Arterial Stiffness Assessed by Cardio-Ankle Vascular Index


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. The Mechanism of Arterial Stiffness
3. Physiological Examinations of Arterial Stiffness
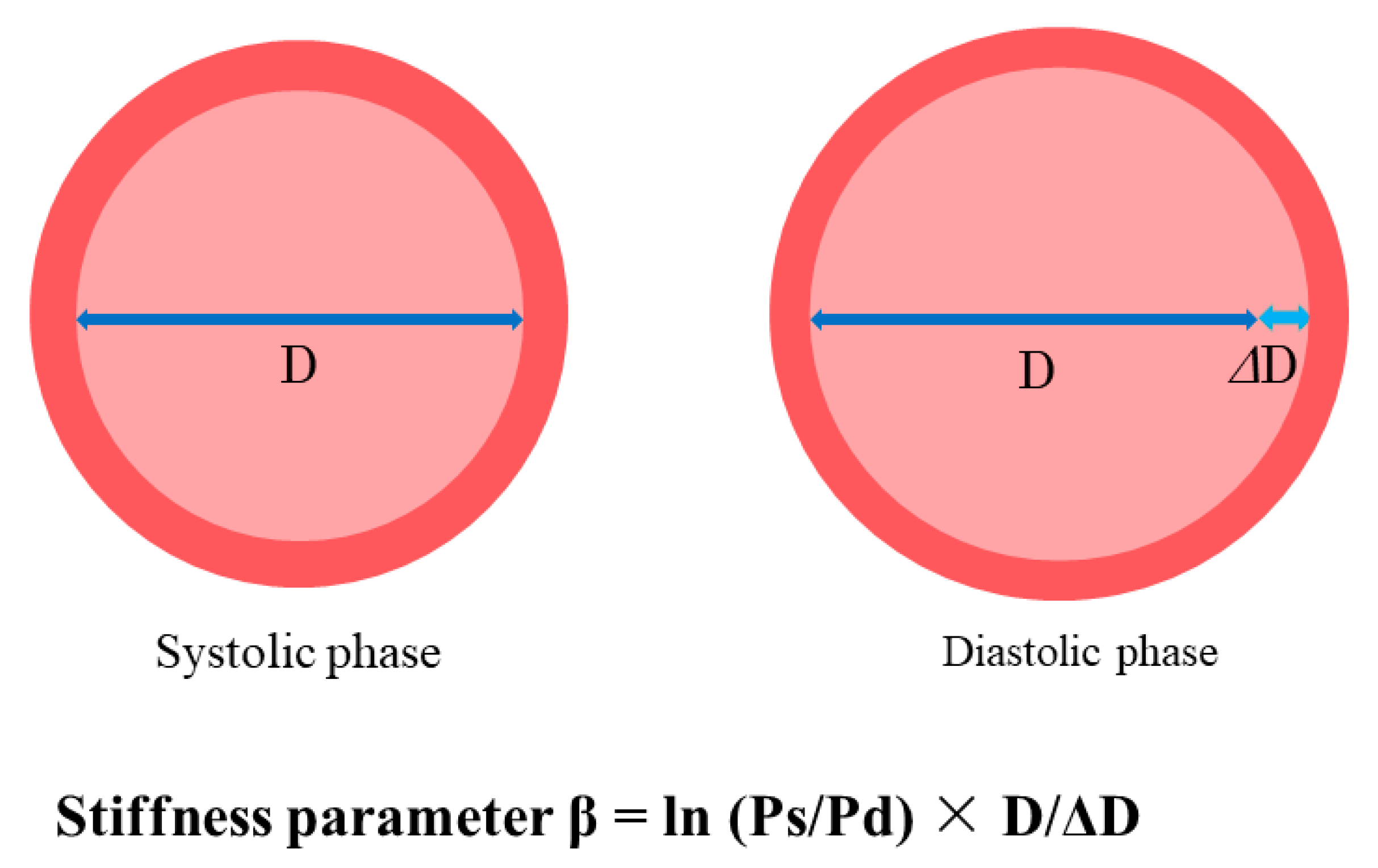
4. Mechanical Principles of CAVI
= D2/(2DΔD + ΔD2)
≅ D/2ΔD
= a [2(ρ/ΔP) × ln(Ps/Pd) × haPWV2] + b
5. Strengthens and Limitation of CAVI
6. Arterial Stiffness and Organ Damage
7. CAVI and Diagnosis of Diastolic Dysfunction and Heart Failure with Preserved Ejection Fraction
8. CAVI and Cardiovascular Risk Factors
9. CAVI and Adverse Cardiovascular Events
10. CAVI and Prognosis of Heart Failure
11. Future Perspective
12. Conclusions
Funding
Conflicts of Interest
References
- Shirai, K.; Saiki, A.; Nagayama, D.; Tatsuno, I.; Shimizu, K.; Takahashi, M. The Role of Monitoring Arterial Stiffness with Cardio-Ankle Vascular Index in the Control of Lifestyle-Related Diseases. Pulse 2015, 3, 118–133. [Google Scholar] [CrossRef] [PubMed]
- Shirai, K.; Utino, J.; Otsuka, K.; Takata, M. A Novel Blood Pressure-independent Arterial Wall Stiffness Parameter; Cardio-Ankle Vascular Index (CAVI). J. Atheroscler. Thromb. 2006, 13, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Handa, H.; Nagasawa, S.; Okumura, A.; Moritake, K. Stiffness and elastic behavior of human intracranial and extracranial arteries. J. Biomech. 1980, 13, 175–184. [Google Scholar] [CrossRef]
- Cocciolone, A.J.; Hawes, J.Z.; Staiculescu, M.C.; Johnson, E.O.; Murshed, M.; Wagenseil, J.E. Elastin, arterial mechanics, and cardiovascular disease. Am. J. Physiol. Circ. Physiol. 2018, 315, H189–H205. [Google Scholar] [CrossRef] [PubMed]
- Duca, L.; Blaise, S.; Romier, B.; Laffargue, M.; Gayral, S.; El Btaouri, H.; Kawecki, C.; Guillot, A.; Martiny, L.; Debelle, L.; et al. Matrix aging and vascular impacts: Focus on elastin fragmentation. Cardiovasc. Res. 2016, 110, 298–308. [Google Scholar] [CrossRef]
- Yu, Q.; Stamenkovic, I. Cell surface-localized matrix metalloproteinase-9 proteolytically activates TGF-beta and promotes tumor invasion and angiogenesis. Genes Dev. 2000, 14, 163–176. [Google Scholar] [PubMed]
- Xu, C.; Zarins, C.K.; Pannaraj, P.S.; Bassiouny, H.S.; Glagov, S. Hypercholesterolemia Superimposed by Experimental Hypertension Induces Differential Distribution of Collagen and Elastin. Arter. Thromb. Vasc. Boil. 2000, 20, 2566–2572. [Google Scholar] [CrossRef]
- O’Connell, M.K.; Murthy, S.; Phan, S.; Xu, C.; Buchanan, J.; Spilker, R.; Dalman, R.L.; Zarins, C.K.; Denk, W.; Taylor, C.A. The three-dimensional micro- and nanostructure of the aortic medial lamellar unit measured using 3D confocal and electron microscopy imaging. Matrix Biol. 2008, 27, 171–181. [Google Scholar] [CrossRef]
- Tsamis, A.; Krawiec, J.T.; Vorp, D.A. Elastin and collagen fibre microstructure of the human aorta in ageing and disease: A review. J. R. Soc. Interface 2013, 10, 20121004. [Google Scholar] [CrossRef]
- Muniyappa, R.; Sowers, J.R. Role of Insulin Resistance in Endothelial Dysfunction. Rev. Endocr. Metab. Disord. 2013, 14, 5–12. [Google Scholar] [CrossRef]
- Carreau, A.; Kieda, C.; Grillon, C. Nitric oxide modulates the expression of endothelial cell adhesion molecules involved in angiogenesis and leukocyte recruitment. Exp. Cell Res. 2011, 317, 29–41. [Google Scholar] [CrossRef]
- Apostoli, G.L.; Solomon, A.; Smallwood, M.J.; Winyard, P.G.; Emerson, M. Role of inorganic nitrate and nitrite in driving nitric oxide-cGMP-mediated inhibition of platelet aggregation in vitro and in vivo. J. Thromb. Haemost. 2014, 12, 1880–1889. [Google Scholar] [CrossRef]
- Qiu, J.; Zheng, Y.; Hu, J.; Liao, D.; Gregersen, H.; Deng, X.; Fan, Y.; Wang, G. Biomechanical regulation of vascular smooth muscle cell functions: From in vitro to in vivo understanding. J. R. Soc. Interface 2013, 11, 20130852. [Google Scholar] [CrossRef]
- Brandes, R.P.; Fleming, I.; Busse, R. Endothelial aging. Cardiovasc. Res. 2005, 66, 286–294. [Google Scholar] [CrossRef]
- Morris, S.M., Jr. Arginine Metabolism Revisited. J. Nutr. 2016, 146, 2579S–2586S. [Google Scholar] [CrossRef]
- Masaki, N.; Hakuno, D.; Toya, T.; Shiraishi, Y.; Kujiraoka, T.; Namba, T.; Yada, H.; Kimura, K.; Miyazaki, K.; Adachi, T. Association between brachial-ankle pulse wave velocity and the ratio of l-arginine to asymmetricdimethylarginine in patients undergoing coronary angiography. J. Cardiol. 2015, 65, 311–317. [Google Scholar] [CrossRef]
- Tang, W.H.W.; Wang, Z.; Cho, L.; Brennan, D.M.; Hazen, S.L. Diminished Global Arginine Bioavailability and Increased Arginine Catabolism as Metabolic Profile of Increased Cardiovascular Risk. J. Am. Coll. Cardiol. 2009, 53, 2061–2067. [Google Scholar] [CrossRef]
- Caldwell, R.W.; Rodriguez, P.C.; Toque, H.A.; Narayanan, S.P.; Caldwell, R.B. Arginase: A Multifaceted Enzyme Important in Health and Disease. Physiol. Rev. 2018, 98, 641–665. [Google Scholar] [CrossRef]
- Bhatta, A.; Yao, L.; Xu, Z.; Toque, H.A.; Chen, J.; Atawia, R.T.; Fouda, A.Y.; Bagi, Z.; Lucas, R.; Caldwell, R.B.; et al. Obesity-induced vascular dysfunction and arterial stiffening requires endothelial cell arginase 1. Cardiovasc. Res. 2017, 113, 1664–1676. [Google Scholar] [CrossRef]
- Zhang, Q.-J.; McMillin, S.L.; Tanner, J.M.; Palionyte, M.; Abel, E.D.; Symons, J.D. Endothelial nitric oxide synthase phosphorylation in treadmill-running mice: Role of vascular signalling kinases. J. Physiol. 2009, 587, 3911–3920. [Google Scholar] [CrossRef]
