
C-Reactive Protein as a Biomarker for Major Depressive Disorder?



Unit of Clinical Psychiatry, Department of Neurosciences/DIMSC, Polytechnic University of Marche, 60126 Ancona, Italy
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2022, 23(3), 1616; https://doi.org/10.3390/ijms23031616
Submission received: 31 December 2021
/
Revised: 25 January 2022
/
Accepted: 28 January 2022
/
Published: 30 January 2022
(This article belongs to the Special Issue Pathogenesis and Treatment Mechanisms of Depression)
Abstract
:The etiopathogenesis of depression is not entirely understood. Several studies have investigated the role of inflammation in major depressive disorder. The present work aims to review the literature on the association between C-Reactive Protein (CRP) and depression. A systematic review was performed for the topics of ‘CRP’ and ‘depression’ using the PubMed database from inception to December 2021. Fifty-six studies were identified and included in the review. Evidence suggested the presence of dysregulation in the inflammation system in individuals with depression. In most studies, higher blood CRP levels were associated with greater symptom severity, a specific pattern of depressive symptoms, and a worse response to treatment. Moreover, about one-third of depressed patients showed a low-grade inflammatory state, suggesting the presence of a different major depressive disorder (MDD) subgroup with a distinct etiopathogenesis, clinical course, treatment response, and prognosis, which could benefit from monitoring of CRP levels and might potentially respond to anti-inflammatory treatments. This work provides robust evidence about the potential role of CRP and its blood levels in depressive disorders. These findings can be relevant to developing new therapeutic strategies and better understanding if CRP may be considered a valuable biomarker for depression.
1. Introduction
Depression is the most common mental illness affecting around 10–20% of the general population [1]. In 2008, the World Health Organization (WHO) ranked depression as the third cause of burden of disease worldwide and projected that it will rank first by 2030 [2]. Depression also represents the major contributor to suicide deaths, with an incidence of up to 800.000 per year worldwide [3]. It usually manifests in early adulthood, with a mean age onset of approximately 20–25 years [4]. Depression usually occurs 2-fold higher among women than men at all age groups, and several socio-demographic risk factors are implicated in this trend [5,6]. However, the etiopathogenesis of depression is highly complex and not entirely understood. One of the most widely renowned hypotheses is based on the monoaminergic theory [7], although recent researches focused on other pathways, such as the dysregulation of hypothalamus-pituitary-adrenal axis (HPA), genetic susceptibility, and epigenetic modifications, the oxidative stress-induced damage, and the neurodevelopment theory [8,9,10,11,12].
Furthermore, recent evidence suggested a possible role of immune dysregulation in the etiopathogenesis of depression [13,14,15,16]. Accordingly, it has been well documented that individual affected with autoimmune disorders (e.g., rheumatoid arthritis, psoriasis, diabetes mellitus, chronic inflammatory bowel disease, and autoimmune thyroiditis) are more likely to display comorbid depressive symptomatology [17,18,19,20,21,22,23]. Likewise, depression is often associated with other conditions where an increased inflammatory state has been documented, such as in cardiovascular diseases, obesity, smoking status, and specific nutritional deficits [24,25,26]. Furthermore, there is strong evidence that the activation of the innate immune system may lead to “sickness behaviors” characterized by depression-like symptomatology, including anhedonia, weight and appetite loss, memory impairment, as well as cognitive and social dysfunction [27,28].
Furthermore, several studies investigated the role of a set of specific inflammatory biomarkers in depressive disorders, including C-Reactive Protein (CRP) [15,16,29]. CRP is a pentameric acute phase reactant protein secreted mainly by hepatocytes in response to the activation of the innate humoral system [30]. It is easily measured through a blood sample also in its high-sensitivity form (hs-CRP) [31] and used in clinical practice mainly as a biomarker of infection, chronic disease state, and chronic low-grade inflammation [30,32]. CRP usually does not freely cross BBB [33], even though several mechanisms have been hypothesized to explain how CRP can interact with the Central Nervous System (CNS) [33,34]. For instance, it has been suggested that an increase of the blood-brain barrier (BBB) permeability could be determined by severe stress and/or traumatic brain injury [35,36]. Furthermore, neurovascular damage induced by the peripheral myeloid cells, pro-inflammatory cytokines, and the dysregulation of the complement pathways could be a further potential mechanism of action [36,37,38]. In addition, CRP appears to determine BBB disruption, through the binding with some ligands (i.e., Fc gamma receptors, CD16, CD32), expressed in the microglia, astrocytes, and endothelial cells [39]. Moreover, increased levels of CRP and its proinflammatory activity can drive CNS inflammation through microglia and astrocytes activation [40,41,42].
Therefore, the present review aims at systematically investigating the role of CRP in depressive disorders, including Major Depressive Disorder (MDD) and Treatment-Resistant Depression (TRD) in order to better clinically characterize depressed patients, also taking into account the neuroinflammatory state. A secondary aim is evaluating whether CRP may represent a useful biomarker in clinical practice, able to early identify and characterize those depressed patients according to their different illness stages, severity and/or treatment resistance. Moreover, a third aim is at evaluating whether a low- and/or medium neuroinflammatory state may predict different treatment responses and, hence, address clinicians towards a tailored treatment.
2. Material and Methods
2.1. Search Sources and Strategies
This systematic review was performed according to the guidelines recommended by Cochrane Collaboration [43] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [44]. Literature searches were conducted by using PubMed database, from its inception to 10 December 2021, using the following keywords: ((((“C-reactive protein” [Title/Abstract]) OR (CRP [Title/Abstract])) OR (“hs-CRP” [Title/Abstract])) OR (hsCRP [Title/Abstract])) AND (depressi * [Title/Abstract]).
2.2. Study Selection
All studies evaluating the relationship between CRP and depression/depressive disorders/MDD/TRD, based only on human participants and published in English, were screened. Firstly, all papers were screened according to their titles and abstracts and full tests of relevant studies were obtained. Narrative reviews, systematic reviews, meta-analyses, letters to the editor, book chapters, case-reports, case-series, and duplicates were excluded. The following inclusion criteria were considered to be included in the present review: (a) studies investigating CRP levels in depressive/MDD/TRD patients; (b) studies assessing the depressive symptomatology through validated semi-structured clinical interviews and/or rating scales. Exclusion criteria include: (a) studies investigating other inflammatory proteins (e.g., interleukins, fibrinogen), hormones (e.g., cortisol, thyroxine) or other types of biomarkers, even though on sample constituted by depressed/MDD/TRD patients; (b) studies in which depression is comorbid with other organic pathologies (e.g., cancer, rheumatoid arthritis, diabetes mellitus) and/or psychiatric disorders (e.g., schizophrenia, bipolar disorder); (c) in vitro or animal studies.
2.3. Data Extraction and Management
Independently, two authors (S.P. and S.T.V.) read all included full-text papers, by using the abovementioned inclusion and exclusion criteria. All relevant screened papers to be included were collected and data were extracted in a dedicated excel spreadsheet. The disagreement was resolved by discussion and consensus with a third member of the team (L.O.).
2.4. Characteristics of Included Studies
2.5. Quality Assessment
SP and STV independently assessed the quality of included studies using the modified versions of the Newcastle-Ottawa Quality Assessment Scale, adopted for cross-sectional (Table 2), case-control (Table 3), cohort studies (Table 4) and RCT (Table 5) [99]. The scale investigated the selection, comparability, and the main outcomes of the studies. A score of 7 or above is considered for a good quality; a score of 5–6 indicate a satisfactory quality level and scores less than 5 usually indicate unsatisfactory studies (Supplementary Material: PRISMA_2020_checklist). Eventually, disagreement was resolved by L.O.
3. Results
3.1. Studies on the Association between CRP Levels and Depression
3.1.1. Cross-Sectional Studies
A cross-sectional population-based study evaluated the association between depression and CRP in 6126 adults, assessed with the Center for Epidemiologic Studies Depression (CESD) scale [70]. Subjects with depressive symptoms (CESD ≥ 16) displayed on average a CRP concentration of 0.43 mg/L (95% CI = 0.16–0.72) higher than the healthy controls. In addition, the authors found that this association appeared to persist, also when the sample size was limited only to depressed patients without any chronic disease. A large population-based cross-sectional study recruited 5447 Korean people aged > 20 years, from the Korean National Health and Nutrition Examination Survey (KNHANES VII-1), to assess the association between hs-CRP and depression [61]. High hs-CRP levels were defined as ≥ 3.0 mg/L and depression evaluated through the Patient Health Questionnaire-9 (PHQ-9). Individuals with high CRP levels had a significantly higher rate of depression compared to the others. In addition, hs-CRP levels were independently associated with PHQ-9 scores, even after adjustment of confounders. Furthermore, the authors found that this association appeared to be more prominent in younger adults than in older patients [61]. Using the abovementioned nationwide cross-sectional survey (i.e., KNHANES), Cho et al. (2021) [52] confirmed in a sample of 10,702 adults, that individuals with high hs-CRP levels (>3.0 mg/L) were more likely to have depressive symptomatology and suicidal ideation compared to those participants with low hs-CRP concentrations. In the subgroups analysis, the association was more prominent in the non-geriatric subsample (i.e., ≤64 years), in males, in obese adults, and in those who did not report regular aerobic physical activity.
A US-population-based study coming from the National Health and Nutrition Examination Survey (NHANES), recruited 16 patients with atypical MDD, 93 with nonatypical MDD and 1682 healthy individuals, to measure CRP levels [58]. Subjects with atypical MDD exhibited higher CRP levels than those subjects without MDD (mean difference = 1.56 mg/L) or nonatypical MDD (mean difference = 1.40 mg/L) control, even after adjusting for confounders, anxiety disorders, BMI, and smoking [47]. A recent retrospective, observational, cross-sectional study evaluated the differences between elevated CRP levels (i.e., CRP > 3 mg/L and ≤ 10 mg/L) in subjects with MDD, bipolar disorder (BD), and obsessive-compulsive disorder (OCD) [47]. The authors recruited 388 patients (156 MDD, 135 BD and 97 OCD). The results suggested that elevated CRP levels might be a transdiagnostic biomarker in different psychiatric disorders, although multiple confounders might explain the presence of elevated CRP levels in a substantial portion of psychiatric patients [47]. Huang and Lin (2007) [59] reported higher hs-CRP levels in both MDD (n = 23) and BD-I (n = 13) groups compared to healthy controls (n = 31). No significant associations were found between CRP levels and MDD, even after adjusting for covariates; while a significant association was found between CRP levels and BD-I, even after adjusting for covariates (p = 0.043). A cross-sectional study aimed at investigating differences between CRP levels in patients with acute schizophrenia (n = 458), unipolar depression (n = 319), BD (n = 146), BD depression (n = 114) and BD mania (n = 32), did not find significant differences between groups [74]. However, more than one-third (38.6%) of the unipolar depression patients displayed high CRP levels (i.e., >3 mg/L) [74]. A cross-sectional study recruiting 1535 adolescents aged 13–16 years from a province-wide youth survey, did not find any association between CRP levels and depressive symptoms [49]. Chang et al. (2012) [50] evaluated whether CRP levels were associated with depressive symptoms and cognitive impairment in MDD patients. The authors found that among 149 recruited subjects, there was no association between CRP levels and HAM-D scores in the medication-free MDD subgroup.
A large cross-sectional study conducted by Menezes et al., 2017, including 14,821 Brazilian participants of the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil), investigated the possible association between CRP levels and depression [68]. Current depression was assessed by Clinical Interview Schedule-Revised (CIS-R) and participants were divided into three groups: (a) negative at CIS-R and not using antidepressant; (b) negative at CIS-R but using antidepressants; (c) positive at CIS-R. No association between serum CRP levels, current depression, and use of antidepressants was found [68]. Another cross-sectional study, including 9459 Chinese middle-aged and elderly participants of the China Health and Retirement Longitudinal Study, did not find any correlation between CRP levels and depressive symptoms after adjusting for confounders [76]. A recent large cross-sectional study assessing serum hs-CRP levels and depression symptoms using CESD, in 26,638 healthy adults, recruited at the Cooper Clinic in Dallas, Texas, reported an association between hs-CRP levels and depression which could be more likely explained by obesity status [62]. An observational study investigated the association between CRP levels and depression also considering shared genetic and environmental factors [75]. Data were collected from 2577 twins and 899 singletons in Colombo, Sri Lanka. Depression was assessed using the revised Beck Depression Inventory (BDI-II) and the heritability of CRP levels was evaluated through Structural Equation Modelling. No association between CRP levels and depression was found. Moreover, in males the variance in CRP levels was explained by shared environment and non-shared environment, while in females it was explained by genetic and non-shared environment [75].
3.1.2. Case-Control Studies
A recent case-control study compared 84 depressed patients, by classifying them in two groups, i.e., those with inflammation (CRP levels ≥ 3 mg/L) and those without inflammation [80]. The authors found, after adjusting for potential confounders, that the low-grade inflammatory group showed higher depression severity, somatic symptoms, state anxiety, and fatigue, but not anhedonia, compared to the group with inflammation. They also reported a poorer quality of life and an increase in guilty feelings, pessimism, concentration difficulties, and indecision [80].
A study recruiting 26,894 participants with a lifetime diagnosis of MDD, evaluated using the Composite International Diagnostic Interview (CIDI), were compared with 59,000 healthy control subjects regarding CRP levels [83]. CRP levels were significantly higher in patients with depression than in the control group (2.4 mg/L compared with 2.1 mg/L, p < 0.001). Furthermore, MDD patients showed more frequently a low-grade inflammation state (i.e., CRP > 3 mg/L) than control subjects (21.1% compared with 16.8%, respectively) [83].
