TGF–β3 Loaded Electrospun Polycaprolacton Fibre Scaffolds for Rotator Cuff Tear Repair: An in Vivo Study in Rats

 and
and 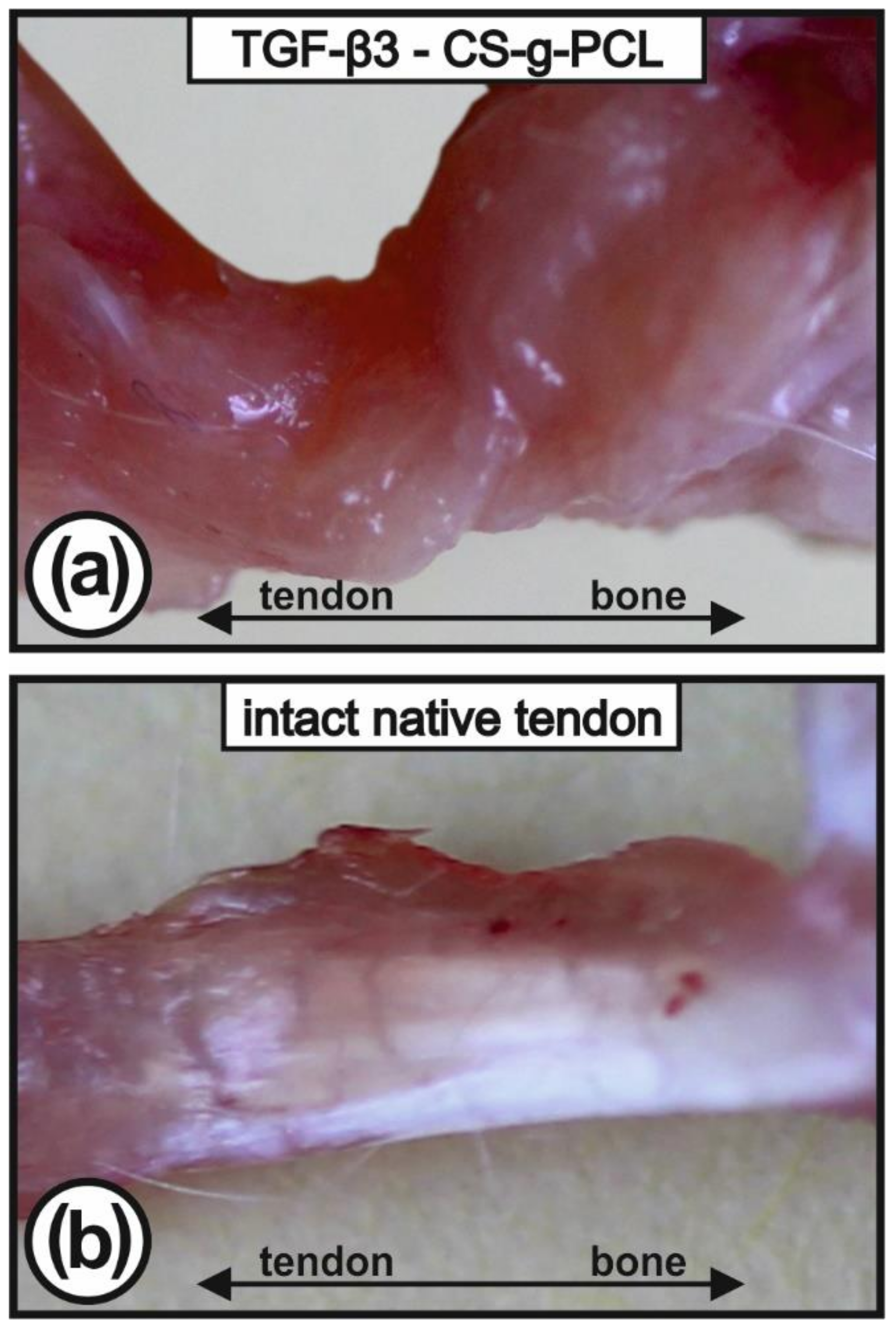{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Clinical Observations
2.2. Macroscopical Appearance of Tendon-to-Bone Interface
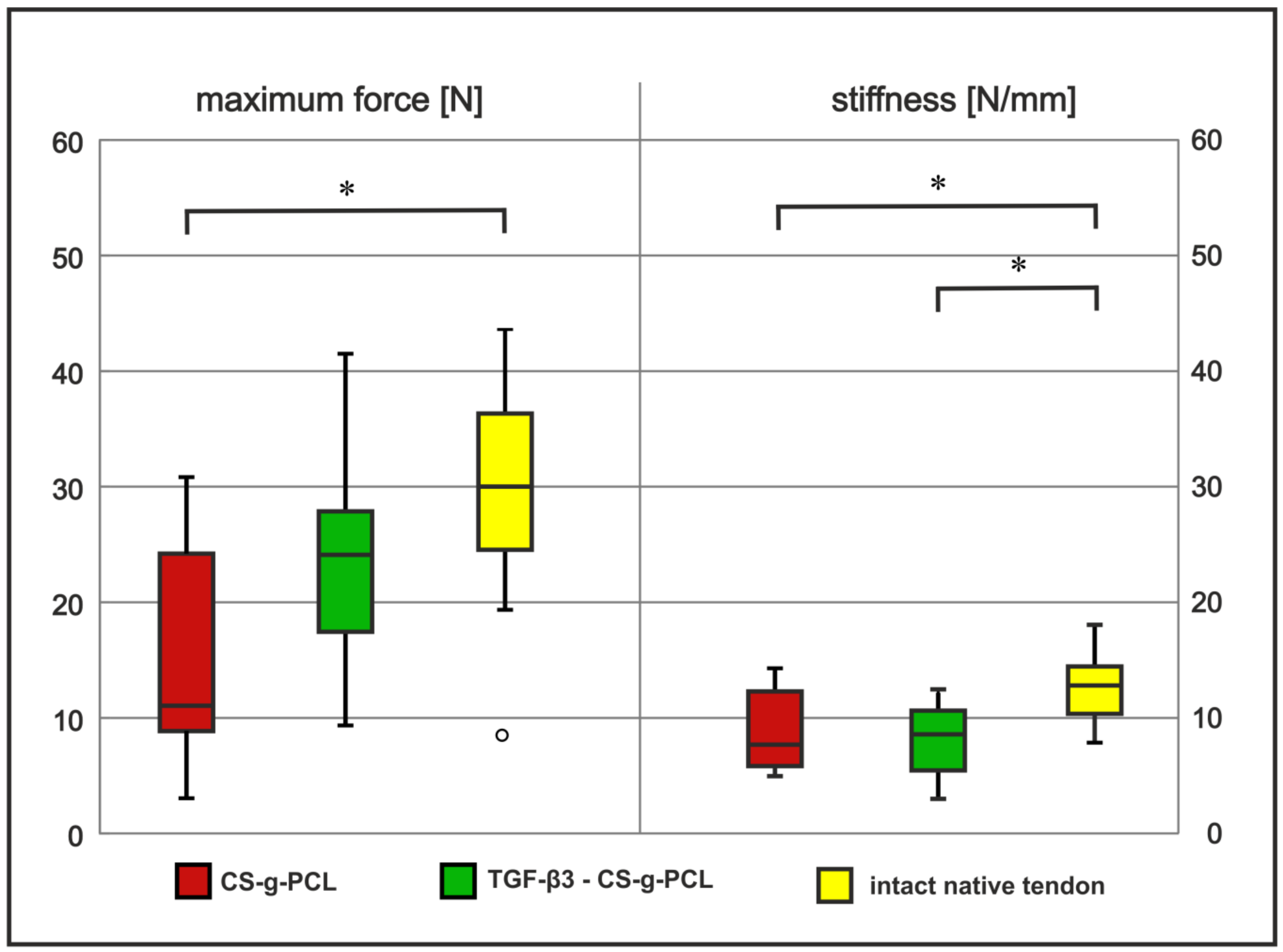
2.3. Tendon Healing in Rats: Biomechanical Testing
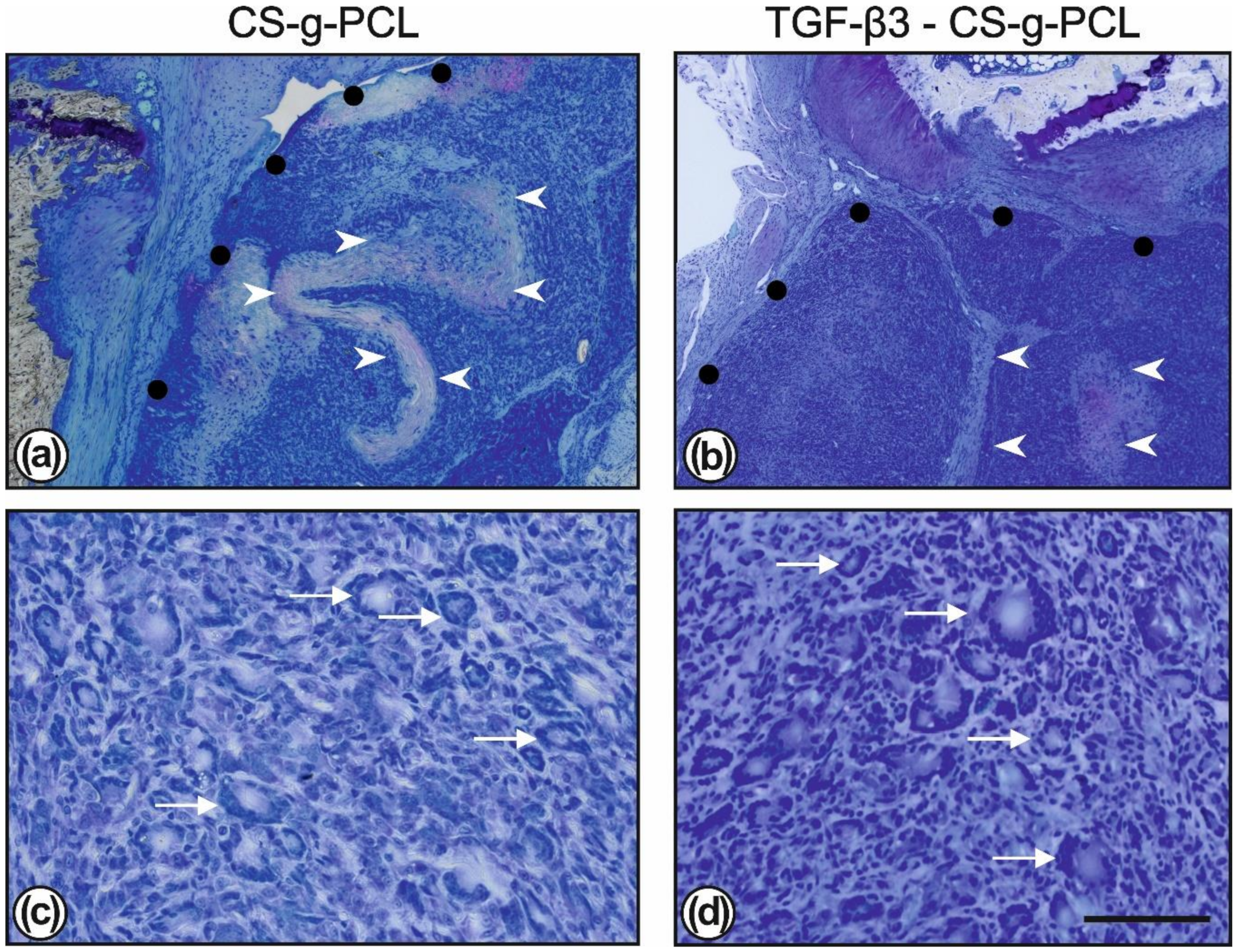
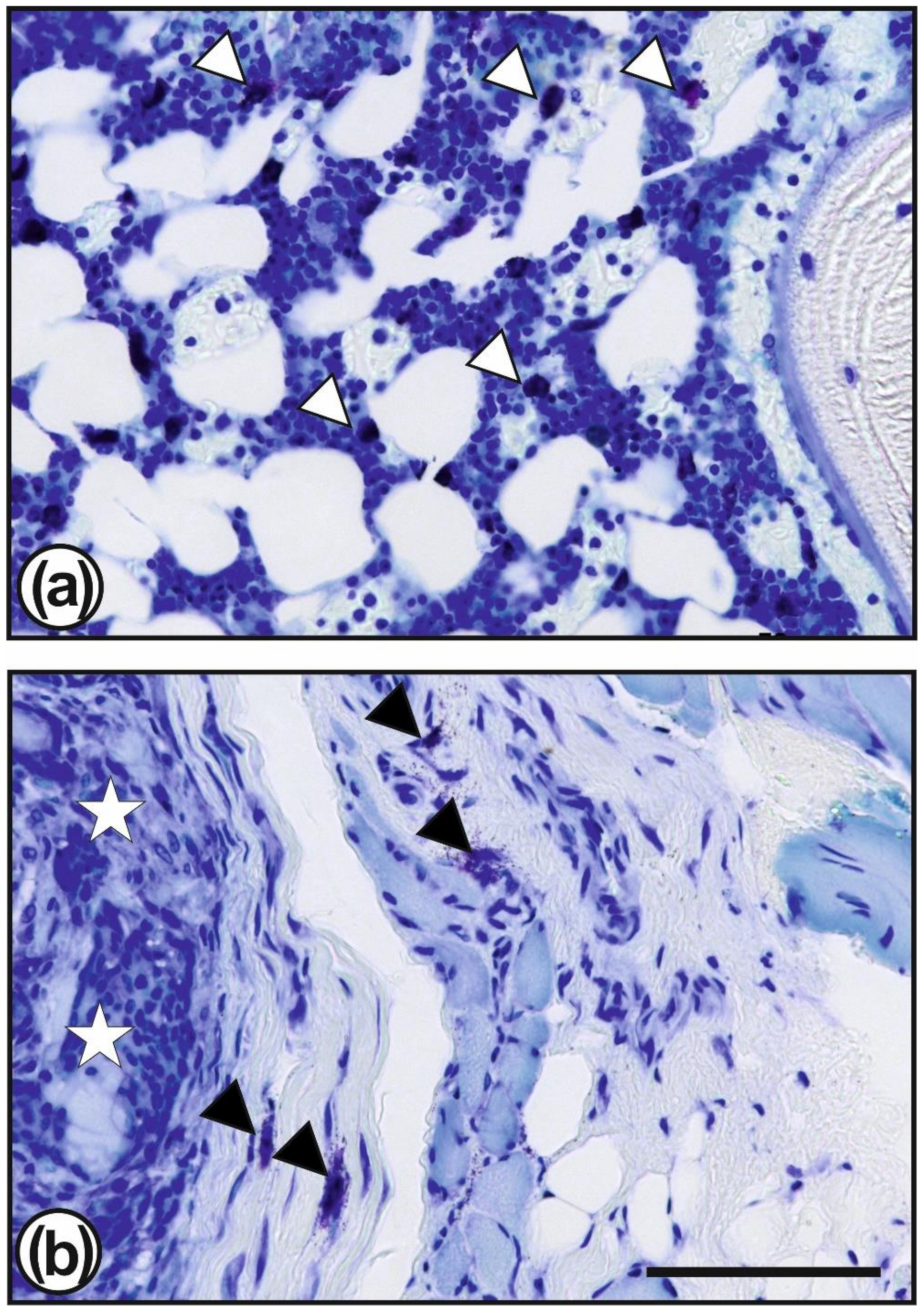
2.4. Tendon Healing in Rats: Histology
3. Discussion
4. Materials and Methods
4.1. CS–g–PCL Coated Fibre Scaffold
4.2. Sterilisation
4.3. Loading of the CS–g–PCL Coated PCL Fibre Scaffolds With TGF–β3
4.4. Animal Study
4.5. Biomechanical Testing
4.6. Embedding in Technovit® 9100 New
4.7. Toluidine Blue Staining
4.8. Chloroacetate Esterase Staining
4.9. Microscopy
4.10. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| TGF | Transforming Growth Factor |
| CS–g–PCL | chitosan coated polycaprolacton |
| PCL | chitosan coated polycaprolacton |
| Scx | Scleraxis |
| Tnmd | Tenomodulin |
| Sox9 | Transcription factor SOX-9 |
| Coll1α1 | Collagen 1α1 |
| Coll3α1 | Collagen 3α1 |
| MMP9 | Matrix metallopeptidase 9 |
| MMP13 | Matrix metallopeptidase 13 |
References
- Derwin, K.A.; Galatz, L.M.; Ratcliffe, A.; Thomopoulos, S. Enthesis repair: Challenges and opportunities for effective tendon-to-bone healing. J. Bone Joint Surg. Am. 2018, 100, e109. [Google Scholar]
- Yamamoto, A.; Takagishi, K.; Osawa, T.; Yanagawa, T.; Nakajima, D.; Shitara, H.; Kobayashi, T. Prevalence and risk factors of a rotator cuff tear in the general population. J. Shoulder Elbow Surg. 2010, 19, 116–120. [Google Scholar]
- Gumina, S.; Passaretti, D.; Candela, V. Epidemiology and demographics of the rotator cuff tear. In Rotator Cuff Tear; Gumina, S., Ed.; Pathogenesis, Evaluation and Treatment; Springer International Publishing: Cham, Switzerland, 2017; pp. 53–59. [Google Scholar]
- Laron, D.; Samagh, S.P.; Liu, X.; Kim, H.T.; Feeley, B.T. Muscle degeneration in rotator cuff tears. J. Shoulder Elbow Surg. 2012, 21, 164–174. [Google Scholar]
- Killian, M.L.; Cavinatto, L.M.; Ward, S.R.; Havlioglu, N.; Thomopoulos, S.; Galatz, L.M. Chronic degeneration leads to poor healing of repaired massive rotator cuff tears in rats. Am. J. Sports Med. 2015, 43, 2401–2410. [Google Scholar]