- Fulton, D.; Gratton, J.-P.; McCabe, T.J.; Fontana, J.; Fujio, Y.; Walsh, K.; Franke, T.F.; Papapetropoulos, A.; Sessa, W.C. Regulation of endothelium-derived nitric oxide production by the protein kinase Akt. Nature 1999, 399, 597–601. [Google Scholar] [CrossRef]
- Montagnani, M.; Chen, H.; Barr, V.A.; Quon, M.J. Insulin-stimulated activation of eNOS is independent of Ca2+ but requires phosphorylation by Akt at Ser(1179). J. Biol. Chem. 2001, 276, 30392–30398. [Google Scholar] [CrossRef]
- Gélinas, D.S.; Bernatchez, P.N.; Rollin, S.; Bazan, N.G.; Sirois, M.G. Immediate and delayed VEGF-mediated NO synthesis in endothelial cells: Role of PI3K, PKC and PLC pathways. Br. J. Pharmacol. 2002, 137, 1021–1030. [Google Scholar] [CrossRef]
- Luiking, Y.C.; Have, G.A.M.T.; Wolfe, R.R.; Deutz, N.E.P. Arginine de novo and nitric oxide production in disease states. Am. J. Physiol. Metab. 2012, 303, E1177–E1189. [Google Scholar] [CrossRef]
- Shi, W.; Meininger, C.J.; Haynes, T.E.; Hatakeyama, K.; Wu, G. Regulation of Tetrahydrobiopterin Synthesis and Bioavailability in Endothelial Cells. Cell Biophys. 2004, 41, 415–434. [Google Scholar] [CrossRef]
- Crabtree, M.J.; Channon, K.M. Synthesis and recycling of tetrahydrobiopterin in endothelial function and vascular disease. Nitric Oxide 2011, 25, 81–88. [Google Scholar] [CrossRef]
- Soucy, K.G.; Ryoo, S.; Benjo, A.; Lim, H.K.; Gupta, G.; Sohi, J.S.; Elser, J.; Aon, M.A.; Nyhan, D.; Shoukas, A.A.; et al. Impaired shear stress-induced nitric oxide production through decreased NOS phosphorylation contributes to age-related vascular stiffness. J. Appl. Physiol. 2006, 101, 1751–1759. [Google Scholar] [CrossRef]
- Jung, S.M.; Jandu, S.; Steppan, J.; Belkin, A.; An, S.S.; Pak, A.; Choi, E.Y.; Nyhan, D.; Butlin, M.; Viegas, K.; et al. Increased tissue transglutaminase activity contributes to central vascular stiffness in eNOS knockout mice. Am. J. Physiol. Circ. Physiol. 2013, 305, H803–H810. [Google Scholar] [CrossRef]
- Chang, H.C.; Guarente, L. SIRT1 and other sirtuins in metabolism. Trends Endocrinol. Metab. 2014, 25, 138–145. [Google Scholar] [CrossRef]
- Rahman, S.; Islam, R. Mammalian Sirt1: Insights on its biological functions. Cell Commun. Signal. 2011, 9, 11. [Google Scholar] [CrossRef]
- Zu, Y.; Liu, L.; Lee, M.Y.; Xu, C.; Liang, Y.; Man, R.Y.; Vanhoutte, P.M.; Wang, Y. SIRT1 Promotes Proliferation and Prevents Senescence Through Targeting LKB1 in Primary Porcine Aortic Endothelial Cells. Circ. Res. 2010, 106, 1384–1393. [Google Scholar] [CrossRef]
- Zarzuelo, M.J.; López-Sepúlveda, R.; Sanchez, M.; Romero, M.; Gomez-Guzman, M.; Ungvary, Z.; Pérez-Vizcaíno, F.; Jimenez, R.; Duarte, J. SIRT1 inhibits NADPH oxidase activation and protects endothelial function in the rat aorta: Implications for vascular aging. Biochem. Pharmacol. 2013, 85, 1288–1296. [Google Scholar] [CrossRef]
- Gogulamudi, V.R.; Cai, J.; Lesniewski, L.A. Reversing age-associated arterial dysfunction: Insight from preclinical models. J. Appl. Physiol. 2018, 125, 1860–1870. [Google Scholar] [CrossRef]
- Fry, J.L.; Al Sayah, L.; Weisbrod, R.M.; Van Roy, I.; Weng, X.; Cohen, R.A.; Bachschmid, M.M.; Seta, F. Vascular Smooth Muscle Sirtuin-1 Protects Against Diet-Induced Aortic Stiffness. Hypertension 2016, 68, 775–784. [Google Scholar] [CrossRef]
- Nisoli, E.; Tonello, C.; Cardile, A.; Cozzi, V.; Tedesco, L.; Falcone, S.; Carruba, M.O.; Bracale, R.; Valerio, A.; Cantoni, O.; et al. Calorie Restriction Promotes Mitochondrial Biogenesis by Inducing the Expression of eNOS. Science 2005, 310, 314–317. [Google Scholar] [CrossRef]
- Gao, D.; Zuo, Z.; Tian, J.; Ali, Q.; Lin, Y.; Lei, H.; Sun, Z. Activation of SIRT1 Attenuates Klotho Deficiency-Induced Arterial Stiffness and Hypertension by Enhancing AMP-Activated Protein Kinase Activity. Hypertension 2016, 68, 1191–1199. [Google Scholar] [CrossRef]
- Ding, Y.; Han, Y.; Lu, Q.; An, J.; Zhu, H.; Xie, Z.; Song, P.; Zou, M.-H. Peroxynitrite-Mediated SIRT (Sirtuin)-1 Inactivation Contributes to Nicotine-Induced Arterial Stiffness in Mice. Arter. Thromb. Vasc. Boil. 2019, 39, 1419–1431. [Google Scholar] [CrossRef]
- Guzik, T.J.; Touyz, R.M. Oxidative Stress, Inflammation, and Vascular Aging in Hypertension. Hypertension 2017, 70, 660–667. [Google Scholar] [CrossRef]
- Payne, R.A.; Wilkinson, I.B.; Webb, D.J. Arterial stiffness and hypertension: Emerging concepts. Hypertension 2010, 55, 9–14. [Google Scholar] [CrossRef]
- Briet, M.; Boutouyrie, P.; Laurent, S.; London, G.M. Arterial stiffness and pulse pressure in CKD and ESRD. Kidney Int. 2012, 82, 388–400. [Google Scholar] [CrossRef]
- Goldsmith, D.; Ritz, E.; Covic, A. Vascular calcification: A stiff challenge for the nephrologist: Does preventing bone disease cause arterial disease? Kidney Int. 2004, 66, 1315–1333. [Google Scholar] [CrossRef]
- Nitta, K. Vascular calcification in patients with chronic kidney disease. Ther. Apher. Dial. 2011, 15, 513–521. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Guo, C.-Y.; Benjamin, E.; Larson, M.G.; Keyes, M.J.; Vita, J.; Vasan, R.S.; Levy, D. Cross-Sectional Correlates of Increased Aortic Stiffness in the Community: The Framingham Heart Study. Circulation 2007, 115, 2628–2636. [Google Scholar] [CrossRef]
- Boesen, M.E.; Singh, D.; Menon, B.K.; Frayne, R. A systematic literature review of the effect of carotid atherosclerosis on local vessel stiffness and elasticity. Atherosclerosis 2015, 243, 211–222. [Google Scholar] [CrossRef]
