Risk Factors for the Development of Psoriasis

{kind=link}
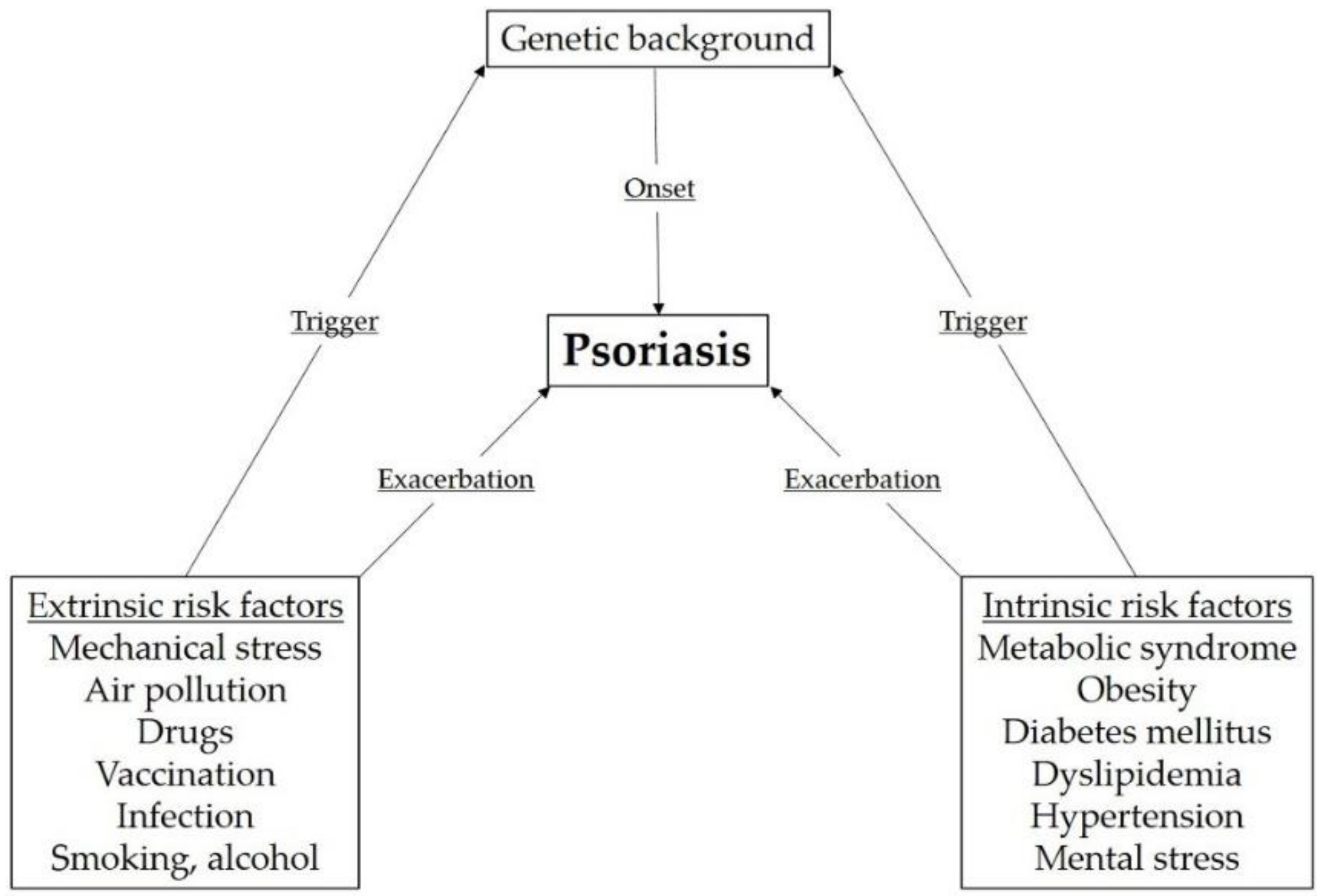
Abstract
1. Introduction
2. Extrinsic Risk Factors
2.1. Mechanical Stress
2.2. Air Pollutants and Sun Exposure
2.3. Drugs
2.4. Vaccination
2.5. Infection
2.6. Lifestyle
3. Intrinsic Risk Factors
3.1. Obesity
3.2. Diabetes Mellitus
3.3. Dyslipidemia
3.4. Hypertension
3.5. Mental Stress
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| PSORS1 | Psoriasis susceptibility 1 |
| DM | Diabetes mellitus |
| UV | Ultraviolet |
| NGF | Nerve growth factor |
| TRM | Resident memory T cells |
| IFN | Interferon |
| PUVA | Psoralen ultraviolet A |
| cAMP | Cyclic adenosine monophosphate |
| TNF | Tumor necrosis factor |
| IL | Interleukin |
| BCG | Bacillus Calmette–Guerin |
| Th | T helper |
| S. | Staphylococcus |
| HIV | Human immunodeficiency virus |
| BMI | Body mass index |
| HDL | High-density lipoprotein |
References
- Boehncke, W.H.; Schon, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Nestle, F.O.; Kaplan, D.H.; Barker, J. Psoriasis. N. Engl. J. Med. 2009, 361, 496–509. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M.; IMPACT project team. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Invest. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Michalek, I.M.; Loring, B.; John, S.M. A systematic review of worldwide epidemiology of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Trembath, R.C.; Clough, R.L.; Rosbotham, J.L.; Jones, A.B.; Camp, R.D.; Frodsham, A.; Browne, J.; Barber, R.; Terwilliger, J.; Lathrop, G.M.; et al. Identification of a major susceptibility locus on chromosome 6p and evidence for further disease loci revealed by a two stage genome-wide search in psoriasis. Hum. Mol. Genet. 1997, 6, 813–820. [Google Scholar] [CrossRef]
- Burden, A.D.; Javed, S.; Bailey, M.; Hodgins, M.; Connor, M.; Tillman, D. Genetics of psoriasis: Paternal inheritance and a locus on chromosome 6p. J. Invest. Dermatol. 1998, 110, 958–960. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sagoo, G.S.; Tazi-Ahnini, R.; Barker, J.W.; Elder, J.T.; Nair, R.P.; Samuelsson, L.; Traupe, H.; Trembath, R.C.; Robinson, D.A.; Iles, M.M. Meta-analysis of genome-wide studies of psoriasis susceptibility reveals linkage to chromosomes 6p21 and 4q28-q31 in Caucasian and Chinese Hans population. J. Invest. Dermatol. 2004, 122, 1401–1405. [Google Scholar] [CrossRef]
- Nair, R.P.; Stuart, P.E.; Nistor, I.; Hiremagalore, R.; Chia, N.V.C.; Jenisch, S.; Weichenthal, M.; Abecasis, G.R.; Lim, H.W.; Christophers, E. Sequence and haplotype analysis supports HLA-C as the psoriasis susceptibility 1 gene. Am. J. Hum. Genet. 2006, 78, 827–851. [Google Scholar] [CrossRef]
- Chen, L.; Tsai, T.F. HLA-Cw6 and psoriasis. Br. J. Dermatol. 2018, 178, 854–862. [Google Scholar] [CrossRef]
- Kawada, A.; Tezuka, T.; Nakamizo, Y.; Kimura, H.; Nakagawa, H.; Ohkido, M.; Ozawa, A.; Ohkawara, A.; Kobayashi, H.; Harada, S.; et al. A survey of psoriasis patients in Japan from 1982 to 2001. J. Dermatol. Sci. 2003, 31, 59–64. [Google Scholar] [CrossRef]
- Takahashi, H.; Nakamura, K.; Kaneko, F.; Nakagawa, H.; Iizuka, H.; Japanese Society for Psoriasis Research. Analysis of psoriasis patients registered with the Japanese Society for Psoriasis Research from 2002–2008. J. Dermatol. 2011, 38, 1125–1129. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Takahashi, H.; Kawada, A.; Iizuka, H.; Nakagawa, H.; Japanese Society for Psoriasis Research. Epidemiological survey from 2009 to 2012 of psoriatic patients in Japanese Society for Psoriasis Research. J. Dermatol. 2018, 45, 293–301. [Google Scholar] [CrossRef]
- Alolabi, N.; White, CP.; Cin, A.D. The Koebner phenomenon and breast reconstruction: Psoriasis eruption along the surgical incision. Can. J. Plast. Surg. 2011, 19, 143–144. [Google Scholar] [CrossRef] [PubMed]
- Arias-Santiago, S.; Espineira-Carmona, M.J.; Aneiros-Fernandez, J. The Koebner phenomenon: Psoriasis in tattoos. CMAJ 2013, 185, 585. [Google Scholar] [CrossRef]
- Binitha, M.P.; Betsy, A.; Lekha, T. Psoriasis occurring as a koebner phenomenon over keloids. Indian J. Dermatol. 2013, 58, 329. [Google Scholar] [CrossRef]
