
Matrix Metallopeptidase-Gene Signature Predicts Stage I Lung Adenocarcinoma Survival Outcomes


1
Department of Environmental and Occupational Health, School of Public Health, University of Pittsburgh, Pittsburgh, PA 15261, USA
2
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei 11490, Taiwan
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2023, 24(3), 2382; https://doi.org/10.3390/ijms24032382
Submission received: 21 December 2022
/
Revised: 16 January 2023
/
Accepted: 22 January 2023
/
Published: 25 January 2023
(This article belongs to the Special Issue Advances in the Molecular Biology of Lung Disease)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Tumor recurrence poses a significant challenge to the clinical management of stage I lung adenocarcinoma after curative surgical resection. Matrix metalloproteinases (MMPs) increase expression and correlate with recurrence and metastasis in surgically resected non-small cell lung cancer. However, the impact of MMPs on survival outcome varies, and their roles in patients with stage I lung adenocarcinoma remain unclear. In two discovery cohorts, we first analyzed 226 stage I–II lung adenocarcinoma cases in the GSE31210 cohort using a clustering-based method and identified a 150-gene MMP cluster with increased expression in tumors associated with worse survival outcomes. A similar analysis was performed on 517 lung adenocarcinoma cases in the Cancer Genome Atlas cohort. A 185-gene MMP cluster was identified, which also showed increased expression in tumors and correlated with poor survival outcomes. We further streamlined from the discovery cohorts a 36-gene MMP signature significantly associated with recurrence and worse overall survival in patients with stage I lung adenocarcinoma after surgical resection. After adjusting for covariates, the high MMP-gene signature expression remained an independent risk factor. In addition, the MMP-gene signature showed enrichment in epidermal growth factor receptor wild-type lung tumors, especially for those with Kirsten rat sarcoma virus mutations. Using an independent validation cohort, we further validated the MMP-gene signature in 70 stage I lung adenocarcinoma cases. In conclusion, MMP-gene signature is a potential predictive and prognostic biomarker to stratify patients with stage I lung adenocarcinoma into subgroups based on their risk of recurrence for aiding physicians in deciding the personalized adjuvant therapeutics.
1. Introduction
Lung cancer is the leading cancer-related death worldwide, with a 5-year survival rate of 22% [1]. About 80% of lung cancer patients are diagnosed with locally advanced or metastatic disease when curative surgery is no longer feasible [2]. Regardless of curative surgery for early-stage lung cancer, 20% to 40% of stage I patients will have tumor recurrence, which remains the leading cause of cancer-related death [3,4,5,6,7,8]. Patients with stage I lung adenocarcinoma, the most common histological subtype, vary in survival outcomes [8,9]. This indicates that the current TNM staging system fails to distinguish patients at a higher risk of recurrence for stage I lung cancer following surgical resection [10].
Although adjuvant chemotherapy has been shown to decrease tumor recurrence and prolong survival in completely resected stage II or III non-small cell lung cancer (NSCLC), its role in stage I disease remains controversial [11]. The current National Comprehensive Cancer Network guidelines for NSCLC recommend postoperative chemotherapy for patients with stage IB (T2a, N0) disease and negative surgical margins who have high-risk features, including tumors larger than 4 cm, poorly differentiated tumors, vascular invasion, visceral pleural involvement, wedge resection, and unknown lymph node status (Nx) [12]. Furthermore, Osimertinib is also recommended as an adjuvant therapy option for eligible patients with completely resected stage IB to IIIA NSCLC with epidermal growth factor receptor (EGFR) exon 19 deletions or L858R mutations who have previously received adjuvant chemotherapy or are ineligible to receive platinum-based chemotherapy [13]. Nevertheless, previous studies showed that patients with stage I disease did not benefit from adjuvant chemotherapy after surgical resection except for survival advantage for stage IB patients who had tumor size ≥4 cm [14]. This is probably because patients with stage I disease and a low risk of recurrence may not benefit from routine adjuvant chemotherapy. However, patients with high-risk factors such as large tumor size (≥4 cm) demonstrated a significant survival difference in favor of adjuvant chemotherapy. This highlights the need for reliable predictive biomarkers to stratify high-risk stage I disease for adjuvant chemotherapy.
Degradation of the extracellular matrix and penetration of the basement membrane have been shown to involve in tumor invasion and metastasis [15,16]. The matrix metalloproteinases (MMPs) are a family of 24 proteolytic enzymes that degrade the extracellular matrix and are involved in many phases of cancer progression, including invasiveness, angiogenesis, and metastasis [16,17,18,19]. Studies have shown that high levels of MMPs were expressed in lung tumors and correlated with tumor recurrence and poor survival outcomes in patients with surgically resected non-small cell lung cancer (NSCLC) [20,21,22,23,24,25,26,27,28]. In addition, each MMP can degrade multiple substrates, and many substrates are degraded by various MMPs, suggesting that multiple MMPs may involve in either physiological processes or disease progression such as cancer [29]. However, previous studies assessed the individual MMP as a prognostic marker, which may overlook the effect of co-expressed MMPs and related genes on survival outcomes, leading to inconsistent results [30]. Moreover, the function of different types of MMPs vary, and their effects on survival outcomes for stage I lung adenocarcinoma remain unknown.
In this study, we analyzed two publicly available lung adenocarcinoma datasets from GSE31210 and the Cancer Genome Atlas using the clustering-based method and discovered MMP-enriched gene clusters. A streamlined 36-gene molecular signature was identified from these two MMP-gene clusters as a potential biomarker to predict survival outcomes in patients with stage I lung adenocarcinoma after complete resection. Finally, we validated the utility of the predictive and prognostic transcriptome MMP-gene signature in an independent cohort.
2. Results
2.1. MMPs Overexpress in Lung Tumors and Correlate with Survival Outcomes in the GSE31210 Cohort
To examine MMP expression in lung tumors, we analyzed the gene expression of 226 lung adenocarcinoma samples and 20 normal lung samples from the GSE31210 stage I–II lung adenocarcinoma cohort (Supplementary Table S1). We performed an unsupervised hierarchical clustering analysis showing the heatmap of differentially expressed genes (absolute fold change >2.5, FDR < 0.05) between tumor and normal tissue (Figure 1A) in this cohort. The results showed a 150-gene cluster with enriched MMPs, including MMP1, MMP3, MMP9, MMP11, MMP12, and MMP13 (Figure 1A and Supplementary Table S2) and increased expression in tumors compared to normal lung tissue (Figure 1B). In addition, tissue inhibitors of metalloproteinases (TIMPs) such as TIMP-1 increased expression in tumors, but TIMP-2 and TIMP-3 decreased expression in tumors in contrast to normal lung tissue (Figure 1B). The ingenuity pathway analysis of the 150-gene cluster showed significant pathways associated with the participation of MMPs (Figure 1C and Supplementary Table S3). An unsupervised hierarchical clustering heatmap revealed four lung adenocarcinoma subgroups clustered with the 150-gene cluster (Figure 1D). Overall, the MMP-gene cluster expression from subgroup 1 to subgroup 4 was consistent with the expression pattern from low to high. In addition, patients with higher gene cluster expression correlated with worse progression-free survival (PFS) and overall survival (OS) than those with lower expression (Figure 1E and Supplementary Figure S1A).
2.2. MMPs Overexpress in Lung Tumors and Correlate with Survival Outcomes in TCGA Cohort
To validate the results from the GSE31210 cohort, we performed a transcriptome analysis of the Cancer Genome Atlas (TCGA) lung adenocarcinoma cohort (Supplementary Table S4), which included 517 lung tumor samples and 59 adjacent normal lung tissue samples. The unsupervised hierarchical clustering heatmap based on the differentially expressed genes (absolute fold change >2.5, FDR < 0.05) between the tumor and the adjacent normal lung tissue (Figure 2A). Consistently, the result showed a 185-gene cluster with enriched MMPs, including MMP1, MMP3, MMP9, MMP10, MMP11, MMP12, and MMP13 (Figure 2A and Supplementary Table S2), showing increased expression in tumors than adjacent normal lung tissue (Figure 2B). Furthermore, TIMP-1 increased expression in tumors, but TIMP-2, TIM-3, and TIMP-4 decreased expression in tumors compared with normal lung tissue (Figure 1B). Similar to the results from the GSE31210 cohort, ingenuity pathway analysis of the 185-gene cluster revealed significant pathways mainly involving MMPs in the TCGA lung adenocarcinoma cohort (Figure 2C and Supplementary Table S5). An unsupervised hierarchical clustering heatmap revealed four lung adenocarcinoma subgroups clustered with the 185-gene cluster (Figure 2D). Similarly, patients with higher MMP-gene cluster expression correlated with worse PFS and OS than those with lower expression (Figure 2E and Supplementary Figure S2A).
2.3. Development of a 36-Gene MMP Signature and Network Analysis
To search for more stable molecular signatures associated with MMPs in these two cohorts, we identified 36 overlapping genes from the MMP-related gene clusters between GSE31210 and TCGA cohort, termed the 36-gene MMP signature (Figure 3A and Supplementary Table S2). Ingenuity pathway analysis of the 36-gene MMP signature also showed significant pathways with enrichment related to MMPs (Figure 3B and Supplementary Table S6). The network analysis of the 150-gene cluster from the GSE31210 cohort showed the prediction of critical upstream regulators such as MYBL2, E2F8, FOXM1, and FHL2 to regulate this interaction network transcriptionally (Figure 3C). In addition, the 185-gene cluster from the TCGA cohort revealed the network’s connection of MAPK/ERK and NFκB pathway (Figure 3D).