- Whitlock, M.C.; Hundley, W.G. Non-invasive imaging of flow and vascular function in disease of the aorta. JACC: Cardiovasc. Imaging 2015, 8, 1094–1106. [Google Scholar]
- Poleszczuk, J.; Debowska, M.; Dabrowski, W.; Wojcik-Zaluska, A.; Zaluska, W.; Waniewski, J. Subject-specific pulse wave propagation modeling: Towards enhancement of cardiovascular assessment methods. PLoS ONE 2018, 13, e0190972. [Google Scholar] [CrossRef]
- Benetos, A.; Thomas, F.; Joly, L.; Blacher, J.; Pannier, B.; Labat, C.; Salvi, P.; Smulyan, H.; Safar, M.E. Pulse pressure amplification a mechanical biomarker of cardiovascular risk. J. Am. Coll. Cardiol. 2010, 55, 1032–1037. [Google Scholar] [CrossRef]
- Laskey, W.K.; Wu, J.; Schulte, P.J.; Hernandez, A.F.; Yancy, C.W.; Heidenreich, P.A.; Bhatt, D.L.; Fonarow, G.C. Association of Arterial Pulse Pressure With Long-Term Clinical Outcomes in Patients With Heart Failure. JACC: Hear. Fail. 2016, 4, 42–49. [Google Scholar] [CrossRef]
- Ghiadoni, L.; Bruno, R.M.; Stea, F.; Virdis, A.; Taddei, S. Central blood pressure, arterial stiffness, and wave reflection: New targets of treatment in essential hypertension. Curr. Hypertens. Rep. 2009, 11, 190–196. [Google Scholar] [CrossRef]
- Wilkinson, I.B.; MacCallum, H.; Flint, L.; Cockcroft, J.R.; Newby, D.E.; Webb, D.J. AI The influence of heart rate on augmentation index and central arterial pressure in humans. J. Physiol. 2000, 525, 263–270. [Google Scholar] [CrossRef]
- Scandale, G.; Dimitrov, G.; Recchia, M.; Carzaniga, G.; Minola, M.; Perilli, E.; Carotta, M.; Catalano, M. Arterial stiffness and subendocardial viability ratio in patients with peripheral arterial disease. J. Clin. Hypertens. 2018, 20, 478–484. [Google Scholar] [CrossRef]
- Asmar, R.; Benetos, A.; Topouchian, J.; Laurent, P.; Pannier, B.; Brisac, A.-M.; Target, R.; Levy, B.I. Assessment of Arterial Distensibility by Automatic Pulse Wave Velocity Measurement. Hypertension 1995, 26, 485–490. [Google Scholar] [CrossRef]
- Millasseau, S.C.; Stewart, A.D.; Patel, S.J.; Redwood, S.R.; Chowienczyk, P.J. Evaluation of carotid-femoral pulse wave velocity: Influence of timing algorithm and heart rate. Hypertension 2005, 45, 222–226. [Google Scholar] [CrossRef]
- Liu, S.; Kim, E.D.; Wu, A.; Meyer, M.L.; Cheng, S.; Hoogeveen, R.C.; Ballantyne, C.M.; Tanaka, H.; Heiss, G.; Selvin, E.; et al. Central and peripheral pulse wave velocity and subclinical myocardial stress and damage in older adults. PLoS ONE 2019, 14, e0212892. [Google Scholar] [CrossRef]
- Yamashina, A.; Tomiyama, H.; Takeda, K.; Tsuda, H.; Arai, T.; Hirose, K.; Koji, Y.; Hori, S.; Yamamoto, Y. Validity, Reproducibility, and Clinical Significance of Noninvasive Brachial-Ankle Pulse Wave Velocity Measurement. Hypertens. Res. 2002, 25, 359–364. [Google Scholar] [CrossRef]
- Matsui, Y.; Kario, K.; Ishikawa, J.; Eguchi, K.; Hoshide, S.; Shimada, K. Reproducibility of Arterial Stiffness Indices (Pulse Wave Velocity and Augmentation Index) Simultaneously Assessed by Automated Pulse Wave Analysis and Their Associated Risk Factors in Essential Hypertensive Patients. Hypertens. Res. 2004, 27, 851–857. [Google Scholar] [CrossRef]
- Dhindsa, M.; Sommerlad, S.M.; DeVan, A.E.; Barnes, J.N.; Sugawara, J.; Ley, O.; Tanaka, H. Interrelationships among noninvasive measures of postischemic macro- and microvascular reactivity. J. Appl. Physiol. 2008, 105, 427–432. [Google Scholar] [CrossRef]
- Allan, R.; Delaney, C.; Miller, M.; Spark, J.; Allan, R.; Miller, M. A Comparison of Flow-mediated Dilatation and Peripheral Artery Tonometry for Measurement of Endothelial Function in Healthy Individuals and Patients with Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 263–269. [Google Scholar] [CrossRef]
- Akima, T.; Makkar, R.; Nishioka, T.; Dohad, S.; Iida, K.; Goland, S.; Kar, S.; Luo, H.; Siegel, R.J. Impact of nitroglycerin and verapamil on coronary arterial distensibility as assessed by intravascular ultrasound. J. Invasive Cardiol. 2009, 21, 162–167. [Google Scholar]
- Sasaki, O.; Nishioka, T.; Inoue, Y.; Isshiki, A.; Akima, T.; Toyama, K.; Koike, A.; Ando, T.; Yuhara, M.; Sato, S.-I.; et al. Longitudinal heterogeneity of coronary artery distensibility in plaques related to acute coronary syndrome. Clin. Res. Cardiol. 2012, 101, 545–551. [Google Scholar] [CrossRef]
- Bramwell, J.C.; Hill, A.V. The Velocity of the Pulse Wave in Man. Proc. R. Soc. B Boil. Sci. 1922, 93, 298–306. [Google Scholar] [CrossRef]
- Hasegawa, M. Fundamental research on human aortic pulse wave velocity. Jikei Med. J. 1970, 85, 742–760. [Google Scholar]
- Hasegawa, M.; Arai, C. Clinical estimation of vascular elastic function and practical application. Connect. Tissue 1995, 27, 149–157. [Google Scholar]
- Takahashi, K.; Yamamoto, T.; Tsuda, S.; Okabe, F.; Shimose, T.; Tsuji, Y.; Suzuki, K.; Otsuka, K.; Takata, M.; Shimizu, K.; et al. Coefficients in the CAVI Equation and the Comparison Between CAVI With and Without the Coefficients Using Clinical Data. J. Atheroscler. Thromb. 2019, 26, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, T.; Ito, H. Assessment of Arterial Stiffness Using the Cardio-Ankle Vascular Index. Pulse 2016, 4, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Boardman, H.; Lewandowski, A.J.; Lazdam, M.; Kenworthy, Y.; Whitworth, P.; Zwager, C.L.; Francis, J.M.; Aye, C.Y.; Williamson, W.; Neubauer, S.; et al. Aortic stiffness and blood pressure variability in young people: A multimodality investigation of central and peripheral vasculature. J. Hypertens. 2017, 35, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Takaki, A.; Ogawa, H.; Wakeyama, T.; Iwami, T.; Kimura, M.; Hadano, Y.; Matsuda, S.; Miyazaki, Y.; Matsuda, T.; Hiratsuka, A.; et al. Cardio-Ankle Vascular Index is a New Noninvasive Parameter of Arterial Stiffness. Circ. J. 2007, 71, 1710–1714. [Google Scholar] [CrossRef]