- Morais, P.; Oliveira, M.; Matos, J. Striae: A potential precipitating factor for Koebner phenomenon in psoriasis? Dermatol. Online J. 2013, 19, 18186. [Google Scholar] [PubMed]
- Charalambous, H.; Bloomfield, D. Psoriasis and radiotherapy: Exacerbation of psoriasis following radiotherapy for carcinoma of the breast (the Koebner phenomenon). Clin. Oncol. 2000, 12, 192–193. [Google Scholar]
- Muller, H.; Fah, J.; Dummer, R. Unusual Koebner phenomenon in psoriasis caused by varicella and UVB. Hautarzt 1997, 48, 130–132. [Google Scholar]
- Streit, E.; Vogelgsang, L.E. ECG-induced Koebner phenomenon. N. Engl. J. Med. 2017, 377, 2180. [Google Scholar] [CrossRef]
- Weiss, G.; Shemer, A.; Trau, H. The Koebner phenomenon: Review of the literature. J. Eur. Acad. Dermatol. Venereol. 2002, 16, 241–248. [Google Scholar] [CrossRef]
- Camargo, C.M.; Brotas, A.M.; Ramos-e-Silva, M.; Carneiro, S. Isomorphic phenomenon of Koebner: Facts and controversies. Clin. Dermatol. 2013, 31, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Raychaudhuri, S.P.; Jiang, W.Y.; Raychaudhuri, S.K. Revisiting the Koebner phenomenon: Role of NGF and its receptor system in the pathogenesis of psoriasis. Am. J. Pathol. 2008, 172, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.; Lebwohl, M. The effect of weight on the efficacy of biologic therapy in patients with psoriasis. J. Am. Acad. Dermatol. 2008, 58, 443–446. [Google Scholar] [CrossRef]
- Boyman, O.; Hefti, H.P.; Conrad, C.; Nickoloff, B.J.; Suter, M.; Nestle, F.O. Spontaneous development of psoriasis in a new animal model shows an essential role for resident T cells and tumor necrosis factor-alpha. J. Exp. Med. 2004, 199, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Boyman, O.; Conrad, C.; Tonel, G.; Gilliet, M.; Nestle, F.O. The pathogenic role of tissue-resident immune cells in psoriasis. Trends. Immunol. 2007, 28, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Cheuk, S.; Wiken, M.; Blomqvist, L.; Nylen, S.; Talme, T.; Stahle, M.; Eidsmo, L. Epidermal Th22 and Tc17 cells form a localized disease memory in clinically healed psoriasis. J. Immunol. 2014, 192, 3111–3120. [Google Scholar] [CrossRef]
- Zhang, L.J. Type1 interferons potential initiating factors linking skin wounds with psoriasis pathogenesis. Front. Immunol. 2019, 10, 1440. [Google Scholar] [CrossRef]
- Puri, P.; Nandar, S.K.; Kathuria, S.; Ramesh, V. Effects of air pollution on the skin: A review. Indian J. Dermatol. Venereol. Leprol. 2017, 83, 415–423. [Google Scholar]
- Liaw, F.Y.; Chen, W.L.; Kao, T.W.; Chang, Y.W.; Huang, C.F. Exploring the link between cadmium and psoriasis in a nationally representative sample. Sci. Rep. 2017, 7, 1723. [Google Scholar] [CrossRef]
- Zhang, P.; Wu, M.X. A clinical review of phototherapy for psoriasis. Lasers Med. Sci. 2018, 33, 173–180. [Google Scholar] [CrossRef]
- Rutter, K.J.; Watson, R.E.; Cotterell, L.F.; Brenn, T.; Griffiths, C.E.; Rhodes, L.E. Severely photosensitive psoriasis: A phenotypically defined patient subset. J. Invest. Dermatol. 2009, 129, 2861–2867. [Google Scholar] [CrossRef] [PubMed]
- Balak, D.M.; Hajdarbegovic, E. Drug-induced psoriasis: Clinical perspectives. Psoriasis 2017, 7, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.K.; Del Rosso, J.Q. Drug-provoked psoriasis: Is it drug induced or drug aggravated?: Understanding pathophysiology and clinical relevance. J. Clin. Aesthet. Dermatol. 2010, 3, 32–38. [Google Scholar]
- Justiniano, H.; Berlingeri-Ramos, A.C.; Sanchez, J.L. Pattern analysis of drug-induced skin diseases. Am. J. Dermatopathol. 2008, 30, 352–369. [Google Scholar] [CrossRef] [PubMed]
- Tsankov, N.; Angelova, I.; Kazandjieva, J. Drug-induced psoriasis. Recognition and management. Am. J. Clin. Dermatol. 2000, 1, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, T.C.; Highet, A. A clinical dilemma while treating hypercholesterolaemia in psoriasis. Br. J. Dermatol. 2003, 149, 1305–1306. [Google Scholar] [CrossRef] [PubMed]