2.4. High 36-Gene MMP Signature Expression Predicts Poor Survival Outcomes in GSE3120 Stage I Lung Adenocarcinomas
To determine the prognostic value of the streamlined 36-gene MMP signature in stage I lung adenocarcinoma cases, we performed unsupervised hierarchical clustering heatmap analysis of the gene signature and stage I lung adenocarcinoma from the GSE31210 cohort. The result revealed three lung adenocarcinoma subgroups clustered with the gene signature (Figure 4A). In survival analysis, patients with higher gene signature expression were associated with worse PFS and OS than those with lower expression (Figure 4B and Supplementary Figure S1B). Notably, the patient cluster with increased MMP gene signature expression remained an independent risk factor for PFS and OS in patients with stage I lung adenocarcinoma after adjustment of other covariates, including stage, gender, age, smoking, and mutation status (Supplementary Table S7). We also analyzed the gene mutation, gender, and smoking status in these subgroups, and the results revealed that lung cancer subgroups with higher MMPs-gene signature expression were associated with a higher proportion of EGFR wild type, Kirsten rat sarcoma virus (KRAS) mutation, triple-negative mutations, male, and ever-smoker (Figure 4C). Consistently, the GSEA showed that the 36-gene MMP signature enriched in EGFR wild-type lung tumors, especially in KRAS-driven lung tumors (Figure 4D).
2.5. High 36-Gene MMP Signature Expression Predicts Poor Survival Outcomes in TCGA Stage I Lung Adenocarcinomas
We further used the 36-gene MMPs signature to analyze the TCGA stage I lung adenocarcinoma cases. Unsupervised hierarchical clustering heatmap of the gene signature and the stage I cases showed four lung adenocarcinoma subgroups (Figure 5A). In survival analysis, patients with higher MMPs-gene signature expression correlated with poor survival outcomes than those with lower expression (Figure 5B and Supplementary Figure S2B). We also analyzed the gene mutation, gender, and smoking status in these subgroups. The results revealed that mutation statuses were differentially distributed between subgroups, suggesting that the MMP-gene signature was associated with driver oncogenes. (Figure 5C). Furthermore, a higher proportion of males and smoking history were correlated with higher MMP-gene signature expression in lung cancer subgroups (Figure 5C).
2.6. A 36-Gene MMPs Signature Is Validated in An Independent Lung Cancer Cohort
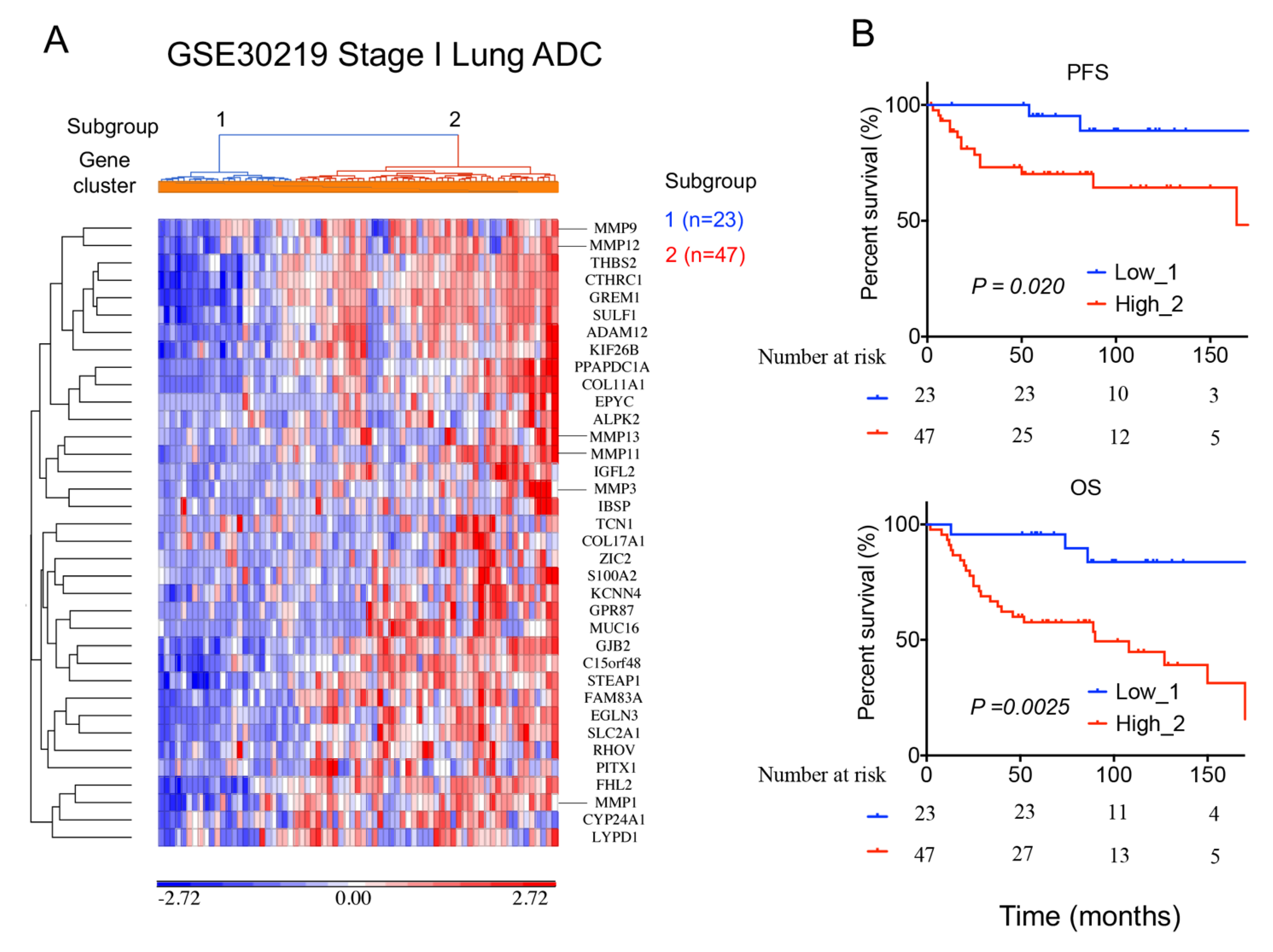
To validate the 36-gene MMPs signature in an independent lung cancer cohort, we analyzed 70 stage I (T1N0M0) lung adenocarcinoma cases from the GSE30219 cohort (Supplementary Table S8). The unsupervised hierarchical clustering heatmap of the gene signature and stage I cases showed two lung adenocarcinoma subgroups (Figure 6A). Consistently, patients with higher MMP-gene signature expression correlated with worse PFS and OS compared to those with lower expression (Figure 6B).
3. Discussion
Surgical resection is the primary curative therapeutic option in patients with stage I lung adenocarcinoma. However, tumor recurrence remains one of the leading causes of cancer-related deaths, highlighting the urgent need for accurate predictive biomarkers to improve clinical management of stage I lung adenocarcinoma after surgical resection. In this study, we performed transcriptome analysis using a clustering-based method. We discovered MMP-enriched gene clusters, which increased expression in tumors compared to normal lung tissue and correlated with poor prognosis in two independent lung adenocarcinoma cohorts. We further identified a 36-gene MMP-gene signature from these two MMP-gene clusters, which showed enrichment in EGFR wild-type lung tumors, especially for those with KRAS mutations. In addition, the high MMP-gene signature expression independently predicts recurrence and poor overall survival in patients with stage I lung adenocarcinoma after complete resection. Finally, an independent cohort was used to validate the MMP-gene signature’s robustness successfully.
Although individual MMPs have been reported to correlate with survival outcomes in patients with surgically resected NSCLC, these results were inconsistent or not reproducible in different cohorts [31,32,33,34,35,36,37,38,39,40,41], and their effects on stage I lung adenocarcinoma remain unclear. We hypothesized that various MMPs were heterogeneously expressed in lung adenocarcinoma, and their effects on survival outcomes varied. Here, we performed unsupervised hierarchical clustering of DEGs between tumor and normal lung tissue in two lung adenocarcinoma cohorts. Our results showed MMP-enriched gene clusters containing MMP1, MMP3, MMP9, MMP11, MMP12, and MMP13 in these two cohorts. Notably, these MMPs were clustered together and overexpressed in lung tumors compared to normal lung tissue, suggesting that they display similar gene expression patterns and may be functionally related during lung tumorigenesis. We also analyzed tissue inhibitors of metalloproteinases (TIMPs) expression, including four paralogues (TIMP1–TIMP4) initially characterized as inhibitors of MMPs [42]. TIMP-1 increased expression in tumors compared to normal lung tissue in the cohorts. In contrast, TIMP-2, TIMP-3, and TIMP-4 showed lower expression in the tumors. These results demonstrated that TIMP expression, like MMP expression, varied in lung adenocarcinoma and has been reported to correlate with survival outcomes [43,44,45].
