
Bare Metal Stents on Resveratrol-Coated Balloons in Porcine Coronary and Peripheral Arteries

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Pharmacokinetics
2.2. Histological Analysis
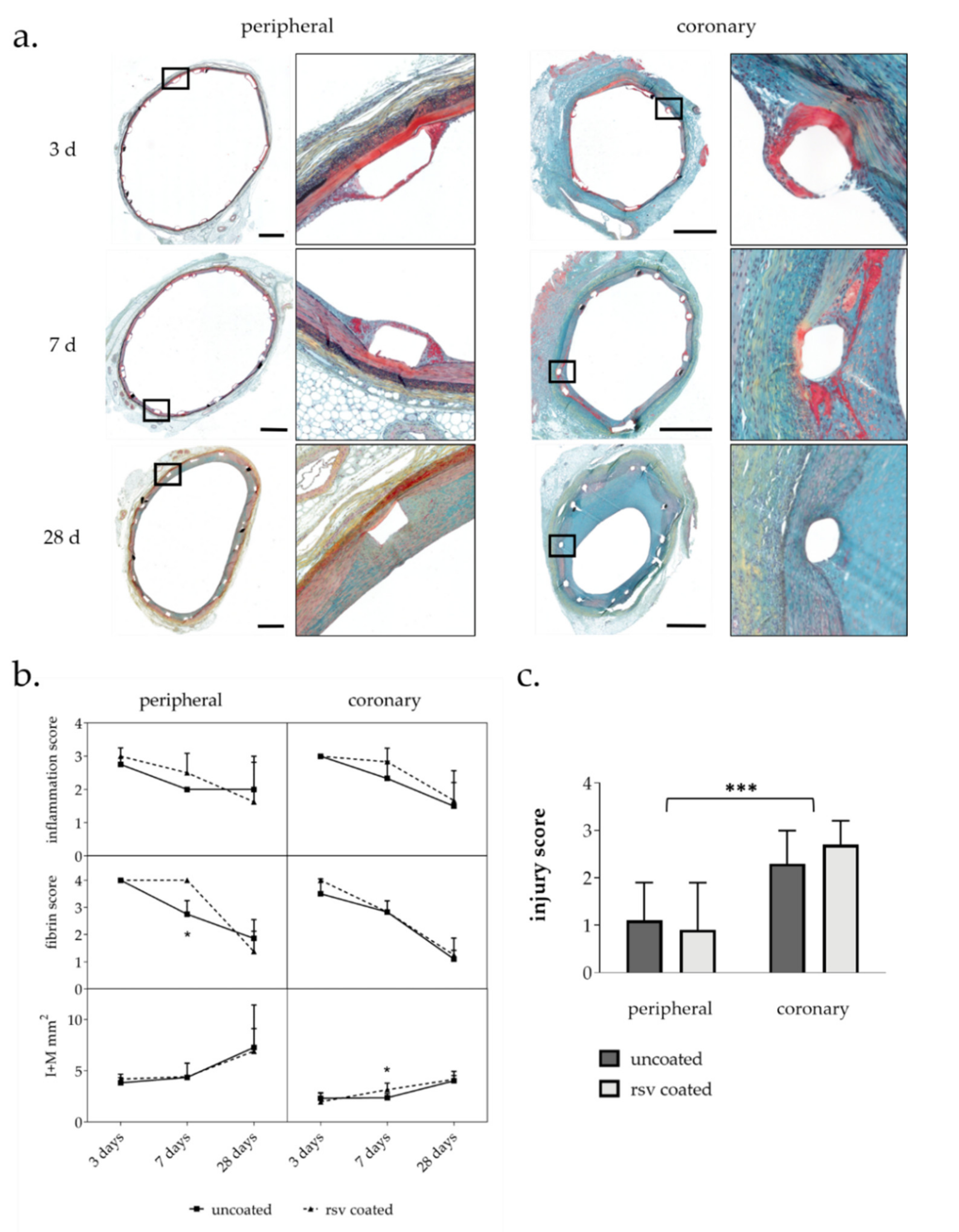
2.2.1. Injury Score and Morphometry
2.2.2. Inflammation Score and Fibrin Score
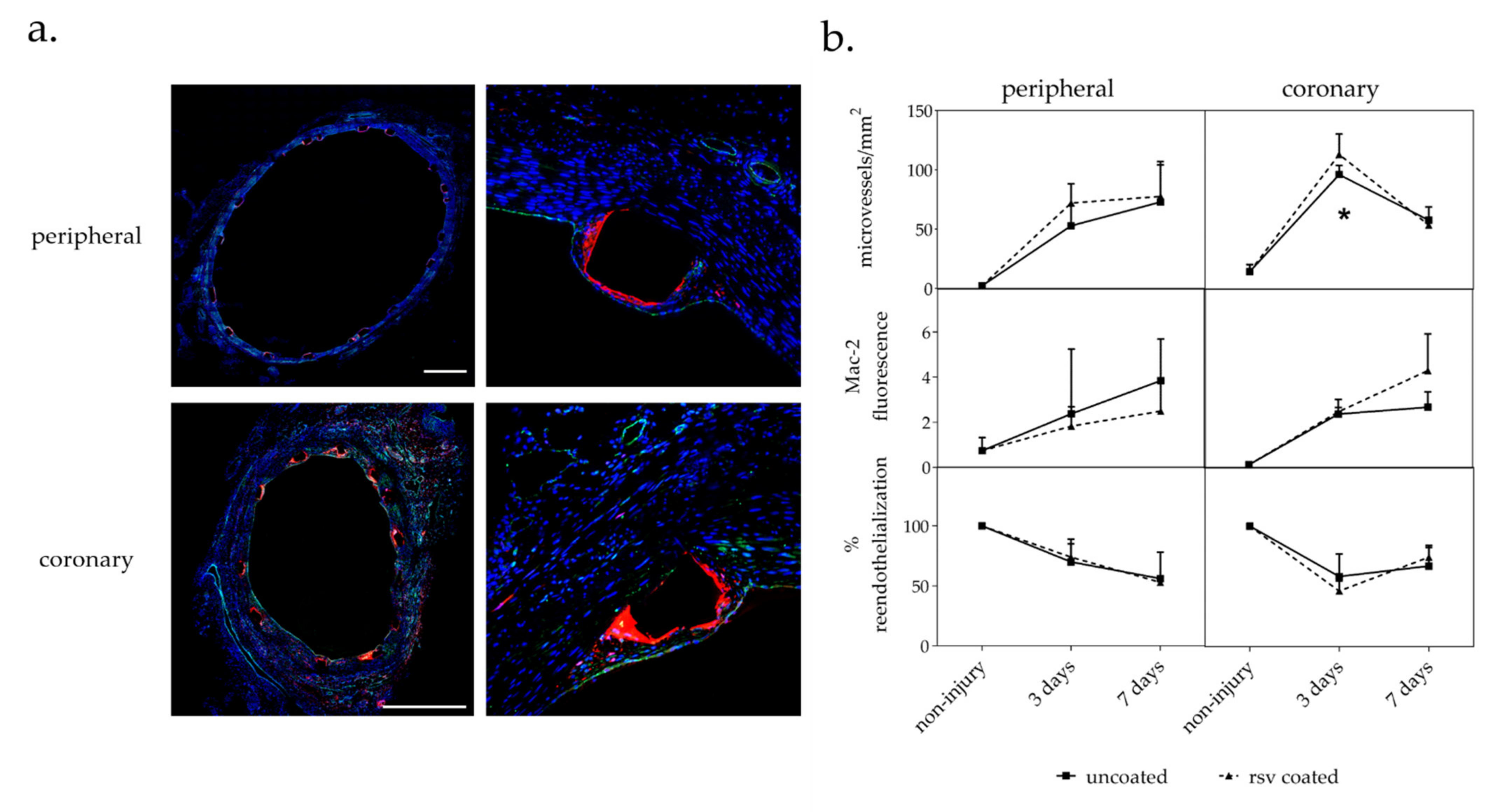
2.3. Immunohistochemical Analysis
2.3.1. Vasa Vasorum Neovascularization
2.3.2. Macrophages
2.3.3. Reendothelialization
3. Discussion
4. Materials and Methods
4.1. Catheter Preparation
4.2. Animal Experiments
4.3. Resveratrol Analysis by HPLC-UV
4.4. Histochemistry and Morphometry
4.5. Immunohistochemistry
4.6. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Animals | Survival | Artery Type | Staining Method | Vessels (Uncoated, RSV Coated) | Section Levels | Sections per Level | Sections Total |
|---|---|---|---|---|---|---|---|
| 4 | 3 d | peripheral | Movat | 4, 4 | 1 | 1 | 8 |
| Mac-2/CD31 | 4, 4 | 1 | 2 | 16 | |||
| coronary | Movat | 6, 6 | 1 | 1 | 12 | ||
| Mac-2/CD31 | 6, 6 | up to 3 | up to 4 | 43 | |||
| 4 | 7 d | peripheral | Movat | 4, 4 | 1 | 1 | 8 |
| Mac-2/CD31 | 4, 4 | 1 | 2 | 16 | |||
| coronary | Movat | 6, 6 | 1 | 1 | 12 | ||
| Mac-2/CD31 | 4, 6 | up to 3 | up to 4 | 32 | |||
| 8 | 28 d | peripheral | Movat | 7, 8 | 1 | 1 | 15 |
| coronary | Movat | 11, 12 | 1 | 1 | 23 |
References
- Clever, Y.; Cremers, B.; Krauß, B.; Böhm, M.; Speck, U.; Laufs, U.; Scheller, B. Paclitaxel and sirolimus differentially affect growth and motility of endothelial progenitor cells and coronary artery smooth muscle cells. EuroIntervention 2011, 7, K32–K42. [Google Scholar] [CrossRef]
- Iakovou, I.; Schmidt, T.; Bonizzoni, E.; Ge, L.; Sangiorgi, G.; Stankovic, G.; Airoldi, F.; Chieffo, A.; Montorfano, M.; Carlino, M.; et al. Incidence, Predictors, and Outcome of Thrombosis After Successful Implantation of Drug-Eluting Stents. JAMA 2005, 293, 2126–2130. [Google Scholar] [CrossRef] [PubMed]
- McFadden, E.P.; Stabile, E.; Regar, E.; Cheneau, E.; Ong, A.T.; Kinnaird, T.; Suddath, W.O.; Weissman, N.J.; Torguson, R.; Kent, K.M.; et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet 2004, 364, 1519–1521. [Google Scholar] [CrossRef]