- Fisher, D.A.; Elias, P.M.; LeBoit, P.L. Exacerbation of psoriasis by the hypolipidemic agent, gemfibrozil. Arch. Dermatol. 1988, 124, 854–855. [Google Scholar] [CrossRef] [PubMed]
- Fry, L.; Baker, B.S. Triggering psoriasis: The role of infections and medications. Clin. Dermatol. 2007, 25, 606–615. [Google Scholar] [CrossRef]
- van der Fits, L.; Mourits, S.; Voerman, J.S.; Kant, M.; Boon, L.; Laman, J.D.; Cornelissen, F.; Mus, A.M.; Florencia, E.; Prens, E.P.; et al. Imiquimod-induced psoriasis-like skin inflammation in mice is mediated via the IL-23/IL-17 axis. J. Immunol. 2009, 182, 5836–45. [Google Scholar] [CrossRef]
- Bonigen, J.; Raynaud-Donzel, C.; Hureaux, J.; Kramkimel, N.; Blom, A.; Jeudy, G.; Berton, A.L.; Hubiche, T.; Bedane, C.; Legoupil, D.; et al. Anti-PD1-induced psoriasis: A study of 21 patients. J. Eur. Acad. Dermatol. Venereol. 2017, 31, e254–e257. [Google Scholar] [CrossRef]
- Kim, D.W.; Park, S.K.; Woo, S.H.; Yun, S.K.; Kim, H.U.; Park, J. New-onset psoriasis induced by rituximab therapy for non-Hodgkin lymphoma in a child. Eur. J. Dermatol. 2016, 26, 190–191. [Google Scholar] [CrossRef] [PubMed]
- Guidelli, G.M.; Fioravanti, A.; Rubegni, P.; Feci, L. Induced psoriasis after rituximab therapy for rheumatoid arthritis: A case report and review of the literature. Rheumatol. Int. 2013, 33, 2927–2930. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.; Wang, E.; Leon, A.; Huynh, M.; Wehner, M.; Matro, R.; Lions, E.; Liao, W.; Haemel, A. Tumor necrosis factor-alpha inhibitor-induced psoriasis: Systematic review of clinical features, histopathological findings, and management experience. J. Am. Acad. Dermatol. 2017, 76, 334–341. [Google Scholar] [CrossRef]
- Collamer, A.N.; Guerrero, K.T.; Henning, J.S.; Battafarano, D.F. Psoriatic skin lesions induced by tumor necrosis factor antagonist therapy: A literature review and potential mechanisms of action. Arthritis Rheum. 2008, 59, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Munera-Campos, M.; Ballesca, F.; Carrascosa, J.M. Paradoxical reactions to biologic therapy in psoriasis: A review of the literature. Actas Dermosifiliogr. 2018, 109, 791–800. [Google Scholar] [CrossRef]
- Collamer, A.N.; Battafarano, D.F. Psoriatic skin lesions induced by tumor necrosis factor antagonist therapy: Clinical features and possible immunopathogenesis. Semin. Arthritis. Rheum. 2010, 40, 233–240. [Google Scholar] [CrossRef]
- Rahier, J.F.; Moutschen, M.; Van Gompel, A.; Van Ranst, M.; Louis, E.; Segaert, S.; Masson, P.; Keyser, D.F. Vaccinations in patients with immune-mediated inflammatory diseases. Rheumatology 2010, 49, 1815–1827. [Google Scholar] [CrossRef]
- Lopez, A.; Mariette, X.; Bachelez, H.; Belot, A.; Bonnotte, B.; Hachulla, E.; Lahfa, M.; Lortholary, O.; Loulergue, P.; Paul, S.; et al. Vaccination recommendations for the adult immunosuppressed patient: A systematic review and comprehensive field synopsis. J. Autoimmun. 2017, 80, 10–27. [Google Scholar] [CrossRef]
- Wine-Lee, L.; Keller, S.C.; Wilck, M.B.; Gluckman, S.J.; Van Voorhees, A.S. From the Medical Board of the National Psoriasis Foundation: Vaccination in adult patients on systemic therapy for psoriasis. J. Am. Acad. Dermatol. 2013, 69, 1003–1013. [Google Scholar] [CrossRef]
- Gunes, A.T.; Fetil, E.; Akarsu, S.; Ozbagcivan, O.; Babayeva, L. Possible triggering effect of influenza vaccination on psoriasis. J. Immunol. Res. 2015, 2015, 258430. [Google Scholar] [CrossRef]
- Sbidian, E.; Eftekahri, P.; Viguier, M.; Laroche, L.; Chosidow, O.; Gosselin, P.; Trouche, F.; Bonnet, N.; Arfi, C.; Tubach, F.; et al. National survey of psoriasis flares after 2009 monovalent H1N1/seasonal vaccines. Dermatology 2014, 229, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.S.; Kim, S.J.; Kim, S.H.; Kwak, Y.G.; Park, H.J. New onset guttate psoriasis following pandemic H1N1 influenza vaccination. Ann. Dermatol. 2013, 25, 489–492. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Luca, S.; Mihaescu, T. History of BCG vaccine. Maedica 2013, 8, 53–58. [Google Scholar] [PubMed]
- Koca, R.; Altinyazar, H.C.; Numanoglu, G.; Unalacak, M. Guttate psoriasis-like lesions following BCG vaccination. J. Trop. Pediatr. 2004, 50, 178–179. [Google Scholar] [CrossRef] [PubMed]