Consistent with this assumption, the network analysis also demonstrated direct and indirect interaction among MMPs and associated genes within the gene clusters. Therefore, using individual MMP as a predictive or prognostic biomarker to predict survival outcomes may not be sufficient or representative, contributing to inconsistent results in the current knowledge. Furthermore, adjuvant chemotherapy and radiotherapy also influence survival outcomes and may affect survival analysis in surgically resected NSCLC. Therefore, we performed the survival analysis of patients with stage I lung adenocarcinoma who received surgical resection without adjuvant chemotherapy or radiotherapy in the GSE31210 and GSE30219 cohorts. Despite the incomplete data of adjuvant therapy after surgery in the TCGA cohort, the result was consistent with other cohorts in that the higher MMP-gene signature expression was associated with recurrence and poor overall survival in patients with surgically resected stage I lung adenocarcinoma.
Our results showed that the 36-gene MMP signature displayed enrichment in EGFR wild-type lung tumors, especially for those with KRAS mutations compared to ALK translocation and triple-negative mutations, suggesting that these signature genes may be associated with KRAS-driven pathways. Consistently, lung cancer subgroups with higher MMP-gene signature expression in the cohorts have a higher proportion of male and smoking history, which has been linked to KRAS mutations [46,47]. Previous studies have shown that patients with stage I lung adenocarcinoma and KRAS mutations have a significantly higher risk of recurrence than those without the mutation [48,49]. In agreement, a recent meta-analysis suggested that KRAS mutations are associated with poor survival outcomes, especially in patients with lung adenocarcinoma and stage I disease [50]. These findings may be partly explained by the high MMP-gene signature expression associated with lung adenocarcinoma with KRAS mutations and correlated with recurrence and worse overall survival, as seen in our results. Remarkably, the patients in the GSE31210 cohorts showed a higher EGFR mutation rate (61%) compared to the TCGA cohort (11%), which is consistent with the Asians with higher EGFR mutation rates in lung adenocarcinoma such as the GSE31210 cohort conducted in Japan [51]. Nonetheless, the MMP-gene signature remained robust to predict survival outcomes regardless of the heterogenicity, such as ethnicity, mutation status, and different platforms within these cohorts.
Several MMPs inhibitors (MMPIs) were developed and used to treat various cancer types in clinical trials during the late 1990s and early 2000s [52,53,54]. Even though the MMPIs showed promising effects in blocking tumor growth and metastasis in preclinical studies, clinical trials of these drugs were not successful [55,56,57]. Multiple reasons have been postulated for the explanation, including the difference between human and murine biology, the non-specificity of MMPIs, and the drug administration being at an advanced stage [58]. Preclinical testing reflected that MMPIs successfully inhibited early-stage cancers and hematogenous metastases while having less effect on large tumors [56]. It has been proposed that new trials should be designed to use MMPIs in patients with early-stage cancers and a high risk of metastasis after surgery or as neoadjuvant therapy prior to surgery [58]. The MMP-gene signature may be a useful predictive biomarker for future clinical trials to identify patients with early-stage lung adenocarcinoma and a high risk of recurrence for MMPI treatment after curative surgery.
4. Materials and Methods
4.1. Patient and Expression Data
4.1.1. GSE31210 Cohort
The microarray expression data and clinical data were previously obtained under an IRB-approved protocol with informed consent, and downloaded from the National Center for Biotechnology Information Gene Expression Omnibus database (http://www.ncbi.nlm.nih.gov/geo, accessed on 18 April 2019) [59]. Raw gene-expression data were normalized by MAS5. A total of 226 lung adenocarcinoma cases comprised 168 stage I and 58 stage II cases, and 20 normal lung tissue were subjected to expression profiling (Supplementary Table S1). The 204 cases who received complete resection with free resection margins and no involvement of mediastinal lymph nodes and did not receive postoperative chemotherapy and/or radiotherapy, unless relapsed, were subjected to survival analyses. Twenty-two cases were excluded from prognosis analysis due to incomplete resection or adjuvant therapy.
4.1.2. TCGA Cohort
TCGA lung adenocarcinoma RNAseq and clinical data were previously obtained under an IRB-approved protocol with informed consent, and downloaded from UCSC Xena (http://xena.ucsc.edu/, accessed on 4 May 2019) [60]. A total of 517 lung adenocarcinoma cases and 59 adjacent lung tissue were subjected to expression profiling (Supplementary Table S4). Among the 517 cases, 277 stage I cases with survival data were subjected to survival analysis.
4.1.3. GSE30219 Cohort
The microarray expression data and clinical data were previously obtained under an IRB-approved protocol, with informed consent, and downloaded from the National Center for Biotechnology Information Gene Expression Omnibus database (http://www.ncbi.nlm.nih.gov/geo, accessed on 5 May 2019) [61]. Raw gene-expression data were normalized by robust multi-array average (RMA). A total of 70 stage I (T1N0M0) lung adenocarcinoma cases who received surgery and did not receive postoperative chemotherapy and/or radiotherapy selected from 293 lung cancer cases were subjected to survival analysis (Supplementary Table S8).
4.2. Ingenuity Pathway Analysis (IPA)
MMP-related gene clusters and signatures, including 150-gene cluster, 185-gene cluster, and 36-gene MMP signature, were used to carry out gene set enrichment analysis using Ingenuity pathway analysis (IPA, http://www.ingenuity.com, accessed on 8 May 2019). IPA was used to determine which pathways were differentially represented in the identified significant genes, compared to the Ingenuity knowledge base.
4.3. Gene Set Enrichment Analysis (GSEA)
GSEA was applied using ranked lists of genes from the GSE31210 cohort based on mutation status and sorted by Signal2Noise. After Kolmogorov–Smirnoff testing, a 36-gene MMP signature showing a P < 0.05 was considered enriched between mutation status under comparison.
4.4. Bioinformatic and Statistical Analysis
Differential expression analysis between tumor and normal lung tissue was performed using Partek Genomics Suite (Partek, St. Louis, MO, USA), and the Benjamini–Hochberg method was used to adjust the raw P values for multiple testing. Only genes with fold change (up- and down-regulated) >2.5 and FDR < 0.05 were considered as differentially expressed genes (DEGs). MMP and TIMP expression between tumor and normal lung tissue were compared by Student’s t test. A hierarchical clustering heatmap was conducted using Partek Genomics Suite. Survival was compared using Kaplan–Meyer analysis. The stratification of signature as high or low depends on the expression level with significant differences in the survival outcomes and the lowest log-rank P value among subgroups. The log-rank test was used to compare survival or event-free survival between groups, and Cox proportional hazards modeling was used for univariate and multivariate analyses. Chi-squared test was used to compare frequencies in one or more categories. P < 0.05 was considered significant.
5. Conclusions
In summary, we analyzed transcriptome data of lung adenocarcinoma cases in two discovery cohorts using a clustering-based approach and discovered MMP-enriched gene clusters. A streamlined 36-gene MMPs signature was further identified and successfully predicted recurrence and worse overall survival in patients with stage I lung adenocarcinoma after curative surgery in discovery and validation cohorts. These results will be necessary for the proper stratification of early-stage patients with a high risk of disease recurrence and worse overall survival for optimized follow-up schedules and the use of adjuvant therapeutics such as chemotherapy or MMPIs in future clinical trials.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijms24032382/s1.
Author Contributions
Conceptualization, C.-H.L. and Y.P.D.; formal analysis, C.-H.L.; investigation, C.-H.L. and Y.P.D.; funding acquisition Y.P.D.; resources, Y.P.D.; supervision, Y.P.D.; writing—original draft, C.-H.L.; writing—review and editing, Y.P.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by R01 grants from the National Institutes of Health HL-125128 (NHLBI), AI-133351 (NIAID), and Tri-Service General Hospital Grant (TSGH-E-111235). The funding agencies had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
Details about IRB approval in the lung cancer cohorts can be found in the Materials and Methods.
Informed Consent Statement
Details about informed consent in the lung cancer cohorts can be found in the Materials and Methods.
Data Availability Statement
The datasets generated and/or analyzed are available as Supplementary Materials in the current study.