A case-control study comparing 25 patients aged ≥55 years at their first depressive episode, assessed through Hamilton Depression Rating Scale (HAMD), and 27 age-matched healthy controls, found that subjects with current depressive disorders showed 40-fold higher CRP levels compared to control group [81]. The authors suggested that the late-onset depression was associated with higher CRP levels. Moreover, CRP levels were strongly and positively associated with depression severity [81]
Another study proposed CRP as a biomarker to differentiate MDD and BD type 2 (BD-II), by recruiting 88 BD-II, 72 drug-naïve MDD and 96 healthy controls [79]. The authors found that a baseline CRP level of 621.6 ng/mL could discriminate between MDD and BD-II in both depressed and euthymic states [79].
A case control study investigating the differences in serum CRP levels between elderly (≥60 years) depressed patients and healthy elderly individuals (202 with unipolar depression and 202 healthy subjects), found no significant differences between CRP levels in the two groups [86]. In addition, the authors reported that CRP levels were not associated with age and about 30% of the sample showed CRP level > 3 mg/L [86].
3.1.3. Cohort Studies
A prospective cohort study investigated the relationship between long-term patterns of systemic inflammation and late-life depression symptomatology using the Atherosclerosis Risk in Communities (ARIC) Study, a large community-based prospective cohort study [94]. The study measured CRP levels and depressive symptoms (by using CESD) in 4476 participants over a 21-year period spanning from middle-to-late-life, at three moments (at the current moment, 14 years before, and 21 years before the current visit). Individuals with stable elevated CRP levels (>3 mg/L at all three visits) showed greater depressive symptomatology at older ages, after adjusting for covariates. Moreover, stable elevated CRP levels were associated with an increased risk for late-life depressive symptomatology [94].
A UK general population-based birth cohort study, named the Avon Longitudinal Study of Parents and Children (ALSPAC), evaluating CRP levels in 1561 participants, identified population sub-groups of young people characterized by different longitudinal patterns of CRP levels. Subjects who displayed a pattern of increasing CRP levels from childhood to early adulthood had a higher risk of moderate/severe depression at 18 years, compared to those who had persistently low CRP levels [29]. Subjects who displayed persistently elevated CRP levels also had increased ORs of moderate/severe depression at 18 years, even though this association was not statistically significant. Overall, an increase in low-grade inflammatory levels from childhood to early adulthood is strongly associated with the risk of developing depression in early adulthood [29].
A cohort study selected 1508 young individuals who were evaluated regarding the incidence of low-grade inflammation (i.e., CRP < 3 mg/L at baseline) and the depressive state using the Beck Depression Inventory (BDI) [100]. The authors found that the incidence of low-grade inflammation was more frequent in patients with depressive symptoms than among healthy controls (OR = 2.05; 95% CI = 1.31–3.21, p < 0.001). After adjusting for age, sex, metabolic syndrome, BMI, levels of physical activity, smoking, presence of hepatic steatosis, and waist circumference, it was confirmed the association of depressive symptoms and low-grade inflammation. New cases of inflammation were associated with depressive symptoms (OR = 1.76; 95% CI = 1.03–3.02, p = 0.04) [100].
Findings coming from the Great Smoky Mountains Study, a prospective cohort study investigating CRP levels in a cohort of 1334 adolescents and young adults, did not find any association between CRP levels and later depression status [89]. Multiple depressive episodes appeared to predict later CRP levels [89].
In 3397 older adults, an examination based on the English Longitudinal Study of Ageing studied the directional associations between CRP levels and depressive symptomatology [88]. Baseline high CRP levels were associated with depression symptoms severity. Baseline elevated depressive symptomatology was not associated with subsequent high CRP levels [88].
3.2. Studies on Gender Differences of CRP Levels in Depression
3.2.1. Cross-Sectional Studies
A cross-sectional study assessed 6005 Finns aged >30 years for depression, using BDI and CIDI, and for CRP levels [54]. Higher BDI-21 scores were associated with higher CRP levels only in men (p < 0.001), even after adjustment for confounders [54]. Moreover, in men the more recent dysthymic disorder or at least moderate depressive episode was associated with higher CRP levels, compared to females (p = 0.006) [54]. Another cross-sectional study, based on the KNHANES, aimed at investigating the sex difference in the association between hs-CRP levels and depression, recruited 5483 Korean adults (2373 men and 3110 women) assessed with PHQ-9 (cut-off for depression > 10) [64]. Men with high hs-CRP levels (>3.0 mg/L) reported a higher prevalence of depression than those with lower levels (p < 0.0001). No statistically significant association was observed between hs-CRP levels and depression among women [64]. Similar findings were found in another Korean cross-sectional study, in which 596 participants (224 men and 345 women) from the Korean Social life, Health and Aging Project Health Examination (KSHAP-HE) cohort, were assessed for depressive symptoms through the CES-D and for serum CRP levels [71]. The authors reported that elevated CRP levels were independently associated with depressive symptoms in elderly Koreans, but this association was observed only in men both before and after adjusting for covariates [71].
Ford and Erlinger (2004) [55] found in 6914 participants (3154 men and 3760 women), recruited from the NHANES survey, that a history of MDD was associated with elevated CRP levels and that this association was much stronger among men than women. Moreover, CRP levels were higher among men who had a recent episode of depression and who had recurrent depression. A cross-sectional study evaluated whether there was a gender difference in the association between depressive episodes and hs-CRP [66]. From the genetically homogeneous Northern Finland 1966 Birth Cohort, 5269 participants (2641 male and 2828 female) were assessed with the Hopkins Symptom Checklist-25 (HSCL-25) and were measured CRP levels, by reporting that elevated CRP levels in males might increase the probability for severe current and recurrent depressive episodes. This association was not found in women [66]. Another cross-sectional study, including 764 (336 male and 579 female) individuals assessed through the Short Zung Self Rating Depression Scale (SZRDS), showed a positive correlation between hs-CRP levels and depression mood, exclusively in men [67].
A population-based study investigating the role of gender in the association between CRP levels and depressive severity, recruited 231 individuals (142 female and 89 men) with MDD from the Genome-Based Therapeutics Drugs Depression (GENDEP) study [63]. The subjects were assessed for hs-CRP levels and depression using the Montgomery Åsberg Depression Rating Scale (MADRS). Findings showed that higher CRP levels were significantly associated with greater overall depressive symptoms severity, which was significant among women but not in men. Moreover, women with higher CRP levels had an increase in specific depressive symptoms severity such as observed mood, cognitive symptoms, interest-activity, and suicidality [63]. A cross-sectional study included 563 adolescent girls, aged 12–18 years, aimed at investigating the association between hs-CRP levels and depressive symptomatology assessed through BDI-II [72]. Serum hs-CRP levels were 0.61 (0.30–0.88) mg/L in the non-depressed group, 0.97 (0.50–1.82) mg/L in the group with a mild depression score, 1.04 (0.57–1.60) mg/L in those with a moderate depression score, and 0.84 (0.45–2.64) mg/L in girls with severe depression (p < 0.001). Multinomial logistic regression analysis, controlling for covariates, showed that depression scores were positively associated with serum hs-CRP levels (p < 0.001) [72].
3.2.2. Cohort Studies
A longitudinal study aimed at examining the association between depression and hs-CRP levels, found a positive association between BDI scores and serum hs-CRP levels only in women [90].
A 2010 longitudinal study investigated the association between depressive symptoms and CRP levels in 3302 mid-life women [92]. The assessment included CESD and blood CRP levels at the baseline and after 7 years. Results showed that higher CESD scores predicted higher CRP levels and vice versa over a 7-year period [92].
A retrospective cohort study evaluating the association between CRP levels and increased risk of de novo MDD, recruiting 1494 women randomly selected and assessed through the Structured Clinical Interview for DS-IV-TR Research Version, Non-Patient edition (SCID-I/NP), reported a hazard ratio for depression increased by 44% for each standard deviation increase in log-transformed hs-CRP, indicating that serum hs-CRP was an independent risk factor for de novo MDD in women [93].
3.2.3. RCT Studies
A recent RCT evaluated the sex differences in the association between CRP levels and the response to antidepressant treatments [97]. Participants were assessed with HAMD-17 at baseline and at weeks 1, 2, 3, 4, 6, and 8 after the treatment. Elevated baseline CRP levels were associated with the worst antidepressant treatment outcome only in female samples [97].
3.3. Studies on Ethnic Differences of CRP Levels in Depression
Cross-Sectional Studies
A cross-sectional study evaluated the association between social integration, race/ethnicity, inflammation, and depressive symptoms in US participants through the NHANES survey [51]. Participants were administered PHQ-8 and measured hs-CRP levels. Social integration and CRP levels were found to operate independently in their association with depressive symptoms only for the white population but not the black or the Hispanic one [51]. A cross-sectional study evaluated whether specific symptom clusters were associated with CRP levels and whether race/ethnicity affected this association in a sample of 10,149 U.S. individuals from the NHANES survey [48]. Depressive symptomatology was assessed by PHQ-9, and serum hs-CRP was quantified. Somatic symptoms were related to CRP levels (p < 0.001), only in non-Hispanic white individuals [48].
3.4. Studies on Severity/Specific Cluster Domains in the Association between CRP Levels and Depression
3.4.1. Cross-Sectional Studies
A study involving 5909 patients aimed at investigating the possible association between inflammation and specific depressive symptoms, found that CRP levels were associated with symptoms of fatigue (p < 0.001), restless sleep (p = 0.03), low energy (p = 0.02) and feeling depressed (p = 0.04) [73]. These associations were absent in patients under antidepressant medication [73].
Case and Stewart [48] evaluated if specific symptom clusters were associated with CRP levels, by recruiting a sample of 10,149 U.S. individuals from the NHANES survey. Depressive symptoms were assessed by PHQ-9, and serum hs-CRP was quantified. Somatic symptoms were related to CRP levels (p < 0.001) [48]. A recent network analysis investigated the association between inflammation and a specific depression phenotype [69]. PHQ-9 was administered to a sample of 4157 adults from the NHANES while hs-CRP levels were measured to identify possible inflammatory phenotypes of depression [69]. The elevated CRP group (>3 mg/L) showed greater symptom connectivity, concentration, psychomotor difficulties, and treatment-resistant depression [69].
A cross-sectional study evaluated the association between CRP levels, depressive symptoms, and cognitive impairment in 149 MDD patients treated with antidepressants for six weeks [50]. Scale for Depression (HAM-D), Continuous Performance Test (CPT), Finger-Tapping Test (FTT), and Wisconsin Card-Sorting Test (WCST) were administered to the sample. Baseline CRP levels were negatively and significantly associated with performance in the FTT and WCST after six weeks of treatment (respectively, p = 0.006 and p = 0.021), reporting a significant association between CRP levels and the domains of attention and executive cognitive function. After six weeks of treatment, patients with higher baseline CRP levels still exhibited poor psychomotor speed and poor executive functioning [50].
A cross-sectional study recruiting 43,896 adults examined the association between CRP levels and depression in terms of executive functioning [56]. MINI and Ruff Figural Fluency Test (RFFT) were administered to the sample. The study reported that depression and higher CRP levels were both associated with worse executive functioning, even after covariates adjustment. Moreover, depressed subjects with higher levels of CRP showed poorer executive functioning than the control individuals [56].
3.4.2. Cohort Studies
A prospective cohort study investigated whether depression and apathy in the elderly subjects could be associated with CRP levels [91]. The study was conducted on 599 subjects assessed annually from age 85 to 90 through Mini-Mental State Examination (MMSE) and the Geriatric Depression Scale 15-items (GDS-15). Higher baseline CRP levels were associated with severe depressive symptoms but not apathy [91].
3.5. Studies on Genetic Correlation and Single-Nucleotide Polymorphisms (SNPs) in the Association between CRP Levels and Depression
3.5.1. Cross-Sectional Studies
A cross-sectional study explored whether CRP levels may covary with depressive symptoms due to allelic variation in the CRP gene [57]. The study recruited 868 healthy community volunteers who were assessed through CESD, plasma CRP levels and genome CRP SNPs. No direct association between CESD and CRP levels was found. One haplotype (T-G-C) was associated with CRP level (p = 0.014), but no one was related to depressive symptoms. Plasma CRP levels were predicted by the interaction of the A-G-T haplotype with depressive symptomatology (p = 0.009). Higher CESD scores were associated positively with CRP levels among individuals with the A-G-T haplotype (p = 0.004) [57].
A cross-sectional study exploring whether CRP SNPs were related to depressive symptoms and antidepressants efficacy assessed 440 patients with first-episode depression through HAMD-17, finding gender-specific SNP differences [65]. In particular, male patients with SNP rs1800947G exhibited lower insomnia scores while rs2794521CC showed lower scores of anxiety/physical symptoms, total HAMD-17 score; female patients with rs2794521TT had higher scores of insomnia and lower antidepressants efficacy [65]. A large cross-sectional study included 3700 men ≥ 70 years in determining if polymorphisms of SNPs rs1130864 and rs1205 were associated with MDD [45]. GDS-15 and genome CRP SNPs evaluations were used. The odds of depression increased by 2% (95% CI = 1–4%) for every unit (mg/L) increase of CRP and nearly doubled for men with CRP ≥ 3 mg/L vs. < 1 mg/L. Nevertheless, the association between high CRP (i.e., ≥3 mg/L) and depression was no longer significant after the analyses were adjusted for confounders. Men with the CT and TT genotypes of rs1130864 had greater odds of CRP ≥ 3 mg/L than CC carriers, but there was no association between this polymorphism and the presence of prevalent depression. The G > A polymorphism of SNP rs1205 was associated with a 24% lower CRP concentration than other genotypes. Men with the rs1205 AA genotype had greater odds of having clinically significant depression than participants with the GA and GG genotypes [45]. Similarly, a cross-sectional study studied the association between variants in the CRP gene that influence protein levels and depression in 990 people aged ≥65 years whose psychopathology was assessed through MINI and CESD [46]. The minor alleles of rs1130864 and rs1417938 were associated with a decreased risk of depression in women (p = 0.002). Conversely, rs1205 was found to be nominally associated with both an increased risk of depression and lower circulating CRP levels in women [46].