- Takayama, K.; Satoh, T.; Hayashi, M.; Yokozeki, H. Psoriatic skin lesions induced by BCG vaccination. Acta. Derm. Venereol. 2008, 88, 621–622. [Google Scholar]
- Wee, J.S.; Natkunarajah, J.; Moosa, Y.; Marsden, R.A. Erythrodermic pustular psoriasis triggered by intravesical bacillus Calmette-Guerin immunotherapy. Clin. Exp. Dermatol. 2012, 37, 455–457. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, A.; Mathena, J.; Albano, J.D.; Yacovone, M.; Collins, L. Safety evaluation of adenovirus type 4 and type 7 vaccine live, oral in military recruits. Vaccine 2016, 34, 4558–4564. [Google Scholar] [CrossRef] [PubMed]
- Macias, V.C.; Cunha, D. Psoriasis triggered by tetanus-diphtheria vaccination. Cutan. Ocul. Toxicol. 2013, 32, 164–165. [Google Scholar] [CrossRef]
- Yoneyama, S.; Kamiya, K.; Kishimoto, M.; Komine, M.; Ohtsuki, M. Generalized exacerbation of psoriasis vulgaris induced by pneumococcal polysaccharide vaccine. J. Dermatol. 2019, (in press). [CrossRef]
- Telfer, N.R.; Chalmers, R.J.; Whale, K.; Colman, G. The role of streptococcal infection in the initiation of guttate psoriasis. Arch. Dermatol. 1992, 128, 39–42. [Google Scholar] [CrossRef]
- Rachakonda, T.D.; Dhillon, J.S.; Florek, A.G.; Armstrong, A.W. Effect of tonsillectomy on psoriasis: A systematic review. J. Am. Acad. Dermatol. 2015, 72, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.J.E.; Kell, D.B.; Pretorius, E. Bacterial dysbiosis and translocation in psoriasis vulgaris. Front. Cell. Infect. Microbiol. 2019, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Tomi, N.S.; Kranke, B.; Aberer, E. Staphylococcal toxins in patients with psoriasis, atopic dermatitis, and erythroderma, and in healthy control subjects. J. Am. Acad. Dermatol. 2005, 53, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, A.; Grywalska, E.; Socha, M.; Rolinski, J.; Franciszkiewicz-Pietrzak, K.; Rudnicka, L.; Rudzki, M.; Krasowska, D. Prevalence and possible role of candida species in patients with psoriasis: A systematic review and meta-analysis. Mediat. Inflamm. 2018, 2018, 9602362. [Google Scholar] [CrossRef] [PubMed]
- Kashem, S.W.; Kaplan, D.H. Skin immunity to candida albicans. Trends Immunol. 2016, 37, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Mallon, E.; Bunker, C.B. HIV-associated psoriasis. AIDS Patient Care STDS 2000, 14, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.B.; Wu, K.K.; Lee, M.P.; Bhutani, T.; Wu, J.J. Psoriasis risk factors and triggers. Cutis. 2018, 102, 18–20. [Google Scholar] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Dhillon, J.S.; Armstrong, E.J. Psoriasis and smoking: A systematic review and meta-analysis. Br. J. Dermatol. 2014, 170, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Han, J.; Choi, H.K.; Qureshi, A.A. Smoking and risk of incident psoriasis among women and men in the United States: A combined analysis. Am. J. Epidemiol. 2012, 175, 402–413. [Google Scholar] [CrossRef]
- Naldi, L.; Chatenoud, L.; Linder, D.; Belloni, F.A.; Peserico, A.; Virgili, A.R.; Bruni, P.L.; Ingordo, V.; Scocco, G.L.; Solaroli, C.; et al. Cigarette smoking, body mass index, and stressful life events as risk factors for psoriasis: Results from an Italian case-control study. J. Dermatol. 2005, 125, 61–67. [Google Scholar] [CrossRef]
- Lee, E.J.; Han, K.D.; Han, J.H.; Lee, J.H. Smoking and risk of psoriasis: A nationwide cohort study. J. Am. Acad. Dermatol. 2017, 77, 573–575. [Google Scholar] [CrossRef] [PubMed]
- Brenaut, E.; Horreau, C.; Pouplard, C.; Barnetche, T.; Paul, C.; Richard, M.A.; Joly, P.; Matire, M.L.; Aractingi, S.; Aubin, F.; et al. Alcohol consumption and psoriasis: A systematic literature review. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Murzaku, E.C.; Bronsnick, T.; Rao, B.K. Diet in dermatology: Part II. Melanoma, chronic urticaria, and psoriasis. J. Am. Acad. Dermatol. 2014, 71, 1053-e1. [Google Scholar] [CrossRef] [PubMed]