Acknowledgments
We thank Zhong Chen in the Tumor Biology Section and Clinical Genomics Unit, Head and Neck Surgery Branch, National Institute on Deafness and Other Communication Disorders, National Institutes of Health for her helpful comments and suggestions. We acknowledge the use of the PartekGS software licensed through the Molecular Biology Information Service of the Health Sciences Library System at the University of Pittsburgh.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Schabath, M.B.; Cote, M.L. Cancer Progress and Priorities: Lung Cancer. Cancer Epidemiol. Biomarkers Prev. 2019, 28, 1563–1579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martini, N.; Bains, M.S.; Burt, M.E.; Zakowski, M.F.; McCormack, P.; Rusch, V.W.; Ginsberg, R.J. Incidence of local recurrence and second primary tumors in resected stage I lung cancer. J. Thorac. Cardiovasc. Surg. 1995, 109, 120–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harpole, D.H., Jr.; Herndon, J.E., 2nd; Young, W.G., Jr.; Wolfe, W.G.; Sabiston, D.C., Jr. Stage I nonsmall cell lung cancer. A multivariate analysis of treatment methods and patterns of recurrence. Cancer 1995, 76, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Al-Kattan, K.; Sepsas, E.; Fountain, S.W.; Townsend, E.R. Disease recurrence after resection for stage I lung cancer. Eur. J. Cardiothorac. Surg. 1997, 12, 380–384. [Google Scholar] [CrossRef]
- Nakagawa, T.; Okumura, N.; Ohata, K.; Igai, H.; Matsuoka, T.; Kameyama, K. Postrecurrence survival in patients with stage I non-small cell lung cancer. Eur. J. Cardiothorac. Surg. 2008, 34, 499–504. [Google Scholar] [CrossRef] [Green Version]
- Hung, J.J.; Jeng, W.J.; Chou, T.Y.; Hsu, W.H.; Wu, K.J.; Huang, B.S.; Wu, Y.C. Prognostic value of the new International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society lung adenocarcinoma classification on death and recurrence in completely resected stage I lung adenocarcinoma. Ann. Surg. 2013, 258, 1079–1086. [Google Scholar] [CrossRef]
- Tsutani, Y.; Suzuki, K.; Koike, T.; Wakabayashi, M.; Mizutani, T.; Aokage, K.; Saji, H.; Nakagawa, K.; Zenke, Y.; Takamochi, K.; et al. High-Risk Factors for Recurrence of Stage I Lung Adenocarcinoma: Follow-up Data From JCOG0201. Ann. Thorac. Surg. 2019, 108, 1484–1490. [Google Scholar] [CrossRef]
- Ujiie, H.; Kadota, K.; Chaft, J.E.; Buitrago, D.; Sima, C.S.; Lee, M.C.; Huang, J.; Travis, W.D.; Rizk, N.P.; Rudin, C.M.; et al. Solid Predominant Histologic Subtype in Resected Stage I Lung Adenocarcinoma Is an Independent Predictor of Early, Extrathoracic, Multisite Recurrence and of Poor Postrecurrence Survival. J. Clin. Oncol. 2015, 33, 2877–2884. [Google Scholar] [CrossRef]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef]
- Chaft, J.E.; Shyr, Y.; Sepesi, B.; Forde, P.M. Preoperative and Postoperative Systemic Therapy for Operable Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2022, 40, 546–555. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef]
- Wu, Y.L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef]
- Strauss, G.M.; Herndon, J.E., 2nd; Maddaus, M.A.; Johnstone, D.W.; Johnson, E.A.; Harpole, D.H.; Gillenwater, H.H.; Watson, D.M.; Sugarbaker, D.J.; Schilsky, R.L.; et al. Adjuvant paclitaxel plus carboplatin compared with observation in stage IB non-small-cell lung cancer: CALGB 9633 with the Cancer and Leukemia Group B, Radiation Therapy Oncology Group, and North Central Cancer Treatment Group Study Groups. J. Clin. Oncol. 2008, 26, 5043–5051. [Google Scholar] [CrossRef] [Green Version]
- Stamenkovic, I. Matrix metalloproteinases in tumor invasion and metastasis. Semin. Cancer Biol. 2000, 10, 415–433. [Google Scholar] [CrossRef]
- Winkler, J.; Abisoye-Ogunniyan, A.; Metcalf, K.J.; Werb, Z. Concepts of extracellular matrix remodelling in tumour progression and metastasis. Nat. Commun. 2020, 11, 5120. [Google Scholar] [CrossRef]
- Kessenbrock, K.; Plaks, V.; Werb, Z. Matrix metalloproteinases: Regulators of the tumor microenvironment. Cell 2010, 141, 52–67. [Google Scholar] [CrossRef] [Green Version]
- Shuman Moss, L.A.; Jensen-Taubman, S.; Stetler-Stevenson, W.G. Matrix metalloproteinases: Changing roles in tumor progression and metastasis. Am. J. Pathol. 2012, 181, 1895–1899. [Google Scholar] [CrossRef] [Green Version]
- Niland, S.; Riscanevo, A.X.; Eble, J.A. Matrix Metalloproteinases Shape the Tumor Microenvironment in Cancer Progression. Int. J. Mol. Sci. 2021, 23, 146. [Google Scholar] [CrossRef]
- Passlick, B.; Sienel, W.; Seen-Hibler, R.; Wockel, W.; Thetter, O.; Mutschler, W.; Pantel, K. Overexpression of matrix metalloproteinase 2 predicts unfavorable outcome in early-stage non-small cell lung cancer. Clin. Cancer Res. 2000, 6, 3944–3948. [Google Scholar]
- Cai, M.; Onoda, K.; Takao, M.; Kyoko, I.Y.; Shimpo, H.; Yoshida, T.; Yada, I. Degradation of tenascin-C and activity of matrix metalloproteinase-2 are associated with tumor recurrence in early stage non-small cell lung cancer. Clin. Cancer Res. 2002, 8, 1152–1156. [Google Scholar] [PubMed]
- Sienel, W.; Hellers, J.; Morresi-Hauf, A.; Lichtinghagen, R.; Mutschler, W.; Jochum, M.; Klein, C.; Passlick, B.; Pantel, K. Prognostic impact of matrix metalloproteinase-9 in operable non-small cell lung cancer. Int. J. Cancer 2003, 103, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Hong, K.P.; Hong, S.H.; Kang, S.; Chung, K.Y.; Cho, S.H. MMP expression profiling in recurred stage IB lung cancer. Oncogene 2004, 23, 845–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, H.S.; Hansen, G.; Richter, G.; Taege, C.; Simm, A.; Silber, R.E.; Burdach, S. Matrix metalloproteinase-12 expression correlates with local recurrence and metastatic disease in non-small cell lung cancer patients. Clin. Cancer Res. 2005, 11, 1086–1092. [Google Scholar] [CrossRef]
- Hsu, C.P.; Shen, G.H.; Ko, J.L. Matrix metalloproteinase-13 expression is associated with bone marrow microinvolvement and prognosis in non-small cell lung cancer. Lung Cancer 2006, 52, 349–357. [Google Scholar] [CrossRef]
- Safranek, J.; Pesta, M.; Holubec, L.; Kulda, V.; Dreslerova, J.; Vrzalova, J.; Topolcan, O.; Pesek, M.; Finek, J.; Treska, V. Expression of MMP-7, MMP-9, TIMP-1 and TIMP-2 mRNA in lung tissue of patients with non-small cell lung cancer (NSCLC) and benign pulmonary disease. Anticancer Res. 2009, 29, 2513–2517. [Google Scholar]
- Li, M.; Xiao, T.; Zhang, Y.; Feng, L.; Lin, D.; Liu, Y.; Mao, Y.; Guo, S.; Han, N.; Di, X.; et al. Prognostic significance of matrix metalloproteinase-1 levels in peripheral plasma and tumour tissues of lung cancer patients. Lung Cancer 2010, 69, 341–347. [Google Scholar] [CrossRef]
- Lee, C.Y.; Shim, H.S.; Lee, S.; Lee, J.G.; Kim, D.J.; Chung, K.Y. Prognostic effect of matrix metalloproteinase-9 in patients with resected Non small cell lung cancer. J. Cardiothorac. Surg. 2015, 10, 44. [Google Scholar] [CrossRef] [Green Version]
- Greenlee, K.J.; Werb, Z.; Kheradmand, F. Matrix metalloproteinases in lung: Multiple, multifarious, and multifaceted. Physiol. Rev. 2007, 87, 69–98. [Google Scholar] [CrossRef] [Green Version]
- Hadler-Olsen, E.; Winberg, J.O.; Uhlin-Hansen, L. Matrix metalloproteinases in cancer: Their value as diagnostic and prognostic markers and therapeutic targets. Tumour Biol. 2013, 34, 2041–2051. [Google Scholar] [CrossRef]
- Ylisirnio, S.; Hoyhtya, M.; Turpeenniemi-Hujanen, T. Serum matrix metalloproteinases -2, -9 and tissue inhibitors of metalloproteinases -1, -2 in lung cancer--TIMP-1 as a prognostic marker. Anticancer Res. 2000, 20, 1311–1316. [Google Scholar]
- Kim, S.J.; Rabbani, Z.N.; Dewhirst, M.W.; Vujaskovic, Z.; Vollmer, R.T.; Schreiber, E.G.; Oosterwijk, E.; Kelley, M.J. Expression of HIF-1alpha, CA IX, VEGF, and MMP-9 in surgically resected non-small cell lung cancer. Lung Cancer 2005, 49, 325–335. [Google Scholar] [CrossRef]
- Shimanuki, Y.; Takahashi, K.; Cui, R.; Hori, S.; Takahashi, F.; Miyamoto, H.; Fukurchi, Y. Role of serum vascular endothelial growth factor in the prediction of angiogenesis and prognosis for non-small cell lung cancer. Lung 2005, 183, 29–42. [Google Scholar] [CrossRef]
- Leinonen, T.; Pirinen, R.; Bohm, J.; Johansson, R.; Ropponen, K.; Kosma, V.M. Expression of matrix metalloproteinases 7 and 9 in non-small cell lung cancer. Relation to clinicopathological factors, beta-catenin and prognosis. Lung Cancer 2006, 51, 313–321. [Google Scholar] [CrossRef]
- Hoikkala, S.; Paakko, P.; Soini, Y.; Makitaro, R.; Kinnula, V.; Turpeenniemi-Hujanen, T. Tissue MMP-2 and MMP-9 [corrected] are better prognostic factors than serum MMP-2/TIMP-2--complex or TIMP-1 [corrected] in stage [corrected] I–III lung carcinoma. Cancer Lett 2006, 236, 125–132. [Google Scholar] [CrossRef]