3.5.2. Case-Control Studies
A case-control study investigated whether inherited CRP allelic variations could covary depressive symptoms, in 200 patients, aged 18–65, who were assessed for CRP blood levels and genome CRP SNPs [87]. Patients with a positive family depression history had higher CRP blood levels. Specific inherited CRP SNPs (A allele in rs1417938 and C allele in rs1205) may be responsible for up-regulating serum CRP levels and thus bated with depression occurrence [87]. Another case-control study investigated whether CRP SNPs could regulate plasma CRP levels if inherited CRP allelic variations may covary with depressive symptoms [85]. CRP blood levels and genome CRP SNPs were evaluated in 60 MDD patients with family depression history and 60 healthy control volunteers. A significantly higher circulating CRP level was found in the first group [85].
3.6. Studies Investigating the Association between CRP Levels and Antidepressant Treatment
3.6.1. Cross-Sectional Studies
A large cross-sectional study investigated the association of CRP levels and psychological distress mediated by antidepressants in 10,363 UK adults, found robust associations of log-CRP and General Health Questionnaire (GHQ) among antidepressant users but not for non-users in both cross-sectional (p = 0.01 vs. 0.06, p = 0.28) and longitudinal models (p = 0.006 vs. 0.04, p = 0.39 two waves post-baseline) [60].
A cross-sectional study investigating the effects of agomelatine on CRP levels in 30 MDD patients assessed with MINI, HAMD, and the Snaith-Hamilton Pleasure Scale (SHAPS), proved that agomelatine significantly reduced depressive symptoms and CRP levels [53]. Higher CRP level variation was associated with higher baseline HAMD scores at the baseline [53].
An observational study analyzed the association between CRP levels with a worse response to escitalopram and a better response to nortriptyline in consideration of genetic disposition to inflammation [77]. A higher polygenic risk score for CRP was found to be associated with a slightly better response to escitalopram and a slightly worse response to nortriptyline, reflected in a statistically significant interaction between polygenic risk score and drug (p = 0.0093) [77].
We already mentioned a cross-sectional study evaluating the correlation of CRP with depressive symptoms and cognitive impairment in 149 MDD patients treated with fluoxetine or venlafaxine for six weeks [50]. Baseline levels of CRP were not correlated with baseline HAM-D scores (p = 0.606) but were significantly associated with treatment response at week 2 (p = 0.020) when patients with higher CRP levels had a poorer treatment response. CRP levels increased significantly after six weeks of treatment (p < 0.001), and CRP levels remained significantly high in patients with higher baseline levels (p < 0.001) [50].
3.6.2. Case-Control Studies
A case-control study evaluated the association between MDD clinical features and hs-CRP levels in a sample of 103 TRD patients and 103 non-TRD patients [84]. Depressive symptoms were investigated through HAMD-17. In the TRD group, the disease course was longer, the onset was earlier, and the educational level was lower. The HAMD score (p = 0.031), anxiety/somatization factor score (p = 0.015), and sleep disorder (p = 0.029) of TRD patients were positively associated with hs-CRP level, while the onset age (p = 0.009) was negatively correlated with the hs-CRP level [84].
A case-control study explored CRP levels in MDD subjects and its phenotypic associations in 102 TRD patients who currently experience depression, 48 treatment-responsive patients not undergoing depression, 48 patients not receiving medication, and 54 healthy volunteers [78]. Higher CRP levels were found in MDD patients compared to controls, and higher CRP levels were found in TRD patients compared to treatment-responsive MDD [78].
A case-control study examining CRP levels to evaluate the impact of SSRI treatment in 32 MDD individuals compared to 20 healthy subjects, following measuring CRP levels before and after SSRI treatment, reported a significant reduction after the treatment, regardless of symptom reduction [82].
3.6.3. RCT Studies
A retrospective study including 75 adult inpatients with MDD aimed at investigating the possibility of using CRP levels as predictors of antidepressant treatment response, found that subjects with high CRP levels had higher HDRS-17 scores, showed lower responses after 3 and 4 weeks of treatment, and lower remission rates [95].
The previously mentioned RCT evaluating the sex differences in the association between CRP levels and the response to antidepressant treatments, found that higher baseline CRP levels were found to be associated with a lower baseline-to-week-8 HAMD-17 reduction in females (p < 0.0001) but not in males (p = 0.632) [97].
A multicenter open-label RCT tested the hypothesis that CRP levels can predict differential response to escitalopram and nortriptyline [98]. CRP levels at baseline differentially predicted treatment outcomes with the two antidepressants. For patients with low levels of CRP (i.e., <1 mg/L), the improvement at MADRS total score was 3 points higher with escitalopram. For patients with higher CRP levels, the improvement in the MADRS score was 3 points higher with nortriptyline [98]. A RCT investigated the efficacy of anti-inflammatory (celecoxib) augmentation of antidepressant treatment in MDD patients and evaluated whether treatment response depended on baseline inflammation levels [96]. Data from 119 participants showed no evidence of superior efficacy of celecoxib augmentation over placebo and neither that pretreatment inflammation levels could modify the effect of celecoxib augmentation versus placebo [96].
3.7. Quality Assessment
Based on our judgment, 40 studies were rated as “good” studies [16,45,46,48,49,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,68,71,72,73,75,76,78,81,83,88,89,90,92,93,94,96,97,98,100] and 16 as “satisfactory” studies [47,50,67,69,70,74,77,79,80,82,84,85,86,87,91,95]. The main misses were the lack of justified and satisfactory sample size calculation before the study, the absence of non-respondent information and, in some studies, the lack of comparability (Supplementary: Newcastle-ottawa quality assessment scale Tables S1–S4).
4. Discussion
Overall, an increasing amount of evidence has suggested the presence of a dysregulation in the inflammation system in depressed patients [13,15,16,101]. Different pathways seem to be involved such as the kynurenine pathways hypothesis of depression in which there is excessive activation of the indoleamine-2,3-dioxygenase (IDO) [102]. This enzyme is present in microglia, astrocytes, and neurons and catabolizes tryptophan into kynurenine, a neurotoxic substrate, and it is responsible of reducing the amount of available tryptophan to produce serotonin [103]. Moreover, enzymes of inflammation such as manganese superoxide dismutase (MnSOD), myeloperoxidase (MPO), and inducible nitric oxide synthase (iNOS) were involved in the genesis of depressive disorder, by actively inducing the production of free radical, fatty acid, cellular DNA, and other factors that may lead to brain damage [104,105]. Indeed, several studies demonstrated an association between recurrent depressive disorders and increased activity of the enzymes mentioned above [105,106,107,108]. Another mechanism which was suggested to be implicated is represented by the oxidative stress which may predispose to an increased activity of reactive oxygen species (ROS) [10]. An imbalance between the antioxidant system and oxidizing agents may lead to macromolecules damage, alteration of normal cell signaling pathways, and structural and functional alteration [109,110,111]. Specific regions of the hippocampus (CA1 and CA4 region), cells in the dorsolateral region of the striatum, and neurons in the third and fifth layer of the cerebral cortex are most sensitive to damage [110]. Moreover, in patients suffering from depression, an increased expression of malondialdehyde, NO, and thiol protein group was reported. This is associated with reduced total antioxidant status, which can lead to deteriorated efficiency of operational memory, declarative memory, and verbal fluency [112,113]. Furthermore, oxidative and inflammatory pathways are strictly interconnected [114]. Indeed, oxidative stress induces inflammation through Nuclear Factor-kB (NF-kB) and consequently may cause an increased production of free radicals [114].
Furthermore, researchers also investigated the role of cytokines and acute-phase proteins in order to evaluate if it is possible to recognize specific inflammatory biomarkers for depression [16,115,116,117]. In particular, a research field of interest consists of identifying specific subgroups of MDD patients with a specific inflammatory pattern which may be associated with a different treatment response and, hence, needed a personalized, tailored treatment strategy. Among these inflammatory biomarkers, numerous studies focused on depression and CRP [15,29,56,115,118]. In fact, CRP is an acute-phase reactant protein, produced by the liver in response to inflammatory state and it is easily and cheap to be measured through a blood sample [24,30].
Overall, the present systematic review reported that most studies here retrieved, found a positive association between elevated CRP levels and depression [29,51,52,54,55,61,63,64,66,67,69,70,71,72,73,80,81,83,90,91,92,93,94,100]. Conversely, other studies did not confirm this association [49,50,62,68,74,76,86,88,89].
Specifically, CRP levels seem to be associated with depressive symptoms severity [29,63,72,80,81,90,91,92]. Furthermore, several studies investigated whether there was a specific pattern of depressive symptoms related to higher CRP levels, suggesting an association with symptoms of fatigue, restless sleep, low energy, concentration difficulties, poor psychomotor speed, and poor executive functioning [50,56,63,69,73]. In addition, CRP levels seem to be related to somatic symptoms [48] and not to apathy [91].
Higher CRP levels were observed in atypical MDD with respect to the typical manifestation [58], and were associated with reduced quality of life [80] and late-onset depression [81]. Moreover, hs-CRP levels seem to be an independent risk factor of depression and elevated hs-CRP levels could be a predictor of the onset of MDD [93]. Finally, stable elevated CRP levels were associated with increased risk for late-life depression symptoms [80] and the occurrence of multiple depressive episodes seems to improve later CRP levels, maybe by increasing the risk for cardiovascular and metabolic disease [89].
Evidence suggested also that CRP levels may vary among gender and/or ethnic differences. Lee et al. (2019) [64] reported a higher prevalence of depression in men with high CRP levels. The association was not observed in women. These results are consistent with other studies in which a positive association between CRP levels and depression was observed only in males. On the other hand, other studies displayed opposite results with a positive association between CRP levels and depression only among women [63,72,90,92,97]. Few studies reported that CRP levels were independently associated with depressive symptoms only in the white non-Hispanic population [48,51]. These results indicate a biological difference, yet to be understood, between gender/race/ethnicity that can independently modify the relationship between CRP levels and depression.
Among the studies included in the present systematic review, only three studies investigated CRP as a biomarker to differentiate psychiatric disorders [59,74,79]. Chang et al. (2017) [79] suggested that CRP levels of 621.6 mg/L could discriminate between MDD and BD-II in both depressed and euthymic states. The same results come from a study by Hanug and Lin (2007) [59] that reported persisted high CRP levels in BD-I after adjusting for covariates and not in MDD. On the contrary, in another study no differences were observed in CRP levels across different psychiatric diagnoses [86].
Furthermore, it would appear that there is a subgroup of depressed patients who showed a low-grade inflammatory state (i.e., CRP > 3.0 mg/L) [29,47,61,69,74,80,83,86,100], corroborating the hypothesis that inflammation might contribute to developing some types of depression, but not all of them [75]. Indeed, about a third of all depressed patients seem to express CRP levels > 3.0 mg/L [86,119,120]. Data were confirmed by a recent meta-analysis that included 13,541 depressed patients and 155,728 controls [121]. In 27% of the depressive patients there was a low-grade of inflammation (i.e., CRP > 3.0 mg/L) and over half of the patients showed a mildly elevated CRP level [121]. This may point out that a chronic low-grade inflammation could be associated with a different MDD subgroup with a distinct etiopathogenesis, clinical course, treatment response, and prognosis [13,72,121]. Indeed, 30% of patients with depression do not get relief from standard antidepressant therapy and this may be due to this low-grade inflammatory state [122].
Based on the abovementioned inflammatory theory of depression, several studies investigated the association between CRP levels and antidepressant treatment [123]. A wide range of studies reported that elevated levels of CRP were associated with TRD patients [50,60,78,84,95,97]. Conversely, other studies showed that lower levels of CRP were associated with a better and faster response to SSRI treatment [63,98]. Indeed, anti-inflammatory action of SSRI and serotonin and noradrenaline inhibitors (SNRIs) has been hypothesized through which they can indirectly reduce depressive symptoms [124,125,126], even though the findings are still contradictory [77]. Little evidence reported that antidepressant treatment may decrease CRP levels [82,124], although a recent meta-analysis conducted by Wiedlocha et al. (2018) [127] did not show significant effect on CRP levels using antidepressants. Based on the inflammatory theory, anti-inflammatory drugs (e.g., non-steroidal anti-inflammatory drugs or anti-cytokine) could be useful in the treatment of depression [128,129,130,131], despite findings so far are contradictory [96,132,133].
Different mechanisms were assumed to explain how a low-grade inflammation may interact with the severity of depressive symptoms, including cognitive impairment, and with treatment resistance in MDD patients [56,121,134]. A possible explanation is that low-grade inflammation (i.e., CRP > 3 mg/L) may lead to cerebral inflammation by decreasing neurotrophic support, oxidative stress damage, increasing glutamatergic excitotoxicity, and affecting neuronal serotonin transporter activity [135] which, then, may determine a microstructural disintegration which predominantly affects frontal pathways and corresponding executive function [136]. Moreover, it can also affect the dopaminergic neurons related to cognitive function, including psychomotor speed, memory, and executive cognitive function [137,138,139,140]. For these reasons, interventions that reduce inflammation may improve cognitive functioning in depression [56]. Moreover, patients with MDD might be stratified for CRP levels to distinguish different clinical profiles that could be responsive to second-line treatment with anti-inflammatory drugs [78].
Furthermore, several studies have investigated the role of SNPs in the association between CRP levels and depression with mixed results [45,46,57,65,85,87].