- Poikolainen, K.; Karvonen, J.; Pukkala, E. Excess mortality related to alcohol and smoking among hospital-treated patients with psoriasis. Arch. Dermatol. 1999, 135, 1490–1493. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; DeCoffe, D.; Molcan, E.; Gibson, D.L. Diet-induced dysbiosis of the intestinal microbiota and the effects on immunity and disease. Nutrients 2012, 4, 1095–1119. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, J.W.; Netea, M.G. A salty taste to autoimmunity. N. Engl. J. Med. 2013, 368, 2520–2521. [Google Scholar] [CrossRef] [PubMed]
- Manzel, A.; Muller, D.N.; Hafler, D.A.; Erdman, S.E.; Linker, R.A.; Kleinewietfeld, M. Role of “Western diet” in inflammatory autoimmune diseases. Curr. Allergy Asthma Rep. 2014, 14, 404. [Google Scholar] [CrossRef]
- Barrea, L.; Nappi, F.; Di Somma, C.; Savanelli, M.C.; Falco, A.; Balato, A.; Balato, N.; Savastano, S. Environmental risk factors in psoriasis: The point of view of the nutritionist. Int. J. Environ. Res. Public Health 2016, 13, 743. [Google Scholar] [CrossRef]
- Love, T.J.; Qureshi, A.A.; Karlson, E.W.; Gelfand, J.M.; Choi, H.K. Prevalence of the metabolic syndrome in psoriasis: Results from the national health and nutrition examination survey, 2003–2006. Arch. Dermatol. 2011, 147, 419–424. [Google Scholar] [CrossRef]
- Langan, S.M.; Seminara, N.M.; Shin, D.B.; Troxel, A.B.; Kimmel, S.E.; Mehta, N.N.; Margolis, D.J.; Gelfand, J.M. Prevalence of metabolic syndrome in patients with psoriasis: A population-based study in the United Kingdom. J. Invest. Dermatol. 2012, 132, 556–562. [Google Scholar] [CrossRef]
- Coto-Segura, P.; Eiris-Salvado, N.; Gonzalez-Lara, L.; Queiro-Silva, R.; Martinez-Camblor, P.; Maldonado-Seral, C.; Garcia-Garcia, B.; Palacios-Garcia, L.; Gomez-Bernal, S.; Santos-Juanes, J.; et al. Psoriasis, psoriatic arthritis and type 2 diabetes mellitus: A systematic review and meta-analysis. Br. J. Dermatol. 2013, 169, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Takahashi, I.; Honma, M.; Ishida-Yamamoto, A.; Iizuka, H. Prevalence of metabolic syndrome in Japanese psoriasis patients. J. Dermatol. Sci. 2010, 57, 143–144. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Iizuka, H. Psoriasis and metabolic syndrome. J. Dermatol. 2012, 39, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Bremmer, S.; Van Voorhees, A.S.; Hsu, S.; Korman, N.J.; Lebwohl, M.G.; Young, M.; Bebo Jr, B.F.; Blauvelt, A. Obesity and psoriasis: From the medical board of the national psoriasis foundation. J. Am. Cad. Dermatol. 2010, 63, 1058–1069. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.; Skov, L. Psoriasis and obesity. Dermatology 2016, 232, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Lindegard, B. Diseases associated with psoriasis in a general population of 159,200 middle-aged, urban, native Swedes. Dermatologica 1986, 172, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Henseler, T.; Christophers, E. Disease concomitance in psoriasis. J. Am. Acad. Dermatol. 1995, 32, 982–986. [Google Scholar] [CrossRef]
- Debbaneh, M.; Millsop, J.W.; Bhatia, B.K.; Koo, J.; Liao, W. Diet and psoriasis, part I: Impact of weight loss interventions. J. Am. Acad. Dermatol. 2014, 71, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Neimann, A.L.; Shin, D.B.; Wang, X.; Margolis, D.J.; Troxel, A.B.; Gelfand, J.M. Prevalence of cardiovascular risk factors in patients with psoriasis. J. Am. Acad. Dermatol. 2006, 55, 829–835. [Google Scholar] [CrossRef]
- Herron, M.D.; Hinckley, M.; Hoffman, M.S.; Papenfuss, J.; Hansen, C.B.; Callis, K.P.; Krueger, G.G. Impact of obesity and smoking on psoriasis presentation and management. Arch. Dermatol. 2005, 141, 1527–1534. [Google Scholar] [CrossRef]
- Mallbris, L.; Granath, F.; Hamsten, A.; Stahle, M. Psoriasis is associated with lipid abnormalities at the onset of skin disease. J. Am. Acad. Dermatol. 2006, 54, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. The association between psoriasis and obesity: A systematic review and meta-analysis of observational studies. Nutr. Diabetes 2012, 2, e54. [Google Scholar] [CrossRef] [PubMed]
- Setty, A.R.; Curhan, G.; Choi, H.K. Obesity, waist circumference, weight change, and the risk of psoriasis in women: Nurses’ Health Study II. Arch. Intern. Med. 2007, 167, 1670–1675. [Google Scholar] [CrossRef] [PubMed]
