
Using a Polygenic Score to Predict the Risk of Developing Primary Osteoporosis

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
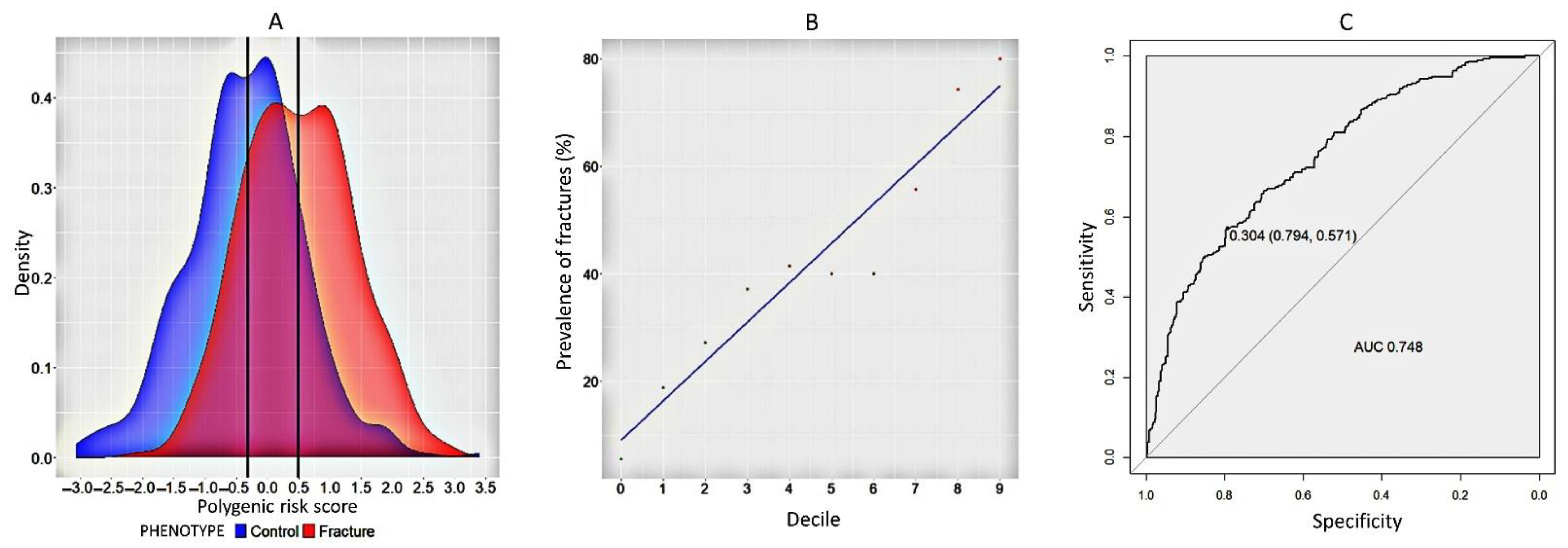
2.1. Model for Predicting Fracture Risk in Women
2.2. Model to Predict the Formation of Low BMD in Women
2.3. A Model to Predict Fractures and Low BMD in Comorbid Women
3. Discussion
4. Methods and Materials
4.1. Phenotypic Information
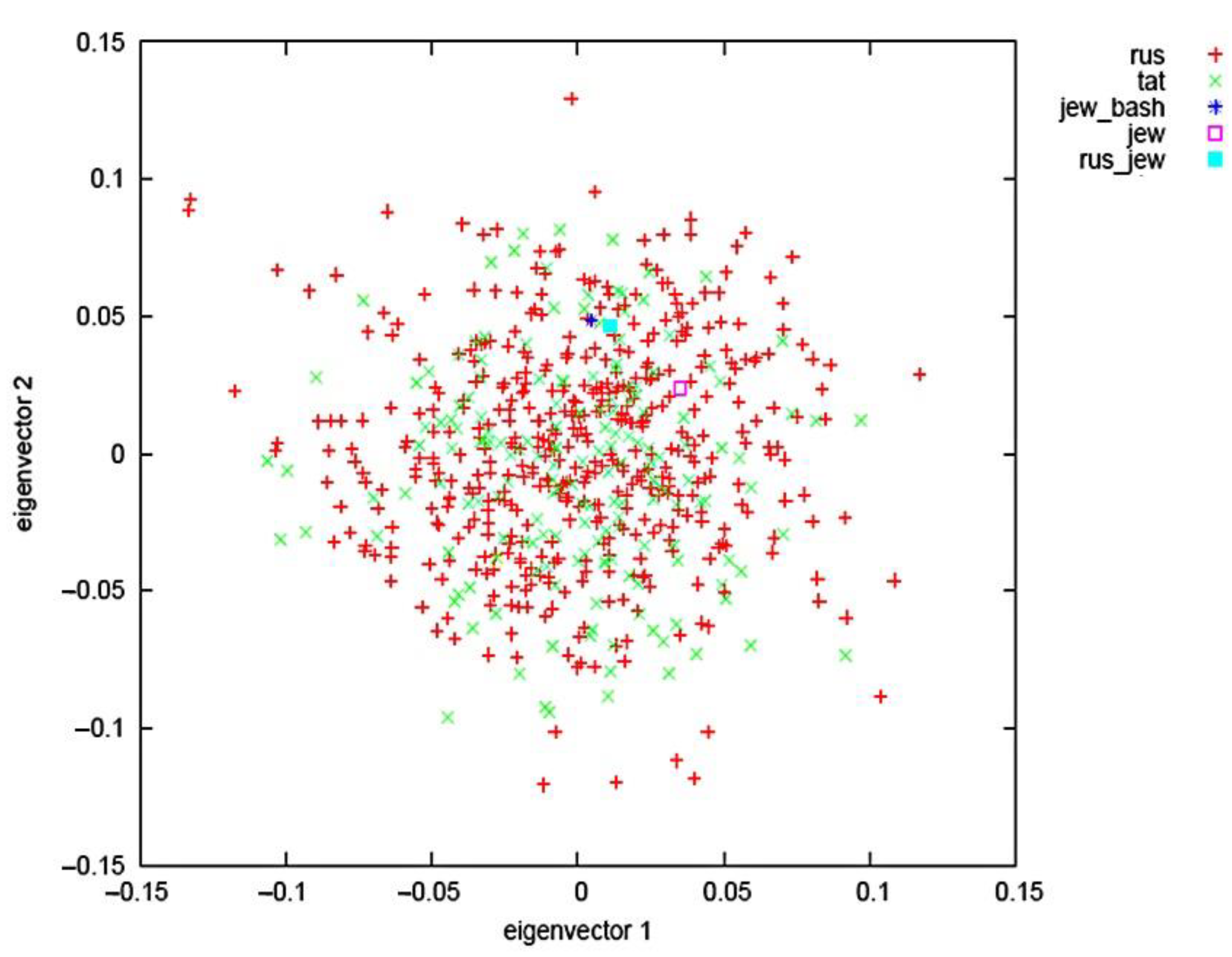
4.2. Genetic Data, Quality Control and Analysis
4.3. Statistical Analysis
- Quality control of baseline data with the exclusion of polymorphic loci that are linkage disequilibrium and do not support the Hardy-Weinberg equilibrium.
- Analysis of polygenic risk assessment.
- PGS specificity and sensitivity analysis using ROC-analysis.
- The search for the most sensitive and specific model of polygenic fracture risk and low BMD was completed on the basis of ROC-analysis on the basis of RStudio, in which the sensitivity and specificity of the model as well as the AUC, a numerical index of the area under the ROC-curve, were assessed.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanis, J.; Cooper, C.; Rizzoli, R.; Reginster, J. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2019, 30, 3–44. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.A.; John, P.K.; Scott, E.Y.; Laetitia, L.; John, G.L.; Ryan, C.C.; Nicholas, A.V.; Forgetta, V.; Kleinman, A.; Mohanty, S.T.; et al. An atlas of genetic influences on osteoporosis in humans and mice. Nat. Genet. 2019, 51, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, M.B.; Buckwalter, J.; Saltzman, C. Osteoporosis: The increasing role of the orthopaedist. Iowa Orthop. J. 1999, 19, 43–52. [Google Scholar] [PubMed]
- Panday, K.; Gona, A.; Humphrey, M.B. Medication-induced osteoporosis: Screening and treatment strategies. Ther. Adv. Musculoskelet Dis. 2014, 6, 185–202. [Google Scholar] [CrossRef]
- Hanxuan, L.; Zhousheng, X.; Quarles, L.D.; Wei, L. Osteoporosis: Mechanism, molecular target and current status on drug development. Curr. Med. Chem. 2020, 28, 1489–1507. [Google Scholar] [CrossRef]
- Wiedl, A.; Stefan, F.; Annabel, F.; Edgar, M. Fractures’ associated mortality risk in orthogeriatric inpatients: A Prospective 2-year survey. Eur. Geriatr. Med. 2021, 1, 61–68. [Google Scholar] [CrossRef]
- Marshall, D.; Johnell, O.; Wedel, H. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. Br. Med. J. 1996, 312, 1254–1259. [Google Scholar] [CrossRef]
- Estrada, K.; Styrkarsdottir, U.; Evangelou, E.; Hsu, Y.H.; Duncan, E.L.; Ntzani, E.E.; Oei, L.; Albagha, O.M.; Amin, N.; Kemp, J.P.; et al. Genome-wide meta-analysis identifies 56 bone mineral density loci and reveals 14 loci associated with risk of fracture. Nat. Genet. 2012, 44, 491–501. [Google Scholar] [CrossRef]