- Horinaka, S.; Yagi, H.; Ishimura, K.; Fukushima, H.; Shibata, Y.; Sugawara, R.; Ishimitsu, T. Cardio-ankle vascular index (CAVI) correlates with aortic stiffness in the thoracic aorta using ECG-gated multi-detector row computed tomography. Atherosclerosis 2014, 235, 239–245. [Google Scholar] [CrossRef]
- Yambe, T.; Yoshizawa, M.; Saijo, Y.; Yamaguchi, T.; Shibata, M.; Konno, S.; Nitta, S.; Kuwayama, T. Brachio-ankle pulse wave velocity and cardio-ankle vascular index (CAVI). Biomed. Pharmacother. 2004, 58, S95–S98. [Google Scholar] [CrossRef]
- Shirai, K.; Hiruta, N.; Song, M.; Kurosu, T.; Suzuki, J.; Tomaru, T.; Miyashita, Y.; Saiki, A.; Takahashi, M.; Suzuki, K.; et al. Cardio-ankle vascular index (CAVI) as a novel indicator of arterial stiffness: Theory, evidence and perspectives. J. Atheroscler. Thromb. 2011, 18, 924–938. [Google Scholar] [CrossRef]
- Kubozono, T.; Miyata, M.; Ueyama, K.; Nagaki, A.; Otsuji, Y.; Kusano, K.; Kubozono, O.; Tei, C. Clinical Significance and Reproducibility of New Arterial Distensibility Index. Circ. J. 2007, 71, 89–94. [Google Scholar] [CrossRef]
- Ibata, J.; Sasaki, H.; Kakimoto, T.; Matsuno, S.; Nakatani, M.; Kobayashi, M.; Tatsumi, K.; Nakano, Y.; Wakasaki, H.; Furuta, H.; et al. Cardio-ankle vascular index measures arterial wall stiffness independent of blood pressure. Diabetes Res. Clin. Pr. 2008, 80, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Pearman, M.E.; Park, W.; Alkatan, M.; Machin, D.R.; Tanaka, H. Impact of blood pressure perturbations on arterial stiffness. Am. J. Physiol. Integr. Comp. Physiol. 2015, 309, 1540–1545. [Google Scholar] [CrossRef] [PubMed]
- Shirai, K.; Song, M.; Suzuki, J.; Kurosu, T.; Oyama, T.; Nagayama, D.; Miyashita, Y.; Yamamura, S.; Takahashi, M. Contradictory effects of β1- and α1- aderenergic receptor blockers on cardio-ankle vascular stiffness index (CAVI)--CAVI independent of blood pressure. J. Atheroscler. Thromb. 2011, 18, 49–55. [Google Scholar] [CrossRef]
- Williams, B. Evaluating interventions to reduce central aortic pressure, arterial stiffness and morbidity–mortality. J. Hypertens. 2012, 30, S13–S18. [Google Scholar] [CrossRef] [PubMed]
- Masugata, H.; Senda, S.; Okuyama, H.; Murao, K.; Inukai, M.; Hosomi, N.; Yukiiri, K.; Nishiyama, A.; Kohno, M.; Goda, F. Comparison of central blood pressure and cardio-ankle vascular index for association with cardiac function in treated hypertensive patients. Hypertens. Res. 2009, 32, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Gohbara, M.; Iwahashi, N.; Sano, Y.; Akiyama, E.; Maejima, N.; Tsukahara, K.; Hibi, K.; Kosuge, M.; Ebina, T.; Umemura, S.; et al. Clinical Impact of the Cardio-Ankle Vascular Index for Predicting Cardiovascular Events After Acute Coronary Syndrome. Circ. J. 2016, 80, 1420–1426. [Google Scholar] [CrossRef]
- Mei, C.C.; Zhang, J.; Jing, H.X. Fluid mechanics of Windkessel effect. Med Boil. Eng. 2018, 56, 1357–1366. [Google Scholar] [CrossRef]
- Fujimoto, N.; Onishi, K.; Dohi, K.; Tanabe, M.; Kurita, T.; Takamura, T.; Yamada, N.; Nobori, T.; Ito, M. Hemodynamic Characteristics of Patients with Diastolic Heart Failure and Hypertension. Hypertens. Res. 2008, 31, 1727–1735. [Google Scholar] [CrossRef][Green Version]
- O’Rourke, M.F.; Hashimoto, J. Mechanical factors in arterial aging: A clinical perspective. J. Am. Coll. Cardiol. 2007, 50, 1–13. [Google Scholar] [CrossRef]
- Hori, M.; Inoue, M.; Kitakaze, M.; Tsujioka, K.; Ishida, Y.; Fukunami, M.; Nakajima, S.; Kitabatake, A.; Abe, H. Loading sequence is a major determinant of afterload-dependent relaxation in intact canine heart. Am. J. Physiol. Circ. Physiol. 1985, 249, H747–H754. [Google Scholar] [CrossRef] [PubMed]
- Mottram, P.M.; Haluska, B.A.; Leano, R.; Carlier, S.; Case, C.; Marwick, T.H. Relation of arterial stiffness to diastolic dysfunction in hypertensive heart disease. Heart 2005, 91, 1551–1556. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuka, S.; Kakihana, M.; Watanabe, H.; Sugishita, Y. Chronically decreased aortic distensibility causes deterioration of coronary perfusion during increased left ventricular contraction. J. Am. Coll. Cardiol. 1994, 24, 1406–1414. [Google Scholar] [CrossRef]
- Tritakis, V.; Tzortzis, S.; Ikonomidis, I.; Dima, K.; Pavlidis, G.; Trivilou, P.; Paraskevaidis, I.; Katsimaglis, G.; Parissis, J.; Lekakis, J. Association of arterial stiffness with coronary flow reserve in revascularized coronary artery disease patients. World J. Cardiol. 2016, 8, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.P.; Tunin, R.; Kass, D.A. Effect of reduced aortic compliance on cardiac efficiency and contractile function of in situ canine left ventricle. Circ. Res. 1992, 71, 490–502. [Google Scholar] [CrossRef] [PubMed]
- Berbari, A.; Mancia, G. Arterial Disorders: Definition, Clinical Manifestations, Mechanisms and Therapeutic Approaches, Chapter 26, Arterial Function; Springer International Publishing: Cham, Switzerland, 2015; pp. 373–375. [Google Scholar]