- Takemoto, N.; Tada, M.; Hida, Y.; Asano, T.; Cheng, S.; Kuramae, T.; Hamada, J.; Miyamoto, M.; Kondo, S.; Moriuchi, T. Low expression of reversion-inducing cysteine-rich protein with Kazal motifs (RECK) indicates a shorter survival after resection in patients with adenocarcinoma of the lung. Lung Cancer 2007, 58, 376–383. [Google Scholar] [CrossRef]
- Liu, D.; Nakano, J.; Ishikawa, S.; Yokomise, H.; Ueno, M.; Kadota, K.; Urushihara, M.; Huang, C.L. Overexpression of matrix metalloproteinase-7 (MMP-7) correlates with tumor proliferation, and a poor prognosis in non-small cell lung cancer. Lung Cancer 2007, 58, 384–391. [Google Scholar] [CrossRef]
- Matsuyama, M.; Chijiwa, T.; Inoue, Y.; Abe, Y.; Nishi, M.; Miyazaki, N.; Furukawa, D.; Mukai, M.; Suemizu, H.; Sekido, Y.; et al. Alternative splicing variant of vascular endothelial growth factor-A is a critical prognostic factor in non-small cell lung cancer. Oncol. Rep. 2009, 22, 1407–1413. [Google Scholar]
- Grossi, F.; Spizzo, R.; Bordo, D.; Cacitti, V.; Valent, F.; Rossetto, C.; Follador, A.; Di Terlizzi, S.; Aita, M.; Morelli, A.; et al. Prognostic stratification of stage IIIA pN2 non-small cell lung cancer by hierarchical clustering analysis of tissue microarray immunostaining data: An Alpe Adria Thoracic Oncology Multidisciplinary Group study (ATOM 014). J. Thorac. Oncol. 2010, 5, 1354–1360. [Google Scholar] [CrossRef] [Green Version]
- Zheng, S.; Chang, Y.; Hodges, K.B.; Sun, Y.; Ma, X.; Xue, Y.; Williamson, S.R.; Lopez-Beltran, A.; Montironi, R.; Cheng, L. Expression of KISS1 and MMP-9 in non-small cell lung cancer and their relations to metastasis and survival. Anticancer Res. 2010, 30, 713–718. [Google Scholar]
- Peng, W.J.; Zhang, J.Q.; Wang, B.X.; Pan, H.F.; Lu, M.M.; Wang, J. Prognostic value of matrix metalloproteinase 9 expression in patients with non-small cell lung cancer. Clin. Chim. Acta 2012, 413, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Kessenbrock, K.; Wang, C.Y.; Werb, Z. Matrix metalloproteinases in stem cell regulation and cancer. Matrix Biol. 2015, 44–46, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Yu, H.; Liu, S.Y.; Xiao, X.S.; Dong, W.H.; Chen, Y.N.; Xu, W.; Zhu, T. Prognostic value of tissue inhibitor of metalloproteinase-2 expression in patients with non-small cell lung cancer: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0124230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selvaraj, G.; Kaliamurthi, S.; Lin, S.; Gu, K.; Wei, D.Q. Prognostic Impact of Tissue Inhibitor of Metalloproteinase-1 in Non- Small Cell Lung Cancer: Systematic Review and Meta-Analysis. Curr. Med. Chem. 2019, 26, 7694–7713. [Google Scholar] [CrossRef]
- Mino, N.; Takenaka, K.; Sonobe, M.; Miyahara, R.; Yanagihara, K.; Otake, Y.; Wada, H.; Tanaka, F. Expression of tissue inhibitor of metalloproteinase-3 (TIMP-3) and its prognostic significance in resected non-small cell lung cancer. J. Surg. Oncol. 2007, 95, 250–257. [Google Scholar] [CrossRef]
- Liu, L.; Liu, J.; Shao, D.; Deng, Q.; Tang, H.; Liu, Z.; Chen, X.; Guo, F.; Lin, Y.; Mao, M.; et al. Comprehensive genomic profiling of lung cancer using a validated panel to explore therapeutic targets in East Asian patients. Cancer Sci. 2017, 108, 2487–2494. [Google Scholar] [CrossRef]
- Liu, S.Y.; Sun, H.; Zhou, J.Y.; Jie, G.L.; Xie, Z.; Shao, Y.; Zhang, X.; Ye, J.Y.; Chen, C.X.; Zhang, X.C.; et al. Clinical characteristics and prognostic value of the KRAS G12C mutation in Chinese non-small cell lung cancer patients. Biomark Res. 2020, 8, 22. [Google Scholar] [CrossRef]
- Woo, T.; Okudela, K.; Yazawa, T.; Wada, N.; Ogawa, N.; Ishiwa, N.; Tajiri, M.; Rino, Y.; Kitamura, H.; Masuda, M. Prognostic value of KRAS mutations and Ki-67 expression in stage I lung adenocarcinomas. Lung Cancer 2009, 65, 355–362. [Google Scholar] [CrossRef]
- Izar, B.; Zhou, H.; Heist, R.S.; Azzoli, C.G.; Muzikansky, A.; Scribner, E.E.; Bernardo, L.A.; Dias-Santagata, D.; Iafrate, A.J.; Lanuti, M. The prognostic impact of KRAS, its codon and amino acid specific mutations, on survival in resected stage I lung adenocarcinoma. J. Thorac. Oncol. 2014, 9, 1363–1369. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.M.; Zhu, Q.G.; Ding, X.X.; Lin, S.; Zhao, J.; Guan, L.; Li, T.; He, B.; Zhang, H.Q. Prognostic value of EGFR and KRAS in resected non-small cell lung cancer: A systematic review and meta-analysis. Cancer Manag. Res. 2018, 10, 3393–3404. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Au, J.S.; Thongprasert, S.; Srinivasan, S.; Tsai, C.M.; Khoa, M.T.; Heeroma, K.; Itoh, Y.; Cornelio, G.; Yang, P.C. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER). J. Thorac. Oncol. 2014, 9, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Hirte, H.; Vergote, I.B.; Jeffrey, J.R.; Grimshaw, R.N.; Coppieters, S.; Schwartz, B.; Tu, D.; Sadura, A.; Brundage, M.; Seymour, L. A phase III randomized trial of BAY 12-9566 (tanomastat) as maintenance therapy in patients with advanced ovarian cancer responsive to primary surgery and paclitaxel/platinum containing chemotherapy: A National Cancer Institute of Canada Clinical Trials Group Study. Gynecol. Oncol. 2006, 102, 300–308. [Google Scholar]
- Bramhall, S.R.; Schulz, J.; Nemunaitis, J.; Brown, P.D.; Baillet, M.; Buckels, J.A. A double-blind placebo-controlled, randomised study comparing gemcitabine and marimastat with gemcitabine and placebo as first line therapy in patients with advanced pancreatic cancer. Br. J. Cancer 2002, 87, 161–167. [Google Scholar] [CrossRef]
- Sparano, J.A.; Bernardo, P.; Stephenson, P.; Gradishar, W.J.; Ingle, J.N.; Zucker, S.; Davidson, N.E. Randomized phase III trial of marimastat versus placebo in patients with metastatic breast cancer who have responding or stable disease after first-line chemotherapy: Eastern Cooperative Oncology Group trial E2196. J. Clin. Oncol. 2004, 22, 4683–4690. [Google Scholar] [CrossRef]
- Coussens, L.M.; Fingleton, B.; Matrisian, L.M. Matrix metalloproteinase inhibitors and cancer: Trials and tribulations. Science 2002, 295, 2387–2392. [Google Scholar] [CrossRef]
- Winer, A.; Janosky, M.; Harrison, B.; Zhong, J.; Moussai, D.; Siyah, P.; Schatz-Siemers, N.; Zeng, J.; Adams, S.; Mignatti, P. Inhibition of Breast Cancer Metastasis by Presurgical Treatment with an Oral Matrix Metalloproteinase Inhibitor: A Preclinical Proof-of-Principle Study. Mol. Cancer Ther. 2016, 15, 2370–2377. [Google Scholar] [CrossRef]
- Overall, C.M.; Lopez-Otin, C. Strategies for MMP inhibition in cancer: Innovations for the post-trial era. Nat. Rev. Cancer 2002, 2, 657–672. [Google Scholar] [CrossRef]
- Winer, A.; Adams, S.; Mignatti, P. Matrix Metalloproteinase Inhibitors in Cancer Therapy: Turning Past Failures Into Future Successes. Mol. Cancer Ther. 2018, 17, 1147–1155. [Google Scholar] [CrossRef] [Green Version]
- Okayama, H.; Kohno, T.; Ishii, Y.; Shimada, Y.; Shiraishi, K.; Iwakawa, R.; Furuta, K.; Tsuta, K.; Shibata, T.; Yamamoto, S.; et al. Identification of genes upregulated in ALK-positive and EGFR/KRAS/ALK-negative lung adenocarcinomas. Cancer Res. 2012, 72, 100–111. [Google Scholar] [CrossRef] [Green Version]
- Hoadley, K.A.; Yau, C.; Hinoue, T.; Wolf, D.M.; Lazar, A.J.; Drill, E.; Shen, R.; Taylor, A.M.; Cherniack, A.D.; Thorsson, V.; et al. Cell-of-Origin Patterns Dominate the Molecular Classification of 10,000 Tumors from 33 Types of Cancer. Cell 2018, 173, 291–304.e6. [Google Scholar] [CrossRef] [Green Version]
- Rousseaux, S.; Debernardi, A.; Jacquiau, B.; Vitte, A.L.; Vesin, A.; Nagy-Mignotte, H.; Moro-Sibilot, D.; Brichon, P.Y.; Lantuejoul, S.; Hainaut, P.; et al. Ectopic activation of germline and placental genes identifies aggressive metastasis-prone lung cancers. Sci. Transl. Med. 2013, 5, 186ra66. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
MMPs increase expression in lung tumors and are associated with survival outcomes in the GSE31210 cohort; 226 lung adenocarcinoma patient samples and 20 normal lung samples from the GSE31210 stage I–II lung adenocarcinoma cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap of differentially expressed genes between tumor and normal lung tissue was performed. A 150-gene cluster with enriched MMPs was identified (square). (B) The MMPs, including MMP1, MMP3, MMP7, MMP9, MMP11, MMP12, and MMP13, increased expression in tumors compared to normal lung tissue. TIMP-1 increased expression in tumors, but TIMP-2 and TIMP-3 decreased expression in tumors compared to normal lung tissue. Data shown are mean ± S.D. **** p < 0.0001 and * p < 0.005 using Student’s t test. (C) Ingenuity pathway analysis of the 150-gene cluster showed significant pathways. (D) Unsupervised hierarchical clustering heatmap revealed four lung adenocarcinoma subgroups clustered with 150-gene cluster (E) Kaplan–Meier survival analysis of patient subgroups based on the 150-gene cluster was performed using the log-rank test.