- Thorsness, R.; Romeo, A. Massive rotator cuff tears: Trends in surgical management. Orthopedics 2016, 39, 145–151. [Google Scholar]
- Rossi, L.A.; Rodeo, S.A.; Chahla, J.; Ranalletta, M. Current concepts in rotator cuff repair techniques: Biomechanical, functional, and structural outcomes. Orthop. J. Sports Med. 2019, 7, 2325967119868674. [Google Scholar]
- Le, B.T.N.; Wu, X.L.; Lam, P.H.; Murrell, G.A.C. Factors predicting rotator cuff retears: An analysis of 1000 consecutive rotator cuff repairs. Am. J. Sports Med. 2014, 42, 1134–1142. [Google Scholar]
- Ciampi, P.; Scotti, C.; Nonis, A.; Vitali, M.; Di Serio, C.; Peretti, G.M.; Fraschini, G. The benefit of synthetic versus biological patch augmentation in the repair of posterosuperior massive rotator cuff tears: A 3–year follow–up study. Am. J. Sports Med. 2014, 42, 1169–1175. [Google Scholar]
- Seppel, G.; Plath, J.E.; Völk, C.; Seiberl, W.; Buchmann, S.; Waldt, S.; Imhoff, A.B.; Braun, S. Long–term results after arthroscopic repair of isolated subscapularis tears. Am. J. Sports Med. 2017, 45, 759–766. [Google Scholar]
- McCarron, J.A.; Derwin, K.A.; Bey, M.J.; Polster, J.M.; Schils, J.P.; Ricchetti, E.T.; Iannotti, J.P. Failure with continuity in rotator cuff repair “healing”. Am. J. Sports Med. 2013, 41, 134–141. [Google Scholar]
- Lorbach, O.; Baums, M.H.; Kostuj, T.; Pauly, S.; Scheibel, M.; Carr, A.; Zargar, N.; Saccomanno, M.F.; Milano, G. Advances in biology and mechanics of rotator cuff repair. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 530–541. [Google Scholar]
- Patel, S.; Gualtieri, A.P.; Lu, H.H.; Levine, W.N. Advances in biologic augmentation for rotator cuff repair. Ann. N. Y. Acad. Sci. 2016, 1383, 97–114. [Google Scholar]
- Calejo, I.; Costa–Almeida, R.; Reis, R.L.; Gomes, M.E. Enthesis tissue engineering: Biological requirements meet at the interface. Tissue Eng. Part B Rev. 2019, 25, 330–356. [Google Scholar]
- Zhang, X.; Bogdanowicz, D.; Erisken, C.; Lee, N.M.; Lu, H.H. Biomimetic scaffold design for functional and integrative tendon repair. J. Shoulder Elbow Surg. 2012, 21, 266–277. [Google Scholar]
- Kim, B.S.; Kim, E.J.; Choi, J.S.; Jeong, J.H.; Jo, C.H.; Cho, Y.W. Human collagen–based multilayer scaffolds for tendon–to–bone interface tissue engineering. J. Biomed. Mater. Res. A 2014, 102, 4044–4054. [Google Scholar]
- Font Tellado, S.; Balmayor, E.R.; Van Griensven, M. Strategies to engineer tendon/ligament–to–bone interface: Biomaterials, cells and growth factors. Adv. Drug Deliv. Rev. 2015, 94, 126–140. [Google Scholar]