However, despite the encouraging and interesting findings coming from the present systematic review, there are several limitations in the present review to be discussed. Firstly, most studies display a methodological heterogeneity in terms of study design, different sample sizes, inclusion/exclusion criteria, various diagnostic tools, and recruitment settings. Secondly, not all included studies controlled for potential confounding variables in the association between depression and inflammation and, hence, this may limit the generalizability of the findings in those studies which report positive associations between CRP levels and depression. Thirdly, the socio-demographic characteristic of the samples is extremely dis-homogeneous in terms of gender, race, ethnicity, etc. In this regard, few studies specifically investigated (if any) differences occur in the association between CRP levels and depression, considering gender, ethnicity, type of MDD severity, clinical course, illness duration, type of concomitant treatment and so forth. Furthermore, from a clinical point of view, studies here retrieved showed different phases of illness (i.e., acute, and chronic phase, remitted patients, early-onset or late-onset patients, etc.). Finally, antidepressant treatment has not been always reported (i.e., patients with stable antidepressant treatment, patients with not stable antipsychotic medication, free-drug patients, naïve-drug patients, not specific antidepressant medication, etc.).
Further studies are needed in order to better understand the core mechanism through which CRP may interact in depression and which role CRP may have in characterizing subgroups of depressed patients and guide treatment strategies. More methodologically homogeneous and more geographically defined studies also focusing on gender and ethnicity CRP variability could be useful in better understanding biological differences among different sexes and races and guide more personalized and patient-tailored interventions. Similarly, further studies should be implemented for investigating the different MDD phases and the different clinical depression subtypes, in order to identify whether a specific subgroup of MDD patients may benefit from monitoring CRP levels from a clinical and therapeutic point of view. Furthermore, there is the need for more studies that investigate how CRP and inflammation status may determine changes in the CNS of depressed patients, by implementing neuroimaging studies. Moreover, more RCT studies are needed in order to investigate the role of antidepressant and anti-inflammatory therapy in depressed patients with a low-grade of inflammation.
5. Conclusions
In conclusion, this systematic review provides robust evidence about the potential role of CRP and its blood levels in depression. Indeed, patients with elevated CRP levels seem to be associated with a greater symptom severity, specific pattern of depressive symptoms and a worst treatment response, although it is still unclear if inflammation may contribute directly to the pathogenesis of depression or whether it may rather be a consequence of the illness and covariates interaction. Moreover, about one-third of depressed patients showed a low-grade inflammatory state (i.e., CRP > 3.0 mg/L), by suggesting the presence of a different MDD subgroup with a distinct etiopathogenesis, clinical course, treatment response, and prognosis which may benefit of a monitoring of CRP levels and might potentially respond to anti-inflammatory treatments. These findings are indeed extremely relevant for the development of new interventional strategies and in order to better understand if CRP may be considered a useful biomarker for depression.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijms23031616/s1.
Author Contributions
Conceptualization, L.O. and S.P.; methodology, L.O. and S.P.; formal analysis, S.P. and S.T.V.; data curation, S.P., S.T.V. and L.O.; writing-original draft preparation, S.P. and L.O., writing-review and editing, L.O., and V.S.; supervision, U.V. All authors have read and agreed to the published version of the manuscript.
Funding
The research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R. Prevalence of Depression in the Community from 30 Countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008; Available online: https://apps.who.int/iris/handle/10665/43942 (accessed on 20 December 2021).
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/254610 (accessed on 20 December 2021).
- Malhi, G.S.; Mann, J.J. Depression. Lancet 2018, 392, 2299–2312. [Google Scholar] [CrossRef]
- Kessler, R.C.; Bromet, E.J. The Epidemiology of Depression Across Cultures. Annu. Rev. Public Health 2013, 34, 119–138. [Google Scholar] [CrossRef] [Green Version]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- Perez-Caballero, L.; Torres-Sanchez, S.; Romero-López-Alberca, C.; González-Saiz, F.; Mico, J.A.; Berrocoso, E. Monoaminergic system and depression. Cell Tissue Res. 2019, 377, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Yirmyia, R.; Noraberg, J.; Brene, S.; Hibbeln, J.; Perini, G.; Kubera, M.; Bob, P.; Lerer, B.; Maj, M. The inflammatory & neurodegenerative (I&ND) hypothesis of depression: Leads for future research and new drug developments in depression. Metab. Brain Dis. 2009, 24, 27–53. [Google Scholar] [CrossRef]
- Keller, J.; Gomez, R.; Williams, G.; Lembke, A.; Lazzeroni, L.; Murphy, G.M.; Schatzberg, A.F. HPA axis in major depression: Cortisol, clinical symptomatology and genetic variation predict cognition. Mol. Psychiatry 2017, 22, 527–536. [Google Scholar] [CrossRef]
- Czarny, P.; Wigner, P.; Galecki, P.; Sliwinski, T. The interplay between inflammation, oxidative stress, DNA damage, DNA repair and mitochondrial dysfunction in depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 80, 309–321. [Google Scholar] [CrossRef]
- Gałecki, P.; Talarowska, M. Neurodevelopmental theory of depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 80, 267–272. [Google Scholar] [CrossRef]
- Uchida, S.; Yamagata, H.; Seki, T.; Watanabe, Y. Epigenetic mechanisms of major depression: Targeting neuronal plasticity. Psychiatry Clin. Neurosci. 2018, 72, 212–227. [Google Scholar] [CrossRef] [Green Version]
- Gałecki, P.; Talarowska, M. Inflammatory theory of depression. Psychiatr. Polska 2018, 52, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, D.R.; Rapaport, M.H.; Miller, B.J. A meta-analysis of blood cytokine network alterations in psychiatric patients: Comparisons between schizophrenia, bipolar disorder and depression. Mol. Psychiatry 2016, 21, 1696–1709. [Google Scholar] [CrossRef] [PubMed]
- Nobis, A.; Zalewski, D.; Waszkiewicz, N. Peripheral Markers of Depression. J. Clin. Med. 2020, 9, 3793. [Google Scholar] [CrossRef] [PubMed]
- Osimo, E.F.; Pillinger, T.; Rodriguez, I.M.; Khandaker, G.M.; Pariante, C.M.; Howes, O.D. Inflammatory markers in depression: A meta-analysis of mean differences and variability in 5166 patients and 5083 controls. Brain Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Siegmann, E.-M.; Müller, H.H.O.; Luecke, C.; Philipsen, A.; Kornhuber, J.; Grömer, T.W. Association of Depression and Anxiety Disorders With Autoimmune Thyroiditis: A Systematic Review and Meta-analysis. JAMA Psychiatry 2018, 75, 577–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Parra, S.; Daudén, E. Psoriasis and Depression: The Role of Inflammation. Actas Dermo-Sifiliográficas 2019, 110, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.L.; Stiernborg, M.; Skott, E.; Söderström, Å.; Giacobini, M.; Lavebratt, C. Proinflammatory mediators and their associations with medication and comorbid traits in children and adults with ADHD. Eur. Neuropsychopharmacol. 2020, 41, 118–131. [Google Scholar] [CrossRef]
- Fragoulis, G.E.; Cavanagh, J.; Tindell, A.; Derakhshan, M.; Paterson, C.; Porter, D.; McInnes, I.B.; Siebert, S. Depression and anxiety in an early rheumatoid arthritis inception cohort. associations with demographic, socioeconomic and disease features. RMD Open 2020, 6, e001376. [Google Scholar] [CrossRef]
- Huang, Y.; Su, Y.; Chen, H.; Liu, H.; Hu, J. Serum Levels of CRP are Associated with Depression in a Middle-aged and Elderly Population with Diabetes Mellitus: A Diabetes Mellitus-Stratified Analysis in a Population-Based Study. J. Affect. Disord. 2021, 281, 351–357. [Google Scholar] [CrossRef]
- Pope, J.E.; Choy, E.H. C-reactive protein and implications in rheumatoid arthritis and associated comorbidities. Semin. Arthritis Rheum. 2021, 51, 219–229. [Google Scholar] [CrossRef]
- Byrne, G.; Rosenfeld, G.; Leung, Y.; Qian, H.; Raudzus, J.; Nunez, C.; Bressler, B. Prevalence of Anxiety and Depression in Patients with Inflammatory Bowel Disease. Can. J. Gastroenterol. Hepatol. 2017, 2017, 6496727. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. Clinical Application of C-Reactive Protein for Cardiovascular Disease Detection and Prevention. Circulation 2003, 107, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.; Byrne, M.L.; et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef] [Green Version]
- Benros, M.; Pedersen, M.G.; Rasmussen, H.; Eaton, W.W.; Nordentoft, M.; Mortensen, P.B. A Nationwide Study on the Risk of Autoimmune Diseases in Individuals With a Personal or a Family History of Schizophrenia and Related Psychosis. Am. J. Psychiatry 2014, 171, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, R. Cytokine, Sickness Behavior, and Depression. Neurol. Clin. 2006, 24, 441–460. [Google Scholar] [CrossRef] [Green Version]
- McFarland, D.C.; Walsh, L.E.; Saracino, R.; Nelson, C.J.; Breitbart, W.; Rosenfeld, B. The Sickness Behavior Inventory-Revised: Sickness behavior and its associations with depression and inflammation in patients with metastatic lung cancer. Palliat. Support. Care 2020, 19, 312–321. [Google Scholar] [CrossRef]
- Osimo, E.F.; Stochl, J.; Zammit, S.; Lewis, G.; Jones, P.B.; Khandaker, G.M. Longitudinal population subgroups of CRP and risk of depression in the ALSPAC birth cohort. Compr. Psychiatry 2019, 96, 152143. [Google Scholar] [CrossRef]
- Nehring, S.M.; Goyal, A.; Bansal, P.; Patel, B.C. C Reactive Protein. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: http://www.ncbi.nlm.nih.gov/books/NBK441843/ (accessed on 20 December 2021).