- Cardoso, C.R.; Ferreira, M.T.; Leite, N.C.; Barros, P.N.; Conte, P.H.; Salles, G.F. Microvascular degenerative complications are associated with increased aortic stiffness in type 2 diabetic patients. Atherosclerosis 2009, 205, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.J.; Park, C.-Y.; Park, S.E.; Rhee, E.J.; Lee, W.Y.; Oh, K.W.; Park, S.W.; Kim, S.W.; Song, S. The association between regional arterial stiffness and diabetic retinopathy in type 2 diabetes. Atherosclerosis 2012, 225, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Karalliedde, J.; De Angelis, L.; Goldsmith, D.; Viberti, G. Aortic Pulse Wave Velocity and Albuminuria in Patients with Type 2 Diabetes. J. Am. Soc. Nephrol. 2005, 16, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- O’Rourke, M.F.; Safar, M.E. Relationship between aortic stiffening and microvascular disease in brain and kidney: Cause and logic of therapy. Hypertension 2005, 46, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Owan, T.E.; Herges, R.M.; Jacobsen, S.J.; Hodge, D.O.; Roger, V.L.; Redfield, M.M. Trends in Prevalence and Outcome of Heart Failure with Preserved Ejection Fraction. New Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef]
- Tsuchihashi-Makaya, M.; Hamaguchi, S.; Kinugawa, S.; Yokota, T.; Goto, D.; Yokoshiki, H.; Kato, N.; Takeshita, A.; Tsutsui, H.; for the JCARE-CARD Investigators. Characteristics and Outcomes of Hospitalized Patients With Heart Failure and Reduced vs Preserved Ejection Fraction. Circ. J. 2009, 73, 1893–1900. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics--2013 update: A report from the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, P.; Gaggin, H.K.; Dec, G.W. ACC/AHA Versus ESC Guidelines on Heart Failure: JACC Guideline Comparison. J. Am. Coll. Cardiol. 2019, 73, 2756–2768. [Google Scholar] [CrossRef] [PubMed]
- Hogg, K.; Swedberg, K.; McMurray, J. Heart failure with preserved left ventricular systolic function; epidemiology, clinical characteristics, and prognosis. J. Am. Coll. Cardiol. 2004, 43, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.S.; Xu, H.; Matsouaka, R.A.; Bhatt, D.L.; Heidenreich, P.A.; Hernandez, A.F.; Devore, A.D.; Yancy, C.W.; Fonarow, G.C. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J. Am. Coll. Cardiol. 2017, 70, 2476–2486. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the Diagnosis and Treatment Of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Kawaguchi, M.; Hay, I.; Fetics, B.; Kass, D.A. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: Implications for systolic and diastolic reserve limitations. Circulation 2003, 107, 714–720. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Roger, V.L.; Rodeheffer, R.J.; Bursi, F.; Borlaug, B.A.; Ommen, S.R.; Kass, D.A.; Redfield, M.M. Cardiac structure and ventricular-vascular function in persons with heart failure and preserved ejection fraction from Olmsted County, Minnesota. Circulation 2007, 115, 1982–1990. [Google Scholar] [CrossRef]
- Meguro, T.; Nagatomo, Y.; Nagae, A.; Seki, C.; Kondou, N.; Shibata, M.; Oda, Y. Elevated Arterial Stiffness Evaluated by Brachial-Ankle Pulse Wave Velocity is Deleterious for the Prognosis of Patients With Heart Failure. Circ. J. 2009, 73, 673–680. [Google Scholar] [CrossRef]
- Zile, M.; Baicu, C.; Gaasch, W. Diastolic heart failure-abnormalities in active relaxation and passive stiffness of the left ventricle. ACC Curr. J. Rev. 2004, 13, 36. [Google Scholar] [CrossRef]
- Kasner, M.; Westermann, D.; Steendijk, P.; Gaub, R.; Wilkenshoff, U.; Weitmann, K.; Hoffmann, W.; Poller, W.; Schultheiss, H.P.; Pauschinger, M.; et al. Utility of Doppler echocardiography and tissue Doppler imaging in the estimation of diastolic function in heart failure with normal ejection fraction: A comparative Doppler-conductance catheterization study. Circulation 2007, 116, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Mitter, S.S.; Shah, S.J.; Thomas, J.D. A Test in Context: E/A and E/e’ to Assess Diastolic Dysfunction and LV Filling Pressure. J. Am. Coll. Cardiol. 2017, 69, 1451–1464. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef] [PubMed]
- Sakane, K.; Miyoshi, T.; Doi, M.; Hirohata, S.; Kaji, Y.; Kamikawa, S.; Ogawa, H.; Hatanaka, K.; Kitawaki, T.; Kusachi, S.; et al. Association of new arterial stiffness parameter, the cardio-ankle vascular index, with left ventricular diastolic function. Heart 2005, 91, 1551–1556. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, T.; Doi, M.; Hirohata, S.; Sakane, K.; Kamikawa, S.; Kitawaki, T.; Kaji, Y.; Kusano, K.F.; Ninomiya, Y.; Kusachi, S. Cardio-Ankle Vascular Index is Independently Associated with the Severity of Coronary Atherosclerosis and Left Ventricular Function in Patients with Ischemic Heart Disease. J. Atheroscler. Thromb. 2010, 17, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Takeda, K.; Turuya, K.; Mukai, H.; Muto, Y.; Okuda, H.; Furusho, M.; Ueno, T.; Nakashita, S.; Miura, S.; et al. Left Ventricular Mass Index Is an Independent Determinant of Diastolic Dysfunction in Patients on Chronic Hemodialysis: A Tissue Doppler Imaging Study. Nephron Clin. Pr. 2011, 117, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Masugata, H.; Senda, S.; Goda, F.; Yamagami, A.; Okuyama, H.; Kohno, T.; Hosomi, N.; Yukiiri, K.; Noma, T.; Kiyomoto, H.; et al. Tissue Doppler Echocardiography for Predicting Arterial Stiffness Assessed by Cardio-Ankle Vascular Index. Tohoku J. Exp. Med. 2009, 217, 139–146. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Masaki, M.; Komamura, K.; Goda, A.; Hirotani, S.; Otsuka, M.; Nakabo, A.; Fukui, M.; Fujiwara, S.; Sugahara, M.; Lee-Kawabata, M.; et al. Elevated arterial stiffness and diastolic dysfunction in subclinical hypothyroidism. Circ. J. 2014, 78, 1494–1500. [Google Scholar] [CrossRef] [PubMed]