- Li, Y.; Xiao, Y.; Liu, C. The horizon of materiobiology: A perspective on material–guided cell behaviors and tissue engineering. Chem. Rev. 2017, 117, 4376–4421. [Google Scholar]
- Woodruff, M.A.; Hutmacher, D.W. The return of a forgotten polymer: Polycaprolactone in the 21st century. Prog. Polym. Sci. 2010, 35, 1217–1256. [Google Scholar]
- Azimi, B.; Nourpanah, P.; Rabiee, M.; Arbab, S. Poly (ε-caprolactone) fiber: An overview. J. Eng. Fiber Fabr. 2014, 9, 74–85. [Google Scholar]
- Bianco, S.T.; Moser, H.L.; Galatz, L.M.; Huang, A.H. Biologics and stem cell-based therapies for rotator cuff repair. Ann. N. Y. Acad. Sci. 2019, 1442, 35–47. [Google Scholar]
- Menon, R.S.; Wragg, N.M.; Wilson, S.L. Rotator cuff repair augmentation using osteoinductive growth factors. SN Compr. Clin. Med. 2019, 1, 267–276. [Google Scholar]
- Mondal, D.; Griffith, M.; Venkatraman, S.S. Polycaprolactone-based biomaterials for tissue engineering and drug delivery: Current scenario and challenges. Int. J. Polym. Mater. Polym. Biomater. 2016, 65, 255–265. [Google Scholar]
- Siddiqui, N.; Asawa, S.; Birru, B.; Baadhe, R.; Rao, S. PCL-based composite scaffold matrices for tissue engineering applications. Mol. Biotechnol. 2018, 60, 506–532. [Google Scholar]
- Darney, P.D.; Monroe, S.E.; Klaisle, C.M.; Alvarado, A. Clinical evaluation of the Capronor contraceptive implant: Preliminary report. Am. J. Obstet. Gynecol. 1989, 160, 1292–1295. [Google Scholar]
- Kim, J.; Kudisch, M.; Mudumba, S.; Asada, H.; Aya-Shibuya, E.; Bhisitkul, R.B.; Desai, T.A. Biocompatibility and pharmacokinetic analysis of an intracameral polycaprolactone drug delivery implant for glaucoma. Invest. Ophthalmol. Vis. Sci. 2016, 57, 4341–4346. [Google Scholar]
- Pfeiffer, D.; Stefanitsch, C.; Wankhammer, K.; Müller, M.; Dreyer, L.; Krolitzki, B.; Zernetsch, H.; Glasmacher, B.; Lindner, C.; Lass, A.; et al. Endothelialization of electrospun polycaprolactone (PCL) small caliber vascular grafts spun from different polymer blends. J. Biomed. Mater. Res. A 2014, 102, 4500–4509. [Google Scholar]
- Fuchs, J.; Mueller, M.; Daxböck, C.; Stückler, M.; Lang, I.; Leitinger, G.; Bock, E.; El-Heliebi, A.; Moser, G.; Glasmacher, B.; et al. Histological processing of un-/cellularized thermosensitive electrospun scaffolds. Histochem. Cell Biol. 2018, 151, 343–356. [Google Scholar]
