Primary Liver Cancer by Subtype. Available online: https://www.iarc.who.int/news-events/global-regional-and-national-burden-of-primary-liver-cancer-by-subtype/ (accessed on 14 February 2023).
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef]
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, A.K.; Soerjomataram, I. Global burden of primary liver cancer in 2020 and predictions to 2040. J. Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.; Hallouch, O.; Chernyak, V.; Kamaya, A.; Sirlin, C.B. Epidemiology of hepatocellular carcinoma: Target population for surveillance and diagnosis. Abdom. Radiol. 2018, 43, 13–25. [Google Scholar] [CrossRef]
- Baecker, A.; Liu, X.; La Vecchia, C.; Zhang, Z.F. Worldwide incidence of hepatocellular carcinoma cases attributable to major risk factors. Eur. J. Cancer Prev. 2018, 27, 205–212. [Google Scholar] [CrossRef]
- Konyn, P.; Ahmed, A.; Kim, D. Current epidemiology in hepatocellular carcinoma. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 1295–1307. [Google Scholar] [CrossRef]
- Huang, D.Q.; Singal, A.G.; Kono, Y.; Tan, D.J.H.; El-Serag, H.B.; Loomba, R. Changing global epidemiology of liver cancer from 2010 to 2019: NASH is the fastest growing cause of liver cancer. Cell Metab. 2022, 34, 969–977.e2. [Google Scholar] [CrossRef]
- World Health Organization International Agency for Research on Cancer. Liver. Available online: http://gco.iarc.fr/today/data/factsheets/cancers/11-Liver-fact-sheet.pdf (accessed on 12 February 2023).
- Shen, C.; Jiang, X.; Li, M.; Luo, Y. Hepatitis Virus and Hepatocellular Carcinoma: Recent Advances. Cancers 2023, 15, 533. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef]
- Ailioaie, L.M.; Litscher, G. Curcumin and Photobiomodulation in Chronic Viral Hepatitis and Hepatocellular Carcinoma. Int. J. Mol. Sci. 2020, 21, 7150. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.T.; Wang, J.J.; Zhu, Y.; Agopian, V.G.; Tseng, H.R.; Yang, J.D. Diagnostic Criteria and LI-RADS for Hepatocellular Carcinoma. Clin. Liver Dis. 2021, 17, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.; Bashir, M.R.; Corwin, M.T.; Cruite, I.; Dietrich, C.F.; Do, R.K.G.; Ehman, E.C.; Fowler, K.J.; Hussain, H.K.; Jha, R.C.; et al. LI-RADS Evidence Working Group. Evidence Supporting LI-RADS Major Features for CT- and MR Imaging-based Diagnosis of Hepatocellular Carcinoma: A Systematic Review. Radiology 2018, 286, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Karademir, S. Staging of hepatocellular carcinoma. Hepatoma. Res. 2018, 4, 58. [Google Scholar] [CrossRef]
- Moura Cunha, G.; Chernyak, V.; Fowler, K.J.; Sirlin, C.B. Up-to-Date Role of CT/MRI LI-RADS in Hepatocellular Carcinoma. J. Hepatocell. Carcinoma 2021, 8, 513–527. [Google Scholar] [CrossRef]
- Cunha, G.M.; Sirlin, C.B.; Fowler, K.J. Imaging diagnosis of hepatocellular carcinoma: LI-RADS. Chin. Clin. Oncol. 2021, 10, 3. [Google Scholar] [CrossRef]
- De Muzio, F.; Grassi, F.; Dell’Aversana, F.; Fusco, R.; Danti, G.; Flammia, F.; Chiti, G.; Valeri, T.; Agostini, A.; Palumbo, P.; et al. A Narrative Review on LI-RADS Algorithm in Liver Tumors: Prospects and Pitfalls. Diagnostics 2022, 12, 1655. [Google Scholar] [CrossRef]
- Roberts, L.R.; Sirlin, C.B.; Zaiem, F.; Almasri, J.; Prokop, L.J.; Heimbach, J.K.; Murad, M.H.; Mohammed, K. Imaging for the diagnosis of hepatocellular carcinoma: A systematic review and meta-analysis. Hepatology 2018, 67, 401–421. [Google Scholar] [CrossRef]
- Kwee, S.A.; Tiirikainen, M.; Sato, M.M.; Acoba, J.D.; Wei, R.; Jia, W.; Le Marchand, L.; Wong, L.L. Transcriptomics Associates Molecular Features with 18F-Fluorocholine PET/CT Imaging Phenotype and Its Potential Relationship to Survival in Hepatocellular Carcinoma. Cancer Res. 2019, 79, 1696–1704. [Google Scholar] [CrossRef]
- Howard, B.A.; Wong, T.Z. 18F-FDG-PET/CT Imaging for Gastrointestinal Malignancies. Radiol. Clin. N. Am. 2021, 59, 737–753. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Lee, J.S.H.; Zhang, M. Magnetic nanoparticles in MR imaging and drug delivery. Adv. Drug Deliv. Rev. 2008, 60, 1252–1265. [Google Scholar] [CrossRef] [PubMed]
- Chee, H.L.; Gan, C.R.R.; Ng, M.; Low, L.; Fernig, D.G.; Bhakoo, K.K.; Paramelle, D. Biocompatible Peptide-Coated Ultrasmall Superparamagnetic Iron Oxide Nanoparticles for In Vivo Contrast-Enhanced Magnetic Resonance Imaging. ACS Nano 2018, 12, 6480–6491. [Google Scholar] [CrossRef]
- Mittal, A.; Roy, I.; Gandhi, S. Magnetic Nanoparticles: An Overview for Biomedical Applications. Magnetochemistry 2022, 8, 107. [Google Scholar] [CrossRef]
- Xu, Y.H.; Yang, J.; Meng, J.; Wang, H. Targeted MR Imaging Adopting T1-Weighted Ultra-Small Iron Oxide Nanoparticles for Early Hepatocellular Carcinoma: An in vitro and in vivo Study. Chin. Med. Sci. J. 2020, 35, 142–150. [Google Scholar] [CrossRef]
- Liao, R.; Tang, Z.; Li, X.; Lv, L.; Yang, C.; Xiong, H.; Zhou, B.; Yu, J.; Zhang, D. Proton Magnetic Resonance Spectroscopy at 3.0T in Rabbit With VX2 Liver Cancer: Diagnostic Efficacy and Correlations With Tumor Size. Front. Oncol. 2022, 12, 846308. [Google Scholar] [CrossRef]