Figure 1.
MMPs increase expression in lung tumors and are associated with survival outcomes in the GSE31210 cohort; 226 lung adenocarcinoma patient samples and 20 normal lung samples from the GSE31210 stage I–II lung adenocarcinoma cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap of differentially expressed genes between tumor and normal lung tissue was performed. A 150-gene cluster with enriched MMPs was identified (square). (B) The MMPs, including MMP1, MMP3, MMP7, MMP9, MMP11, MMP12, and MMP13, increased expression in tumors compared to normal lung tissue. TIMP-1 increased expression in tumors, but TIMP-2 and TIMP-3 decreased expression in tumors compared to normal lung tissue. Data shown are mean ± S.D. **** p < 0.0001 and * p < 0.005 using Student’s t test. (C) Ingenuity pathway analysis of the 150-gene cluster showed significant pathways. (D) Unsupervised hierarchical clustering heatmap revealed four lung adenocarcinoma subgroups clustered with 150-gene cluster (E) Kaplan–Meier survival analysis of patient subgroups based on the 150-gene cluster was performed using the log-rank test.
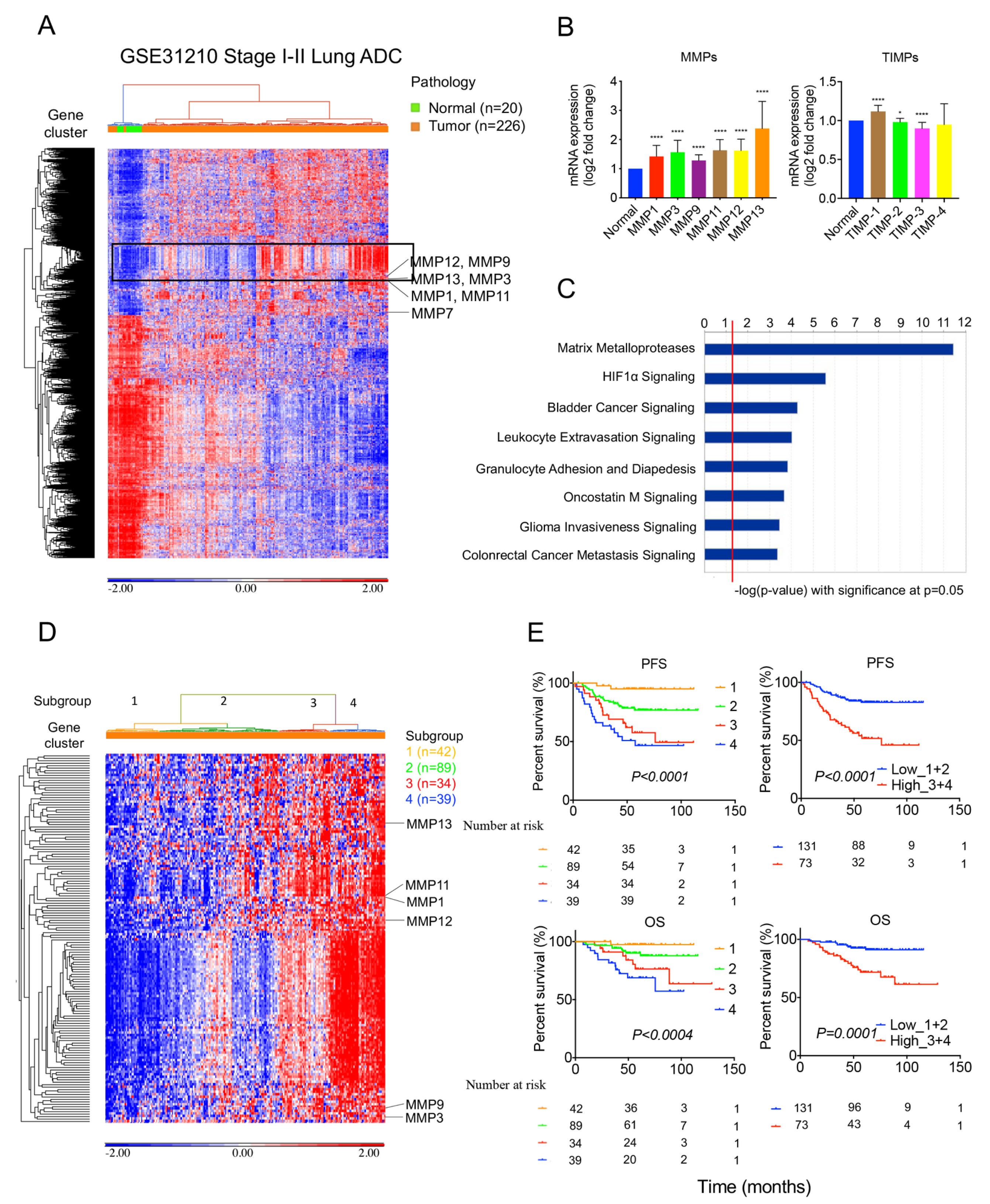
Figure 2.
MMPs increase expression in lung tumors and are associated with survival outcomes in the TCGA cohort; 517 lung adenocarcinoma patient samples and 59 normal adjacent lung samples from the TCGA lung adenocarcinoma cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap of differentially expressed genes between tumor and normal lung tissue was performed. A 185-gene cluster with enriched MMPs was identified (square). (B) The MMPs, including MMP1, MMP3, MMP9, MMP11, MMP12, and MMP13, increased expression in tumors more than normal lung tissue. TIMP-1 increased expression in tumors, but TIMP-2, TIM-3, and TIMP-4 decreased expression in tumors compared with normal lung tissue. Data shown are mean ± S.D. **** p < 0.0001 using Student’s t test. (C) Ingenuity pathway analysis of the 185-gene cluster showed significant pathways. (D) An unsupervised hierarchical clustering heatmap revealed four lung adenocarcinoma subgroups clustered with a 185-gene cluster. (E) Kaplan–Meier survival analysis of patient subgroups based on a 185-gene cluster was performed using the log-rank test.
Figure 2.
MMPs increase expression in lung tumors and are associated with survival outcomes in the TCGA cohort; 517 lung adenocarcinoma patient samples and 59 normal adjacent lung samples from the TCGA lung adenocarcinoma cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap of differentially expressed genes between tumor and normal lung tissue was performed. A 185-gene cluster with enriched MMPs was identified (square). (B) The MMPs, including MMP1, MMP3, MMP9, MMP11, MMP12, and MMP13, increased expression in tumors more than normal lung tissue. TIMP-1 increased expression in tumors, but TIMP-2, TIM-3, and TIMP-4 decreased expression in tumors compared with normal lung tissue. Data shown are mean ± S.D. **** p < 0.0001 using Student’s t test. (C) Ingenuity pathway analysis of the 185-gene cluster showed significant pathways. (D) An unsupervised hierarchical clustering heatmap revealed four lung adenocarcinoma subgroups clustered with a 185-gene cluster. (E) Kaplan–Meier survival analysis of patient subgroups based on a 185-gene cluster was performed using the log-rank test.