- Baudequin, T.; Gaut, L.; Mueller, M.; Huepkes, A.; Glasmacher, B.; Duprez, D.; Bedoui, F.; Legallais, C. The osteogenic and tenogenic differentiation potential of C3H10T1/2 (mesenchymal stem cell model) cultured on PCL/PLA electrospun scaffolds in the absence of specific differentiation medium. Materials 2017, 10, E1387. [Google Scholar]
- Gryshkov, O.; Mutsenko, V.; Suresh, S.; Glasmacher, B. Cryopreservation of cell-seeded electrospun materials: Towards biobanking of tissue-engineered constructs. Int. J. Artif. Organs 2019, 42, 399. [Google Scholar]
- Venugopal, J.; Ma, L.L.; Yong, T.; Ramakrishna, S. In vitro study of smooth muscle cells on polycaprolactone and collagen nanofibrous matrices. Cell Bio. Int. 2005, 29, 861–867. [Google Scholar]
- De Cassan, D.; Sydow, S.; Schmidt, N.; Behrens, P.; Roger, Y.; Hoffmann, A.; Hoheisel, A.L.; Glasmacher, B.; Hänsch, R.; Menzel, H. Attachment of nanoparticulate drug-release systems on poly(ε-caprolactone) nanofibers via a graftpolymer as interlayer. Colloids Surf. B Biointerfaces 2018, 163, 309–320. [Google Scholar]
- Gniesmer, S.; Brehm, R.; Hoffmann, A.; de Cassan, D.; Menzel, H.; Hoheisel, A.L.; Glasmacher, B.; Willbold, E.; Reifenrath, J.; Wellmann, M.; et al. In vivo analysis of vascularization and biocompatibility of electrospun polycaprolactone fibre scaffolds in the rat femur chamber. J. Tissue Eng. Regen. Med. 2019, 13, 1190–1202. [Google Scholar]
- Cao, H.; McHugh, K.; Chew, S.Y.; Anderson, J.M. The topographical effect of electrospun nanofibrous scaffolds on the in vivo and in vitro foreign body reaction. J. Biomed. Mater. Res. A 2010, 93, 1151–1159. [Google Scholar]
- Barry, F.; Boynton, R.E.; Liu, B.; Murphy, J.M. Chondrogenic differentiation of mesenchymal stem cells from bone marrow: Differentiation-dependent gene expression of matrix components. Exp. Cell Res. 2001, 268, 189–200. [Google Scholar]
- Mueller, M.B.; Fischer, M.; Zellner, J.; Berner, A.; Dienstknecht, T.; Prantl, L.; Kujat, R.; Nerlich, M.; Tuan, R.S.; Angele, P. Hypertrophy in mesenchymal stem cell chondrogenesis: Effect of TGF-beta isoforms and chondrogenic conditioning. Cells Tissues Organs 2010, 192, 158–166. [Google Scholar]
- Matsiko, A.; Levingstone, T.J.; Gleeson, J.P.; O’Brien, F.J. Incorporation of TGF-beta 3 within collagen–hyaluronic acid scaffolds improves their chondrogenic potential. Adv. Healthc. Mater. 2015, 4, 1175–1179. [Google Scholar]