- Sobhani, T.; Shahbazi-Gahrouei, D.; Zahraei, M.; Hejazi, S.H.; Dousti, F.; Rostami, M. Novel MR imaging nanoprobe for hepatocellular carcinoma detection based on manganese-zinc ferrite nanoparticles: In vitro and in vivo assessments. J. Cancer Res. Clin. Oncol. 2022; ahead of print. [Google Scholar] [CrossRef]
- Jia, W.; Han, Y.; Mao, X.; Xu, W.; Zhang, Y. Nanotechnology strategies for hepatocellular carcinoma diagnosis and treatment. RSC Adv. 2022, 12, 31068–31082. [Google Scholar] [CrossRef]
- Hu, Z.; Chi, C.; Liu, M.; Guo, H.; Zhang, Z.; Zeng, C.; Ye, J.; Wang, J.; Tian, J.; Yang, W.; et al. Nanoparticle-mediated radiopharmaceutical-excited fluorescence molecular imaging allows precise image-guided tumor-removal surgery. Nanomedicine 2017, 13, 1323–1331. [Google Scholar] [CrossRef]
- Shi, X.; Cao, C.; Zhang, Z.; Tian, J.; Hu, Z. Radiopharmaceutical and Eu3+ doped gadolinium oxide nanoparticles mediated triple-excited fluorescence imaging and image-guided surgery. J. Nanobiotechnol. 2021, 19, 212. [Google Scholar] [CrossRef]
- Sun, J.; Li, X.; Chen, A.; Cai, W.; Peng, X.; Li, L.; Fan, B.; Wang, L.; Zhang, H.; Zhang, R. A Dual-Modality MR/PA Imaging Contrast Agent Based on Ultrasmall Biopolymer Nanoparticles for Orthotopic Hepatocellular Carcinoma Imaging. Int. J. Nanomed. 2019, 16, 9893–9904. [Google Scholar] [CrossRef]
- Zhao, D.; Cao, J.; Zhang, L.; Zhang, S.; Wu, S. Targeted Molecular Imaging Probes Based on Magnetic Resonance Imaging for Hepatocellular Carcinoma Diagnosis and Treatment. Biosensors 2022, 12, 342. [Google Scholar] [CrossRef] [PubMed]
- Rashidiani, J.; Kamali, M.; Sedighian, H.; Akbariqomi, M.; Mansouri, M.; Kooshki, H. Ultrahigh sensitive enhanced-electrochemiluminescence detection of cancer biomarkers using silica NPs/graphene oxide: A comparative study. Biosens. Bioelectron. 2018, 102, 226–233. [Google Scholar] [CrossRef]
- Yang, S.; Zhang, F.; Wang, Z.; Liang, Q. A graphene oxide-based label-free electrochemical aptasensor for the detection of alpha-fetoprotein. Biosens. Bioelectron. 2018, 112, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Wang, L.; Zhang, H.; Liu, S.; Jiang, J. An Electrochemical Sandwich Immunosensor Based on Signal Amplification Technique for the Determination of Alpha-Fetoprotein. Front. Chem. 2020, 8, 589560. [Google Scholar] [CrossRef] [PubMed]
- Wei, T.; Zhang, W.; Tan, Q.; Cui, X.; Dai, Z. Electrochemical Assay of the Alpha Fetoprotein-L3 Isoform Ratio To Improve the Diagnostic Accuracy of Hepatocellular Carcinoma. Anal. Chem. 2018, 90, 13051–13058. [Google Scholar] [CrossRef]
- Singh, G.; Yoshida, E.M.; Rathi, S.; Marquez, V.; Kim, P.; Erb, S.R.; Salh, B.S. Biomarkers for hepatocellular cancer. World J. Hepatol. 2020, 12, 558–573. [Google Scholar] [CrossRef]
- Zhou, J.M.; Wang, T.; Zhang, K.H. AFP-L3 for the diagnosis of early hepatocellular carcinoma: A meta-analysis. Medicine 2021, 100, e27673. [Google Scholar] [CrossRef]
- Zhu, R.; Yang, J.; Xu, L.; Dai, W.; Wang, F.; Shen, M.; Zhang, Y.; Zhang, H.; Chen, K.; Cheng, P.; et al. Diagnostic Performance of Des-γ-carboxy Prothrombin for Hepatocellular Carcinoma: A Meta-Analysis. Gastroenterol. Res. Pract. 2014, 2014, 529314. [Google Scholar] [CrossRef]
- Chen, J.; Wu, G.; Li, Y. Evaluation of Serum Des-Gamma-Carboxy Prothrombin for the Diagnosis of Hepatitis B Virus-Related Hepatocellular Carcinoma: A Meta-Analysis. Dis. Markers 2018, 2018, 8906023. [Google Scholar] [CrossRef]
- Zhao, S.; Long, M.; Zhang, X.; Lei, S.; Dou, W.; Hu, J.; Du, X.; Liu, L. The diagnostic value of the combination of Golgi protein 73, glypican-3 and alpha-fetoprotein in hepatocellular carcinoma: A diagnostic meta-analysis. Ann. Transl. Med. 2020, 8, 536. [Google Scholar] [CrossRef]
- Moctezuma-Velázquez, C.; Lewis, S.; Lee, K.; Amodeo, S.; Llovet, J.M.; Schwartz, M.; Abraldes, J.G.; Villanueva, A. Non-invasive imaging criteria for the diagnosis of hepatocellular carcinoma in non-cirrhotic patients with chronic hepatitis B. JHEP Rep. 2021, 3, 100364. [Google Scholar] [CrossRef] [PubMed]
- Chartampilas, E.; Rafailidis, V.; Georgopoulou, V.; Kalarakis, G.; Hatzidakis, A.; Prassopoulos, P. Current Imaging Diagnosis of Hepatocellular Carcinoma. Cancers 2022, 14, 3997. [Google Scholar] [CrossRef]
- Joo, I.; Lee, J.M.; Koh, Y.H.; Choi, S.H.; Lee, S.; Chung, J.W. 2022 Korean Liver Cancer Association-National Cancer Center Korea Practice Guidelines for Imaging Diagnosis of Hepatocellular Carcinoma: What’s New? Korean J. Radiol. 2023, 24, 1–5. [Google Scholar] [CrossRef]
- Llovet, J.M.; Villanueva, A.; Marrero, J.A.; Schwartz, M.; Meyer, T.; Galle, P.R.; Lencioni, R.; Greten, T.F.; Kudo, M.; Mandrekar, S.J.; et al. AASLD Panel of Experts on Trial Design in HCC. Trial Design and Endpoints in Hepatocellular Carcinoma: AASLD Consensus Conference. Hepatology 2021, 73, 158–191. [Google Scholar] [CrossRef] [PubMed]
- El Dika, I.; Makki, I.; Abou-Alfa, G.K. Hepatocellular carcinoma, novel therapies on the horizon. Chin. Clin. Oncol. 2021, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Machairas, N.; Tsilimigras, D.I.; Pawlik, T.M. Current Landscape of Immune Checkpoint Inhibitor Therapy for Hepatocellular Carcinoma. Cancers 2022, 14, 2018. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Aziz, H.; Pawlik, T.M. Critical Analysis of the Updated Barcelona Clinic Liver Cancer (BCLC) Group Guidelines. Ann. Surg. Oncol. 2022, 29, 7231–7234. [Google Scholar] [CrossRef]
