Improved Survival in Hepatocellular Carcinoma Patients with Cardiac Arrhythmia by Amiodarone Treatment through Autophagy

 ,
,
Abstract
1. Introduction
2. Results
2.1. Demographic Characteristics
2.2. The Cause-Specific Hazard Ratio and 3-Year Cumulative Survival of HCC Patients
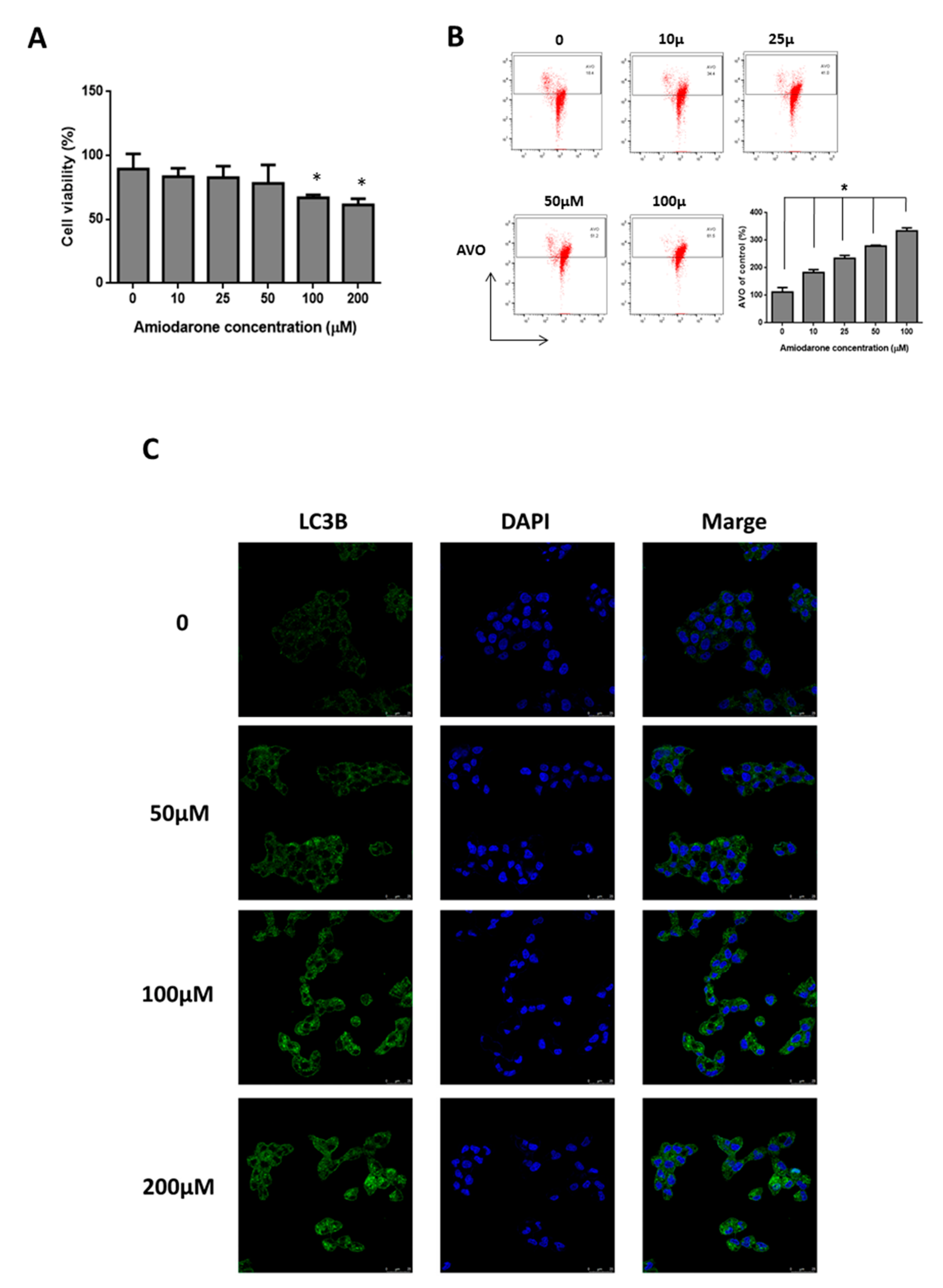
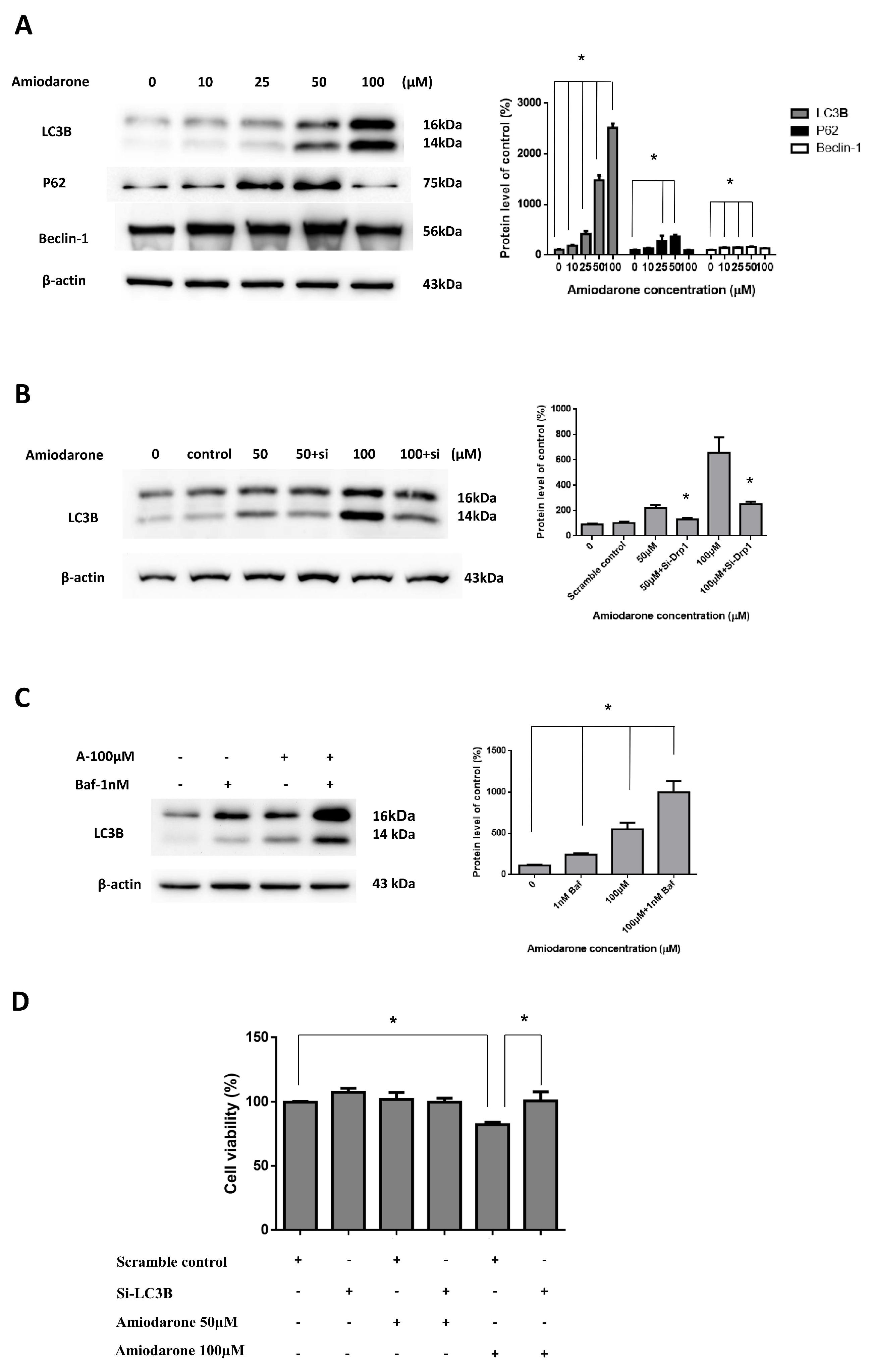
2.3. Amiodarone Induced HepG2 Cell Death via Autophagic Activation
3. Discussion
4. Materials and Methods
4.1. Data Sources
4.2. Ethical Approval and Informed Consent
4.3. Hepatocellular Carcinoma Population
4.4. Amiodarone Use
4.5. Study Outcome
4.6. Covariate Assessment
4.7. Cell Culture
4.8. Cell Viability Assay
4.9. Quantification of Acidic Vesicular Organelles (AVO) Development
4.10. Immunofluorescence Microscopy
4.11. Western Blot Analysis
4.12. Transfection Experiments
4.13. Tissue Array Immunohistochemistry
4.14. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AF | Atrial fibrillation |
| aHR | Adjusted hazard ratio |
| AVO | Acidic vesicular organelles |
| CI | Confidence interval |
| DAPI | 4′,6-diamidino-2-phenylindole |
| EGV | Esophagogastric varices |
| FBS | Fetal Bovine Serum |
| GI | Gastrointestinal |
| HCC | Hepatocellular carcinoma |
| HBV | Hepatitis B virus |
| HCV | Hepatitis C virus |
| HE | Hepatic encephalopathy |
| HR | Hazard ratio |
| IHC | Immunohistochemistry |
| K-M | Kaplan–Meier |
| NHI | National Health Insurance |
| NHIRD | National Health Insurance Research Database |
| PBS | Phosphate buffer saline |
| PEI | Percutaneous ethanol injection |
| RCIPD | Registry for Catastrophic Illness Patients Database |
| RFA | Radiofrequency ablation |
| SD | Standard deviation |
| TAE | Transarterial embolization |
| TFEB | Transcription Factor EB |
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Bruix, J.; Gores, G.J.; Mazzaferro, V. Hepatocellular carcinoma: Clinical frontiers and perspectives. Gut 2014, 63, 844–855. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Tiong, L.; Maddern, G.J. Systematic review and meta-analysis of survival and disease recurrence after radiofrequency ablation for hepatocellular carcinoma. Br. J. Surg. 2011, 98, 1210–1224. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Bruix, J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology 2003, 37, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Salem, R.; Lewandowski, R.J.; Mulcahy, M.F.; Riaz, A.; Ryu, R.K.; Ibrahim, S.; Atassi, B.; Baker, T.; Gates, V.; Miller, F.H.; et al. Radioembolization for hepatocellular carcinoma using Yttrium-90 microspheres: A comprehensive report of long-term outcomes. Gastroenterology 2010, 138, 52–64. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferrom, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; Santoro, A.; Raoul, J.L.; Forner, A.; Schwartz, M.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- He, X.X.; Li, Y.; Ren, H.P.; Tian, D.A.; Lin, J.S. 2010 guideline for the management of hepatocellular carcinoma recommended by the American Association for the Study of Liver Diseases. Chin. J. Hepatol. 2011, 19, 249–250. [Google Scholar]
- Lozy, F.; Karantza, V. Autophagy and cancer cell metabolism. Semin. Cell Dev. Biol. 2012, 23, 395–401. [Google Scholar] [CrossRef]
- Lan, S.H.; Wu, S.Y.; Zuchini, R.; Lin, X.Z.; Su, I.J.; Tsai, T.F.; Lin, Y.J.; Wu, C.T.; Liu, H.S. Autophagy suppresses tumorigenesis of hepatitis B virus-associated hepatocellular carcinoma through degradation of microRNA-224. Hepatology 2014, 59, 505–517. [Google Scholar] [CrossRef]
- Lin, C.W.; Chen, Y.S.; Lin, C.C.; Chen, Y.J.; Lo, G.H.; Lee, P.H.; Kuo, P.L.; Dai, C.Y.; Huang, J.F.; Chung, W.L.; et al. Amiodarone as an autophagy promoter reduces liver injury and enhances liver regeneration and survival in mice after partial hepatectomy. Sci. Rep. 2015, 5, 15807. [Google Scholar] [CrossRef] [PubMed]
- Kowalik, M.A.; Perra, A.; Ledda-Columbano, G.M.; Ippolito, G.; Piacentini, M.; Columbano, A.; Falasca, L. Induction of autophagy promotes the growth of early preneoplastic rat liver nodules. Oncotarget 2016, 7, 5788–5799. [Google Scholar] [CrossRef] [PubMed]
- NHIA. National Health Insurance Annual Report 2015–2016; National Health Insurance Administration, Ministry of Health and Welfare: Taipei, Taiwan, 2015. [Google Scholar]
- Su, V.Y.; Hu, Y.W.; Chou, K.T.; Ou, S.M.; Lee, Y.C.; Lin, E.Y.; Chen, T.J.; Tzeng, C.H.; Liu, C.J. Amiodarone and the risk of cancer: A nationwide population-based study. Cancer 2013, 119, 1699–1705. [Google Scholar] [CrossRef]