- Speck, U.; Häckel, A.; Schellenberger, E.; Kamann, S.; Löchel, M.; Clever, Y.P.; Peters, D.; Scheller, B.; Trog, S.; Bettink, S. Drug Distribution and Basic Pharmacology of Paclitaxel/Resveratrol-Coated Balloon Catheters. Cardiovasc. Interv. Radiol. 2018, 41, 1599–1610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albrecht, T.; Waliszewski, M.; Roca, C.; Redlich, U.; Tautenhahn, J.; Pech, M.; Halloul, Z.; Gögebakan, Ö.; Meyer, D.-R.; Gemeinhardt, I.; et al. Two-Year Clinical Outcomes of the CONSEQUENT Trial: Can Femoropopliteal Lesions be Treated with Sustainable Clinical Results that are Economically Sound? Cardiovasc. Interv. Radiol. 2018, 41, 1008–1014. [Google Scholar] [CrossRef] [PubMed]
- Tepe, G.; Gögebakan, O.; Redlich, U.; Tautenhahn, J.; Ricke, J.; Halloul, Z.; Meyer, D.-R.; Waliszewski, M.; Schnorr, B.; Zeller, T. Angiographic and Clinical Outcomes After Treatment of Femoro-Popliteal Lesions with a Novel Paclitaxel-Matrix-Coated Balloon Catheter. Cardiovasc. Intervent. Radiol. 2017, 40, 1535–1544. [Google Scholar] [CrossRef]
- Scicchitano, P.; Cameli, M.; Maiello, M.; Modesti, P.A.; Muiesan, M.L.; Novo, S.; Palmiero, P.; Saba, P.S.; Pedrinelli, R.; Ciccone, M.M. Nutraceuticals and dyslipidaemia: Beyond the common therapeutics. J. Funct. Foods 2014, 6, 11–32. [Google Scholar] [CrossRef]
- Tome-Carneiro, J.; Gonzalves, M.; Larossa, M.; Yanez-Gascon, M.; Garcia-Almagro, F.J.; Ruiz-Ros, J.A.; Garcia-Conesa, M.T.; Barberan, T.; Espin, J.E. One-year consumption of a grape nutraceutical containing resveratrol improves the inflammatory and fibrinolytic status of patients in primary prevention of cardiovascular disease. Am. J. Cardiol. 2012, 110, 356–363. [Google Scholar] [CrossRef]
- Zou, J.; Huang, Y.; Cao, K.; Yang, G.; Yin, H.; Len, J.; Hsieh, T.-C.; Wu, J.M. Effect of resveratrol on intimal hyperplasia after endothelial denudation in an experimental rabbit model. Life Sci. 2000, 68, 153–163. [Google Scholar] [CrossRef]
- Yurdagul, A., Jr.; Kleinedler, J.J.; McInnis, M.C.; Khandelwal, A.R.; Spence, A.L. Resveratrol Promotes Endothelial Cell Wound Healing under Laminar Shear Stress Through an Estrogen Receptor-Alpha-Dependent Pathway. Am. J. Physiol. 2014, 306, H797–H806. [Google Scholar]