- Ayoub, W.S.; Jones, P.D.; Yang, J.D.; Martin, P. Emerging drugs for the treatment of hepatocellular carcinoma. Expert Opin. Emerg. Drugs 2022, 27, 141–149. [Google Scholar] [CrossRef]
- Llovet, J.M.; Castet, F.; Heikenwalder, M.; Maini, M.K.; Mazzaferro, V.; Pinato, D.J.; Pikarsky, E.; Zhu, A.X.; Finn, R.S. Immunotherapies for hepatocellular carcinoma. Nat. Rev. Clin. Oncol. 2022, 19, 151–172. [Google Scholar] [CrossRef]
- Rizzo, A.; Ricci, A.D.; Fanizzi, A.; Massafra, R.; De Luca, R.; Brandi, G. Immune-Based Combinations versus Sorafenib as First-Line Treatment for Advanced Hepatocellular Carcinoma: A Meta-Analysis. Curr. Oncol. 2023, 30, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Zhong, B.Y.; Jin, Z.C.; Chen, J.J.; Zhu, H.D.; Zhu, X.L. Role of Transarterial Chemoembolization in the Treatment of Hepatocellular Carcinoma. J. Clin. Transl. Hepatol. 2023, 11, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.Y.; Zhang, K.J.; Xie, Y.M.; Liu, J.W.; Xiao, Z.Q. Immunotherapies for advanced hepatocellular carcinoma. Front. Pharmacol. 2023, 14, 1138493. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Ricci, A.D. Challenges and Future Trends of Hepatocellular Carcinoma Immunotherapy. Int. J. Mol. Sci. 2022, 23, 11363. [Google Scholar] [CrossRef]
- Yang, S.; Cai, C.; Wang, H.; Ma, X.; Shao, A.; Sheng, J.; Yu, C. Drug delivery strategy in hepatocellular carcinoma therapy. Cell Commun. Signal 2022, 20, 26. [Google Scholar] [CrossRef]
- Feng, Y.; Wu, W.; Li, M. Metal-organic frameworks for hepatocellular carcinoma therapy and mechanism. Front. Pharmacol. 2022, 13, 1025780. [Google Scholar] [CrossRef]
- Valery, P.C.; Laversanne, M.; Clark, P.J.; Petrick, J.L.; McGlynn, K.A.; Bray, F. Projections of primary liver cancer to 2030 in 30 countries worldwide. Hepatology 2018, 67, 600–611. [Google Scholar] [CrossRef]
- Qi, Y.; Wang, H.; Zhang, Q.; Liu, Z.; Wang, T.; Wu, Z.; Wu, W. CAF-Released Exosomal miR-20a-5p Facilitates HCC Progression via the LIMA1-Mediated β-Catenin Pathway. Cells 2022, 11, 3857. [Google Scholar] [CrossRef]
- Spikes, J.D. The Historical Development of Ideas on Applications of Photosensitized Reactions in the Health Sciences. In Primary Photo-Processes in Biology and Medicine; Bensasson, R.V., Jori, G., Land, E.J., Truscott, T.G., Eds.; Springer: Boston, MA, USA, 1985; pp. 209–227. [Google Scholar] [CrossRef]
- Dolmans, D.E.; Fukumura, D.; Jain, R.K. Photodynamic therapy for cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef]
- Ailioaie, L.M.; Ailioaie, C.; Litscher, G. Latest Innovations and Nanotechnologies with Curcumin as a Nature-Inspired Photosensitizer Applied in the Photodynamic Therapy of Cancer. Pharmaceutics 2021, 13, 1562. [Google Scholar] [CrossRef]
- Baptista, M.S.; Cadet, J.; Di Mascio, P.; Ghogare, A.A.; Greer, A.; Hamblin, M.R.; Lorente, C.; Nunez, S.C.; Ribeiro, M.S.; Thomas, A.H.; et al. Type I and Type II Photosensitized Oxidation Reactions: Guidelines and Mechanistic Pathways. Photochem. Photobiol. 2017, 93, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Rezende, T.K.L.; Barbosa, H.P.; Dos Santos, L.F.; de O Lima, K.; Alves de Matos, P.; Tsubone, T.M.; Gonçalves, R.R.; Ferrari, J.L. Up conversion rare Earths nanomaterials applied to photodynamic therapy and bioimaging. Front. Chem. 2022, 10, 1035449. [Google Scholar] [CrossRef] [PubMed]
- Mansoori, B.; Mohammadi, A.; Amin Doustvandi, M.; Mohammadnejad, F.; Kamari, F.; Gjerstorff, M.F.; Baradaran, B.; Hamblin, M.R. Photodynamic therapy for cancer: Role of natural products. Photodiagn. Photodyn. Ther. 2019, 26, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.O.; Ha, K.S. New insights into the mechanisms for photodynamic therapy-induced cancer cell death. Int. Rev. Cell Mol. Biol. 2012, 295, 139–174. [Google Scholar] [CrossRef] [PubMed]
- Mishchenko, T.; Balalaeva, I.; Gorokhova, A.; Vedunova, M.; Krysko, D.V. Which cell death modality wins the contest for photodynamic therapy of cancer? Cell Death Dis. 2022, 13, 455. [Google Scholar] [CrossRef]
- Chen, Z.; Liu, L.; Liang, R.; Luo, Z.; He, H.; Wu, Z.; Tian, H.; Zheng, M.; Ma, Y.; Cai, L. Bioinspired Hybrid Protein Oxygen Nanocarrier Amplified Photodynamic Therapy for Eliciting Anti-tumor Immunity and Abscopal Effect. ACS Nano 2018, 12, 8633–8645. [Google Scholar] [CrossRef]
- Ding, J.; Jin, Y.; Zhu, F.; Zhu, C.; Peng, J.; Su, T.; Cai, J. Facile Synthesis of NaYF4:Yb Up-Conversion Nanoparticles Modified with Photosensitizer and Targeting Antibody for In Vitro Photodynamic Therapy of Hepatocellular Carcinoma. J. Healthc. Eng. 2022, 2022, 4470510. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, D.; Cao, Y.; Wang, Y.; Wang, F.; Zhang, F.; Zheng, S. Biodegradable Hypocrellin B nanoparticles coated with neutrophil membranes for hepatocellular carcinoma photodynamics therapy effectively via JUNB/ROS signaling. Int. Immunopharmacol. 2021, 99, 107624. [Google Scholar] [CrossRef]
- National Institutes of Health. U.S. National Library of Medicine. Available online: https://clinicaltrials.gov/ct2/results?cond=Hepatocellular+Carcinoma+&term=PDT&cntry=&state=&city=&dist= (accessed on 30 March 2023).