- Huang, T.P.; Liu, P.H.; Lien, A.S.; Yang, S.L.; Chang, H.H.; Yen, H.R. A nationwide population-based study of traditional Chinese medicine usage in children in Taiwan. Complement. Ther. Med. 2014, 22, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Goldschlager, N.; Epstein, A.E.; Naccarelli, G.V.; Olshansky, B.; Singh, B.; Collard, H.R.; Murphy, E. A practical guide for clinicians who treat patients with amiodarone: 2007. Heart Rhythm. 2007, 4, 1250–1259. [Google Scholar] [CrossRef] [PubMed]
- Bolos, D.; Finn, R.S. Systemic therapy in HCC: Lessons from brivanib. J. Hepatol. 2014, 61, 947–950. [Google Scholar] [CrossRef][Green Version]
- Abdel-Rahman, O.; Elsayed, Z.A. Combination trans arterial chemoembolization (TACE) plus sorafenib for the management of unresectable hepatocellular carcinoma: A systematic review of the literature. Dig. Dis. Sci. 2013, 58, 3389–3396. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Numata, K.; Moriya, S.; Shimoyama, Y.; Ishii, T.; Nozaki, A.; Kondo, M.; Morimoto, M.; Maeda, S.; Sakamaki, K.; et al. Hepatocellular carcinoma: Concomitant sorafenib promotes necrosis after radiofrequency ablation—Propensity score matching analysis. Radiology 2014, 272, 598–604. [Google Scholar] [CrossRef]
- Greten, T.F.; Wang, X.W.; Korangy, F. Current concepts of immune based treatments for patients with HCC: From basic science to novel treatment approaches. Gut 2015, 64, 842–848. [Google Scholar] [CrossRef]
- Finn, R.S. Drug therapy: Sorafenib. Hepatology 2010, 51, 1843–1849. [Google Scholar] [CrossRef]
- Yang, T.L.; Hu, Y.F.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Tuan, T.C.; Chao, T.F.; Chung, F.P.; Lei, H.J.; Chen, S.A. Atrial fibrillation influences survival in patients with hepatocellular carcinoma: Experience from a single center in Taiwan. J. Chin. Med. Assoc. 2014, 77, 117–121. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lan, S.H.; Wu, S.Y.; Zuchini, R.; Lin, X.Z.; Su, I.J.; Tsai, T.F.; Lin, Y.J.; Wu, C.T.; Liu, H.S. Autophagy-preferential degradation of MIR224 participates in hepatocellular carcinoma tumorigenesis. Autophagy 2014, 10, 1687–1689. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Ye, L.; Bai, Y.; Sun, A.; Cox, B.; Liu, D.; Li, Y.; Liotta, D.; Snyder, J.P.; Fu, H.; et al. Autophagy and apoptosis in hepatocellular carcinoma induced by EF25-(GSH)2: A novel curcumin analog. PLoS ONE 2014, 9, e107876. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.L.; Liu, S.T.; Wang, Y.W.; Lin, W.S.; Huang, S.M. Amiodarone promotes cancer cell death through elevated truncated SRSF3 and downregulation of miR-224. Oncotarget 2018, 9, 13390–13406. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.Y.; Lan, S.H.; Liu, H.S. Degradative autophagy selectively regulates CCND1 (cyclin D1) and MIR224, two oncogenic factors involved in hepatocellular carcinoma tumorigenesis. Autophagy 2019, 15, 729–730. [Google Scholar] [CrossRef] [PubMed]
- White, E. The role for autophagy in cancer. J. Clin. Investig. 2015, 125, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Buratta, S.; Urbanelli, L.; Ferrara, G.; Sagini, K.; Goracci, L.; Emiliani, C. A role for the autophagy regulator Transcription Factor EB in amiodarone-induced phospholipidosis. Biochem. Pharmacol. 2015, 95, 201–209. [Google Scholar] [CrossRef]
- Arrigo, M.; Bettex, D.; Rudiger, A. Management of atrial fibrillation in critically ill patients. Crit. Care Res. Pract. 2014, 2014, 840615. [Google Scholar] [CrossRef]
- Van Cott, T.E.; Yehle, K.S.; DeCrane, S.K.; Thorlton, J.R. Amiodarone-induced pulmonary toxicity: Case study with syndrome analysis. Heart Lung 2013, 42, 262–266. [Google Scholar] [CrossRef]
- Padmanabhan, H. Amiodarone and thyroid dysfunction. South Med. J. 2010, 103, 922–930. [Google Scholar] [CrossRef]
- Passman, R.S.; Bennett, C.L.; Purpura, J.M.; Kapur, R.; Johnson, L.N.; Raisch, D.W.; West, D.P.; Edwards, B.J.; Belknap, S.M.; Liebling, D.B.; et al. Amiodarone-associated optic neuropathy: A critical review. Am. J. Med. 2012, 125, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Memon, K.; Kulik, L.; Lewandowski, R.J.; Wang, E.; Ryu, R.K.; Riaz, A.; Nikolaidis, P.; Miller, F.H.; Yaghmai, V.; Baker, T.; et al. Alpha-fetoprotein response correlates with EASL response and survival in solitary hepatocellular carcinoma treated with transarterial therapies: A subgroup analysis. J. Hepatol. 