- Khosla, S.; Hofbauer, L.C. Osteoporosis treatment: Recent developments and ongoing challenges. Lancet Diabetes Endocrinol. 2017, 5, 898–907. [Google Scholar] [CrossRef]
- Marie, P.J. Strontium ranelate: A dual mode of action rebalancing bone turnover in favour of bone formation. Curr. Opin. Rheumatol. 2006, 18, 11–15. [Google Scholar] [CrossRef]
- Bolland, M.J.; Siu, A.T.; Mason, B.H.; Horne, A.M.; Ames, R.W.; Grey, A.B.; Gamble, G.D.; Reid, I.R. Evaluation of the FRAX and Garvan fracture risk calculators in older women. J. Bone Miner. Res. 2011, 26, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, S.K.; Nguyen, N.D.; Center, J.R.; Pocock, N.A.; Eisman, J.A.; Nguyen, T.V. Prognosis of fracture: Evaluation of predictive accuracy of the FRAX algorithm and Garvan nomogram. Osteoporos. Int. 2010, 21, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Coupland, C. Derivation and validation of updated QFracture algorithm to predict risk of osteoporotic fracture in primary care in the United Kingdom: Prospective open cohort study. BMJ 2012, 344, 3427. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.-L.; Shen, H.; Liu, A.; Dong, S.-S.; Zhang, L.; Deng, F.-Y.; Zhao, Q.; Deng, H.-W. A road map for understanding molecular and genetic determinants of osteoporosis. Nat. Rev. Endocrinol. 2020, 16, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-J.; Zhang, L.; Papasian, C.J.; Deng, H.-W. Genome-wide association studies for osteoporosis: A 2013 update. J. Bone Metab. 2014, 21, 99–116. [Google Scholar] [CrossRef]
- Khusnutdinova, E.K.; Victorova, T.V.; Fatkchlislamova, R.I.; Galeyeva, A.R. Relative contributions of the caucasoid and mongoloid components to the formation of ethnic groups of the Volga-Ural region as estimated from DNA polymorphism. Genetika. 1999, 35, 1132–1137. [Google Scholar]
- Lewis, C.M.; Evangelos, V. Polygenic risk scores: From research tools to clinical instruments. Genome Med. 2020, 12, 44. [Google Scholar] [CrossRef]
- Torkamani, A.; Wineinger, N.E.; Topol, E.J. The personal and clinical utility of polygenic risk scores. Nat. Rev. Genet. 2018, 19, 581–590. [Google Scholar] [CrossRef]
- Lambert, S.A.; Abraham, G.; Inouye, M. Towards clinical utility of polygenic risk scores. Hum. Mol. Genet. 2019, 28, R133–R142. [Google Scholar] [CrossRef]
- Lu, T.; Forgetta, V.; Keller-Baruch, J.; Nethander, M.; Bennett, D.; Forest, M.; Bhatnagar, S.; Walters, R.G.; Lin, K.; Chen, Z.; et al. Improved prediction of fracture risk leveraging a genome-wide polygenic risk score. Genome Med. 2021, 13, 1–15. [Google Scholar] [CrossRef]