- Breen, D.; Dolinsky, V.W.; Zhang, H.; Ghanim, H.; Guo, J.; Mroziewicz, M.; Tsiani, E.L.; Bendeck, M.P.; Dandona, P.; Dyck, J.R.; et al. Resveratrol inhibits neointimal formation after arterial injury through an endothelial nitric oxide synthase-dependent mechanism. Atherosclerosis 2012, 222, 375–381. [Google Scholar] [CrossRef]
- Khandelwal, A.R.; Hebert, V.Y.; Dugas, T.R. Essential role of ER-α-dependent NO production in resveratrol-mediated inhibition of restenosis. Am. J. Physiol. Circ. Physiol. 2010, 299, H1451–H1458. [Google Scholar] [CrossRef]
- Kleinedler, J.J.; Foley, J.D.; Orchard, E.A.; Dugas, T.R. Novel nanocomposite stent coating releasing resveratrol and quercetin reduces neointimal hyperplasia and promotes re-endothelialization. J. Control Release 2012, 159, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Shaito, A.; Posadino, A.M.; Younes, N.; Hasan, H.; Halabi, S.; Alhababi, D.; Al-Mohannadi, A.; Abdel-Rahman, W.M.; Eid, A.H.; Nasrallah, G.K.; et al. Potential Adverse Effects of Resveratrol: A Literature Review. Int. J. Mol. Sci. 2020, 21, 2084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gualdoni, G.A.; Kovarik, J.J.; Hofer, J.; Dose, F.; Pignitter, M.; Doberer, D.; Steinberger, P.; Somoza, V.; Wolzt, M.; Zlabinger, G.J. Resveratrol enhances TNF-α production in human monocytes upon bacterial stimulation. Biochim. Biophys. Acta (BBA) Gen. Subj. 2014, 1840, 95–105. [Google Scholar] [CrossRef]
- Li, H.; Xia, N.; Hasselwander, S.; Daiber, A. Resveratrol and Vascular Function. Int. J. Mol. Sci. 2019, 20, 2155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilgic, T. Comparison of the Effect of Local and Systemic Injection of Resveratrol on Cutaneous Wound Healing in Rats. Int. J. Low. Extrem. Wounds 2021, 20, 55–59. [Google Scholar] [CrossRef]