2012, 56, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Ueno, M.; Hayami, S.; Shigekawa, Y.; Kawai, M.; Hirono, S.; Okada, K.; Tamai, H.; Shingaki, N.; Mori, Y.; Ichinose, M.; et al. Prognostic impact of surgery and radiofrequency ablation on single nodular HCC 5 cm: Cohort study based on serum HCC markers. J. Hepatol. 2015, 63, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Bruix, J. Biomarkers for early diagnosis of hepatocellular carcinoma. Lancet Oncol. 2012, 13, 750–751. [Google Scholar] [CrossRef]
- Llovet, J.M.; Fuster, J.; Bruix, J.; Barcelona-Clinic Liver Cancer, G. The Barcelona approach: Diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transplant. 2004, 10, S115–S120. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Llovet, J.M.; Bruix, J. Chemoembolization for intermediate HCC: Is there proof of survival benefit? J. Hepatol. 2012, 56, 984–986. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kwak, S.C.; Kim, D.K.; Park, S.W.; Kim, H.S.; Kim, Y.S.; Lee, D.; Lee, J.W.; Lee, C.G.; Lee, H.K.; et al. Effects of Huang Bai (Phellodendri Cortex) and Three Other Herbs on GnRH and GH Levels in GT1-7 and GH3 Cells. Evid. Based. Complement. Altern. Med. 2016, 2016, 9389028. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.H.; Chen, W.C.; Tsan, Y.T.; Chen, M.J.; Shih, W.T.; Tsai, Y.H.; Chen, P.C. Statin use and the risk of cirrhosis development in patients with hepatitis C virus infection. J. Hepatol. 2015, 63, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.N.; Lin, C.L.; Lin, M.C.; Lai, C.H.; Lin, H.H.; Yang, C.H.; Sung, F.C.; Kao, C.H. Risk of leukaemia in children infected with enterovirus: A nationwide, retrospective, population-based, Taiwanese-registry, cohort study. Lancet Oncol. 2015, 16, 1335–1343. [Google Scholar] [CrossRef]
- Wu, C.Y.; Chen, Y.J.; Ho, H.J.; Ho, H.J.; Hsu, Y.C.; Kuo, K.N.; Wu, M.S.; Lin, J.T. Association between nucleoside analogues and risk of hepatitis B virus-related hepatocellular carcinoma recurrence following liver resection. JAMA 2012, 308, 1906–1914. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with HCC (N = 558) | |||||