- Fujio, K.; Komai, T.; Inoue, M.; Morita, K.; Okamura, T.; Yamamoto, K. Revisiting the regulatory roles of the TGF–β family of cytokines. Autoimmun. Rev. 2016, 15, 917–922. [Google Scholar]
- Morikawa, M.; Derynck, R.; Miyazono, K. TGF-β and the TGF-β family: Context-dependent roles in cell and tissue physiology. Cold Spring Harb. Perspect. Biol. 2016, 8, a021873. [Google Scholar]
- Deng, Y.; Sun, A.X.; Overholt, K.J.; Yu, G.Z.; Fritch, M.R.; Alexander, P.G.; Shen, H.; Tuan, R.S.; Lin, H. Enhancing chondrogenesis and mechanical strength retention in physiologically relevant hydrogels with incorporation of hyaluronic acid and direct loading of TGF-β. Acta Biomater. 2019, 83, 167–176. [Google Scholar]
- Leung, M.; Jana, S.; Tsao, C.-T.; Zhang, M. Tenogenic differentiation of human bone marrow stem cells via a combinatory effect of aligned chitosan–poly–caprolactone nanofibers and TGF-β3. J. Mater. Chem. B 2013, 1, 6516–6524. [Google Scholar]
- Manning, C.N.; Kim, H.M.; Sakiyama–Elbert, S.; Galatz, L.M.; Havlioglu, N.; Thomopoulos, S. Sustained delivery of transforming growth factor beta three enhances tendon-to-bone healing in a rat model. J. Orthop. Res. 2011, 29, 1099–1105. [Google Scholar]
- Kovacevic, D.; Fox, A.J.; Bedi, A.; Ying, L.; Deng, X.H.; Warren, R.F.; Rodeo, S.A. Calcium-phosphate matrix with or without TGF-β3 improves tendon-bone healing after rotator cuff repair. Am. J. Sports Med. 2011, 39, 811–819. [Google Scholar]
- Willbold, E.; Wellmann, M.; Welke, B.; Angrisani, N.; Gniesmer, S.; Kampmann, A.; Hoffmann, A.; de Cassan, D.; Menzel, H.; Hoheisel, A.L.; et al. Possibilities and limitations of electrospun chitosan–coated polycaprolactone grafts for rotator cuff tear repair. J. Tissue Eng. Regen. Med. 2019, in press. [Google Scholar]
- Arimura, H.; Shukunami, C.; Tokunaga, T.; Karasugi, T.; Okamoto, N.; Taniwaki, T.; Sakamoto, H.; Mizuta, H.; Hiraki, Y. TGF-β1 improves biomechanical strength by extracellular matrix accumulation without increasing the number of tenogenic lineage cells in a rat rotator cuff repair model. Am. J. Sports Med. 2017, 45, 2394–2404. [Google Scholar]
- Roth, S.P.; Brehm, W.; Groß, C.; Scheibe, P.; Schubert, S.; Burk, J. Transforming Growth Factor Beta 3-Loaded Decellularized Equine Tendon Matrix for Orthopedic Tissue Engineering. Int. J. Mol. Sci. 2019, 20, E5474. [Google Scholar]