- Dugas, T.R.; Brewer, G.; Longwell, M.; Fradella, T.; Braun, J.; Astete, C.E.; Jennings, M.H.; Sabliov, C.M. Nanoentrapped polyphenol coating for sustained drug release from a balloon catheter. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 107, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Shamseddin, A.; Crauste, C.; Durand, E.; Villeneuve, P.; Dubois, G.; Pavlickova, T.; Durand, T.; Vercauteren, J.; Veas, F. Resveratrol-Linoleate protects from exacerbated endothelial permeability via a drastic inhibition of the MMP-9 activity. Biosci. Rep. 2018, 38, BSR20171712. [Google Scholar] [CrossRef] [Green Version]
- Kamann, S.; Haase, T.; Stolzenburg, N.; Löchel, M.; Peters, D.; Schnorr, J. Resveratrol-Coated Balloon Catheters in Porcine Coronary and Peripheral Arteries. Int. J. Mol. Sci. 2019, 20, 2285. [Google Scholar] [CrossRef] [Green Version]
- Scheller, B.; Speck, U.; Abramjuk, C.; Bernhardt, U.; Böhm, M.; Nickenig, G. Paclitaxel Balloon Coating, a Novel Method for Prevention and Therapy of Restenosis. Circulation 2004, 110, 810–814. [Google Scholar] [CrossRef] [PubMed]
- Galili, O.; Herrmann, J.; Woodrum, J.; Sattler, K.J.; Lerman, L.O.; Lerman, A. Adventitial vasa vasorum heterogeneity among different vascular beds. J. Vasc. Surg. 2004, 40, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Hildebrandt, H.A.; Gossl, M.; Mannheim, D.; Versari, D.; Herrmann, J.; Spendlove, D.; Bajanowski, T.; Malyar, N.M.; Erbel, R.; Lerman, L.O.; et al. Differential distribution of vasa vasorum in different vascular beds in humans. Atherosclerosis 2008, 199, 47–54. [Google Scholar] [CrossRef]
- Dong, S.; Hughes, R.C. Macrophage surface glycoproteins binding to galectin-3 (Mac-2-antigen). Glycoconj. J. 1997, 14, 267–274. [Google Scholar] [CrossRef]
- Tolva, V.; Mazzola, S.M.; Zerbi, P.; Casana, R.; Albertini, M.; Calvillo, L.; Selmin, F.; Cilurzo, F. A successful experimental model for intimal hyperplasia prevention using a resveratrol-delivering balloon. J. Vasc. Surg. 2016, 63, 788–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, K.R.; Andreadi, C.; Britton, R.G.; Horner-Glister, E.; Karmokar, A.; Sale, S.; Brown, V.A.; Brenner, D.E.; Singh, R.; Steward, W.P.; et al. Sulfate Metabolites Provide an Intracellular Pool for Resveratrol Generation and Induce Autophagy with Senescence. Sci. Transl. Med. 2013, 5, 205ra133. [Google Scholar] [CrossRef] [Green Version]