|---|---|---|---|---|---|
| Non-Amiodarone Users (n = 221) | Amiodarone Users (n = 221) | p-Value | |||
| n | % | n | % | ||
| Follow-up time, months (median, 25th and 75th percentile) | 17.64(5.55–37.84) | 27.30(13.01–45.63) | |||
| Gender | |||||
| Women | 84 | 38.01 | 84 | 38.01 | 0.99 |
| Men | 137 | 61.99 | 137 | 61.99 | |
| Age, years | |||||
| 18–64 | 34 | 15.38 | 34 | 15.38 | 0.99 |
| More than 65 | 187 | 84.62 | 187 | 84.62 | |
| Median (25th and 75th percentile) † | 72.58(67.98–77.65) | 73.31(68.30–77.57) | 0.7911 | ||
| Co-morbidities | |||||
| HBV | 61 | 27.6 | 61 | 27.6 | 0.99 |
| HCV | 118 | 53.39 | 118 | 53.39 | 0.99 |
| Liver cirrhosis | 193 | 87.33 | 193 | 87.33 | 0.99 |
| HE | 13 | 5.88 | 13 | 5.88 | 0.99 |
| Ascites | 66 | 29.86 | 66 | 29.86 | 0.99 |
| EGV | 34 | 15.38 | 34 | 15.38 | 0.99 |
| Hepatectomy | 6 | 2.71 | 6 | 2.71 | 0.99 |
| RFA or PEI | 45 | 20.36 | 45 | 20.36 | 0.99 |
| TAE | 98 | 44.34 | 98 | 44.34 | 0.99 |
| Variable | Death no. | Crude † | Adjusted ‡-Model 1 | Adjusted-Model 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (n = 288) | HR | 95% C.I. | p-Value | HR | 95% C.I. | p-Value | HR | 95% C.I. | p-Value | |
| Amiodarone drug used | ||||||||||
| Non-amiodarone users | 143 | 1.00 | reference | 1.00 | reference | 1.00 | reference | |||
| Amiodarone users | 145 | 0.83 | (0.66–1.04) | 0.11 | 0.77 | (0.61–0.97) | 0.0294 | 0.75 | (0.59–0.95) | 0.0155 |
| Gender | ||||||||||
| Women | 113 | 1.00 | reference | 1.00 | reference | 1.00 | reference | |||
| Men | 175 | 0.89 | (0.7–1.13) | 0.322 | 0.95 | (0.74–1.22) | 0.678 | 0.94 | (0.73–1.21) | 0.6082 |
| Age group | ||||||||||
| 18–64 | 38 | 1.00 | reference | 1.00 | reference | 1.00 | reference | |||
| More than 65 | 250 | 1.31 | (0.93–1.85) | 0.1175 | 1.19 | (0.82–1.7) | 0.3606 | 1.2 | (0.83–1.73) | 0.3366 |
| Co-morbidities | ||||||||||
| HBV | ||||||||||
| No | 218 | 1.00 | reference | 1.00 | reference | 1.00 | reference | |||
| Yes | 70 | 0.75 | (0.57–0.98) | 0.04 | 0.8 | (0.58–1.12) | 0.1989 | 0.79 | (0.58–1.08) | 0.1406 |
| HCV | ||||||||||
| No | 132 | 1.00 | reference | 1.00 | reference | 1.00 | reference | |||