- Windgassen, E.B.; Funtowicz, L.; Lunsford, T.N.; Harris, L.A.; Mulvagh, S.L. C-Reactive Protein and High-Sensitivity C-Reactive Protein: An Update for Clinicians. Postgrad. Med. 2011, 123, 114–119. [Google Scholar] [CrossRef]
- Joseph, J.; Depp, C.; Martin, A.S.; Daly, R.E.; Glorioso, D.K.; Palmer, B.; Jeste, D.V. Associations of high sensitivity C-reactive protein levels in schizophrenia and comparison groups. Schizophr. Res. 2015, 168, 456–460. [Google Scholar] [CrossRef] [Green Version]
- Jeon, M.-T.; Kim, K.-S.; Kim, E.S.; Lee, S.; Kim, J.; Hoe, H.-S.; Kim, D.-G. Emerging pathogenic role of peripheral blood factors following BBB disruption in neurodegenerative disease. Ageing Res. Rev. 2021, 68, 101333. [Google Scholar] [CrossRef]
- Felger, J.C.; Haroon, E.; Patel, T.A.; Goldsmith, D.R.; Wommack, E.C.; Woolwine, B.J.; Le, N.-A.; Feinberg, R.; Tansey, M.G.; Miller, A.H. What does plasma CRP tell us about peripheral and central inflammation in depression? Mol. Psychiatry 2020, 25, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Prakash, R.; Carmichael, S.T. Blood−brain barrier breakdown and neovascularization processes after stroke and traumatic brain injury. Curr. Opin. Neurol. 2015, 28, 556–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menard, C.; Pfau, M.L.; Hodes, G.; Kana, V.; Wang, V.X.; Bouchard, S.; Takahashi, A.; Flanigan, M.E.; Aleyasin, H.; LeClair, K.B.; et al. Social stress induces neurovascular pathology promoting depression. Nat. Neurosci. 2017, 20, 1752–1760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aveleira, C.A.; Lin, C.-M.; Abcouwer, S.F.; Ambrosio, A.F.; Antonetti, D.A. TNF-Signals Through PKC/NF-B to Alter the Tight Junction Complex and Increase Retinal Endothelial Cell Permeability. Diabetes 2010, 59, 2872–2882. [Google Scholar] [CrossRef] [Green Version]
- Horn, S.R.; Long, M.M.; Nelson, B.W.; Allen, N.B.; Fisher, P.A.; Byrne, M.L. Replication and reproducibility issues in the relationship between C-reactive protein and depression: A systematic review and focused meta-analysis. Brain Behav. Immun. 2018, 73, 85–114. [Google Scholar] [CrossRef]
- Kuhlmann, C.R.; Librizzi, L.; Closhen, D.; Pflanzner, T.; Lessmann, V.; Pietrzik, C.U.; de Curtis, M.; Luhmann, H.J. Mechanisms of C-Reactive Protein-Induced Blood–Brain Barrier Disruption. Stroke 2009, 40, 1458–1466. [Google Scholar] [CrossRef] [Green Version]
- D’Mello, C.; Le, T.; Swain, M.G. Cerebral Microglia Recruit Monocytes into the Brain in Response to Tumor Necrosis Factor Signaling during Peripheral Organ Inflammation. J. Neurosci. 2009, 29, 2089–2102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKim, D.B.; Weber, M.D.; Niraula, A.; Sawicki, C.M.; Liu, X.; Jarrett, B.L.; Ramirez-Chan, K.; Wang, Y.; Roeth, R.M.; Sucaldito, A.D.; et al. Microglial recruitment of IL-1β-producing monocytes to brain endothelium causes stress-induced anxiety. Mol. Psychiatry 2018, 23, 1421–1431. [Google Scholar] [CrossRef] [Green Version]
- Wesselingh, R.; Butzkueven, H.; Buzzard, K.; Tarlinton, D.; O’Brien, T.; Monif, M. Innate Immunity in the Central Nervous System: A Missing Piece of the Autoimmune Encephalitis Puzzle? Front. Immunol. 2019, 10, 2066. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2009; Volume 5. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Almeida, O.P.; Norman, P.E.; Allcock, R.; van Bockxmeer, F.; Hankey, G.J.; Jamrozik, K.; Flicker, L. Polymorphisms of the CRP gene inhibit inflammatory response and increase susceptibility to depression: The Health in Men Study. Int. J. Epidemiol. 2009, 38, 1049–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ancelin, M.-L.; Farre, A.; Carrière, I.; Ritchie, K.; Chaudieu, I.; Ryan, J. C-reactive protein gene variants: Independent association with late-life depression and circulating protein levels. Transl. Psychiatry 2015, 5, e499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldirola, D.; Daccò, S.; Cuniberti, F.; Grassi, M.; Lorusso, S.; Diaferia, G.; Perna, G. Elevated C-reactive protein levels across diagnoses: The first comparison among inpatients with major depressive disorder, bipolar disorder, or obsessive–compulsive disorder. J. Psychosom. Res. 2021, 150, 110604. [Google Scholar] [CrossRef]
- Case, S.M.; Stewart, J.C. Race/ethnicity moderates the relationship between depressive symptom severity and C-reactive protein: 2005–2010 NHANES data. Brain Behav. Immun. 2014, 41, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Chaiton, M.; O’Loughlin, J.; Karp, I.; Lambert, M. Depressive Symptoms and C-Reactive Protein Are Not Associated in a Population-Based Sample of Adolescents. Int. J. Behav. Med. 2010, 17, 216–222. [Google Scholar] [CrossRef]
- Chang, H.H.; Lee, I.H.; Gean, P.W.; Lee, S.-Y.; Chi, M.H.; Yang, Y.K.; Lu, R.-B.; Chen, P.S. Treatment response and cognitive impairment in major depression: Association with C-reactive protein. Brain Behav. Immun. 2012, 26, 90–95. [Google Scholar] [CrossRef]
- Chapman, A.; Santos-Lozada, A.R. Racial and ethnic differences in the associations between social integration, C-reactive protein and depressive symptoms. SSM-Popul. Health 2020, 12, 100663. [Google Scholar] [CrossRef]
- Cho, S.H.; Lim, J.-E.; Lee, J.; Lee, J.S.; Jeong, H.-G.; Lee, M.-S.; Ko, Y.-H.; Han, C.; Ham, B.-J.; Han, K.-M. Association between high-sensitivity C-reactive protein levels and depression: Moderation by age, sex, obesity, and aerobic physical activity. J. Affect. Disord. 2021, 291, 375–383. [Google Scholar] [CrossRef]
- De Berardis, D.; Fornaro, M.; Orsolini, L.; Iasevoli, F.; Tomasetti, C.; de Bartolomeis, A.; Serroni, N.; De Lauretis, I.; Girinelli, G.; Mazza, M.; et al. Effect of agomelatine treatment on C-reactive protein levels in patients with major depressive disorder: An exploratory study in «real-world,» everyday clinical practice. CNS Spectr. 2017, 22, 342–347. [Google Scholar] [CrossRef]
- Elovainio, M.; Aalto, A.-M.; Kivimäki, M.; Pirkola, S.; Sundvall, J.; Lönnqvist, J.; Reunanen, A. Depression and C-Reactive Protein: Population-Based Health 2000 Study. Psychosom. Med. 2009, 71, 423–430. [Google Scholar] [CrossRef]
- Ford, D.E.; Erlinger, T.P. Depression and C-reactive protein in US adults: Data from the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2004, 164, 1010–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mac Giollabhui, N.; Alloy, L.B.; Schweren, L.J.S.; Hartman, C.A. Investigating whether a combination of higher CRP and depression is differentially associated with worse executive functioning in a cohort of 43,896 adults. Brain Behav. Immun. 2021, 96, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Halder, I.; Marsland, A.L.; Cheong, J.; Muldoon, M.F.; Ferrell, R.E.; Manuck, S.B. Polymorphisms in the CRP gene moderate an association between depressive symptoms and circulating levels of C-reactive protein. Brain Behav. Immun. 2010, 24, 160–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hickman, R.J.; Khambaty, T.; Stewart, J.C. C-reactive protein is elevated in atypical but not nonatypical depression: Data from the National Health and Nutrition Examination Survey (NHANES) 1999–2004. J. Behav. Med. 2014, 37, 621–629. [Google Scholar] [CrossRef]
- Huang, T.-L.; Lin, F.-C. High-sensitivity C-reactive protein levels in patients with major depressive disorder and bipolar mania. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2007, 31, 370–372. [Google Scholar] [CrossRef]
- Hughes, A.; Kumari, M. Associations of C-reactive protein and psychological distress are modified by antidepressants, supporting an inflammatory depression subtype: Findings from UKHLS. Brain Behav. Immun. 2017, 66, 89–93. [Google Scholar] [CrossRef] [Green Version]
- Jung, Y.-E.; Kang, K.Y. Elevated hs-CRP level is associated with depression in younger adults: Results from the Korean National Health and Nutrition Examination Survey (KNHANES 2016). Psychoneuroendocrinology 2019, 109, 104397. [Google Scholar] [CrossRef]
- Khan, A.; Leonard, D.; Defina, L.; Barlow, C.E.; Willis, B.; Brown, E.S. Association between C reactive protein and depression in a population of healthy adults: The Cooper Center Longitudinal Study. J. Investig. Med. 2020, 68, 1019–1023. [Google Scholar] [CrossRef]
- Köhler-Forsberg, O.; Buttenschøn, H.; Tansey, K.; Maier, W.; Hauser, J.; Dernovsek, M.Z.; Henigsberg, N.; Souery, D.; Farmer, A.; Rietschel, M.; et al. Association between C-reactive protein (CRP) with depression symptom severity and specific depressive symptoms in major depression. Brain, Behav. Immun. 2017, 62, 344–350. [Google Scholar] [CrossRef]
- Lee, S.; Oh, S.; Jang, S.-I.; Park, E.-C. Sex Difference in the Association between High-sensitivity C-reactive Protein and Depression: The 2016 Korea National Health and Nutrition Examination Survey. Sci. Rep. 2019, 9, 1918. [Google Scholar] [CrossRef]
- Li, X.; Sun, N.; Yang, C.; Liu, Z.; Li, X.; Zhang, K. C-Reactive Protein Gene Variants in Depressive Symptoms & Antidepressants Efficacy. Psychiatry Investig. 2019, 16, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Liukkonen, T.; Silvennoinen-Kassinen, S.; Jokelainen, J.; Räsänen, P.; Leinonen, M.; Meyer-Rochow, V.B.; Timonen, M. The Association Between C-Reactive Protein Levels and Depression: Results from the Northern Finland 1966 Birth Cohort Study. Biol. Psychiatry 2006, 60, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Luukinen, H.; Jokelainen, J.; Hedberg, P. The relationships between high-sensitivity C-reactive protein and incident depressed mood among older adults. Scand. J. Clin. Lab. Investig. 2010, 70, 75–79. [Google Scholar] [CrossRef] [PubMed]
- de Menezes, S.T.; de Figueiredo, R.C.; Goulart, A.C.; Nunes, M.A.; Benseñor, I.M.; Viana, M.C.; Barreto, S.M. Lack of association between depression and C-reactive protein level in the baseline of Longitudinal Study of Adult Health (ELSA-Brasil). J. Affect Disord. 2017, 208, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Moriarity, D.P.; van Borkulo, C.; Alloy, L.B. Inflammatory phenotype of depression symptom structure: A network perspective. Brain, Behav. Immun. 2020, 93, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Pikhart, H.; Hubacek, J.A.; Kubinova, R.; Nicholson, A.; Peasey, A.; Capkova, N.; Poledne, R.; Bobak, M. Depressive symptoms and levels of C-reactive protein: A population-based study. Soc Psychiatry Psychiatr. Epidemiol. 2009, 44, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Song, B.M.; Lee, J.-M.; Choi, W.; Youm, Y.; Chu, S.H.; Park, Y.-R.; Kim, H.C. Association between C reactive protein level and depressive symptoms in an elderly Korean population: Korean Social Life, Health and Aging Project. BMJ Open 2015, 5, e006429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabatabaeizadeh, S.-A.; Abdizadeh, M.F.; Meshkat, Z.; Khodashenas, E.; Darroudi, S.; Fazeli, M.; Ferns, G.A.; Avan, A.; Ghayour-Mobarhan, M. There is an association between serum high-sensitivity C-reactive protein (hs-CRP) concentrations and depression score in adolescent girls. Psychoneuroendocrinology 2018, 88, 102–104. [Google Scholar] [CrossRef] [PubMed]
- White, J.; Kivimäki, M.; Jokela, M.; Batty, G.D. Association of inflammation with specific symptoms of depression in a general population of older people: The English Longitudinal Study of Ageing. Brain Behav. Immun. 2017, 61, 27–30. [Google Scholar] [CrossRef] [Green Version]
- Wysokiński, A.; Margulska, A.; Strzelecki, D.; Kłoszewska, I. Levels of C-reactive protein (CRP) in patients with schizophrenia, unipolar depression and bipolar disorder. Nord. J. Psychiatry 2014, 69, 346–353. [Google Scholar] [CrossRef]
- Zavos, H.M.; Zunszain, P.A.; Jayaweera, K.; Powell, T.R.; Chatzivasileiadou, M.; Harber-Aschan, L.; Adikari, A.; Pannala, G.; Siribaddana, S.; Badini, I.; et al. Relationship between CRP and depression: A genetically sensitive study in Sri Lanka. J. Affect. Disord. 2021, 297, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, J.-L.; Zhang, L.-L.; Guo, L.-L.; Li, H.; Li, D. No association between C-reactive protein and depressive symptoms among the middle-aged and elderly in China: Evidence from the China Health and Retirement Longitudinal Study. Medicine 2018, 97, e12352. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, A.; Fabbri, C.; Rietschel, M.; Hauser, J.; Mors, O.; Maier, W.; Zobel, A.; Farmer, A.; Aitchison, K.J.; McGuffin, P.; et al. Genetic disposition to inflammation and response to antidepressants in major depressive disorder. J. Psychiatr. Res. 2018, 105, 17–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamberlain, S.R.; Cavanagh, J.; de Boer, P.; Mondelli, V.; Jones, D.N.; Drevets, W.C.; Cowen, P.J.; Harrison, N.A.; Pointon, L.; Pariante, C.M.; et al. Treatment-resistant depression and peripheral C-reactive protein. Br. J. Psychiatry 2019, 214, 11–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.H.; Wang, T.-Y.; Lee, I.H.; Lee, S.-Y.; Chen, K.C.; Huang, S.-Y.; Yang, Y.K.; Lu, R.-B.; Chen, P.S. C-reactive protein: A differential biomarker for major depressive disorder and bipolar II disorder. World J. Biol. Psychiatry 2016, 18, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Foley, É.M.; Parkinson, J.T.; Kappelmann, N.; Khandaker, G.M. Clinical phenotypes of depressed patients with evidence of inflammation and somatic symptoms. Compr. Psychoneuroendocrinol. 2021, 8, 100079. [Google Scholar] [CrossRef] [PubMed]
- Mishra, D.; Sardesai, U.; Razdan, R. C-reactive protein level in late-onset depression: A case–control study. Indian J. Psychiatry 2018, 60, 467–471. [Google Scholar] [CrossRef]
- O’Brien, S.M.; Scott, L.V.; Dinan, T. Antidepressant therapy and C-reactive protein levels. Br. J. Psychiatry 2006, 188, 449–452. [Google Scholar] [CrossRef] [Green Version]
- Pitharouli, M.C.; Hagenaars, S.P.; Glanville, K.P.; Coleman, J.R.; Hotopf, M.; Lewis, C.M.; Pariante, C.M. Elevated C-Reactive Protein in Patients With Depression, Independent of Genetic, Health, and Psychosocial Factors: Results From the UK Biobank. Am. J. Psychiatry 2021, 178, 522–529. [Google Scholar] [CrossRef]
- Qiao, J.; Geng, D.; Qian, L.; Zhu, X.; Zhao, H. Correlation of clinical features with hs-CRP in TRD patients. Exp. Ther. Med. 2018, 17, 344–348. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Zhong, H.; Lu, M.; Song, G.; Zhang, X.; Lin, M.; Yang, S.; Qian, M. Higher Serum C Reactive Protein Determined C Reactive Protein Single-Nucleotide Polymorphisms Are Involved in Inherited Depression. Psychiatry Investig. 2018, 15, 824–828. [Google Scholar] [CrossRef] [PubMed]