- Kim, H.M.; Galatz, L.M.; Das, R.; Havlioglu, N.; Rothermich, S.Y.; Thomopoulos, S. The role of transforming growth factor beta isoforms in tendon-to-bone healing. Connect. Tissue Res. 2011, 52, 87–98. [Google Scholar]
- Galatz, L.; Rothermich, S.; VanderPloeg, K.; Petersen, B.; Sandell, L.; Thomopoulos, S. Development of the supraspinatus tendon-to-bone insertion: Localized expression of extracellular matrix and growth factor genes. J. Orthop. Res. 2007, 25, 1621–1628. [Google Scholar]
- Carpenter, J.E.; Thomopoulos, S.; Flanagan, C.L.; DeBano, C.M.; Soslowsky, L.J. Rotator cuff defect healing: A biomechanical and histologic analysis in an animal model. J. Shoulder Elbow Surg. 1998, 7, 599–605. [Google Scholar]
- Tang, L.; Jennings, T.A.; Eaton, J.W. Mast cells mediate acute inflammatory responses to implanted biomaterials. Proc. Natl. Acad. Sci. USA 1998, 95, 8841–8846. [Google Scholar]
- Palmer, J.A.; Abberton, K.M.; Mitchell, G.M.; Morrison, W.A. Macrophage phenotype in response to implanted synthetic scaffolds: An immunohistochemical study in the rat. Cells Tissues Organs 2014, 199, 169–183. [Google Scholar]
- Daentzer, D.; Willbold, E.; Kalla, K.; Bartsch, I.; Masalha, W.; Hallbaum, M.; Hurschler, C.; Kauth, T.; Kaltbeitzel, D.; Hopmann, C.; et al. Bioabsorbable interbody magnesium-polymer cage: Degradation kinetics, biomechanical stiffness, and histological findings from an ovine cervical spine fusion model. Spine (Phila Pa 1976) 2014, 39, E1220–E1227. [Google Scholar]
- Denchai, A.; Tartarini, D.; Mele, E. Cellular response to surface morphology: Electrospinning and computational modeling. Front. Bioeng. Biotechnol. 2018, 6, 155. [Google Scholar]
- Sheikh, Z.; Brooks, P.J.; Barzilay, O.; Fine, N.; Glogauer, M. Macrophages, foreign body giant cells and their response to implantable biomaterials. Materials 2015, 8, 5671–5701. [Google Scholar]
- Shi, X.; von dem Bussche, A.; Hurt, R.H.; Kane, A.B.; Gao, H. Cell entry of one–dimensional nanomaterials occurs by tip recognition and rotation. Nat. Nanotechnol. 2011, 6, 714–719. [Google Scholar]
- Padmore, T.; Stark, C.; Turkevich, L.A.; Champion, J.A. Quantitative analysis of the role of fiber length on phagocytosis and inflammatory response by alveolar macrophages. Biochim. Biophys. Acta 2017, 1861, 58–67. [Google Scholar]