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Jimenez, F.L. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Bianchi, A.; Maroni, P.; Iannarelli, A.; Di Daniele, N.; Iacopino, L.; Renzo, L.D. Adiposity rather than BMI determines metabolic risk. Int. J. Cardiol. 2013, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Tobin, A.M.; Hackett, C.B.; Rogers, S.; Collins, P.; Richards, H.L.; O’Shea, D.; Kirby, B. Body mass index, waist circumference and HOMA-IR correlate with the psoriasis area and severity index in patients with psoriasis receiving phototherapy. Br. J. Dermatol. 2014, 171, 436–438. [Google Scholar] [CrossRef]
- Kumar, S.; Han, J.; Li, T.; Qureshi, A.A. Obesity, waist circumference, weight change and the risk of psoriasis in US women. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Cao, H. Adipocytokines in obesity and metabolic disease. J. Endocrinol. 2014, 220, T47–T59. [Google Scholar] [CrossRef]
- Versini, M.; Jeandel, P.Y.; Rosenthal, E.; Shoenfeld, Y. Obesity in autoimmune diseases: Not a passive bystander. Autoimmun. Rev. 2014, 13, 981–1000. [Google Scholar] [CrossRef]
- Brembilla, N.C.; Boehncke, W.H. Dermal adipocytes’ claim for fame in psoriasis. Exp. Dermatol. 2017, 26, 392–393. [Google Scholar] [CrossRef]
- Wellen, K.E.; Hotamisligil, G.S. Inflammation, stress, and diabetes. J. Clin. Invest. 2005, 115, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, P.S.; Bissonnette, R.; Teixeira, H.D.; Valdecantos, W.C. Systematic review of efficacy of anti-tumor necrosis factor (TNF) therapy in patients with psoriasis previously treated with a different anti-TNF agent. J. Am. Acad. Dermatol. 2016, 75, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J. The long road to leptin. J. Clin. Invest. 2016, 126, 4727–4734. [Google Scholar] [CrossRef] [PubMed]
- Francisco, V.; Pino, J.; Campos-Cabaleiro, V.; Ruiz-Fernandez, C.; Mera, A.; Gonzalez-Gay, M.A.; Gómez, R.; Gualillo, O. Obesity, Fat mass and immune system: Role for leptin. Front. Physiol. 2018, 9, 640. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Sakaida, I.; Uchida, K.; Terai, S.; Okita, K. Leptin enhances TNF-alpha production via p38 and JNK MAPK in LPS-stimulated Kupffer cells. Life Sci. 2005, 77, 1502–1515. [Google Scholar] [CrossRef] [PubMed]
- Naylor, C.; Petri, W.A., Jr. Leptin regulation of immune responses. Trends Mol. Med. 2016, 22, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.J.; Zhang, C.; Li, M.; Zhu, C.Y.; Shi, G.; Fan, Y.M. Leptin levels in patients with psoriasis: A meta-analysis. Clin. Exp. Dermatol. 2013, 38, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Cerman, A.A.; Bozkurt, S.; Sav, A.; Tulunay, A.; Elbasi, M.O.; Ergun, T. Serum leptin levels, skin leptin and leptin receptor expression in psoriasis. Br. J. Dermatol. 2008, 159, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.V.; Scherer, P.E. Adiponectin, the past two decades. J. Mol. Cell Biol. 2016, 8, 93–100. [Google Scholar] [CrossRef]
- Zhu, K.J.; Shi, G.; Zhang, C.; Li, M.; Zhu, C.Y.; Fan, Y.M. Adiponectin levels in patients with psoriasis: A meta-analysis. J. Dermatol. 2013, 40, 438–442. [Google Scholar] [CrossRef]
- Jensen, P.; Zachariae, C.; Christensen, R.; Geiker, N.R.; Schaadt, B.K.; Stender, S.; Hansen, P.R.; Astrup, A.; Skov, L. Effect of weight loss on the severity of psoriasis: A randomized clinical study. JAMA Dermatol. 2013, 149, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Roongpisuthipong, W.; Pongpudpunth, M.; Roongpisuthipong, C.; Rajatanavin, N. The effect of weight loss in obese patients with chronic stable plaque-type psoriasis. Dermatol. Res. Pract. 2013, 2013, 795932. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.L.; Bergstresser, P.R.; Adams-Huet, B.; Cohen, J.B. Relationship of psoriasis severity to obesity using same-gender siblings as controls for obesity. Clin. Exp. Dermatol. 2009, 34, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Del Giglio, M.; Di Francesco, V.; Zamboni, M.; Girolomoni, G. Weight loss improves the response of obese patients with moderate-to-severe chronic plaque psoriasis to low-dose cyclosporine therapy: A randomized, controlled, investigator-blinded clinical trial. Am. J. Clin. Nutr. 2008, 88, 1242–1247. [Google Scholar] [PubMed]