| Yes | 156 | 0.99 | (0.79–1.25) | 0.9556 | 0.97 | (0.71–1.31) | 0.8243 | 0.9 | (0.69–1.17) | 0.4343 |
| Liver cirrhosis | ||||||||||
| No | 40 | 1.00 | reference | 1.00 | reference | |||||
| Yes | 248 | 0.74 | (0.53–1.04) | 0.0821 | 1.09 | (0.7–1.69) | 0.7064 | |||
| HE | ||||||||||
| No | 267 | 1.00 | reference | 1.00 | reference | |||||
| Yes | 21 | 1.65 | (1.05–2.58) | 0.0286 | 1.42 | (0.89–2.28) | 0.1448 | |||
| Ascites | ||||||||||
| No | 173 | 1.00 | reference | 1.00 | reference | |||||
| Yes | 115 | 1.86 | (1.47–2.36) | <0.0001 | 2.24 | (1.73–2.9) | <0.0001 | |||
| EGV | ||||||||||
| No | 237 | 1.00 | reference | |||||||
| Yes | 51 | 1.15 | (0.85–1.56) | 0.3549 | 0.94 | (0.68–1.31) | 0.7245 | |||
| Hepatectomy | ||||||||||
| No | 281 | 1.00 | reference | 1.00 | reference | 1.00 | reference | |||
| Yes | 7 | 0.48 | (0.21–1.08) | 0.0746 | 0.57 | (0.25–1.31) | 0.1866 | 0.66 | (0.29–1.51) | 0.3191 |
| RFA or PEI | ||||||||||
| No | 231 | 1.00 | reference | 1.00 | reference | 1.00 | reference | |||
| Yes | 57 | 0.6 | (0.45–0.81) | 0.0008 | 0.65 | (0.48–0.88) | 0.0051 | 0.64 | (0.47–0.87) | 0.0042 |
| TAE | ||||||||||
| No | 155 | 1.00 | reference | 1.00 | reference | 1.00 | reference | |||
| Yes | 133 | 0.67 | (0.53–0.85) | 0.001 | 0.71 | (0.55–0.91) | 0.0079 | 0.6 | (0.46–0.78) | <0.0001 |
| Variables | Non-User (n = 221) | Users (more than 28 days) | p for Trend † | |
|---|---|---|---|---|
| 28 to 83 days (n = 142) | More than 84 days (n = 79) | |||
| aHR | aHR (95% CI) | aHR (95% CI) | ||
| Total | 1.00 | 1.02(0.79–1.32) | 0.40(0.27–0.58) *** | <0.0001 |
| Gender | ||||
| Women | 1.00 | 1.03(0.67–1.6) | 0.49(0.29–0.83) ** | 0.0156 |
| Men | 1.00 | 1.00(0.73–1.38) | 0.3(0.17–0.52) *** | 0.0002 |
| Age group | ||||
| 18–64 | 1.00 | 1.66(0.73–3.75) | 0.6(0.24–1.53) | 0.5497 |
| More than 65 | 1.00 | 0.95(0.72–1.25) | 0.34(0.23–0.52) *** | <0.0001 |
| Co-morbidities | ||||
| HBV | ||||
| No | 1.00 | 0.93(0.7–1.26) | 0.32(0.21–0.5 )*** | <0.0001 |
| Yes | 1.00 | 1.29(0.76–2.19) | 0.73(0.35–1.54) | 0.7191 |
| HCV | ||||
| No | 1.00 | 0.91(0.62–1.34) | 0.32(0.19–0.55) *** | <0.0001 |
| Yes | 1.00 | 1.15(0.81–1.62) | 0.46(0.27–0.78) ** | 0.0264 |
| Liver cirrhosis | ||||
| No | 1.00 | 0.69(0.34–1.42) | 0.17(0.06–0.45) *** | 0.0003 |