- Wysokiński, A.; Socha, K.; Sołtysik, B.K.; Kłoszewska, I.; Sobów, T.; Kostka, T. Levels of C-reactive protein (CRP) in elderly patients with unipolar depression—Case control analysis. Nord. J. Psychiatry 2016, 70, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Yibulaiyin, H.-; Sun, H.; Yang, Y. Depression is associated with CRP SNPs in patients with family history. Transl. Neurosci. 2017, 8, 201–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au, B.; Smith, K.; Gariépy, G.; Schmitz, N. The longitudinal associations between C-reactive protein and depressive symptoms: Evidence from the English Longitudinal Study of Ageing (ELSA). Int. J. Geriatr. Psychiatry 2014, 30, 976–984. [Google Scholar] [CrossRef]
- Copeland, W.E.; Shanahan, L.; Worthman, C.M.; Angold, A.; Costello, E.J. Cumulative Depression Episodes Predict Later C-Reactive Protein Levels: A Prospective Analysis. Biol. Psychiatry 2012, 71, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Chiriboga, D.E.; Pagoto, S.L.; Rosal, M.C.; Li, W.; Merriam, P.A.; Hébert, J.R.; Whited, M.C.; Ockene, I.S. Association between Depression and C-Reactive Protein. Cardiol. Res. Pract. 2011, 2011, 286509. [Google Scholar] [CrossRef] [Green Version]
- Maas, D.W.; van der Mast, R.C.; de Craen, A.J.M. Increased C-reactive protein is not associated with apathy: The Leiden 85-Plus Study. Int. J. Geriatr. Psychiatry 2009, 24, 1177–1184. [Google Scholar] [CrossRef]
- Matthews, K.A.; Schott, L.L.; Bromberger, J.T.; Cyranowski, J.M.; Everson-Rose, S.A.; Sowers, M. Are there bi-directional associations between depressive symptoms and C-reactive protein in mid-life women? Brain Behav. Immun. 2010, 24, 96–101. [Google Scholar] [CrossRef] [Green Version]
- Pasco, J.A.; Nicholson, G.; Williams, L.; Jacka, F.N.; Henry, A.P.M.J.; Kotowicz, M.; Schneider, H.G.; Leonard, B.E.; Berk, M. Association of high-sensitivity C-reactive protein with de novo major depression. Br. J. Psychiatry 2010, 197, 372–377. [Google Scholar] [CrossRef] [Green Version]
- Sonsin-Diaz, N.; Gottesman, R.; Fracica, E.; Walston, J.; Windham, B.G.; Knopman, D.S.; Walker, K.A. Chronic Systemic Inflammation Is Associated With Symptoms of Late-Life Depression: The ARIC Study. Am. J. Geriatr. Psychiatry 2020, 28, 87–98. [Google Scholar] [CrossRef]
- Zhang, J.; Yue, Y.; Thapa, A.; Fang, J.; Zhao, S.; Shi, W.; Yang, Z.; Li, Y.; Yuan, Y. Baseline serum C-reactive protein levels may predict antidepressant treatment responses in patients with major depressive disorder. J. Affect. Disord. 2019, 250, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Baune, B.T.; Sampson, E.; Louise, J.; Hori, H.; Schubert, K.O.; Clark, S.R.; Mills, N.T.; Fourrier, C. No evidence for clinical efficacy of adjunctive celecoxib with vortioxetine in the treatment of depression: A 6-week double-blind placebo controlled randomized trial. Eur. Neuropsychopharmacol. 2021, 53, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Jha, M.; Minhajuddin, A.; Chin-Fatt, C.; Greer, T.L.; Carmody, T.J.; Trivedi, M.H. Sex differences in the association of baseline c-reactive protein (CRP) and acute-phase treatment outcomes in major depressive disorder: Findings from the EMBARC study. J. Psychiatr. Res. 2019, 113, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Uher, R.; Tansey, K.; Dew, T.; Maier, W.; Mors, O.; Hauser, J.; Dernovsek, M.Z.; Henigsberg, N.; Souery, D.; Farmer, A.; et al. An Inflammatory Biomarker as a Differential Predictor of Outcome of Depression Treatment With Escitalopram and Nortriptyline. Am. J. Psychiatry 2014, 171, 1278–1286. [Google Scholar] [CrossRef]
- Wells, G.A.; Sher, B.; O’Connel, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessment the quality of nonrandomized studies in meta-analyses. Clin. Epidemiol. 2014. [Google Scholar]
- Franco, F.G.D.M.; Laurinavicius, A.G.; Lotufo, P.A.; Conceição, R.D.; Morita, F.; Katz, M.; Wajngarten, M.; Carvalho, J.A.M.; Bosworth, H.B.; Santos, R.D. Persistent Depressive Symptoms are Independent Predictors of Low-Grade Inflammation Onset Among Healthy Individuals. Arq. Bras. de Cardiol. 2017, 109, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Troubat, R.; Barone, P.; Leman, S.; DeSmidt, T.; Cressant, A.; Atanasova, B.; Brizard, B.; El Hage, W.; Surget, A.; Belzung, C.; et al. Neuroinflammation and depression: A review. Eur. J. Neurosci. 2021, 53, 151–171. [Google Scholar] [CrossRef]
- Ramírez, L.A.; Pérez-Padilla, E.A.; García-Oscos, F.; Salgado, H.; Atzori, M.; Pineda, J.C. A new theory of depression based on the serotonin/kynurenine relationship and the hypothalamicpituitary-adrenal axis. Biomedica 2018, 38, 437–450. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G. Editorial: The Kynurenine and Melatonergic Pathways in Psychiatric and CNS Disorders. Curr. Pharm. Des. 2016, 22, 947–948. [Google Scholar] [CrossRef]
- Catena-Dell’Osso, M.; Bellantuono, C.; Consoli, G.; Baroni, S.; Rotella, F.; Marazziti, D. Inflammatory and neurodegenerative pathways in depression: A new avenue for antidepressant development? Curr. Med. Chem. 2011, 18, 245–255. [Google Scholar] [CrossRef]
- Gałecki, P.; Talarowska, M.; Bobińska, K.; Zajączkowska, M.; Su, K.-P.; Maes, M. Impact of oxidative/nitrosative stress and inflammation on cognitive functions in patients with recurrent depressive disorders. Med Sci. Monit. 2014, 20, 110–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.-K.; Paik, J.-W.; Lee, S.-W.; Yoon, D.; Han, C.; Lee, B.-H. Increased plasma nitric oxide level associated with suicide attempt in depressive patients. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2006, 30, 1091–1096. [Google Scholar] [CrossRef]
- Gałecki, P.; Szemraj, J.; Bieńkiewicz, M.; Florkowski, A.; Gałecka, E. Lipid peroxidation and antioxidant protection in patients during acute depressive episodes and in remission after fluoxetine treatment. Pharmacol. Rep. 2009, 61, 436–447. [Google Scholar] [CrossRef]
- Köhler, C.A.; Freitas, T.H.; Maes, M.; De Andrade, N.Q.; Liu, C.S.; Fernandes, B.S.; Stubbs, B.; Solmi, M.; Veronese, N.; Herrmann, N.; et al. Peripheral cytokine and chemokine alterations in depression: A meta-analysis of 82 studies. Acta Psychiatr. Scand. 2017, 135, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Prabakaran, S.; Swatton, J.E.; Ryan, M.M.; Huffaker, S.J.; Huang, J.T.-J.; Griffin, J.L.; Wayland, M.; Freeman, T.; Dudbridge, F.; Lilley, K.S.; et al. Mitochondrial dysfunction in schizophrenia: Evidence for compromised brain metabolism and oxidative stress. Mol. Psychiatry 2004, 9, 684–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maes, M.; Berk, M.; Goehler, L.; Song, C.; Anderson, G.; Gałecki, P.; Leonard, B. Depression and sickness behavior are Janus-faced responses to shared inflammatory pathways. BMC Med. 2012, 10, 66. [Google Scholar] [CrossRef] [Green Version]
- Machado, A.K.; Pan, A.Y.; da Silva, T.M.; Duong, A.; Andreazza, A.C. Upstream Pathways Controlling Mitochondrial Function in Major Psychosis: A Focus on Bipolar Disorder. Can. J. Psychiatry 2016, 61, 446–456. [Google Scholar] [CrossRef] [Green Version]
- Talarowska, M.; Gałecki, P.; Maes, M.; Gardner, A.; Chamielec, M.; Orzechowska, A.; Bobińska, K.; Kowalczyk, E. Malondialdehyde plasma concentration correlates with declarative and working memory in patients with recurrent depressive disorder. Mol. Biol. Rep. 2011, 39, 5359–5366. [Google Scholar] [CrossRef]
- Gałecki, P.; Talarowska, M.; Bobińska, K.; Kowalczyk, E.; Gałecka, E.; Lewiński, A. Thiol protein groups correlate with cognitive impairment in patients with recurrent depressive disorder. Neuro Endocrinol. Lett. 2013, 34, 780–786. [Google Scholar]
- Hayden, M.S.; Ghosh, S. Signaling to NF-kappaB. Genes Dev. 2004, 18, 2195–2224. [Google Scholar] [CrossRef] [Green Version]
- Howren, M.B.; Lamkin, D.M.; Suls, J. Associations of Depression With C-Reactive Protein, IL-1, and IL-6: A Meta-Analysis. Psychosom. Med. 2009, 71, 171–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valkanova, V.; Ebmeier, K.P.; Allan, C.L. CRP, IL-6 and depression: A systematic review and meta-analysis of longitudinal studies. J. Affect. Disord. 2013, 150, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.; Tam, W.W.; Zhang, M.W.; Ho, C.S.; Husain, S.F.; McIntyre, R.S.; Ho, R.C. IL-1β, IL-6, TNF-α and CRP in elderly patients with depression or Alzheimer’s disease: Systematic review and meta-analysis. Sci. Rep. 2018, 8, 12050. [Google Scholar] [CrossRef] [PubMed]
- Haapakoski, R.; Mathieu, J.; Ebmeier, K.P.; Alenius, H.; Kivimäki, M. Cumulative meta-analysis of interleukins 6 and 1β, tumour necrosis factor α and C-reactive protein in patients with major depressive disorder. Brain Behav. Immun. 2015, 49, 206–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wium-Andersen, M.K.; Ørsted, D.D.; Nielsen, S.F.; Nordestgaard, B.G. Elevated C-Reactive Protein Levels, Psychological Distress, and Depression in 73 131 Individuals. JAMA Psychiatry 2013, 70, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Khandaker, G.M.; Pearson, R.M.; Zammit, S.; Lewis, G.; Jones, P.B. Association of Serum Interleukin 6 and C-Reactive Protein in Childhood With Depression and Psychosis in Young Adult Life: A Population-Based Longitudinal Study. JAMA Psychiatry 2014, 71, 1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osimo, E.F.; Baxter, L.J.; Lewis, G.; Jones, P.B.; Khandaker, G.M. Prevalence of low-grade inflammation in depression: A systematic review and meta-analysis of CRP levels. Psychol. Med. 2019, 49, 1958–1970. [Google Scholar] [CrossRef]
- O’Brien, S.M.; Scully, P.; Fitzgerald, P.; Scott, L.V.; Dinan, T.G. Plasma cytokine profiles in depressed patients who fail to respond to selective serotonin reuptake inhibitor therapy. J. Psychiatr. Res. 2007, 41, 326–331. [Google Scholar] [CrossRef]
- Yang, C.; Wardenaar, K.J.; Bosker, F.J.; Li, J.; Schoevers, R.A. Inflammatory markers and treatment outcome in treatment resistant depression: A systematic review. J. Affect. Disord. 2019, 257, 640–649. [Google Scholar] [CrossRef]
- Tuglu, C.; Kara, S.H.; Caliyurt, O.; Vardar, E.; Abay, E. Increased serum tumor necrosis factor-alpha levels and treatment response in major depressive disorder. Psychopharmacology 2003, 170, 429–433. [Google Scholar] [CrossRef]
- Mosiołek, A.; Pięta, A.; Jakima, S.; Zborowska, N.; Mosiołek, J.; Szulc, A. Effects of Antidepressant Treatment on Peripheral Biomarkers in Patients with Major Depressive Disorder (MDD). J. Clin. Med. 2021, 10, 1706. [Google Scholar] [CrossRef] [PubMed]
- Köhler-Forsberg, O.; Lydholm, C.N.; Hjorthøj, C.; Nordentoft, M.; Mors, O.; Benros, M.E. Efficacy of anti-inflammatory treatment on major depressive disorder or depressive symptoms: Meta-analysis of clinical trials. Acta Psychiatr. Scand. 2019, 139, 404–419. [Google Scholar] [CrossRef] [PubMed]
- Więdłocha, M.; Marcinowicz, P.; Krupa, R.; Janoska-Jaździk, M.; Janus, M.; Debowska, W.; Mosiołek, A.; Waszkiewicz, N.; Szulc, A. Effect of antidepressant treatment on peripheral inflammation markers—A meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 80, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Raison, C.L.; Rutherford, R.E.; Woolwine, B.J.; Shuo, C.; Schettler, P.; Drake, D.F.; Haroon, E.; Miller, A.H. A Randomized Controlled Trial of the Tumor Necrosis Factor Antagonist Infliximab for Treatment-Resistant Depression: The Role of Baseline Inflammatory Biomarkers. JAMA Psychiatry 2013, 70, 31. [Google Scholar] [CrossRef]
- Köhler, O.; Benros, M.E.; Nordentoft, M.; Farkouh, M.E.; Iyengar, R.L.; Mors, O.; Krogh, J. Effect of Anti-inflammatory Treatment on Depression, Depressive Symptoms, and Adverse Effects: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Psychiatry 2014, 71, 1381. [Google Scholar] [CrossRef] [PubMed]
- Eyre, H.A.; Air, T.; Proctor, S.; Rositano, S.; Baune, B.T. A critical review of the efficacy of non-steroidal anti-inflammatory drugs in depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2015, 57, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Kappelmann, N.; Lewis, G.; Dantzer, R.; Jones, P.; Khandaker, G. Antidepressant activity of anti-cytokine treatment: A systematic review and meta-analysis of clinical trials of chronic inflammatory conditions. Mol. Psychiatry 2016, 23, 335–343. [Google Scholar] [CrossRef] [Green Version]
- Bekhbat, M.; Chu, K.; Le, N.-A.; Woolwine, B.J.; Haroon, E.; Miller, A.H.; Felger, J.C. Glucose and lipid-related biomarkers and the antidepressant response to infliximab in patients with treatment-resistant depression. Psychoneuroendocrinology 2018, 98, 222–229. [Google Scholar] [CrossRef]
- Bavaresco, D.V.; Uggioni, M.L.R.; Ferraz, S.D.; Marques, R.M.M.; Simon, C.S.; Dagostin, V.S.; Grande, A.J.; da Rosa, M.I. Efficacy of infliximab in treatment-resistant depression: A systematic review and meta-analysis. Pharmacol. Biochem. Behav. 2020, 188, 172838. [Google Scholar] [CrossRef]
- Arteaga-Henríquez, G.; Simon, M.S.; Burger, B.; Weidinger, E.; Wijkhuijs, A.; Arolt, V.; Birkenhager, T.K.; Musil, R.; Müller, N.; Drexhage, H.A. Low-Grade Inflammation as a Predictor of Antidepressant and Anti-Inflammatory Therapy Response in MDD Patients: A Systematic Review of the Literature in Combination With an Analysis of Experimental Data Collected in the EU-MOODINFLAME Consortium. Front. Psychiatry 2019, 10, 458. [Google Scholar] [CrossRef]
- Zhu, C.-B.; Blakely, R.D.; Hewlett, W.A. The Proinflammatory Cytokines Interleukin-1beta and Tumor Necrosis Factor-Alpha Activate Serotonin Transporters. Neuropsychopharmacology 2006, 31, 2121–2131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geerlings, M.I.; Bouter, L.M.; Schoevers, R.A.; Beekman, A.T.F.; Jonker, C.E.E.S.; Deeg, D.J.H.; Schmand, B. Depression and risk of cognitive decline and Alzheimer’s disease. Results of two prospective community-based studies in The Netherlands. Br. J. Psychiatry 2000, 176, 568–575. [Google Scholar] [CrossRef]
- Ozawa, K.; Hashimoto, K.; Kishimoto, T.; Shimizu, E.; Ishikura, H.; Iyo, M. Immune Activation During Pregnancy in Mice Leads to Dopaminergic Hyperfunction and Cognitive Impairment in the Offspring: A Neurodevelopmental Animal Model of Schizophrenia. Biol. Psychiatry 2006, 59, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Capuron, L.; Miller, A.H. Immune system to brain signaling: Neuropsychopharmacological implications. Pharmacol. Ther. 2011, 130, 226–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagawa, K.; Yoshino, H.; Ogawa, Y.; Yamamuro, K.; Kimoto, S.; Noriyama, Y.; Makinodan, M.; Yamashita, M.; Saito, Y.; Kishimoto, T. Maternal Immune Activation Affects Hippocampal Excitatory and Inhibitory Synaptic Transmission in Offspring From an Early Developmental Period to Adulthood. Front. Cell. Neurosci. 2020, 14, 241. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-W.; Chun, W.; Lee, H.J.; Kim, S.-M.; Min, J.-H.; Kim, D.-Y.; Kim, M.-O.; Ryu, H.W.; Lee, S.U. The Role of Microglia in the Development of Neurodegenerative Diseases. Biomedicines 2021, 9, 1449. [Google Scholar] [CrossRef]
Figure 1.