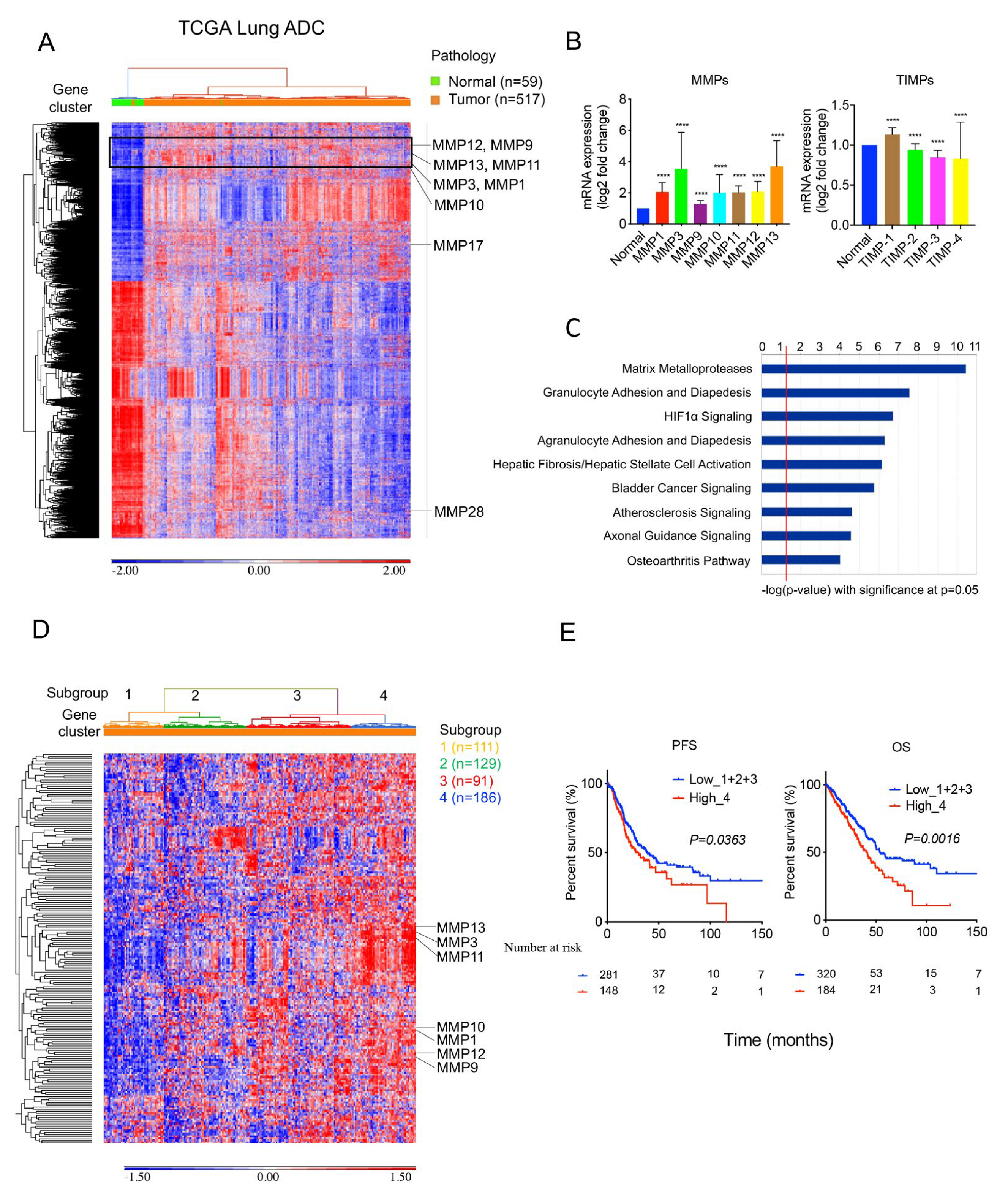
Figure 3.
Characteristics of a 36-gene MMP signature and network analysis: (A) Venn diagram showed 36 MMP-associated genes, which were shared between MMP-enriched gene clusters in GSE31210 and TCGA cohort. (B) Ingenuity pathway analysis of the 36-gene MMP signature showed significant pathways. (C) Networks analysis of the 150-gene cluster from the GSE31210 cohort. (D) Networks analysis of the 185-gene cluster from the TCGA cohort.
Figure 3.
Characteristics of a 36-gene MMP signature and network analysis: (A) Venn diagram showed 36 MMP-associated genes, which were shared between MMP-enriched gene clusters in GSE31210 and TCGA cohort. (B) Ingenuity pathway analysis of the 36-gene MMP signature showed significant pathways. (C) Networks analysis of the 150-gene cluster from the GSE31210 cohort. (D) Networks analysis of the 185-gene cluster from the TCGA cohort.
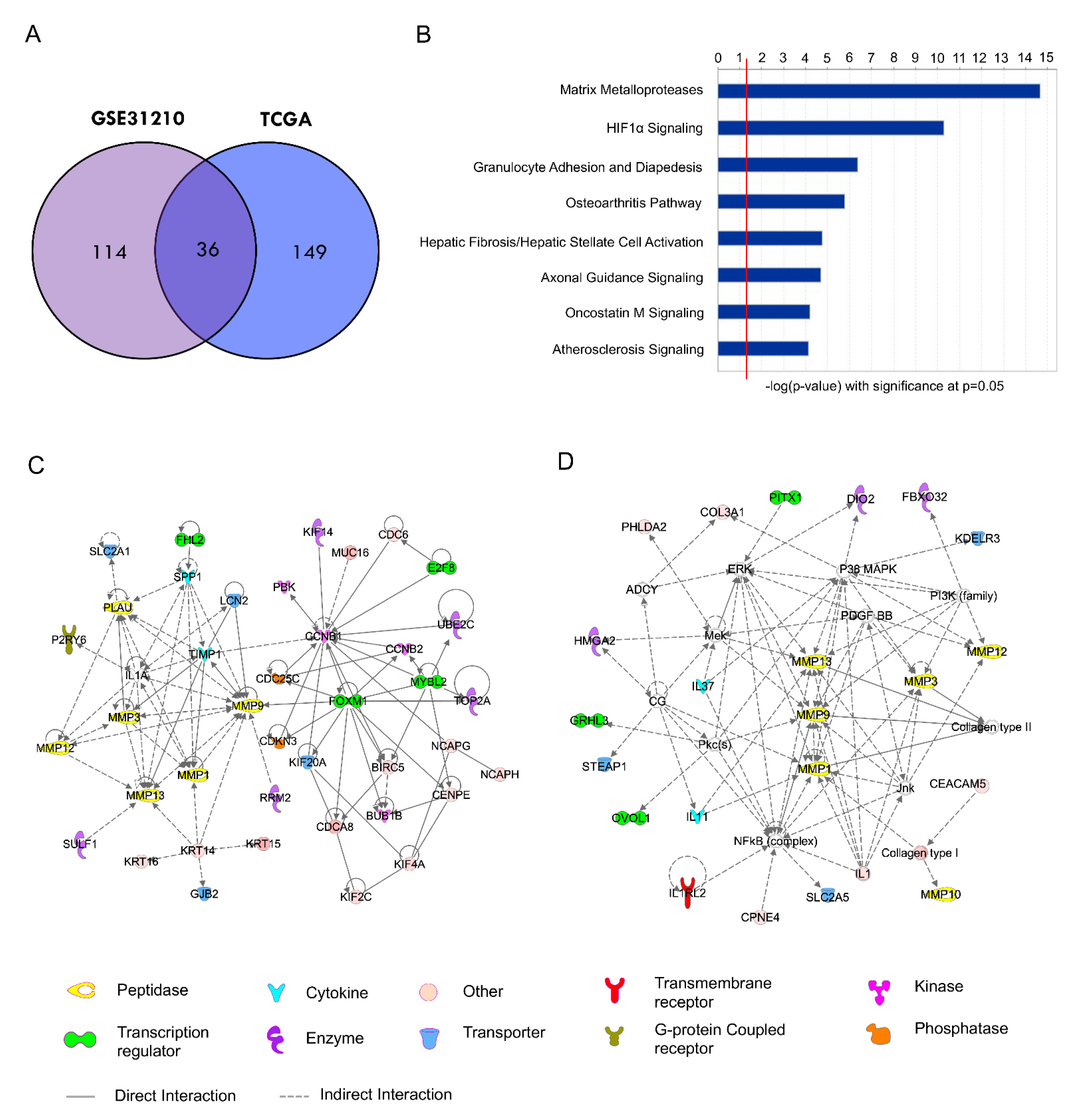
Figure 4.
High MMP gene signature expression predicts poor survival outcomes in stage I lung adenocarcinoma from the GSE31210 cohort; 168 stage I lung adenocarcinoma patient samples from the GSE31210 cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap revealed three lung adenocarcinoma subgroups clustered with the 36-gene MMP signature. (B) Kaplan–Meier survival analysis of patient subgroups based on the 36-gene MMP signature was performed using the log-rank test. (C) The distribution difference among the three subgroups stratified by gene mutation, gender, and smoking status was tested by the Chi-squared test. (D) GSEA showed the enrichment of 36-gene MMP signature based on mutation status in the GSE31210 cohort.
Figure 4.
High MMP gene signature expression predicts poor survival outcomes in stage I lung adenocarcinoma from the GSE31210 cohort; 168 stage I lung adenocarcinoma patient samples from the GSE31210 cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap revealed three lung adenocarcinoma subgroups clustered with the 36-gene MMP signature. (B) Kaplan–Meier survival analysis of patient subgroups based on the 36-gene MMP signature was performed using the log-rank test. (C) The distribution difference among the three subgroups stratified by gene mutation, gender, and smoking status was tested by the Chi-squared test. (D) GSEA showed the enrichment of 36-gene MMP signature based on mutation status in the GSE31210 cohort.