- Namba, T.; Masaki, N.; Matsuo, Y.; Sato, A.; Kimura, T.; Horii, S.; Yasuda, R.; Yada, H.; Kawamura, A.; Takase, B.; et al. Arterial Stiffness Is Significantly Associated With Left Ventricular Diastolic Dysfunction in Patients With Cardiovascular Disease. Int. Hear. J. 2016, 57, 729–735. [Google Scholar] [CrossRef]
- Osawa, K.; Nakanishi, R.; Miyoshi, T.; Rahmani, S.; Ceponiene, I.; Nezarat, N.; Kanisawa, M.; Qi, H.; Jayawardena, E.; Kim, N.; et al. Correlation of Arterial Stiffness With Left Atrial Volume Index and Left Ventricular Mass Index in Young Adults: Evaluation by Coronary Computed Tomography Angiography. Heart Lung Circ. 2019, 28, 932–938. [Google Scholar] [CrossRef]
- Wang, J.; Khoury, D.S.; Thohan, V.; Torre-Amione, G.; Nagueh, S.F. Global Diastolic Strain Rate for the Assessment of Left Ventricular Relaxation and Filling Pressures. Circualation 2007, 115, 1376–1383. [Google Scholar] [CrossRef] [PubMed]
- Dokainish, H.; Sengupta, R.; Pillai, M.; Bobek, J.; Lakkis, N. Usefulness of New Diastolic Strain and Strain Rate Indexes for the Estimation of Left Ventricular Filling Pressure. Am. J. Cardiol. 2008, 101, 1504–1509. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Addetia, K.; Maffessanti, F.; Mor-Avi, V.; Lang, R.M. LA strain for categorization of LV diastolic dysfunction. J. Am. Coll. Cardiol. Imging 2017, 10, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Mizuguchi, Y.; Oishi, Y.; Tanaka, H.; Miyoshi, H.; Ishimoto, T.; Nagase, N.; Oki, T. Arterial Stiffness Is Associated With Left Ventricular Diastolic Function in Patients With Cardiovascular Risk Factors: Early Detection With the Use of Cardio-Ankle Vascular Index and Ultrasonic Strain Imaging. J. Card. Fail. 2007, 13, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Hitsumoto, T.; Shirai, K. Factors affecting high-sensitivity cardiac troponin T elevation in Japanese metabolic syndrome patients. Diabetes Metab. Syndr. Obesity: Targets Ther. 2015, 8, 157–162. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kubozono, T.; Miyata, M.; Ueyama, K.; Nagaki, A.; Hamasaki, S.; Kusano, K.; Kubozono, O.; Tei, C. Association between arterial stiffness and estimated glomerular filtration rate in the Japanese general population. J. Atheroscler. Thromb. 2009, 16, 840–845. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chen, Y.; Liu, J.H.; Zhen, Z.; Zuo, Y.; Lin, Q.; Liu, M.; Zhao, C.; Wu, M.; Cao, G.; Wang, R.; et al. Assessment of left ventricular function and peripheral vascular arterial stiffness in patients with dipper and non-dipper hypertension. J. Investig. Med. 2018, 66, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Yoshihisa, A.; Kanno, Y.; Takiguchi, M.; Sato, A.; Miura, S.; Nakamura, Y.; Yamauchi, H.; Owada, T.; Abe, S.; et al. Relationship of hyperuricemia with mortality in heart failure patients with preserved ejection fraction. Am. J. Physiol. Circ. Physiol. 2015, 309, H1123–H1129. [Google Scholar] [CrossRef] [PubMed]
- Soska, V.; Frantisova, M.; Dobsak, P.; Dusek, L.; Jarkovsky, J.; Novakova, M.; Shirai, K.; Fajkusova, L.; Freiberger, T. Cardio-ankle vascular index in subjects with dyslipidaemia and other cardiovascular risk factors. J. Atheroscler. Thromb. 2013, 20, 443–451. [Google Scholar] [CrossRef]
- Chung, S.-L.; Yang, C.-C.; Chen, C.-C.; Hsu, Y.-C.; Lei, M.-H. Coronary Artery Calcium Score Compared with Cardio-Ankle Vascular Index in the Prediction of Cardiovascular Events in Asymptomatic Patients with Type 2 Diabetes. J. Atheroscler. Thromb. 2015, 22, 1255–1265. [Google Scholar] [CrossRef]
- Lee, C.-J.; Wang, J.-H.; Chen, M.-L.; Yang, C.-F.; Chen, Y.-C.; Hsu, B.-G. Serum Osteoprotegerin is Associated with Arterial Stiffness Assessed According to the Cardio-ankle Vascular Index in Hypertensive Patients. J. Atheroscler. Thromb. 2015, 22, 304–312. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ando, A.; Miyamoto, M.; Kotani, K.; Okada, K.; Nagasaka, S.; Ishibashi, S.; Ando, A. Cardio-Ankle Vascular Index and Indices of Diabetic Polyneuropathy in Patients with Type 2 Diabetes. J. Diabetes Res. 2017, 2017, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, T.; Doi, M.; Noda, Y.; Ohno, Y.; Sakane, K.; Kamikawa, S.; Noguchi, Y.; Ito, H. Arterial stiffness determined according to the cardio-ankle vascular index is associated with paroxysmal atrial fibrillation: A cross-sectional study. Hear. Asia 2014, 6, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Trakarnvanich, T.; Prommool, S.; Kurathong, S.; Teepprasan, T.; Wang, Y. Associations Among Cardio-Ankle Vascular Index, Carotid Intima-Media Thickness, and Fibroblast Growth Factor-21 Levels in Kidney Transplant Patients. Transplant. Proc. 2017, 49, 1791–1796. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Tomaru, T.; Yamamura, S.; Miyashita, Y.; Shirai, K.; Noike, H. Cardio-ankle vascular index is a candidate predictor of coronary atherosclerosis. Circ. J. 2008, 72, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Marcos, M.A.; Recio-Rodríguez, J.I.; Patino-Alonso, M.C.; Agudo-Conde, C.; Gómez-Sanchez, L.; Gomez-Sanchez, M.; Rodríguez-Sánchez, E.; Maderuelo-Fernández, J.; Maderuelo-Fernandez, J.A.; García-Ortiz, L. Cardio-ankle vascular index is associated with cardiovascular target organ damage and vascular structure and function in patients with diabetes or metabolic syndrome, LOD-DIABETES study: A case series report. Cardiovasc. Diabetol. 2015, 14, 41. [Google Scholar] [CrossRef] [PubMed]