- Huang, X.; Zhao, L.; Peng, R. Hypoxia-Inducible Factor 1 and Mitochondria: An Intimate Connection. Biomolecules 2023, 13, 50. [Google Scholar] [CrossRef]
- Chen, J.; Ning, C.; Zhou, Z.; Yu, P.; Zhu, Y.; Tan, G.; Mao, C. Nanomaterials as photothermal therapeutic agents. Prog. Mater. Sci. 2019, 99, 1–26. [Google Scholar] [CrossRef]
- Zhao, L.; Zhang, X.; Wang, X.; Guan, X.; Zhang, X.; Ma, J. Recent advances in selective photothermal therapy of tumor. J. Nanobiotechnol. 2021, 19, 335. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.Y.; Miao, Z.H.; Li, K.; Yang, H.; Zhen, L.; Xu, C.Y. Biocompatible Fe3+-TA coordination complex with high photothermal conversion efficiency for ablation of cancer cells. Colloids Surf. B Biointerfaces 2018, 167, 183–190. [Google Scholar] [CrossRef]
- Chen, S.X.; Ma, M.; Xue, F.; Shen, S.; Chen, Q.; Kuang, Y.; Liang, K.; Wang, X.; Chen, H. Construction of microneedle-assisted co-delivery platform and its combining photodynamic/immunotherapy. J. Control. Release 2020, 324, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Guan, B.; Sun, Z.; Tian, X.; Li, X. Fabrication of an injectable hydrogel with inherent photothermal effects from tannic acid for synergistic photothermal-chemotherapy. J. Mater. Chem. B 2021, 9, 6084–6091. [Google Scholar] [CrossRef] [PubMed]
- Vankayala, R.; Lin, C.C.; Kalluru, P.; Chiang, C.S.; Hwang, K.C. Gold nanoshells-mediated bimodal photodynamic and photothermal cancer treatment using ultra-low doses of near infra-red light. Biomaterials 2014, 35, 5527–5538. [Google Scholar] [CrossRef]
- Kang, S.; Bhang, S.H.; Hwang, S.; Yoon, J.K.; Song, J.; Jang, H.K.; Kim, S.; Kim, B.S. Mesenchymal Stem Cells Aggregate and Deliver Gold Nanoparticles to Tumors for Photothermal Therapy. ACS Nano 2015, 9, 9678–9690. [Google Scholar] [CrossRef]
- Zhao, T.; Qin, S.; Peng, L.; Li, P.; Feng, T.; Wan, J.; Yuan, P.; Zhang, L. Novel hyaluronic acid-modified temperature-sensitive nanoparticles for synergistic chemo-photothermal therapy. Carbohydr. Polym. 2019, 214, 221–233. [Google Scholar] [CrossRef]
- Varon, E.; Blumrosen, G.; Sinvani, M.; Haimov, E.; Polani, S.; Natan, M.; Shoval, I.; Jacob, A.; Atkins, A.; Zitoun, D.; et al. An Engineered Nanocomplex with Photodynamic and Photothermal Synergistic Properties for Cancer Treatment. Int. J. Mol. Sci. 2022, 23, 2286. [Google Scholar] [CrossRef]
- Wang, D.; Su, H.; Kwok, R.T.K.; Hu, X.; Zou, H.; Luo, Q.; Lee, M.M.S.; Xu, W.; Lam, J.W.Y.; Tang, B.Z. Rational design of a water-soluble NIR AIEgen, and its application in ultrafast wash-free cellular imaging and photodynamic cancer cell ablation. Chem. Sci. 2018, 9, 3685–3693. [Google Scholar] [CrossRef]
- Wang, J.; Li, J.; Wang, L.; Han, T.; Wang, D.; Tang, B.Z. AIEgen-based polymer nanocomposites for imaging-guided photothermal therapy. ACS Appl. Polym. Mater. 2020, 2, 4306–4318. [Google Scholar] [CrossRef]
- Jia, R.; Xu, H.; Wang, C.; Su, L.; Jing, J.; Xu, S.; Zhou, Y.; Sun, W.; Song, J.; Chen, X.; et al. NIR-II emissive AIEgen photosensitizers enable ultrasensitive imaging-guided surgery and phototherapy to fully inhibit orthotopic hepatic tumors. J. Nanobiotechnol. 2021, 19, 419. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Zhao, Q. Nanomedicine-Combined Immunotherapy for Cancer. Curr. Med. Chem. 2020, 27, 5716–5729. [Google Scholar] [CrossRef] [PubMed]
- Umut, Ö.; Gottschlich, A.; Endres, S.; Kobold, S. CAR T cell therapy in solid tumors: A short review. Memo 2021, 14, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Jiang, H. Current Challenges and Strategies for Chimeric Antigen Receptor-T-Cell Therapy for Solid Tumors. Crit. Rev. Immunol. 2021, 41, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Xu, H.; Weng, L.; Sun, J.; Jin, Y.; Xiao, C. Activation of cancer immunotherapy by nanomedicine. Front. Pharmacol. 2022, 13, 1041073. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Lv, X.; Huang, S. Photoimmunotherapy: A New Paradigm in Solid Tumor Immunotherapy. Cancer Control 2022, 29, 10732748221088825. [Google Scholar] [CrossRef]
- Jain, R.K.; Martin, J.D.; Stylianopoulos, T. The role of mechanical forces in tumor growth and therapy. Annu. Rev. Biomed. Eng. 2014, 16, 321–346. [Google Scholar] [CrossRef]
- Wagner, J.; Rapsomaniki, M.A.; Chevrier, S.; Anzeneder, T.; Langwieder, C.; Dykgers, A.; Rees, M.; Ramaswamy, A.; Muenst, S.; Soysal, S.D.; et al. A Single-Cell Atlas of the Tumor and Immune Ecosystem of Human Breast Cancer. Cell 2019, 177, 1330–1345.e18. [Google Scholar] [CrossRef]
- Tamura, R.; Tanaka, T.; Akasaki, Y.; Murayama, Y.; Yoshida, K.; Sasaki, H. The role of vascular endothelial growth factor in the hypoxic and immunosuppressive tumor microenvironment: Perspectives for therapeutic implications. Med. Oncol. 2019, 37, 2. [Google Scholar] [CrossRef]
- Abdel-Wahab, A.F.; Mahmoud, W.; Al-Harizy, R.M. Targeting glucose metabolism to suppress cancer progression: Prospective of anti-glycolytic cancer therapy. Pharmacol. Res. 2019, 150, 104511. [Google Scholar] [CrossRef]
- Sun, B.; Hyun, H.; Li, L.T.; Wang, A.Z. Harnessing nanomedicine to overcome the immunosuppressive tumor microenvironment. Acta Pharmacol. Sin. 2020, 41, 970–985. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Choyke, P.L. Near-Infrared Photoimmunotherapy of Cancer. Acc. Chem. Res. 2019, 52, 2332–2339. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Furusawa, A.; Rosenberg, A.; Choyke, P.L. Near-infrared photoimmunotherapy of cancer: A new approach that kills cancer cells and enhances anti-cancer host immunity. Int. Immunol. 2021, 33, 7–15. [Google Scholar] [CrossRef]
- Photoimmune Discoveries. Photo-Immunothérapies. Available online: http://photoimmune.org/photo-immunotherapies/?lang=fr (accessed on 28 March 2023).