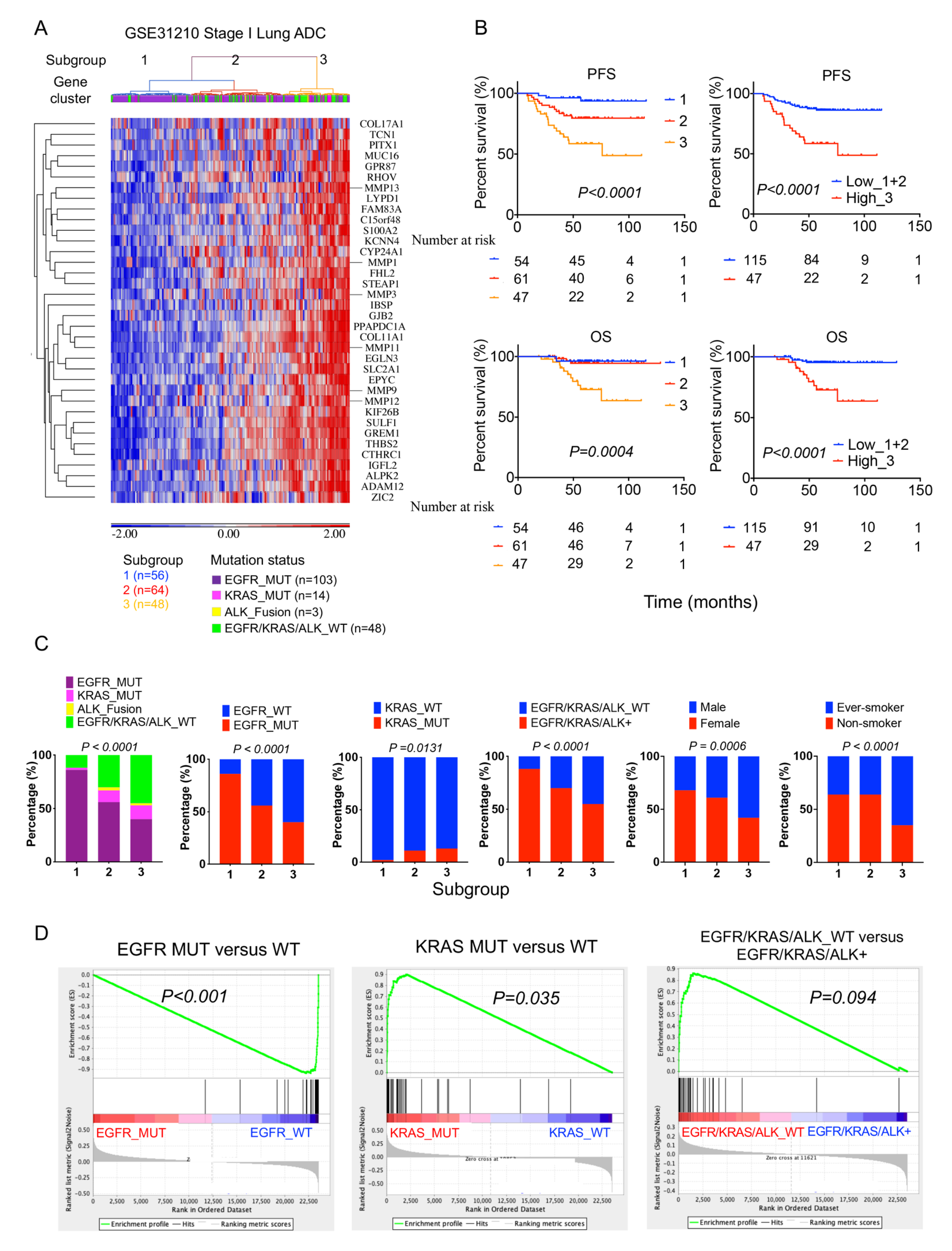
Figure 5.
High MMP gene signature expression predicts poor survival outcomes in stage I lung adenocarcinoma from the TCGA cohort; 277 stage I lung adenocarcinoma patient samples from the TCGA cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap revealed four lung adenocarcinoma subgroups clustered with 36-gene MMP signature. (B) Kaplan–Meier survival analysis of patient subgroups based on the 36-gene MMP signature performed using the log-rank test. (C) The distribution difference among the four subgroups stratified by gene mutation, gender, and smoking status was tested by the Chi-squared test.
Figure 5.
High MMP gene signature expression predicts poor survival outcomes in stage I lung adenocarcinoma from the TCGA cohort; 277 stage I lung adenocarcinoma patient samples from the TCGA cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap revealed four lung adenocarcinoma subgroups clustered with 36-gene MMP signature. (B) Kaplan–Meier survival analysis of patient subgroups based on the 36-gene MMP signature performed using the log-rank test. (C) The distribution difference among the four subgroups stratified by gene mutation, gender, and smoking status was tested by the Chi-squared test.
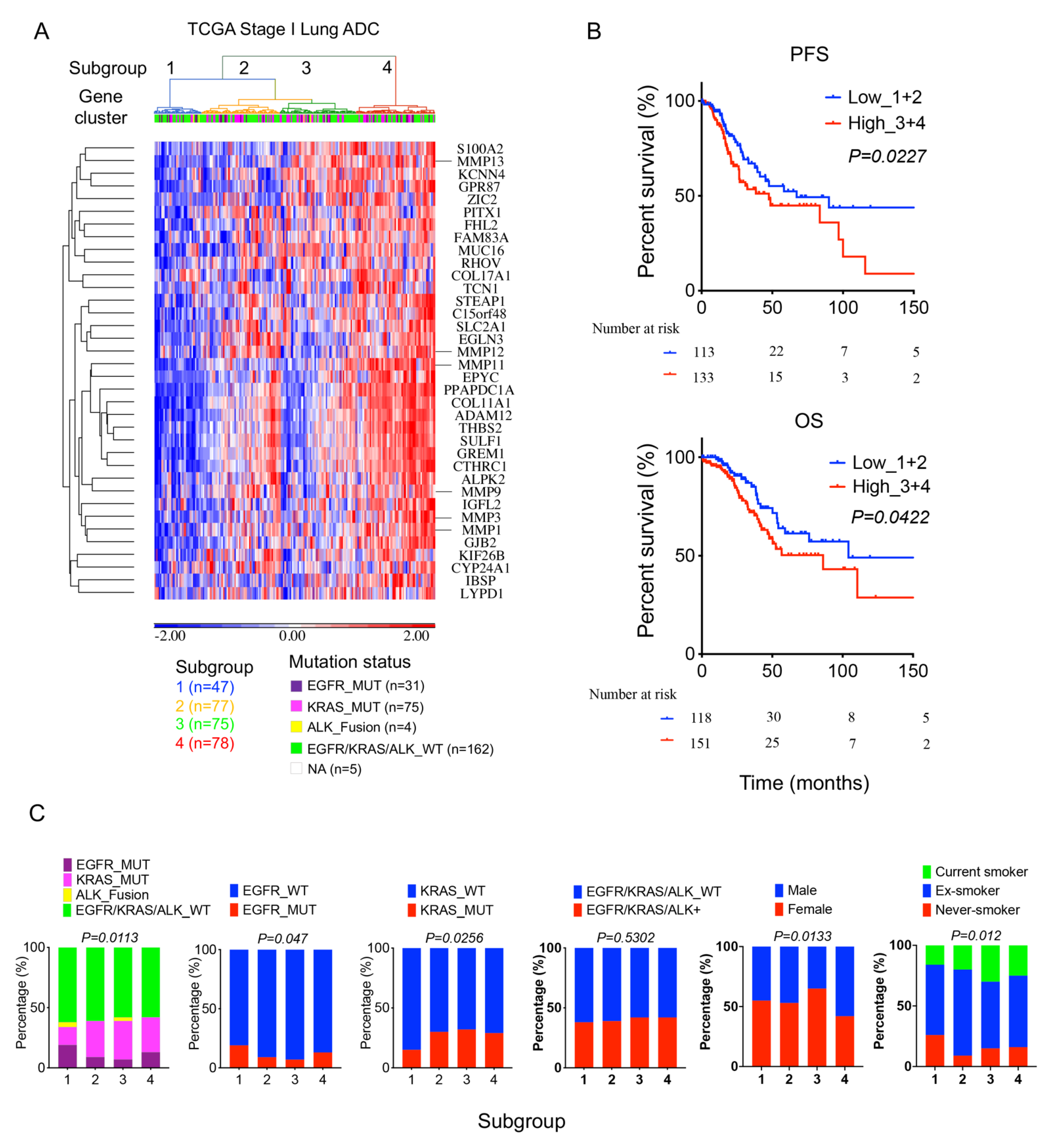
Figure 6.
Validation of the 36-gene MMP signature in an independent GSE30219 lung cancer cohort; 70 stage I lung adenocarcinoma patient samples from the GSE30219 cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap revealed two lung adenocarcinoma subgroups clustered with 36-gene MMP signature. (B) Kaplan–Meier survival analysis of patient subgroups based on the 36-gene MMP signature was performed using the log-rank test.
Figure 6.
Validation of the 36-gene MMP signature in an independent GSE30219 lung cancer cohort; 70 stage I lung adenocarcinoma patient samples from the GSE30219 cohort were analyzed: (A) An unsupervised hierarchical clustering heatmap revealed two lung adenocarcinoma subgroups clustered with 36-gene MMP signature. (B) Kaplan–Meier survival analysis of patient subgroups based on the 36-gene MMP signature was performed using the log-rank test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Liu, C.-H.; Di, Y.P. Matrix Metallopeptidase-Gene Signature Predicts Stage I Lung Adenocarcinoma Survival Outcomes. Int. J. Mol. Sci. 2023, 24, 2382. https://doi.org/10.3390/ijms24032382
AMA Style
Liu C-H, Di YP. Matrix Metallopeptidase-Gene Signature Predicts Stage I Lung Adenocarcinoma Survival Outcomes. International Journal of Molecular Sciences. 2023; 24(3):2382. https://doi.org/10.3390/ijms24032382
Chicago/Turabian StyleLiu, Chia-Hsin, and Yuanpu Peter Di. 2023. "Matrix Metallopeptidase-Gene Signature Predicts Stage I Lung Adenocarcinoma Survival Outcomes" International Journal of Molecular Sciences 24, no. 3: 2382. https://doi.org/10.3390/ijms24032382
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.