- Okura, T.; Watanabe, S.; Kurata, M.; Manabe, S.; Koresawa, M.; Irita, J.; Enomoto, D.; Miyoshi, K.-I.; Fukuoka, T.; Higaki, J. Relationship between Cardio-Ankle Vascular Index (CAVI) and Carotid Atherosclerosis in Patients with Essential Hypertension. Hypertens. Res. 2007, 30, 335–340. [Google Scholar] [CrossRef]
- Miki, K.; Nakano, M.; Aizawa, K.; Hasebe, Y.; Kimura, Y.; Morosawa, S.; Akashi, T.; Morishita, Y.; Miyata, S.; Fukuda, K.; et al. Risk factors and localization of silent cerebral infarction in patients with atrial fibrillation. Heart Rhythm. 2019. [Google Scholar] [CrossRef] [PubMed]
- Hitsumoto, T. Clinical Significance of Skin Autofluorescence in Patients With Type 2 Diabetes Mellitus With Chronic Heart Failure. Cardiol. Res. 2018, 9, 83–89. [Google Scholar] [CrossRef]
- Tanaka, H.; Tomoto, T.; Kosaki, K.; Sugawara, J. Arterial Stiffness of Lifelong Japanese Female Pearl Divers. Am. J. Physiol. Integr. Comp. Physiol. 2016, 310, 975–978. [Google Scholar] [CrossRef]
- Nakagawa, R.; Kuwata, S.; Kurishima, C.; Saiki, H.; Iwamoto, Y.; Sugimoto, M.; Ishido, H.; Masutani, S.; Senzaki, H. Arterial stiffness in patients after Kawasaki disease without coronary artery involvement: Assessment by performing brachial ankle pulse wave velocity and cardio-ankle vascular index. J. Cardiol. 2015, 66, 130–134. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Uurtuya, S.; Taniguchi, N.; Kotani, K.; Yamada, T.; Kawano, M.; Khurelbaatar, N.; Itoh, K.; Lkhagvasuren, T. Comparative study of the cardio-ankle vascular index and ankle–brachial index between young Japanese and Mongolian subjects. Hypertens. Res. 2009, 32, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Sorokin, A.; Kotani, K.; Bushueva, O.; Taniguchi, N.; Lazarenko, V. The Cardio-Ankle Vascular Index and Ankle-Brachial Index in Young Russians. J. Atheroscler. Thromb. 2015, 22, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Yingchoncharoen, T.; Sritara, P. Cardio-Ankle Vascular Index in a Thai Population. Pulse 2017, 4, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Sorokin, A.V.; Kotani, K.; Bushueva, O.Y.; Polonikov, A.V. Antioxidant-related gene polymorphisms associated with the cardio-ankle vascular index in young Russians. Cardiol. Young 2016, 26, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Nagayama, D.; Saiki, A.; Watanabe, R.; Watanabe, Y.; Imamura, H.; Yamaguchi, T.; Ban, N.; Kawana, H.; Nagumo, A.; et al. Cardio-Ankle Vascular Index is Independently Associated with Future Cardiovascular Events in Outpatients with Metabolic Disorders. J. Atheroscler. Thromb. 2016, 23, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Hitsumoto, T. Clinical Usefulness of the Cardio-Ankle Vascular Index as a Predictor of Primary Cardiovascular Events in Patients with Chronic Kidney Disease. J. Clin. Med. Res. 2018, 10, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Satoh-Asahara, N.; Kotani, K.; Yamakage, H.; Yamada, T.; Araki, R.; Okajima, T.; Adachi, M.; Oishi, M.; Shimatsu, A.; Ooishi, M. Cardio-ankle vascular index predicts for the incidence of cardiovascular events in obese patients: A multicenter prospective cohort study (Japan Obesity and Metabolic Syndrome Study: JOMS). Atherosclerosis 2015, 242, 461–468. [Google Scholar] [CrossRef]
- Matsushita, K.; Ding, N.; Kim, E.D.; Budoff, M.; Chirinos, J.A.; Fernhall, B.; Hamburg, N.M.; Kario, K.; Miyoshi, T.; Tanaka, H.; et al. Cardio-ankle vascular index and cardiovascular disease: Systematic review and meta-analysis of prospective and cross-sectional studies. J. Clin. Hypertens. 2019, 21, 16–24. [Google Scholar] [CrossRef]
- Tanaka, A.; Tomiyama, H.; Maruhashi, T.; Matsuzawa, Y.; Miyoshi, T.; Kabutoya, T.; Kario, K.; Sugiyama, S.; Munakata, M.; Ito, H.; et al. Physiological Diagnostic Criteria for Vascular Failure. Hypertension 2018, 72, 1060–1071. [Google Scholar] [CrossRef]
- Tanaka, A.; Tomiyama, H.; Maruhashi, T.; Matsuzawa, Y.; Miyoshi, T.; Kabutoya, T.; Kario, K.; Sugiyama, S.; Munakata, M.; Ito, H.; et al. Official Announcement of Physiological Diagnostic Criteria for Vascular Failure from the Japanese Society for Vascular Failure. Vasc. Fail. 2018, 2, 59–60. [Google Scholar] [CrossRef]
- Ichihara, A.; Yamashita, N.; Takemitsu, T.; Kaneshiro, Y.; Sakoda, M.; Kurauchi-Mito, A.; Itoh, H. Cardio-Ankle Vascular Index and Ankle Pulse Wave Velocity as a Marker of Arterial Fibrosis in Kidney Failure Treated by Hemodialysis. Am. J. Kidney Dis. 2008, 52, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Kato, A. Arterial Stiffening and Clinical Outcomes in Dialysis Patients. Pulse 2015, 3, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Cong, T.; Jiang, S.; Wang, K.; Zhong, L.; Wu, J.; Su, D. Predictive value of brachial-ankle artery pulse wave velocity to heart failure with preserved ejection fraction in hospitalised patients with acute dyspnoea. Pak. J. Med. Sci. 2015, 31, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Khan, H.; Newman, A.B.; Lakatta, E.G.; Forman, D.E.; Butler, J.; Berry, J.D. Arterial Stiffness and Risk of Overall Heart Failure, Heart Failure With Preserved Ejection Fraction, and Heart Failure With Reduced Ejection Fraction: The Health ABC Study (Health, Aging, and Body Composition). Hypertension 2017, 69, 267–274. [Google Scholar] [CrossRef]