PRISMA Flow Diagram [44].
Figure 1.
PRISMA Flow Diagram [44].
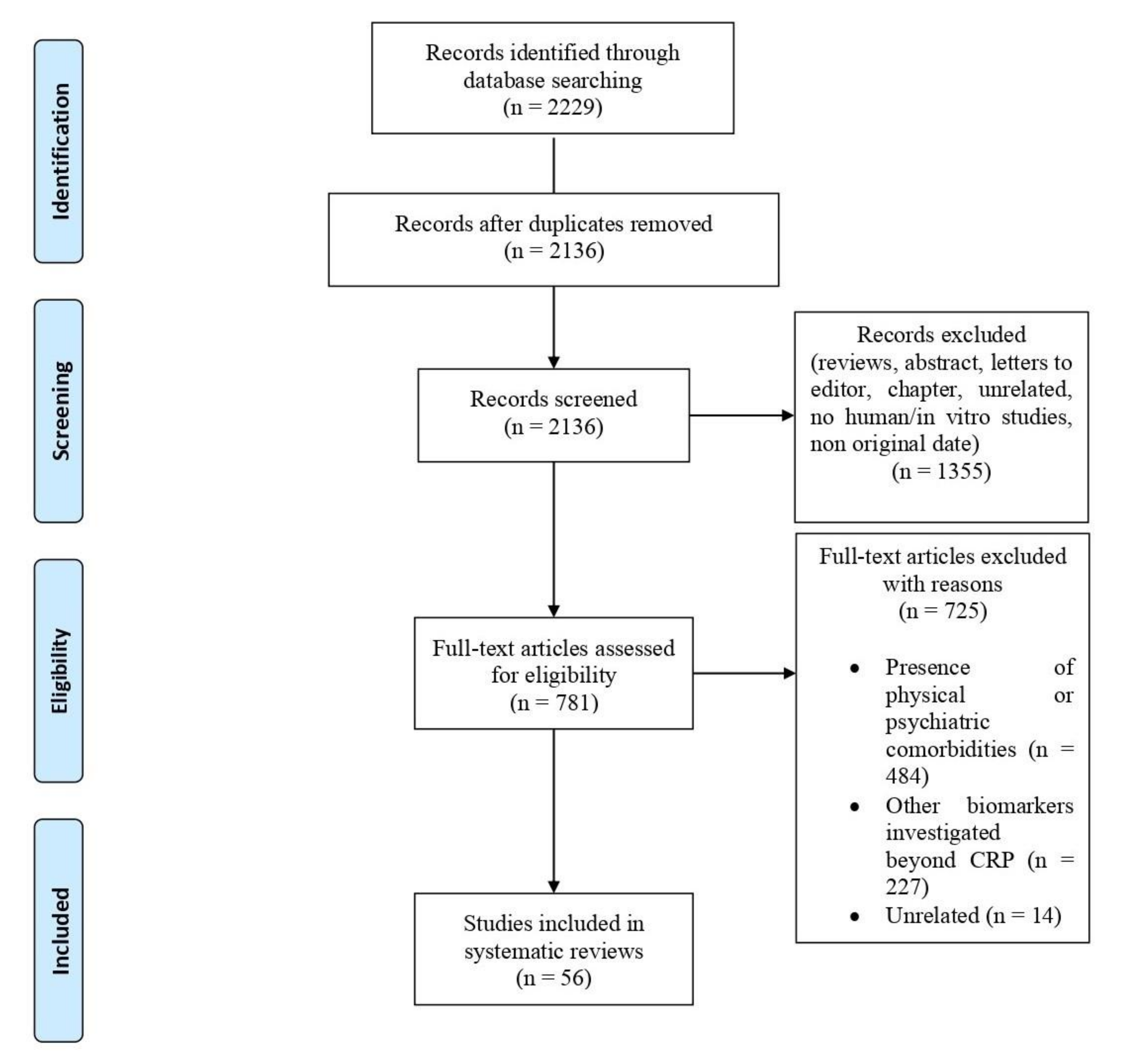

{kind=link}
Table 1.
Summary of included studies.
| Study | Study Design | Primary and Secondary Outcomes | Participants Characteristics | Assessment | Main Findings | Is There an Association between CRP Levels and Depression? |
|---|---|---|---|---|---|---|
| [45] | Cross-sectional study (Australia) | To determine if polymorphisms of SNPs rs1130864 and rs1205 are associated with prevalent depression | 3700 men aged > or = 70 years |
|
|
|
| [46] | Cross-sectional study (France) | Association between variants in the CRP gene that influence protein levels and depression | 990 people aged at least 65 years |
|
|
|
| [47] | Cross-sectional study (Italy) | To compare CRP (i.e., serum CRP > 3 and ≤10 mg/L) in patients with MDD, BD and OCD | 388 inpatients, (156 MDD, 135 BD, 97 OCD) |
|
|
|
| [48] | Cross-sectional study (USA) | To evaluate whether specific symptoms clusters are strongly associated with CRP levels and if race/ethnicity may affect this association | 10,149 adults who participated to the NHANES |
|
|
|
| [49] | Cross-sectional study (Canada) | To examine the association between hs-CRP concentrations and depressive symptoms in youth | 1535 adolescents (aged 13–16) |
|
|
|
| [50] | Cross-sectional study (China) | To evaluate the association between CRP, depressive symptoms and cognitive impairment in MDD patients treated with antidepressants (venlafaxine and fluoxetine) for 6 weeks | 149 MDD subjects (M = 42 F = 107) |
|
|
|
| [51] | Cross-sectional study (USA) | Association between social integration, race/ethnicity, inflammation, and depressive symptoms | 5634 participants aged 40 and older from the NHANES |
|
|
|
| [52] | Cross-sectional study (Republic of Korea) | Examine the association between serum hs-CRP levels and depressive symptoms in adults and explore the potential moderating effects of age, sex, BMI, and aerobic physical activity on the association between hsCRP levels and depression | 10,702 Adults (≥19 years) (M = 4746; F = 5956) |
|
|
|
| [53] | Cross-sectional study (Italy) | To investigate the effects of agomelatine on CRP levels in MDD patients and whether CRP variations are associated with clinical improvement | 30 adult MDD outpatients (M = 12 F = 18) |
|
|
|
| [54] | Cross sectional study (Finland) | To evaluate whether depression is independently associated with elevated CRP levels | 6000 Finns aged > 30 years (M = 2784F = 3257) |
|
|
|
| [55] | Cross-sectional study (USA) | To determine the association between MDD and elevated CRP levels in a nationally representative US cohort | 6914 noninstitutionalized (M = 3154 F = 3760) aged 18–39 yy |
|
|
|
| [56] | Cross-sectional study (USA) | To investigate whether the combination between CRP levels and depression is associated with worse executive functioning | 43,896 adults aged 44.13 years |
|
|
|
| [57] | Cross-sectional study (USA) | To explore whether plasma CRP levels may covary with depressive symptomatology as a function of allelic variation in the CRP gene | 868 healthy community volunteers |
|
|
|
| [58] | Cross-sectional study (US) | To evaluate the association between depression subtypes with inflammatory state | 19 atypical MDD patients, 93 non-atypical MDD, 1682 without MDD |
|
|
|
| [59] | Cross-sectional study (China) | To assess the difference in serum hs-CRP levels between BD-I and MDD | 23 MDD13 BD-I (manic episodes)31 healthy controls |
|
|
|
| [60] | Cross-sectional study (UK) | Associations of CRP and psychological distress mediated by antidepressants, supporting an inflammatory depression subtype | 10,363 UK adults aged 16–98 |
|
|
|
| [61] | Cross-sectional study (Republic of Korea) | To examine the association between hs-CRP levels and depression | 5447 participants coming from KNHANES VII-1 study |
|
|
|
| [62] | Cross-sectional study (USA) | To determine the association between hs-CRP levels and depression in a large sample of healthy adults | 26,638 healthy adults |
|
|
|
| [63] | Cross-sectional study (Germany) | To evaluate the association between CRP levels and depression severity, including specific depressive symptoms | 231 MDD patients (F = 142 M = 89) recruited from GENDEP study |
|
|
|
| [64] | Cross-sectional study | To evaluate the sex difference in the relationship between CRP and depression | 5483 Korean adults (2373 men and 3110 women) recruited from KNHANES |
|
|
|
| [65] | Cross-sectional study (China) | To explore whether CRP SNPs are related to depressive symptoms and antidepressants efficacy | 440 patients with first-episode depression |
|
|
|
| [66] | Cross-sectional study (Finland) | To investigate whether depressive episodes are associated in both genders with hs-CRP levels | 5269 participants (M = 2641 F = 2828) |
|
|
|
| [67] | Cross-sectional study (Finland) | Association between hs-CRP levels and depressed mood among the elderly | 764 subjects aged 70 years or older |
|
|
|
| [68] | Cross-sectional study (Brazil) | To investigate relationship between serum CRP levels and depression | 14,821 participants recruited from ELSA-Brazil study |
|
|
|
| [69] | Cross-sectional study (USA) | To investigate the possible association between inflammation and a specific phenotype of depression | 4157 participants from NHANES (F = 51.3%) with mean age of 47.59 |
|
|
|
| [70] | Cross-sectional study (Czech Republic) | To confirm the possible association between depression and CRP levels | 6126 individuals (45–69 yy) (M = 2829; F = 3297) |
|
|
|
| [71] | Cross-sectional study (Republic of Korea) | Association between CRP levels and depressive symptoms in an elderly Korean population | 569 (M = 224 F = 345) recruited from Korean Social Life, Health and Aging Project Health Examination Cohort aged 60 or over |
|
|
|
| [72] | Cross-sectional study (Iran) | Association between serum hs-CRP levels and depression score in adolescent girls | 563 adolescent girls aged 12–18 years |
|
|
|
| [73] | Cross-sectional study (USA) | To find a possible association between inflammation and specific depressive symptoms | 5909 patients recruited from ELSA |
|
|
|
| [74] | Cross-sectional study (Poland) | To determine whether there are differences in CRP levels between different psychiatric disorder | 458 schizophrenia patients 319 unipolar depression 146 BD 114 BD depression 32 BD mania |
|
|
|
| [75] | Cross-sectional study (Sri Lanka) | To consider the extent to which shared genetic and environmental factors may contribute to the association between CRP levels and depression | 2577 twins and 899 singletons |
|
|
|
| [76] | Cross-sectional study (China) | Possible associations between CRP levels and depressive symptoms among the middle-aged and elderly in China | 9459 Chinese middle-aged and elderly individuals (M = 4404F = 5055 selected on the CHARLS |
|
|
|
| [77] | Cross-sectional study (UK) | Association between CRP levels and a worse response to escitalopram and better response to nortriptyline in consideration of genetic disposition to inflammation | 755 unrelated individuals |
|
|
|
| [78] | Case-control study (UK) | To explore CRP levels in MDD and its phenotypic associations | 102 TRD patients with MDD currently experiencing depression, 48 treatment-responsive patients with MDD not currently experiencing depression, 48 patients with depression who were not receiving medication, and 54 healthy volunteers |
|
|
|
| [79] | Case-control study (China) | To examine whether CRP levels could be used to differentiate between MDD and BD II | 96 healthy controls, 88 BD-II and 72 MDD drug-naïve patients in their major depressive episode |
|
|
|
| [80] | Case-control Study (UK) | To identify a distinct phenotypic profile of depression associated with inflammation | 84 depressed patient divided in two group: with inflammation (CRP ≥ 3 mg/L) (N = 40) and without inflammation (CRP < 3 mg/L) (N = 44) |
|
|
|
| [81] | Case-control study (India) | To compare CRP levels in late-onset depression compared with age-matched healthy controls and evaluate whether (any) association between CRP levels and depressive symptoms severity | 25 patients aged ≥ 55 years with a first depressive episode and 27 age matched healthy controls |
|
|
|
| [82] | Case-control study (USA) | To examine CRP levels in depressive disorders and evaluate the impact of SSRI | A two-part study:1–32 patients with history of depression (20 currently depressed, 12 euthymic) treated with SSRI and 20 healthy comparison group2-CRP measured in 20 MDD patients both before and after SSRI treatment |
|
|
|
| [83] | Case-control study (UK) | To assess the inflammation in MDD subjects through CRP levels and the possible association with genetic, lifestyle, and phenotypic factors | 26,894 MDD patients and 59,000 healthy controls |
|
|
|
| [84] | Case-control study (China) | Correlation of clinical features with hs-CRP levels in TRD patients | 103 TRD and 103 non-TRD patients |
|
|
|
| [85] | Case-control study (China) | Considering CRP SNPs could regulate plasma CRP levels, the study hypothesized that inherited CRP allelic variations may covary with depressive symptomatology | 60 depression patients with family depression history and 60 healthy control volunteers |
|
|
|
| [86] | Case-control study (Poland) | To determine differences regarding CRP levels between elderly patients with unipolar depression and healthy controls | 404 patients (202 with unipolar depression202 healthy controls) |
|
|
|
| [87] | Case-control study (China) | To investigate whether inherited CRP allelic variations may co-vary with depressive symptoms | 200 patients (100 MDD, with or without family depression history and 100 healthy controls) |
|
|
|
| [88] | Cohort study | Association between CRP levels and depressive symptomatology among older adults | 3397 participants from the English Longitudinal Study of Ageing |
|
|
|
| [89] | Cohort study(USA) | To compare the effect of current depression with the effect of cumulative episodes of depression on the CRP levels | 1334 children, adolescents, and young adults |