- Boulanger, G.; Andujar, P.; Pairon, J.-C.; Billon-Galland, M.-A.; Dion, C.; Dumortier, P.; Brochard, P.; Sobaszek, A.; Bartsch, P.; Paris, C.; et al. Quantification of short and long asbestos fibers to assess asbestos exposure: A review of fiber size toxicity. Environ. Health 2014, 13, 59. [Google Scholar]
- Veleirinho, B.; Coelho, D.S.; Dias, P.F.; Maraschin, M.; Pinto, R.; Cargnin-Ferreira, E.; Peixoto, A.; Souza, J.A.; Ribeiro-do-Valle, R.M.; Lopes-da-Silva, J.A. Foreign body reaction associated with PET and PET/chitosan electrospun nanofibrous abdominal meshes. PLoS ONE 2014, 9, e95293. [Google Scholar]
- Duda, S.; Dreyer, L.; Behrens, P.; Wienecke, S.; Chakradeo, T.; Glasmacher, B.; Haastert–Talini, K. Outer electrospun polycaprolactone shell induces massive foreign body reaction and impairs axonal regeneration through 3D multichannel chitosan nerve guides. Biomed. Res. Int. 2014, 2014, 835269. [Google Scholar]
- Barbosa, J.N.; Amaral, I.F.; Aguas, A.P.; Barbosa, M.A. Evaluation of the effect of the degree of acetylation on the inflammatory response to 3D porous chitosan scaffolds. J. Biomed. Mater. Res. A 2010, 93, 20–28. [Google Scholar]
- Mitragotri, S.; Lahann, J. Physical approaches to biomaterial design. Nat. Mater. 2009, 8, 15–23. [Google Scholar]
- Ward, W.K.; Slobodzian, E.P.; Tiekotter, K.L.; Wood, M.D. The effect of microgeometry, implant thickness and polyurethane chemistry on the foreign body response to subcutaneous implants. Biomaterials 2002, 23, 4185–4192. [Google Scholar]
- De Cassan, D.; Becker, A.; Glasmacher, B.; Roger, Y.; Hoffmann, A.; Gengenbach, T.R.; Easton, C.D.; Hänsch, R.; Menzel, H. Blending chitosan–g–poly(caprolactone) by electrospinning to produce functional fiber mats for tissue engineering applications. J. Appl. Polym. Sci. 2019, in press. [Google Scholar]
- Wang, X.; Salick, M.R.; Wang, X.; Cordie, T.; Han, W.; Peng, Y.; Li, Q.; Turng, L.S. Poly(ε–caprolactone) nanofibers with a self-induced nanohybrid shish–kebab structure mimicking collagen fibrils. Biomacromolecules 2013, 14, 3557–3569. [Google Scholar]
- De Cassan, D.; Hoheisel, A.L.; Glasmacher, B.; Menzel, H. Impact of sterilization by electron beam, gamma radiation and X-rays on electrospun poly-(ε-caprolactone) fiber scaffolds. J. Mater. Sci. Mater. Med. 2019, 30, 42. [Google Scholar]
- Sydow, S.; Aniol, A.; Hadler, C.; Menzel, H. Chitosan-azide nanoparticle coating as a degradation barrier in multilayered polyelectrolyte drug delivery systems. Biomolecules 2019, 9, E573. [Google Scholar]