- Yamaguchi, H.; On, J.; Morita, T.; Suzuki, T.; Okada, Y.; Ono, J.; Evdokiou, A. Combination of Near-Infrared Photoimmunotherapy Using Trastuzumab and Small Protein Mimetic for HER2-Positive Breast Cancer. Int. J. Mol. Sci. 2021, 22, 12213. [Google Scholar] [CrossRef] [PubMed]
- Kong, C.; Chen, X. Combined Photodynamic and Photothermal Therapy and Immunotherapy for Cancer Treatment: A Review. Int. J. Nanomed. 2022, 17, 6427–6446. [Google Scholar] [CrossRef]
- Kumar, A.; Moralès, O.; Mordon, S.; Delhem, N.; Boleslawski, E. Could Photodynamic Therapy Be a Promising Therapeutic Modality in Hepatocellular Carcinoma Patients? A Critical Review of Experimental and Clinical Studies. Cancers 2021, 13, 5176. [Google Scholar] [CrossRef]
- Cui, Y.; Xu, Y.; Li, Y.; Sun, Y.; Hu, J.; Jia, J.; Li, X. Antibody Drug Conjugates of Near-Infrared Photoimmunotherapy (NIR-PIT) in Breast Cancers. Technol. Cancer Res. Treat. 2023, 22, 15330338221145992. [Google Scholar] [CrossRef]
- Yamashita, S.; Kojima, M.; Onda, N.; Yoshida, T.; Shibutani, M. Trastuzumab-based near-infrared photoimmunotherapy in xenograft mouse of breast cancer. Cancer Med. 2023, 12, 4579–4589. [Google Scholar] [CrossRef]
- Ormond, A.B.; Freeman, H.S. Dye Sensitizers for Photodynamic Therapy. Materials 2013, 6, 817–840. [Google Scholar] [CrossRef]
- Abrahamse, H.; Hamblin, M.R. New Photosensitizers for photodynamic therapy. Biochem. J. 2016, 473, 347–364. [Google Scholar] [CrossRef]
- Kubrak, T.P.; Kołodziej, P.; Sawicki, J.; Mazur, A.; Koziorowska, K.; Aebisher, D. Some Natural Photosensitizers and Their Medicinal Properties for Use in Photodynamic Therapy. Molecules 2022, 27, 1192. [Google Scholar] [CrossRef] [PubMed]
- Cognetti, D.M.; Johnson, J.M.; Curry, J.M.; Kochuparambil, S.T.; McDonald, D.; Mott, F.; Fidler, M.J.; Stenson, K.; Vasan, N.R.; Razaq, M.A.; et al. Phase 1/2a, open-label, multicenter study of RM-1929 photoimmunotherapy in patients with locoregional, recurrent head and neck squamous cell carcinoma. Head Neck 2021, 43, 3875–3887. [Google Scholar] [CrossRef] [PubMed]
- Paraboschi, I.; Turnock, S.; Kramer-Marek, G.; Musleh, L.; Barisa, M.; Anderson, J.; Giuliani, S. Near-InfraRed PhotoImmunoTherapy (NIR-PIT) for the local control of solid cancers: Challenges and potentials for human applications. Crit. Rev. Oncol. Hematol. 2021, 161, 103325. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Zheng, Q.; Cheng, X.; Hu, S.; Zhang, C.; Zhou, X.; Sun, P.; Wang, W.; Su, Z.; Zou, T.; et al. Chemo-photodynamic therapy with light-triggered disassembly of theranostic nanoplatform in combination with checkpoint blockade for immunotherapy of hepatocellular carcinoma. J. Nanobiotechnol. 2021, 19, 355. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Liu, X.; Liu, X.; Yu, J.; Bai, X.; Wu, X.; Guo, X.; Liu, Z.; Liu, X. Combination of phototherapy with immune checkpoint blockade: Theory and practice in cancer. Front. Immunol. 2022, 13, 955920. [Google Scholar] [CrossRef]
- Mohiuddin, T.M.; Zhang, C.; Sheng, W.; Al-Rawe, M.; Zeppernick, F.; Meinhold-Heerlein, I.; Hussain, A.F. Near Infrared Photoimmunotherapy: A Review of Recent Progress and Their Target Molecules for Cancer Therapy. Int. J. Mol. Sci. 2023, 24, 2655. [Google Scholar] [CrossRef]
- Zhou, J.; Ling, G.; Cao, J.; Ding, X.; Liao, X.; Wu, M.; Zhou, X.; Xu, H.; Long, Q. Transcatheter Intra-Arterial Infusion Combined with Interventional Photothermal Therapy for the Treatment of Hepatocellular Carcinoma. Int. J. Nanomed. 2020, 15, 1373–1385. [Google Scholar] [CrossRef]
- Giammona, G.; Drago, S.E.; Calabrese, G.; Varvarà, P.; Rizzo, M.G.; Mauro, N.; Nicotra, G.; Conoci, S.; Pitarresi, G. Galactosylated Polymer/Gold Nanorods Nanocomposites for Sustained and Pulsed Chemo-Photothermal Treatments of Hepatocarcinoma. Pharmaceutics 2022, 14, 2503. [Google Scholar] [CrossRef]
- Tang, L.; Ling, M.; Syeda, M.Z.; Sun, R.; He, M.; Mu, Q.; Zhu, X.; Huang, C.; Cui, L. A smart nanoplatform for enhanced photo-ferrotherapy of hepatocellular carcinoma. Front. Bioeng. Biotechnol. 2022, 10, 1022330. [Google Scholar] [CrossRef]
- Ding, X.; Liow, C.H.; Zhang, M.; Huang, R.; Li, C.; Shen, H.; Liu, M.; Zou, Y.; Gao, N.; Zhang, Z.; et al. Surface plasmon resonance enhanced light absorption and photothermal therapy in the second near-infrared window. J. Am. Chem. Soc. 2014, 136, 15684–15693. [Google Scholar] [CrossRef]
- Zhen, X.; Pu, K.; Jiang, X. Photoacoustic imaging and photothermal therapy of semiconducting polymer nanoparticles: Signal amplification and second near-infrared construction. Small 2021, 17, 2004723. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Huang, C.; Li, Y.; Huang, F.; Yin, S. NIR-II phototherapy agents with aggregation-induced emission characteristics for tumor imaging and therapy. Biomaterials 2022, 285, 121535. [Google Scholar] [CrossRef] [PubMed]
- Tian, C.; Xue, X.; Chen, Y.; Liu, R.; Wang, Y.; Ye, S.; Fu, Z.; Luo, Y.; Wang, S.; He, X.; et al. Phosphotungstate Acid Doped Polyanilines Nanorods for in situ NIR-II Photothermal Therapy of Orthotopic Hepatocellular Carcinoma in Rabbit. Int. J. Nanomed. 2022, 17, 5565–5579. [Google Scholar] [CrossRef]
- Huang, R.; Liu, W.; Zhang, Q.; Zhu, G.; Qu, W.; Tao, C.; Gao, J.; Fang, Y.; Fu, X.; Zhou, J.; et al. Laser-Induced Combinatorial Chemotherapeutic, Chemodynamic, and Photothermal Therapy for Hepatocellular Carcinoma Based on Oxaliplatin-Loaded Metal−Organic Frameworks. ACS Appl. Mater. Interfaces 2023, 15, 3781–3790. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Abd El Aziz, M.A.; Tartaglia, N.; Ramai, D.; Mohan, B.P.; Cotsoglou, C.; Pusceddu, S.; Giacomelli, L.; Ambrosi, A.; Sacco, R. Microwave Ablation Versus Radiofrequency Ablation for Treatment of Hepatocellular Carcinoma: A Meta-Analysis of Randomized Controlled Trials. Cancers 2020, 12, 3796. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Abd El Aziz, M.A.; Singh, S.; Pusceddu, S.; Milione, M.; Giacomelli, L.; Sacco, R. Statin Use Decreases the Incidence of Hepatocellular Carcinoma: An Updated Meta-Analysis. Cancers 2020, 12, 874. [Google Scholar] [CrossRef]