| Yes | 1.00 | 1.06(0.81–1.4) | 0.52(0.35–0.78) ** | 0.0080 |
| HE | ||||
| No | 1.00 | 1.02(0.78–1.33) | 0.37(0.25–0.55) *** | <0.0001 |
| Yes | 1.00 | 1.06(0.34–3.32) | 0.82(0.17–3.9) | 0.8654 |
| Ascites | ||||
| No | 1.00 | 1.1(0.79–1.53) | 0.37(0.23–0.59) *** | 0.0002 |
| Yes | 1.00 | 0.82(0.54–1.24) | 0.42(0.22–0.79) ** | 0.0103 |
| EGV | ||||
| No | 1.00 | 1.02(0.77–1.35) | 0.37(0.24–0.55) *** | <0.0001 |
| Yes | 1.00 | 1.03(0.54–2) | 0.63(0.23–1.72) | 0.4832 |
| Hepatectomy | ||||
| No | 1.00 | 1(0.77–1.3) | 0.39(0.27–0.57) *** | <0.0001 |
| Yes | 1.00 | 1.35(0.2–9.2) | - | 0.7595 |
| RFA or PEI | ||||
| No | 1.00 | 0.91(0.69–1.21) | 0.33(0.21–0.51) *** | <0.0001 |
| Yes | 1.00 | 1.56(0.86–2.85) | 0.9(0.39–2.05) | 0.7099 |
| TAE | ||||
| No | 1.00 | 0.9(0.64–1.26) | 0.24(0.13–0.44) *** | <0.0001 |
| Yes | 1.00 | 1.12(0.76–1.66) | 0.74(0.46–1.21) | 0.3662 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.-T.; Hsu, W.-F.; Huang, H.-S.; Yen, J.-H.; Lin, M.-C.; Peng, C.-Y.; Yen, H.-R. Improved Survival in Hepatocellular Carcinoma Patients with Cardiac Arrhythmia by Amiodarone Treatment through Autophagy. Int. J. Mol. Sci. 2019, 20, 3978. https://doi.org/10.3390/ijms20163978
Huang S-T, Hsu W-F, Huang H-S, Yen J-H, Lin M-C, Peng C-Y, Yen H-R. Improved Survival in Hepatocellular Carcinoma Patients with Cardiac Arrhythmia by Amiodarone Treatment through Autophagy. International Journal of Molecular Sciences. 2019; 20(16):3978. https://doi.org/10.3390/ijms20163978
Chicago/Turabian StyleHuang, Sheng-Teng, Wei-Fan Hsu, Hung-Sen Huang, Jia-Hau Yen, Mei-Chen Lin, Cheng-Yuan Peng, and Hung-Rong Yen. 2019. "Improved Survival in Hepatocellular Carcinoma Patients with Cardiac Arrhythmia by Amiodarone Treatment through Autophagy" International Journal of Molecular Sciences 20, no. 16: 3978. https://doi.org/10.3390/ijms20163978
APA StyleHuang, S.-T., Hsu, W.-F., Huang, H.-S., Yen, J.-H., Lin, M.-C., Peng, C.-Y., & Yen, H.-R. (2019). Improved Survival in Hepatocellular Carcinoma Patients with Cardiac Arrhythmia by Amiodarone Treatment through Autophagy. International Journal of Molecular Sciences, 20(16), 3978. https://doi.org/10.3390/ijms20163978