- Harikumar, K.; Aggarwal, B.B. Resveratrol: A multitargeted agent for age-associated chronic diseases. Cell Cycle 2008, 7, 1020–1035. [Google Scholar] [CrossRef] [Green Version]
- Naseem, K.M. The role of nitric oxide in cardiovascular diseases. Mol. Asp. Med. 2005, 26, 33–65. [Google Scholar] [CrossRef] [PubMed]
- Forstermann, U.; Munzel, T. Endothelial nitric oxide synthase in vascular disease: From marvel to menace. Circulation 2006, 113, 1708–1714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallerath, T.; Deckert, G.; Ternes, T.; Anderson, H.; Li, H.; Witte, K.; Förstermann, U. Resveratrol, a Polyphenolic Phytoalexin Present in Red Wine, Enhances Expression and Activity of Endothelial Nitric Oxide Synthase. Circulation 2002, 106, 1652–1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, N.; Daiber, A.; Habermeier, A.; Closs, E.; Thum, T.; Spanier, G.; Lu, Q.; Oelze, M.; Torzewski, M.; Lackner, K.J.; et al. Resveratrol Reverses Endothelial Nitric-Oxide Synthase Uncoupling in Apolipoprotein E Knockout Mice. J. Pharmacol. Exp. Ther. 2010, 335, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creasey, H.N.; Brandel, E.Z.; Nguyen, R.; Bashore, M.J.; Jones, C.M. Covalent attachment of resveratrol to stainless steel toward the development of a resveratrol-releasing bare-metal stent. J. Biomed. Mater. Res. Part B Appl. Biomater. 2020, 108, 2344–2353. [Google Scholar] [CrossRef] [PubMed]
- Tomé-Carneiro, J.; Gonzálvez, M.; Larrosa, M.; Yáñez-Gascón, M.J.; García-Almagro, F.J.; Ruiz-Ros, J.A.; Tomas-Barberan, F.; Conesa, M.T.G.; Espín, J.C. Grape Resveratrol Increases Serum Adiponectin and Downregulates Inflammatory Genes in Peripheral Blood Mononuclear Cells: A Triple-Blind, Placebo-Controlled, One-Year Clinical Trial in Patients with Stable Coronary Artery Disease. Cardiovasc. Drugs Ther. 2012, 27, 37–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinedler, J.J.; Foley, J.D.; Alexander, J.S.; Roerig, S.C.; Hebert, V.Y.; Dugas, T.R. Synergistic effect of resveratrol and quercetin released from drug-eluting polymer coatings for endovascular devices. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 99B, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Kelsch, B.; Scheller, B.; Biedermann, M.; Clever, Y.P.; Schaffner, S.; Mahnkopf, D.; Speck, U.; Cremers, B. Dose Response to Paclitaxel-Coated Balloon Catheters in the Porcine Coronary Overstretch and Stent Implantation Model. Investig. Radiol. 2011, 46, 255–263. [Google Scholar] [CrossRef] [PubMed]