- Zhou, J.; Li, M.; Hou, Y.; Luo, Z.; Chen, Q.; Cao, H.; Huo, R.; Xue, C.; Sutrisno, L.; Hao, L.; et al. Engineering of a Nanosized Biocatalyst for Combined Tumor Starvation and Low-Temperature Photothermal Therapy. ACS Nano 2018, 12, 2858–2872. [Google Scholar] [CrossRef]
- Li, X.; Peng, X.H.; Zheng, B.D.; Tang, J.; Zhao, Y.; Zheng, B.Y.; Ke, M.R.; Huang, J.D. New application of phthalocyanine molecules: From photodynamic therapy to photothermal therapy by means of structural regulation rather than formation of aggregates. Chem. Sci. 2018, 9, 2098–2104. [Google Scholar] [CrossRef]
- Ma, W.; Zhu, D.; Li, J.; Chen, X.; Xie, W.; Jiang, X.; Wu, L.; Wang, G.; Xiao, Y.; Liu, Z.; et al. Coating biomimetic nanoparticles with chimeric antigen receptor T cell-membrane provides high specificity for hepatocellular carcinoma photothermal therapy treatment. Theranostics 2020, 10, 1281–1295. [Google Scholar] [CrossRef]
- Pokharel, D.; Roseblade, A.; Oenarto, V.; Lu, J.F.; Bebawy, M. Proteins regulating the intercellular transfer and function of P-glycoprotein in multidrug-resistant cancer. Ecancermedicalscience 2017, 11, 768. [Google Scholar] [CrossRef]
- Ahmed Juvale, I.I.; Abdul Hamid, A.A.; Abd Halim, K.B.; Che Has, A.T. P-glycoprotein: New insights into structure, physiological function, regulation and alterations in disease. Heliyon 2022, 8, e09777. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Bai, Y.; Chen, L.; Fakhri, G.E.; Wang, M. Self-Assembly Nanoparticles for Overcoming Multidrug Resistance and Imaging-Guided Chemo-Photothermal Synergistic Cancer Therapy. Int. J. Nanomed. 2020, 15, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Yang, S.; Liu, C.; He, J.; Li, T.; Fu, C.; Meng, X.; Shao, H. Enhanced Photothermal-Photodynamic Therapy by Indocyanine Green and Curcumin-Loaded Layered MoS2 Hollow Spheres via Inhibition of P-Glycoprotein. Int. J. Nanomed. 2021, 16, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhao, E.; Lam, J.W.Y.; Tang, B.Z. AIE luminogens: Emission brightened by aggregation. Mater. Today 2015, 18, 365–377. [Google Scholar] [CrossRef]
- Lee, M.M.S.; Yu, E.Y.; Chau, J.H.C.; Lam, J.W.Y.; Kwok, R.T.K.; Wang, D.; Tang, B.Z. Inspiration from nature: BioAIEgens for biomedical and sensing applications. Biomaterials 2022, 288, 121712. [Google Scholar] [CrossRef]
- Chai, C.; Zhou, T.; Zhu, J.; Tang, Y.; Xiong, J.; Min, X.; Qin, Q.; Li, M.; Zhao, N.; Wan, C. Multiple Light-Activated Photodynamic Therapy of Tetraphenylethylene Derivative with AIE Characteristics for Hepatocellular Carcinoma via Dual-Organelles Targeting. Pharmaceutics 2022, 14, 459. [Google Scholar] [CrossRef]
- Li, B.; Fu, Y.; Xie, M.; Feng, L.; Niu, X.; Que, L.; You, Z. Gold-based nanoparticles realize photothermal and photodynamic synergistic treatment of liver cancer and improve the anaerobic tumor microenvironment under near-infrared light. Front. Bioeng. Biotechnol. 2022, 10, 957349. [Google Scholar] [CrossRef]
- Durot, I.; Sigrist, R.; Kothary, N.; Rosenberg, J.; Willmann, J.K.; El, K.A. Quantitative ultrasound spectroscopy for differentiation of hepatocellular carcinoma from at-risk and normal liver parenchyma. Clin. Cancer Res. 2019, 25, 6683–6691. [Google Scholar] [CrossRef]
- Zhou, Y.; Chen, J.; Liu, C.; Liu, C.; Lai, P.; Wang, L. Single-shot linear dichroism optical-resolution photoacoustic microscopy. Photoacoustics 2019, 16, 100148. [Google Scholar] [CrossRef]
- Liu, Y.; Bhattarai, P.; Dai, Z.; Chen, X. Photothermal therapy and photoacoustic imaging via nanotheranostics in fighting cancer. Chem. Soc. Rev. 2019, 48, 2053–2108. [Google Scholar] [CrossRef]
- Ferrante, N.D.; Pillai, A.; Singal, A.G. Update on the Diagnosis and Treatment of Hepatocellular Carcinoma. Gastroenterol. Hepatol. 2020, 16, 506–516. [Google Scholar]
- Upputuri, P.K.; Pramanik, M. Recent advances in photoacoustic contrast agents for in vivo imaging. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2020, 12, e1618. [Google Scholar] [CrossRef] [PubMed]
- Luengo Morato, Y.; Ovejero Paredes, K.; Lozano Chamizo, L.; Marciello, M.; Filice, M. Recent Advances in Multimodal Molecular Imaging of Cancer Mediated by Hybrid Magnetic Nanoparticles. Polymers 2021, 13, 2989. [Google Scholar] [CrossRef]
- Deng, H.; Shang, W.; Wang, K.; Guo, K.; Liu, Y.; Tian, J.; Fang, C. Targeted-detection and sequential-treatment of small hepatocellular carcinoma in the complex liver environment by GPC-3-targeted nanoparticles. J. Nanobiotechnol. 2022, 20, 156. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, J.; Wang, Y.; Hui, H.; Li, C.; Yang, J.; Zhang, P.; Fang, C.; Tian, J. Enhanced glypican-3-targeted identification of hepatocellular carcinoma with liver fibrosis by pre-degrading excess fibrotic collagen. Acta Biomater. 2023, 158, 435–448. [Google Scholar] [CrossRef]
- Qi, S.; Liu, G.; Chen, J.; Cao, P.; Lei, X.; Ding, C.; Chen, G.; Zhang, Y.; Wang, L. Targeted Multifunctional Nanoplatform for Imaging-Guided Precision Diagnosis and Photothermal/Photodynamic Therapy of Orthotopic Hepatocellular Carcinoma. Int. J. Nanomed. 2022, 17, 3777–3792. [Google Scholar] [CrossRef]
- Wang, C.; Cheng, X.; Peng, H.; Zang, Y. NIR-Triggered and ROS-Boosted Nanoplatform for Enhanced Chemo/PDT/PTT Synergistic Therapy of Sorafenib in Hepatocellular Carcinoma. Nanoscale Res. Lett. 2022, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Zhang, M.; Wang, W.; Wang, M.; Li, B.; Li, H.; Kuang, D.; Liang, C.; Ren, J.; Duan, X. Covalent organic polymer induces apoptosis of liver cancer cells via photodynamic and photothermal effects. Front. Oncol. 2022, 12, 986839. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| NPs | Experimental Protocol | Conclusions | References |
|---|---|---|---|