- Kim, S.K. Identification of 613 new loci associated with heel bone mineral density and a polygenic risk score for bone mineral density, osteoporosis and fracture. PLoS ONE 2018, 13, e0200785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Schizophrenia Consortium; Purcell, S.M.; Wray, N.R.; Stone, J.L.; Visscher, P.M.; O’Donovan, M.C.; Sullivan, P.F.; Sklar, P. Common polygenic variation contributes to risk of schizophrenia that overlaps with bipolar disorder. Nature 2009, 460, 748. [Google Scholar] [CrossRef] [PubMed]
- Heslot, N.; Jannink, J.L.; Sorrells, M.E. Perspectives for genomic selection applications and research in plants. Crop Sci. 2015, 55, 1–12. [Google Scholar] [CrossRef]
- Hayr, M.K.; Druet, T.; Garrick, D.J. 027 Performance of genomic prediction using haplotypes in New Zealand dairy cattle. J. Anim. Sci. 2016, 94, 13. [Google Scholar] [CrossRef]
- Natarajan, P.; Young, R.; Stitziel, N.O.; Padmanabhan, S.; Baber, U.; Mehran, R.; Sartori, S.; Fuster, V.; Reilly, D.F.; Butterworth, A.; et al. Polygenic risk score identifies subgroup with higher burden of atherosclerosis and greater relative benefit from statin therapy in the primary prevention setting. Circulation 2017, 135, 2091–2101. [Google Scholar] [CrossRef]
- Schunkert, H.; Samani, N.J. Statin treatment: Can genetics sharpen the focus? Lancet 2015, 385, 2227–2229. [Google Scholar] [CrossRef]
- Duncan, L.; Shen, H.; Gelaye, B.; Meijsen, J.; Ressler, K.; Feldman, M.; Peterson, R.; Domingue, B. Analysis of polygenic risk score usage and performance in diverse human populations. Nat. Commun. 2019, 10, 3328. [Google Scholar] [CrossRef]
- Li, Y.M.; Peng, C.; Zhang, J.G.; Zhu, W.; Xu, C.; Lin, Y.; Fu, X.Y.; Tian, Q.; Zhang, L.; Xiang, Y.; et al. Genetic risk factors identified in populations of European descent do not improve the prediction of osteoporotic fracture and bone mineral density in Chinese populations. Sci. Rep. 2019, 9, 6086. [Google Scholar] [CrossRef]
- Forgetta, V.; Keller-Baruch, J.; Forest, M.; Durand, A.; Bhatnagar, S.; Kemp, J.P.; Nethander, M.; Evans, D.; Morris, J.A.; Kiel, D.P.; et al. Development of a polygenic risk score to improve screening for fracture risk: A genetic risk prediction study. PLoS Med. 2020, 17, e1003152. [Google Scholar] [CrossRef]
- Ho-Le, T.P.; Center, J.R.; Eisman, J.A.; Nguyen, H.T.; Nguyen, T.V. Prediction of bone mineral density and fragility fracture by genetic profiling. J. Bone Miner. Res. 2017, 32, 285–293. [Google Scholar] [CrossRef]