- Gan, Q.; Wang, T. Chitosan nanoparticle as protein delivery carrier-systematic examination of fabrication conditions for efficient loading and release. Colloids Surf. B Biointerfaces 2007, 59, 24–34. [Google Scholar]
- Kapacee, Z.; Yeung, C.Y.C.; Lu, Y.; Crabtree, D.; Holmes, D.F.; Kadler, K.E. Synthesis of embryonic tendon-like tissue by hyman marrow stroma/mesenchymal stem cells requires a three-dimensional environment and transforming growth factor β3. Matrix Biol. 2010, 29, 668–677. [Google Scholar]
- Newton, M.D.; Davidson, A.A.; Pomajzl, R.; Seta, J.; Kurdziel, M.D.; Maerz, T. The influence of testing angle on the biomechanical properties of the rat supraspinatus tendon. J. Biomech. 2016, 49, 4159–4163. [Google Scholar]
- Duchman, K.R.; Goetz, J.E.; Uribe, B.U.; Amendola, A.M.; Barber, J.A.; Malandra, A.E.; Fredericks, D.C.; Hettrich, C.M. Delayed administration of recombinant human parathyroid hormone improves early biomechanical strength in a rat rotator cuff repair model. J. Shoulder Elbow Surg. 2016, 25, 1280–1287. [Google Scholar]
- Willbold, E.; Witte, F. Histology and research at the hard tissue–implant interface using Technovit 9100 New embedding technique. Acta Biomater. 2010, 6, 4447–4455. [Google Scholar]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reifenrath, J.; Wellmann, M.; Kempfert, M.; Angrisani, N.; Welke, B.; Gniesmer, S.; Kampmann, A.; Menzel, H.; Willbold, E. TGF–β3 Loaded Electrospun Polycaprolacton Fibre Scaffolds for Rotator Cuff Tear Repair: An in Vivo Study in Rats. Int. J. Mol. Sci. 2020, 21, 1046. https://doi.org/10.3390/ijms21031046
Reifenrath J, Wellmann M, Kempfert M, Angrisani N, Welke B, Gniesmer S, Kampmann A, Menzel H, Willbold E. TGF–β3 Loaded Electrospun Polycaprolacton Fibre Scaffolds for Rotator Cuff Tear Repair: An in Vivo Study in Rats. International Journal of Molecular Sciences. 2020; 21(3):1046. https://doi.org/10.3390/ijms21031046
Chicago/Turabian StyleReifenrath, Janin, Mathias Wellmann, Merle Kempfert, Nina Angrisani, Bastian Welke, Sarah Gniesmer, Andreas Kampmann, Henning Menzel, and Elmar Willbold. 2020. "TGF–β3 Loaded Electrospun Polycaprolacton Fibre Scaffolds for Rotator Cuff Tear Repair: An in Vivo Study in Rats" International Journal of Molecular Sciences 21, no. 3: 1046. https://doi.org/10.3390/ijms21031046