| Lecithin-modified Bi nanoparticles (Bi-Ln NPs) | 24 VX2 HCC rabbits were randomly divided into 4 groups, as follows: group A (IA Bi-Ln NPs + NIR Laser); group B (IV Bi-Ln NPs + NIR Laser); group C (IA PBS + NIR Laser); and group D (IA PBS). | Group A displayed a remarkably superior TIR, a higher tumor necrosis rate and an increased apoptosis rate, compared to all other groups. Transcatheter IA combined with IPTT is safe and effective in killing tumor cells and inhibiting tumor growth, and could be applied in HCC soon. | [114] (Zhou, J. et al., 2020) |
| Galactosylated polymer/gold nanorod nanocomposites: PHEA-g-BIB-pButMA)-g-PEG-GAL embedding AuNRs-C12 and loaded with SOR or LEN i.e., (SOR-NPs) and (LEN-NPs) | Anticancer activity of the SOR-NPs and LEN-NPs was assessed for two HCC cell lines and compared to NHDF. Cells were seeded in a 96-well plate with a density of 1.0 × 104 cells per well (200 μL) and grown for 24 h in a DMEM. Successively, the medium was replaced with a dispersion of SOR-NPs or LEN-NPs. Drug release profiles were evaluated by irradiating the dispersion of nanoparticles with a diode NIR laser (λ = 810 nm, at a power = 0.7 W/mL for 5 or 20 min, at different scheduled time intervals (0 h, 1 h, 3 h, and 6 h). Anticancer activity of the SOR-NPs and LEN-NPs was studied with (810 nm diode laser for 300 s (for SOR-NPs P = 10 W, for LEN-NPs P = 6 W) and without NIR exposure. | The hybrid nanosystems SOR-NPs and LEN-NPs (diameter of about 214 nm and 148 nm, respectively), demonstrated optimum NIR photothermal conversion, high drug loading, and excellent NIR-driven drug release enhancement. These smart drug-loaded hybrid nanosystems for NIR-triggered chemo-phototherapy in HCC with high biocompatibility entered the cancer cells overexpressing ASGPR, where they can release heat and drugs. The innovative approach potentially overcomes MDR in cancer and is a multimodal tool capable of selectively recognizing and killing HCC cells through dual-mode therapy. | [115] (Giammona, G. et al., 2022) |
| SQ890 was encapsulated with a GSH-sensitive polymer (PLGA-SS-mPEG) to obtain biocompatible SQ890@Fe NPs | Treatment of HepG-2 cells with different concentrations of SQ890@Fe NPs showed the potential to infiltrate cancer cells. The tumoricidal efficacy of SQ890@Fe NPs in vivo in mice, after anesthetization and 808 nm illumination (1 W/cm2) for 5 min, increased the temperature at the tumor sites above 50 °C in 5 min, which led to tumor ablation. | Combined PTT and ferrotherapy on SQ890@Fe NPs demonstrated increased efficacy and safety in the treatment of HCC both in vitro and in vivo by mutually promoting two treatment mechanisms. | [116] (Tang, L. et al., 2022) |
| HPW@PANI nanorods | HPW@PANI nanorods were applied for in situ NIR-II PTT in orthotopic HCC in rabbits. 1064 nm laser energy was delivered through an optical fiber inserted interventionally into the VX2 primary tumor, with the protocol being tested for different laser power densities for primary tumor ablation, inhibition of distant tumors, and suppression of peritoneal metastases. | HPW@PANI nanorods prepared via oxidative chemical polymerization exhibited strong NIR-II absorption, higher photothermal conversion efficiency, and excellent biocompatibility. In vivo experiments proved that in situ NIR-II PTT could ablate primary tumors, inhibit distant tumors, and suppress peritoneal metastasis, opening new avenues for the management of deeply camouflaged solid tumors. | [120] (Tian, C. et al., 2022) |
| Multifunctional Oxa@MIL-PDA-PEGTK NPs | After preparation, the Oxa@MIL-PDA-PEGTK NPs were tested for the cumulative release of oxaliplatin and the photothermal effect at different concentrations of NPs using CW irradiation with an 808 nm laser (for 400 s, at a power density of 1 W/cm2). HCC cell line MHCC97H, HCC cell line PLC/PRF/5 and the normal hepatic epithelial cell line L02 were used. Cancer cells were incubated with 100 μg/mL Oxa@MIL-PDA-PEGTK NPs for 4 h, and either left untreated or exposed to 808 nm laser irradiation for 10 min at a power density of 2.0 W/cm2. PLC/PRF/5 cells (1 × 106) were diluted in 100 μL PBS and injected subcutaneously into the right axillary region of male BALB/C-nu mice (5 weeks old). Biodistribution of NPs and photothermal imaging, in vivo tumor growth inhibition, and biochemical examination and pathological analysis of mice were studied. | This multifunctional NP-based DDS could effectively deliver chemotherapeutic agents to tumors. In vitro experiments demonstrated Fe2+ release at tumor sites, increased ROS generation in laser-irradiated cancer cells, while exhibiting low cytotoxicity in non-cancerous cells, facts confirmed by in vivo studies. Design of novel TME-responsive nanoplatforms will soon improve the cure of HCC. | [121] (Huang, R. et al., 2023) |
| Photosensitizer | PTT and PDT Protocol | Conclusions | References |
|---|---|---|---|
| Structural variants of phthalocyanine (Pc) | In vivo PTT efficacy of Pcs on S180 tumors was tested. Pcs were injected into the S180 tumor in mice, after which the area was irradiated with a 685 nm laser for 10 min at a power density of 0.2 W/cm2. | By structural adjustment, the authors obtained three Pc derivatives with PTT activity against human HCC. PcC1 had a very good in vivo PTT effect against S180 tumors in carrier mice. Pc molecular dyes are suitable for PTT, for the advanced promotion of Pc molecular dye-based multifunctional phototheranostic agents. | [125] (Li, X. et al., 2018) |
| CAR-T cell membrane-coated nanoparticles (CIMs) | In vitro antitumor effect was investigated on Huh-7 cell cultures incubated with CIMs, and in vivo after abdominal tumor development with the same cells in BALB/c-nu mice irradiated with an 808 nm laser (0.6 W/cm2, for 5 min). | CIMs demonstrated very good targeting and PTT efficacy, giving rise to a promising method for the treatment of HCC. | [126] (Ma, W. et al., 2020) |