| Study | Number of Animals | Survival Time | Vessel Type | Number of Vessels 1 | Total Dose on Balloon 2 | Dose per mm2 Balloon Surface |
|---|---|---|---|---|---|---|
| pharmacokinetic | 2 | 10 min | coronary | 6 | 1010 ± 74 µg | 4.0 ± 0.3 µg/mm2 |
| 2 | 1 d | coronary | 6 | 1010 ± 74 µg | 4.0 ± 0.3 µg/mm2 | |
| efficacy | 4 | 3 d | coronary | 6 | 1636 ± 29 µg | 6.5 ± 0.1 µg/mm2 |
| 6 | - | - | ||||
| peripheral | 4 | 9748 ± 396 µg | 6.9 ± 0.3 µg/mm2 | |||
| 4 | - | - | ||||
| 4 | 7 d | coronary | 6 | 1636 ± 29 µg | 6.5 ± 0.1 µg/mm2 | |
| 6 | - | - | ||||
| peripheral | 4 | 9748 ± 396 µg | 6.9 ± 0.3 µg/mm2 | |||
| 4 | - | - | ||||
| 8 | 28 d | coronary | 12 | 1636 ± 29 µg | 6.5 ± 0.1 µg/mm2 | |
| 12 | - | - | ||||
| peripheral | 8 | 9748 ± 396 µg | 6.9 ± 0.3 µg/mm2 | |||
| 8 | - | - |
| Survival | Vessel | Balloon Inflation Pressure ATM | µg Total | µg/g Tissue | % of Total Dose |
|---|---|---|---|---|---|
| 10 min | RCA | 10 | 37 | 150 | 3.7 |
| LAD | 8 | 19 | 79 | 1.9 | |
| LCX | 10 | 48 | 161 | 4.8 | |
| RCA | 12 | 24 | 92 | 2.4 | |
| LAD | 10 | 3 | 9 | 0.3 | |
| LCX | 10 | 40 | 147 | 4.0 | |
| mean ± SD | 29 ± 16 | 106 ± 58 | 2.8 ± 1.6 |
| Survival | Analysis Parameter | Peripheral | p-Value | Coronary 1 | p-Value | ||
|---|---|---|---|---|---|---|---|
| Uncoated | RSV Coated | Uncoated | RSV Coated | ||||
| 3 d | n-value | 4 | 4 | 6 | 6 | ||
| Injury score | 0.08 ± 0.03 | 0.06 ± 0.08 | 0.428 | 0.92 ± 0.73 | 0.91 ± 0.29 | 0.999 | |
| Inflammation score | 2.05 ± 0.30 | 2.20 ± 0.17 | 0.999 | 2.45 ± 0.25 | 1.97 ± 0.39 | 0.999 | |
| Fibrin score | 3.50 ± 0.26 | 3.28 ± 0.22 | 0.999 | 2.88 ± 0.50 | 3.29 ± 0.26 | 0.182 | |
| I + M (mm2) | 3.82 ± 0.51 | 4.19 ± 0.47 | 0.486 | 2.31 ± 0.50 | 1.97 ± 0.90 | 0.310 | |
| Macrophages | 2.37 ± 2.87 | 1.83 ± 0.86 | 0.686 | 2.38 ± 0.29 | 2.48 ± 0.55 | 0.818 | |
| % reendothelialization | 70 ± 19 | 74 ± 11 | 0.971 | 58 ± 19 | 46 ± 8 | 0.192 | |