- Gelfand, J.M.; Abuabara, K. Diet and weight loss as a treatment for psoriasis. Arch. Dermatol. 2010, 146, 544–546. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bardazzi, F.; Balestri, R.; Baldi, E.; Antonucci, A.; De Tommaso, S.; Patrizi, A. Correlation between BMI and PASI in patients affected by moderate to severe psoriasis undergoing biological therapy. Dermatol. Ther. 2010, 23, S14–S19. [Google Scholar] [CrossRef] [PubMed]
- Al-Mutairi, N.; Nour, T. The effect of weight reduction on treatment outcomes in obese patients with psoriasis on biologic therapy: A randomized controlled prospective trial. Expert Opin. Biol. Ther. 2014, 14, 749–756. [Google Scholar] [CrossRef]
- Berends, M.A.; Snoek, J.; de Jong, E.M.; van de Kerkhof, P.C.; van Oijen, M.G.; van Krieken, J.H.; Drenth, J.P.H. Liver injury in long-term methotrexate treatment in psoriasis is relatively infrequent. Aliment. Pharmacol. Ther. 2006, 24, 805–811. [Google Scholar] [CrossRef]
- Malatjalian, D.A.; Ross, J.B.; Williams, C.N.; Colwell, S.J.; Eastwood, B.J. Methotrexate hepatotoxicity in psoriatics: Report of 104 patients from Nova Scotia, with analysis of risks from obesity, diabetes and alcohol consumption during long term follow-up. Can. J. Gastroenterol. 1996, 10, 369–375. [Google Scholar] [CrossRef]
- Montaudie, H.; Sbidian, E.; Paul, C.; Maza, A.; Gallini, A.; Aractingi, S.; Aubin, F.; Bachelez, H.; Cribier, B.; Joly, P.; et al. Methotrexate in psoriasis: A systematic review of treatment modalities, incidence, risk factors and monitoring of liver toxicity. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 12–18. [Google Scholar] [CrossRef]
- Shibata, N.; Hayakawa, T.; Hoshino, N.; Minouchi, T.; Yamaji, A.; Uehara, M. Effect of obesity on cyclosporine trough concentrations in psoriasis patients. Am. J. Health. Syst. Pharm. 1998, 55, 1598–1602. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. Psoriasis and the risk of diabetes mellitus: A systematic review and meta-analysis. JAMA Dermatol. 2013, 149, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Kuai, D.; Zhang, L.; Yang, X.; Qiu, B. Psoriasis increased the risk of diabetes: A meta-analysis. Arch. Dermatol. Res. 2012, 304, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Holm, J.G.; Thomsen, S.F. Type 2 diabetes and psoriasis: Links and risks. Psoriasis 2019, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Granata, M.; Skarmoutsou, E.; Trovato, C.; Rossi, G.A.; Mazzarino, M.C.; D’Amico, F. Obesity, type 1 diabetes, and psoriasis: an autoimmune triple flip. Pathobiology 2017, 84, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Guan, Y.; Yang, J. Cytokines in the progression of pancreatic beta-cell dysfunction. Int. J. Endocrinol. 2010, 2010, 515136. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, N.S.; Rui, J.; Hebrok, M.; Herold, K.C. Life and death of beta cells in Type 1 diabetes: A comprehensive review. J. Autoimmun. 2016, 71, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Alnek, K.; Kisand, K.; Heilman, K.; Peet, A.; Varik, K.; Uibo, R. Increased blood levels of growth factors, proinflammatory cytokines, and Th17 cytokines in patients with newly diagnosed type 1 diabetes. PLoS ONE 2015, 10, e0142976. [Google Scholar] [CrossRef] [PubMed]
- Honkanen, J.; Nieminen, J.K.; Gao, R.; Luopajarvi, K.; Salo, H.M.; Ilonen, J.; Knip, M.; Otonkoski, T.; Vaarala, O. IL-17 immunity in human type 1 diabetes. J. Immunol. 2010, 185, 1959–1967. [Google Scholar] [CrossRef]
- Rocha-Pereira, P.; Santos-Silva, A.; Rebelo, I.; Figueiredo, A.; Quintanilha, A.; Teixeira, F. Dislipidemia and oxidative stress in mild and in severe psoriasis as a risk for cardiovascular disease. Clin. Chim. Acta. 2001, 303, 33–39. [Google Scholar] [CrossRef]