| Nanoplatform ICG&Cur@MoS2 | The PTT properties of ICG&Cur@MoS2 NPs were tested in vitro by irradiation with an 808 nm laser at 2.0 W/cm2 for 5 min on ICG&Cur@MoS2 samples at different concentrations. The effect of PTT-PDT in vitro was investigated after irradiation of different groups of HepG-2 cells incubated with ICG, MoS2, ICG@MoS2 or ICG&Cur@MoS2. The effect of PTT-PDT in vivo was investigated by a randomized study on six groups of mice with abdominal tumors induced by experimental H22 cell line. The NIR groups were irradiated in the tumor area with an 808 nm laser (1.2 W/cm2) for 5 min, at 10 h post-injection. Both body weight and tumor size were measured and recorded carefully. | Cell viability in the ICG&Cur@MoS2 + NIR group was significantly lower than that in the ICG@MoS2 + NIR group. The results can be attributed to the synergistic effect of PTT-PDT and P-gp inhibition. ICG@MoS2 + NIR group tumors were significantly smaller than in MoS2 + NIR group. Compared with the control group, P-gp in HepG-2 cells treated with ICG&Cur@MoS2 was significantly inhibited. | [130] (Li, S. et al., 2021) |
| 1-[2-Hydroxyethyl]-4-[4-(1,2,2-triphenylvinyl) styryl]pyridinium bromide (TPE-Py-OH) | For long-term PDT in vitro, HepG2 cells were incubated with various concentrations of TPE-Py-OH, and then exposed to a blue laser with different durations (450 nm, 30 mW/cm2, 18–45 J/cm2). In vivo multiple light-activated PDT was investigated in a randomized study on 5 groups of 8 animals per group with HCC induced by cell line H22. TPE-Py-OH was intratumorally injected, and further irradiated with a blue laser (450 nm, 100 mW/cm2, 10 min, 60 J/cm2). | TPE-Py-OH as an innovative AIE-active PS could be promising for tracking and PDT ablation of HCC with uninterrupted efficacy. | [133] (Chai, C. et al., 2022) |
| P(AAm-co-AN)-AuNRs@CeO2-Ce6 (PA/Ce6) | The antitumor effects of PDT/PTT in vitro were studied on HepG2 cells incubated with PA/Ce6, followed by 660 nm and 880 nm laser irradiation for 600 s. The antitumor efficacy of PDT/PTT in vivo was investigated by monitoring the weight and volume of abdominal HCC in 6 groups of mice randomized as follows: IV saline solution; saline + light (808 nm + laser 660 nm); PA/Ce6; PA/Ce6 + 808 nm laser; PA/Ce6 + 660 nm laser; and PA/ce6 + light (808 nm + 660 nm lasers). | Viability of HepG2 cells incubated with PA/Ce6 was reduced after 660 nm and 880 nm laser irradiation. PA/Ce6 could decompose hydrogen peroxide under laser irradiation and attenuate the anaerobic TME, opening up favorable future opportunities for the management of HCC by synergistic PTT and PDT. | [134] (Li, B. et al., 2022) |
| ICG/Pt@PDA-CXCR4 (IPP-c) | After HepG2 cells were incubated with IPP-c NPs, they were irradiated with an 808 nm laser for 10 min compared with a non-irradiated set. BALB/c nude mice bearing orthotopic SHCC tumors received I.V. IPP-c NPs, after which they were irradiated in the area of liver tumors for 12 min with an 808 nm laser at a dose of 0.8 W/cm2. | CXCR4-targeted multifunctional nanoparticles for mini-invasive phototherapy of orthotopic SHCCs by real-time quantitative optical imaging guidance provide another perspective for constructing a nanoplatform for early-stage HCC phototheranostics. | [143] (Qi, S. et al., 2022) |
| MnO2-SOR-Ce6@PDA- PEG-FA (MSCPF) | Investigation of the photothermal effect of MnO2 and PDA by irradiating H2O, MnO2 and MnO2@PDA samples irradiated with an 808 nm laser for 10 min at a power of 2 W/cm2. A series of MSCPF solutions (50, 100, 200 μg/mL) at different power densities (0.5–2.0 W/cm2) were applied for the test, and the temperature rise was recorded by an NIR thermal camera. In vitro PTT/PDT efficiency was studied on SMMC-7721 cell cultures irradiated with a laser at 808 nm (for PTT, 1.5 W/cm2) or 660 nm (for PDT, 500 mW/cm2) for 10 min, after incubation with Ce6, MCP and MCPF. The antitumor effect of MSCPF NPs was evaluated in vivo on SMMC-7721 tumor-bearing mice randomly divided into four groups. | In comparison with H2O, MnO2 showed a significant temperature rise from 28.9 to 42.7 °C, while MnO2@PDA showed higher photothermal conversion efficiency, with the temperature rising from 28.9 to 53.1 °C in 10 min. MCPF demonstrated high phototoxicity on SMMC-7721 cells and had superior antitumor effects by combining PTT with PDT. A reduction in tumor volume was observed after administration of sorafenib, MCPF and MSCPF. The synergistic tumor-targeted and hypoxia-alleviated nanoplatform (MSCPF) that co-deliver sorafenib, Ce6, and MnO2 for combined chemo/PDT/PTT therapy proved an enhanced antitumor effect in HCC. | [144] (Wang, C. et al., 2022) |
| Supramolecular material Purp@COP | In vitro HCC cell line HepG2 was cultured for 24 h with Purp@COP, after which it was irradiated with an 808 nm NIR laser at a dose of 1 W/cm2 for 10 min. | The supramolecular material Purp@COP had double effects, both photodynamic and photothermal, with the suppression of the proliferation of cancer cells and their significant destruction. Purp@COP could be a PS with potential in the treatment of HCC. | [145] (Xu, W. et al., 2022) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ailioaie, L.M.; Ailioaie, C.; Litscher, G. Synergistic Nanomedicine: Photodynamic, Photothermal and Photoimmune Therapy in Hepatocellular Carcinoma: Fulfilling the Myth of Prometheus? Int. J. Mol. Sci. 2023, 24, 8308. https://doi.org/10.3390/ijms24098308
Ailioaie LM, Ailioaie C, Litscher G. Synergistic Nanomedicine: Photodynamic, Photothermal and Photoimmune Therapy in Hepatocellular Carcinoma: Fulfilling the Myth of Prometheus? International Journal of Molecular Sciences. 2023; 24(9):8308. https://doi.org/10.3390/ijms24098308
Chicago/Turabian StyleAilioaie, Laura Marinela, Constantin Ailioaie, and Gerhard Litscher. 2023. "Synergistic Nanomedicine: Photodynamic, Photothermal and Photoimmune Therapy in Hepatocellular Carcinoma: Fulfilling the Myth of Prometheus?" International Journal of Molecular Sciences 24, no. 9: 8308. https://doi.org/10.3390/ijms24098308