|
|
|
| [40] | Cohort study (Brazil) | To evaluate the association between persistent depressive symptoms and the onset of low-grade inflammation | 1508 young individuals (134 with persistent depressive symptoms and 1374 negative at BDI) |
|
|
|
| [90] | Cohort study (USA) | Association between depression and hs-CRP levels | 508 healthy adults (F = 49%, mean age 48.5 yy) |
|
|
|
| [91] | Cohort study (The Netherlands) | To assess whether depression and apathy had different etiologiesin the elderly | 599 elderly subjects assessed annually form age 85 to 90 |
|
|
|
| [92] | Cohort study (USA) | Association between depressive symptoms and CRP levels in mid-life women | 3302 pre- and early perimenopausal women |
|
|
|
| [29] | Cohort Study (UK) | To evaluate if increasing levels of CRP in childhood and/or early-adulthood is associated with the risk of depression in early-adulthood | 1561 participants (M = 770; F = 791) |
|
|
|
| [93] | Cohort study (Australia) | Association between CRP levels and increased risk of de novo MDD | 1494 randomly selected women |
|
|
|
| [94] | Cohort Study | To examine long-term patterns of systemic inflammation in aging adults and determined whether individuals with chronic elevations in inflammation were at increased risk for having symptoms of depression as older adults | 4476 participants (mean age: 75.5(SD = 5.1)) M = 1775; F = 2701 |
|
|
|
| [95] | Cohort study (China) | To test whether baseline serum CRP levels could predict antidepressant treatment responses | 75 adult inpatients (M = 26 F = 49) with major MDD |
|
|
|
| [96] | RCT (Australia) | To measure the efficacy of anti-inflammatory augmentation of antidepressant treatment in MDD patients and whether treatment response was dependent on baseline inflammation levels | 119 MDD |
|
|
|
| [97] | RCT (USA) | To evaluate the sex differences in the association between CRP levels and the response to antidepressant treatments | 220 individuals (M = 75 F = 145) from EMBARC study |
|
|
|
| [98] | RCT | To test the hypothesis that CRP predicts differential response to escitalopram and nortriptyline | 241 MDD |
|
|
|
BD = bipolar disorder; BDI-II = Beck Depression Inventory; CAPA = Child and Adolescent Psychiatric Assessment; CESD = Center for Epidemiological Studies-Depression scale; CIS-R = Clinical Interview Schedule, Revised; CHARLS = Chine Health and Retirement Longitudinal Study; CIDI = Composite International Diagnostic Interview; CPT = Continuous Performance Test; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders-IV; ELSA = Longitudinal Study of Adult HealthEMARC = Establishing Moderators and Biosignature of Antidepressant Response for Clinical Care; FAST = Functioning Assessment Short Test; FTT = Finger-Tapping Test; GDS-15 = 15-item Geriatric Depression Scale; GENDEP = Genome-Based Therapeutic Drugs for Depression; GHQ = General Health Questionnaire score; HAMD17 = HDRS-17 = 17-item Hamilton Rating Scale for Depression 17; HARS = Hamilton Anxiety Rating Scale; hs-CRP = high sensitivity C-reactive protein; HSCL-25 = Hopkins Symptom Checklist-25; ICD-10 = International Classification of Disease 10th Revision; MADRS = Montgomery-Åsberg Depression Rating Scale scores; MDD = Major depressive disorder; MINI = Mini-International Neuropsychiatric Interview; MMSE = Mini Mental State Examination; NHANES = National Health and Nutrition Examination Survey; OCD = obsessive compulsive disorder; PCS = physical component summary score of the SF-36 Health Survey; PDS = Psychological Distress Scale; PHQ-9: Patient health Questionnaire-9; PRS = Polygenic risk score; RCT = Randomized controlled trial; RFFT = Ruff Figural Fluency Test; SCID-I/NP = Structured Clinical Interview nonpatient version; SHAPS = Snaith-Hamilton Pleasure Scale; SNPs = single-nucleotide polymorphisms; SSRI = Selective Serotonin Reuptake Inhibitor; SZSRDS = Short Zung Self Rating Depression Scale; THINC-It = THINC-Integrated Tool; TRD = treatment resistant depression; WCST = Wisconsin Card-Sorting Test; YAPA = Young and Adult Psychiatric Assessment.
Table 2.
Quality of the included studies, based on modified version of the Newcastle-Ottawa Quality Assessment Scale, adapted for cross-sectional studies.
Table 2.
Quality of the included studies, based on modified version of the Newcastle-Ottawa Quality Assessment Scale, adapted for cross-sectional studies.
| Study | Selection | Comparability | Outcome | Overall | ||||
|---|---|---|---|---|---|---|---|---|
| Representativeness of the sample | Sample size | Non-respondents | Ascertainment of depression | Based on design and analysis | Assessment of the outcome | Statistical test | ||
| [70] | * | / | / | * | * | ** | * | 6 |
| [61] | * | * | / | * | ** | ** | * | 8 |
| [52] | * | / | * | * | ** | ** | * | 8 |
| [58] | * | / | / | ** | ** | ** | * | 7 |
| [47] | / | / | / | * | ** | ** | * | 6 |
| [59] | * | / | / | ** | * | ** | * | 7 |
| [74] | * | / | / | * | * | ** | * | 6 |
| [49] | * | / | / | * | ** | ** | * | 7 |
| [50] | / | / | * | * | / | ** | * | 5 |
| [68] | * | / | / | * | ** | ** | * | 7 |
| [76] | * | / | * | * | ** | ** | * | 8 |
| [62] | * | * | / | * | ** | ** | * | 8 |
| [75] | * | / | / | ** | ** | ** | * | 8 |
| [54] | * | * | / | * | ** | ** | * | 8 |
| [64] | * | * | / | * | ** | ** | * | 8 |
| [71] | * | / | / | * | ** | ** | * | 7 |
| [55] | * | * | / | * | ** | ** | * | 8 |
| [66] | * | * | * | * | ** | ** | * | 9 |
| [67] | * | / | / | * | * | ** | * | 6 |
| [63] | * | / | / | * | ** | ** | * | 7 |
| [72] | * | / | / | * | ** | ** | * | 7 |
| [51] | * | * | / | * | ** | ** | * | 7 |
| [48] | * | / | / | * | ** | ** | * | 7 |
| [73] | * | / | / | * | ** | ** | * | 7 |
| [69] | * | / | / | * | / | ** | * | 5 |
| [56] | * | * | / | * | ** | ** | * | 9 |
| [57] | * | / | / | * | ** | ** | * | 7 |
| [65] | * | / | / | * | ** | ** | * | 7 |
| [45] | * | / | / | * | ** | ** | * | 7 |
| [46] | * | / | / | * | ** | ** | * | 7 |
| [60] | * | * | / | * | ** | ** | * | 8 |
| [53] | * | / | / | * | ** | ** | * | 7 |
| [77] | * | / | / | * | * | ** | * | 6 |
Note: /: 0 point; *: 1 point; **: 2 points.
Table 3.
Quality of the included studies, based on modified version of the Newcastle-Ottawa Quality Assessment Scale, adapted for case-control studies.
Table 3.
Quality of the included studies, based on modified version of the Newcastle-Ottawa Quality Assessment Scale, adapted for case-control studies.
| Study | Selection | Comparability | Exposure | Overall | |||||
|---|---|---|---|---|---|---|---|---|---|
| Is the case definition adequate? | Representativeness of the case | Selection of controls | Definition of controls | Based on design or analysis | Ascertainment of exposure | Same method ascertainment | Non- response rate | ||
| [80] | * | * | / | / | * | * | * | / | 5 |
| [83] | * | * | * | * | ** | * | * | / | 8 |
| [81] | * | * | * | * | * | * | * | / | 7 |
| [79] | * | / | * | / | * | * | * | / | 5 |
| [86] | * | / | * | * | * | * | * | / | 6 |
| [87] | * | / | / | * | * | * | * | / | 5 |
| [85] | * | / | * | * | * | * | * | / | 6 |
| [84] | * | * | * | / | * | * | * | / | 6 |
| [78] | * | / | * | * | ** | * | * | / | 7 |
| [82] | * | / | / | * | * | / | * | / | 5 |
Note: /: 0 point; *: 1 point; **: 2 points.
Table 4.
Quality of the included studies, based on modified version of the Newcastle-Ottawa Quality Assessment Scale, adapted for cohort studies.
Table 4.
Quality of the included studies, based on modified version of the Newcastle-Ottawa Quality Assessment Scale, adapted for cohort studies.
| Study | Selection | Comparability | Outcome | Overall | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the exposed cohort | Selection of the non-exposed cohort | Ascertainment of exposure | Outcome was not present at start | Based on design and analysis | Assessment of outcome | Enough follow-up | Adequacy of follow-up | ||
| [29] | * | * | * | / | ** | * | * | * | 8 |
| [94] | * | * | * | / | ** | * | * | * | 8 |
| [100] | / | * | * | * | ** | * | * | / | 7 |
| [89] | / | * | * | / | ** | * | * | * | 7 |
| [88] | * | * | * | / | ** | * | * | * | 8 |
| [90] | / | * | * | / | ** | * | * | * | 7 |
| [92] | * | * | * | / | ** | * | * | * | 8 |
| [93] | * | * | * | / | ** | * | * | * | 8 |
| [91] | * | * | * | / | / | + | * | * | 6 |
| [95] | / | * | * | / | * | * | / | * | 5 |
Note: /: 0 point; *: 1 point; **: 2 points.
Table 5.
Quality of the included studies, based on modified version of the Newcastle-Ottawa Quality Assessment Scale, adapted for RCT.
Table 5.
Quality of the included studies, based on modified version of the Newcastle-Ottawa Quality Assessment Scale, adapted for RCT.
| Study | Selection | Comparability | Outcome | Overall | |||||
|---|---|---|---|---|---|---|---|---|---|
| Is the case definition adequate? | Representativeness of the case | Selection of control | Definition of control | Based on design and analysis | Assessment of exposure | Same method ascertainment | Non- response rate | ||
| [97] | * | * | * | * | ** | * | * | / | 8 |
| [98] | * | * | * | * | * | * | * | / | 7 |
| [96] | * | * | * | * | * | * | * | / | 7 |
Note: /: 0 point; *: 1 point; **: 2 points.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Orsolini, L.; Pompili, S.; Tempia Valenta, S.; Salvi, V.; Volpe, U. C-Reactive Protein as a Biomarker for Major Depressive Disorder? Int. J. Mol. Sci. 2022, 23, 1616. https://doi.org/10.3390/ijms23031616
AMA Style
Orsolini L, Pompili S, Tempia Valenta S, Salvi V, Volpe U. C-Reactive Protein as a Biomarker for Major Depressive Disorder? International Journal of Molecular Sciences. 2022; 23(3):1616. https://doi.org/10.3390/ijms23031616
Chicago/Turabian StyleOrsolini, Laura, Simone Pompili, Silvia Tempia Valenta, Virginio Salvi, and Umberto Volpe. 2022. "C-Reactive Protein as a Biomarker for Major Depressive Disorder?" International Journal of Molecular Sciences 23, no. 3: 1616. https://doi.org/10.3390/ijms23031616
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.