- Holtzman, N.A.; Marteau, T.M. Will genetics revolutionize medicine? N. Engl. J. Med. 2000, 343, 141–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, M.S.; Gu, J.W.; Morris, D.E. The potential of genes and other markers to inform about risk. Cancer Epidemiol. Biomarkers Prev. 2010, 19, 655. [Google Scholar] [CrossRef]
- Sugrue, L.P.; Desikan, R.S. What are polygenic scores and why are they important? JAMA 2019, 321, 1820–1821. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.V.; Eisman, J.A. Post-GWAS polygenic risk score: Utility and challenges. JMPR Plus 2020, 4, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lello, L.; Raben, T.G.; Yong, S.Y.; Tellier, L.C.A.M.; Hsu, S.D.H. Genomic prediction of 16 complex disease risks including heart attack, diabetes, breast and prostate cancer. Sci. Rep. 2019, 9, 15286. [Google Scholar] [CrossRef] [PubMed]
- Patterson, N.; Price, A.L.; Reich, D. Population structure and eigenanalysis. PLoS Genet. 2006, 2, 2074–2093. [Google Scholar] [CrossRef]
- Chang, C.C.; Chow, C.C.; Tellier, C.L.; Purcell, S.M.; Lee, J.J. Second-generation PLINK: Rising to the challenge of larger and richer datasets. Gigascience 2015, 4, 7. [Google Scholar] [CrossRef]
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef]
- Collister, J.A.; Liu, X.; Clifton, L. Calculating Polygenic Risk Scores (PRS) in UK Biobank: A Practical Guide for Epidemiologists. Front. Genet. 2022, 13, 818574. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Woman | ||
|---|---|---|---|
| N | |||
| With fractures | 294 | 62.16 ± 7.95 | 27.00 ± 3.60 |
| Without fractures | 407 | 60.14 ± 8.01 | 27.80 ± 3.81 |
| With low BMD | 324 | 62.17 ± 7.95 | 27.04 ± 3.60 |
| With normal BMD | 172 | 60.23 ± 7.97 | 28.10 ± 4.90 |
| With low BMD and with fractures | 177 | 60.15 ± 7.43 | 27.00 ± 2.40 |
| With normal BMD and without fracture | 260 | 61.76 ± 7.96 | 28.90 ± 3.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yalaev, B.; Tyurin, A.; Prokopenko, I.; Karunas, A.; Khusnutdinova, E.; Khusainova, R. Using a Polygenic Score to Predict the Risk of Developing Primary Osteoporosis. Int. J. Mol. Sci. 2022, 23, 10021. https://doi.org/10.3390/ijms231710021
Yalaev B, Tyurin A, Prokopenko I, Karunas A, Khusnutdinova E, Khusainova R. Using a Polygenic Score to Predict the Risk of Developing Primary Osteoporosis. International Journal of Molecular Sciences. 2022; 23(17):10021. https://doi.org/10.3390/ijms231710021
Chicago/Turabian StyleYalaev, Bulat, Anton Tyurin, Inga Prokopenko, Aleksandra Karunas, Elza Khusnutdinova, and Rita Khusainova. 2022. "Using a Polygenic Score to Predict the Risk of Developing Primary Osteoporosis" International Journal of Molecular Sciences 23, no. 17: 10021. https://doi.org/10.3390/ijms231710021