- Uyanik, B.S.; Ari, Z.; Onur, E.; Gunduz, K.; Tanulku, S.; Durkan, K. Serum lipids and apolipoproteins in patients with psoriasis. Clin. Chem. Lab. Med. 2002, 40, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, A.; Lecewicz-Torun, B. Activity of serum lipase and the diversity of serum lipid profile in psoriasis. Med. Sci. Monit. 2002, 8, CR9–CR13. [Google Scholar] [PubMed]
- Salihbegovic, E.M.; Hadzigrahic, N.; Suljagic, E.; Kurtalic, N.; Hadzic, J.; Zejcirovic, A.; Bijedic, M.; Handanagic, A. Psoriasis and dyslipidemia. Mater Sociomed 2015, 27, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, A.; Michalak-Stoma, A.; Chodorowska, G.; Szepietowski, J.C. Lipid disturbances in psoriasis: An update. Mediators Inflamm. 2010. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, S.; Angioni, R.; Cattaneo, A.; Beck-Peccoz, P.; Spada, A. Effects of retinoid therapy on insulin sensitivity, lipid profile and circulating adipocytokines. Eur. J. Endocrinol. 2006, 154, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Goldfarb, M.T.; Ellis, C.N.; Voorhees, J.J. Side-effect profile of acitretin therapy in psoriasis. J. Am. Acad. Dermatol. 1989, 20, 1088–1093. [Google Scholar] [CrossRef]
- Ellis, C.N.; Kang, S.; Vinik, A.I.; Grekin, R.C.; Cunningham, W.J.; Voorhees, J.J. Glucose and insulin responses are improved in patients with psoriasis during therapy with etretinate. Arch. Dermatol. 1987, 123, 471–475. [Google Scholar] [CrossRef]
- Grossman, R.M.; Delaney, R.J.; Brinton, E.A.; Carter, D.M.; Gottlieb, A.B. Hypertriglyceridemia in patients with psoriasis treated with cyclosporine. J. Am. Acad. Dermatol. 1991, 25, 648–651. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. The association between psoriasis and hypertension: A systematic review and meta-analysis of observational studies. J. Hypertens. 2013, 31, 433–442. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Lin, S.W.; Chambers, C.J.; Sockolov, M.E.; Chin, D.L. Psoriasis and hypertension severity: Results from a case-control study. PLoS ONE 2011, 6, e18227. [Google Scholar] [CrossRef]
- Salihbegovic, E.M.; Hadzigrahic, N.; Suljagic, E.; Kurtalic, N.; Sadic, S.; Zejcirovic, A.; Mujacic, A. Psoriasis and high blood pressure. Med. Arch. 2015, 69, 13–15. [Google Scholar] [CrossRef]
- Phan, C.; Sigal, M.L.; Lhafa, M.; Barthelemy, H.; Maccari, F.; Esteve, E.; Reguiai, Z.; Perrot, J.L.; Chaby, G.; Maillard, H.; et al. Metabolic comorbidities and hypertension in psoriasis patients in France. Comparisons with French national databases. Ann. Dermatol. Venereol. 2016, 143, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.N.; Han, K.; Song, S.W.; Lee, J.H. Hypertension and risk of psoriasis incidence: An 11-year nationwide population-based cohort study. PLoS ONE 2018, 13, e0202854. [Google Scholar] [CrossRef] [PubMed]
- Snast, I.; Reiter, O.; Atzmony, L.; Leshem, Y.A.; Hodak, E.; Mimouni, D. Psychological stress and psoriasis: A systematic review and meta-analysis. Br. J. Dermatol. 2018, 178, 1044–1055. [Google Scholar] [CrossRef] [PubMed]
- Verhoeven, E.W.; Kraaimaat, F.W.; de Jong, E.M.; Schalkwijk, J.; van de Kerkhof, P.C.; Evers, A.W. Individual differences in the effect of daily stressors on psoriasis: A prospective study. Br. J. Dermatol. 2009, 161, 295–299. [Google Scholar] [CrossRef] [PubMed]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamiya, K.; Kishimoto, M.; Sugai, J.; Komine, M.; Ohtsuki, M. Risk Factors for the Development of Psoriasis. Int. J. Mol. Sci. 2019, 20, 4347. https://doi.org/10.3390/ijms20184347
Kamiya K, Kishimoto M, Sugai J, Komine M, Ohtsuki M. Risk Factors for the Development of Psoriasis. International Journal of Molecular Sciences. 2019; 20(18):4347. https://doi.org/10.3390/ijms20184347
Chicago/Turabian StyleKamiya, Koji, Megumi Kishimoto, Junichi Sugai, Mayumi Komine, and Mamitaro Ohtsuki. 2019. "Risk Factors for the Development of Psoriasis" International Journal of Molecular Sciences 20, no. 18: 4347. https://doi.org/10.3390/ijms20184347
APA StyleKamiya, K., Kishimoto, M., Sugai, J., Komine, M., & Ohtsuki, M. (2019). Risk Factors for the Development of Psoriasis. International Journal of Molecular Sciences, 20(18), 4347. https://doi.org/10.3390/ijms20184347