| neovascularization | 52.98 ± 16.61 | 72.08 ± 16.17 | 0.343 | 96.25 ± 7.66 | 113.19 ± 17.26 | 0.041 * | |
| 7 d | n-value | 4 | 4 | 6 | 6 | ||
| Injury score | 0.18 ± 0.16 | 0.01 ± 0.03 | 0.485 | 0.98 ± 0.40 | 1.11 ± 0.43 | 0.197 | |
| Inflammation score | 1.44 ± 0.33 | 1.88 ± 0.37 | 0.429 | 1.61 ± 0.33 | 2.08 ± 0.57 | 0.242 | |
| Fibrin score | 1.92 ± 0.43 | 2.93 ± 0.50 | 0.029 * | 2.11 ± 0.42 | 2.09 ± 0.45 | 0.999 | |
| I + M (mm2) | 4.35 ± 1.39 | 4.41 ± 1.32 | 0.886 | 2.37 ± 0.40 | 3.15 ± 0.65 | 0.015 * | |
| Macrophages | 3.84 ± 1.85 | 2.49 ± 1.47 | 0.486 | 2.68 ± 0.69 | 4.30 ± 1.62 | 0.114 | |
| % reendothelialization | 56 ± 22 | 53 ± 25 | 0.914 | 67 ± 17 | 74 ± 8 | 0.914 | |
| neovascularization | 72.97 ± 34.07 | 77.67 ± 26.49 | 0.886 | 58.04 ± 11.27 | 53.89 ± 3.86 | 0.761 | |
| 28 d | n-value | 7 | 8 | 10 | 12 | ||
| Injury score | 0.29 ± 0.42 | 0.25 ± 0.28 | 0.814 | 1.53 ± 0.41 | 1.79 ± 0.51 | 0.213 | |
| Inflammation score | 1.21 ± 0.58 | 0.65 ± 0.50 | 0.587 | 0.90 ± 0.45 | 1.02 ± 0.70 | 0.839 | |
| Fibrin score | 0.70 ± 0.35 | 0.64 ± 0.30 | 0.215 | 0.64 ± 0.20 | 0.54 ± 0.16 | 0.857 | |
| I + M (mm2) | 7.27 ± 1.85 | 6.91 ± 4.50 | 0.232 | 4.01 ± 0.52 | 4.15 ± 0.79 | 0.892 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamann, S.; Haase, T.; Stolzenburg, N.; Löchel, M.; Peters-Berg, D.; Schütt, D.; Schnorr, J. Bare Metal Stents on Resveratrol-Coated Balloons in Porcine Coronary and Peripheral Arteries. Int. J. Mol. Sci. 2021, 22, 13099. https://doi.org/10.3390/ijms222313099
Kamann S, Haase T, Stolzenburg N, Löchel M, Peters-Berg D, Schütt D, Schnorr J. Bare Metal Stents on Resveratrol-Coated Balloons in Porcine Coronary and Peripheral Arteries. International Journal of Molecular Sciences. 2021; 22(23):13099. https://doi.org/10.3390/ijms222313099
Chicago/Turabian StyleKamann, Stefanie, Tobias Haase, Nicola Stolzenburg, Melanie Löchel, Daniel Peters-Berg, Denise Schütt, and Jörg Schnorr. 2021. "Bare Metal Stents on Resveratrol-Coated Balloons in Porcine Coronary and Peripheral Arteries" International Journal of Molecular Sciences 22, no. 23: 13099. https://doi.org/10.3390/ijms222313099