- Tsao, C.W.; Lyass, A.; Larson, M.G.; Levy, D.; Hamburg, N.M.; Vita, J.A.; Benjamin, E.J.; Mitchell, G.F.; Vasan, R.S. Relation of Central Arterial Stiffness to Incident Heart Failure in the Community. J. Am. Hear. Assoc. 2015, 4, e002189. [Google Scholar] [CrossRef] [PubMed]
- Chirinos, J.A.; Khan, A.; Bansal, N.; Dries, D.L.; Feldman, H.I.; Ford, V.; Anderson, A.H.; Kallem, R.; Lash, J.P.; Ojo, A.; et al. Arterial stiffness, central pressures, and incident hospitalized heart failure in the chronic renal insufficiency cohort study. Circ. Heart Fail. 2014, 7, 709–716. [Google Scholar] [CrossRef]
- Kang, S.; Fan, H.-M.; Li, J.; Fan, L.-Y.; Miao, A.-Y.; Bao, Y.; Wu, L.-Z.; Zhu, Y.; Zhang, D.-F.; Liu, Z.-M. Relationship of arterial stiffness and early mild diastolic heart failure in general middle and aged population. Eur. Hear. J. 2010, 31, 2799–2807. [Google Scholar] [CrossRef]
- Nakamura, T.; Uematsu, M.; Deyama, J.; Watanabe, Y.; Nakamura, K.; Kobayashi, T.; Saito, Y.; Fujioka, D.; Kawabata, K.-I.; Obata, J.-E.; et al. Pulmonary vascular resistance is associated with brachial-ankle pulse wave velocity and adverse clinical outcomes in patients with heart failure with preserved ejection fraction. J. Card. Fail. 2019. [Google Scholar] [CrossRef]
- Tokitsu, T.; Yamamoto, E.; Oike, F.; Hirata, Y.; Tsujita, K.; Yamamuro, M.; Kaikita, K.; Hokimoto, S. Clinical significance of brachial-ankle pulse-wave velocity in patients with heart failure with preserved left ventricular ejection fraction. J. Hypertens. 2018, 36, 560–568. [Google Scholar] [CrossRef]
- Takae, M.; Yamamoto, E.; Tokitsu, T.; Oike, F.; Nishihara, T.; Fujisue, K.; Sueta, D.; Usuku, H.; Motozato, K.; Ito, M.; et al. Clinical Significance of Brachial-Ankle Pulse Wave Velocity in Patients With Heart Failure With Reduced Left Ventricular Ejection Fraction. Am. J. Hypertens. 2019, 32, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Masugata, H.; Senda, S.; Inukai, M.; Murao, K.; Himoto, T.; Hosomi, N.; Murakami, K.; Noma, T.; Kohno, M.; Okada, H.; et al. Association of cardio-ankle vascular index with brain natriuretic peptide levels in hypertension. J Atheroscler Thromb. 2012, 19, 255–262. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Li, L.; Hu, B.; Gong, S.; Yu, Y.; Dai, H.; Yan, J. Pulmonary Function and Arterial Stiffness in Chronic Heart Failure. BioMed Res. Int. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Hu, B.; Gong, S.; Yu, Y.; Yan, J. Age and cigarette smoking modulate the relationship between pulmonary function and arterial stiffness in heart failure patients. Medicine 2017, 96, e6262. [Google Scholar] [CrossRef] [PubMed]
- Yoshihisa, A.; Takiguchi, M.; Shimizu, T.; Nakamura, Y.; Yamauchi, H.; Iwaya, S.; Owada, T.; Miyata, M.; Abe, S.; Sato, T.; et al. Cardiovascular function and prognosis of patients with heart failure coexistent with chronic obstructive pulmonary disease. J. Cardiol. 2014, 64, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Hitsumoto, T. Efficacy of the Reactive Oxygen Metabolite Test as a Predictor of Initial Heart Failure Hospitalization in Elderly Patients With Chronic Heart Failure. Cardiol. Res. 2018, 9, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Masaki, N.; Sato, A.; Horii, S.; Kimura, T.; Toya, T.; Yasuda, R.; Namba, T.; Yada, H.; Kawamura, A.; Adachi, T. Usefulness of the d-ROMs test for prediction of cardiovascular events. Int. J. Cardiol. 2016, 222, 226–232. [Google Scholar] [CrossRef]
- Miyoshi, T.; Ito, H.; Horinaka, S.; Shirai, K.; Higaki, J.; Orimio, H. Protocol for Evaluating the Cardio-Ankle Vascular Index to Predict Cardiovascular Events in Japan: A Prospective Multicenter Cohort Study. Pulse 2017, 4, 11–16. [Google Scholar] [CrossRef]
- Masaki, N.; Ido, Y.; Yamada, T.; Yamashita, Y.; Toya, T.; Takase, B.; Hamburg, N.M.; Adachi, T. Endothelial Insulin Resistance of Freshly Isolated Arterial Endothelial Cells From Radial Sheaths in Patients With Suspected Coronary Artery Disease. J. Am. Hear. Assoc. 2019, 8, e010816. [Google Scholar] [CrossRef]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Namba, T.; Masaki, N.; Takase, B.; Adachi, T. Arterial Stiffness Assessed by Cardio-Ankle Vascular Index. Int. J. Mol. Sci. 2019, 20, 3664. https://doi.org/10.3390/ijms20153664
Namba T, Masaki N, Takase B, Adachi T. Arterial Stiffness Assessed by Cardio-Ankle Vascular Index. International Journal of Molecular Sciences. 2019; 20(15):3664. https://doi.org/10.3390/ijms20153664
Chicago/Turabian StyleNamba, Takayuki, Nobuyuki Masaki, Bonpei Takase, and Takeshi Adachi. 2019. "Arterial Stiffness Assessed by Cardio-Ankle Vascular Index" International Journal of Molecular Sciences 20, no. 15: 3664. https://doi.org/10.3390/ijms20153664
APA StyleNamba, T., Masaki, N., Takase, B., & Adachi, T. (2019). Arterial Stiffness Assessed by Cardio-Ankle Vascular Index. International Journal of Molecular Sciences, 20(15), 3664. https://doi.org/10.3390/ijms20153664