Clinical Therapeutic Strategy and Neuronal Mechanism Underlying Post-Traumatic Stress Disorder (PTSD)



Abstract
1. Introduction
2. Neuronal Circuits in PTSD Symptoms
3. Clinical Therapeutics for Patients with PTSD
3.1. Psychological Therapy for PTSD Symptoms
3.2. Pharmacological Therapy for PTSD Symptoms
4. Animal Models of PTSD
5. Role of Long-Chain Polyunsaturated Fatty Acids (LCPUFAs) and Fatty Acid Binding Proteins (FABPs) in the Brain
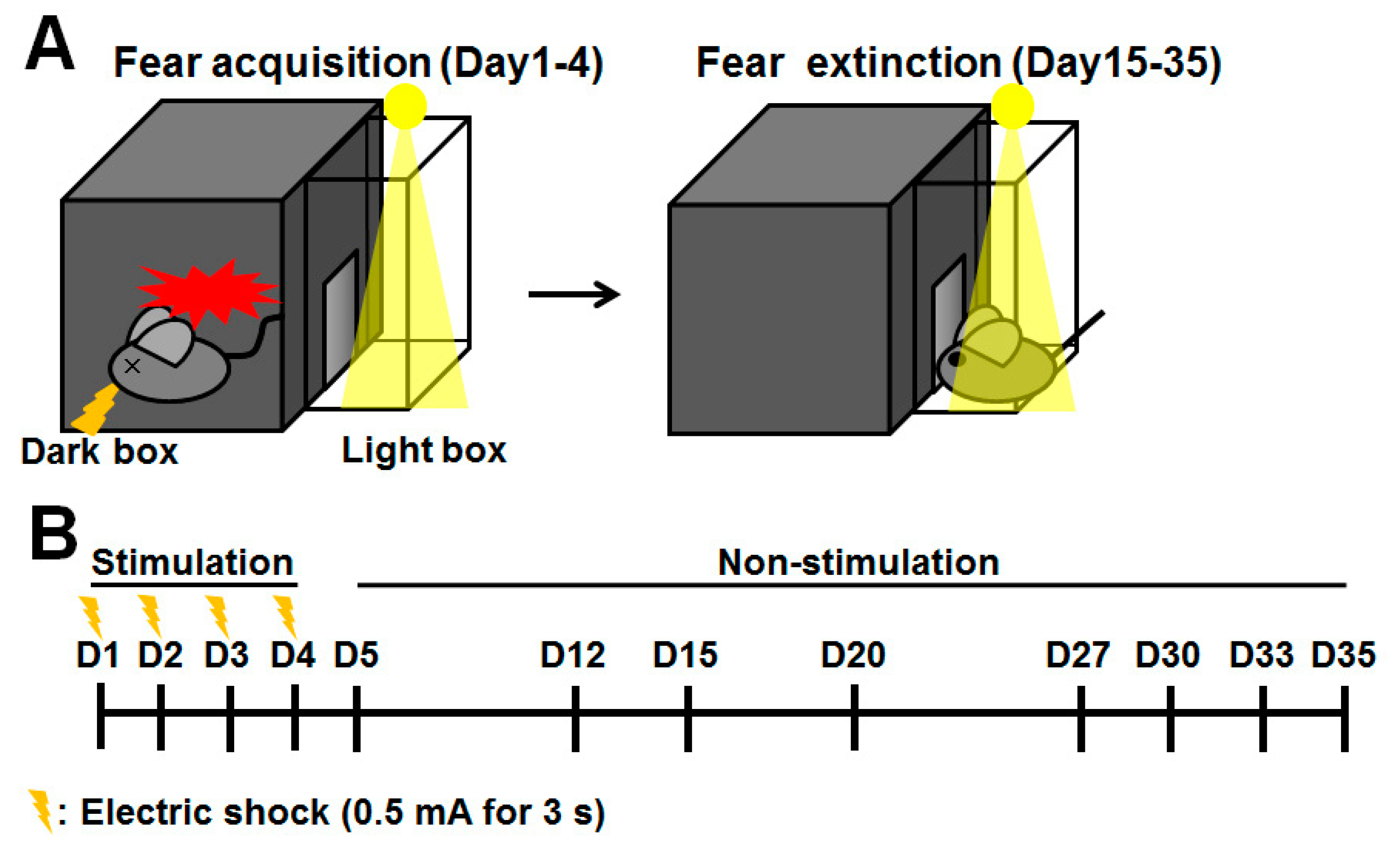
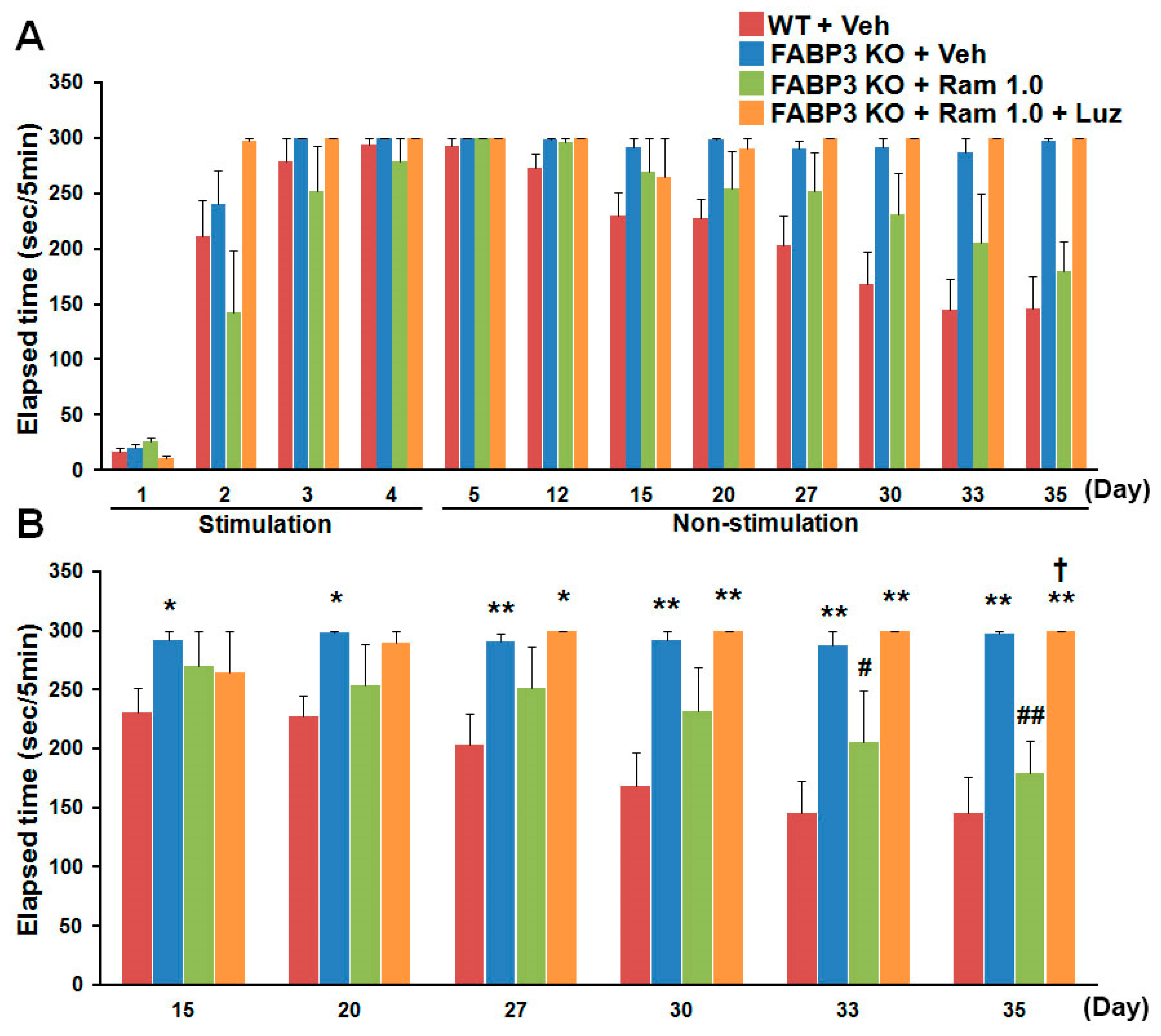
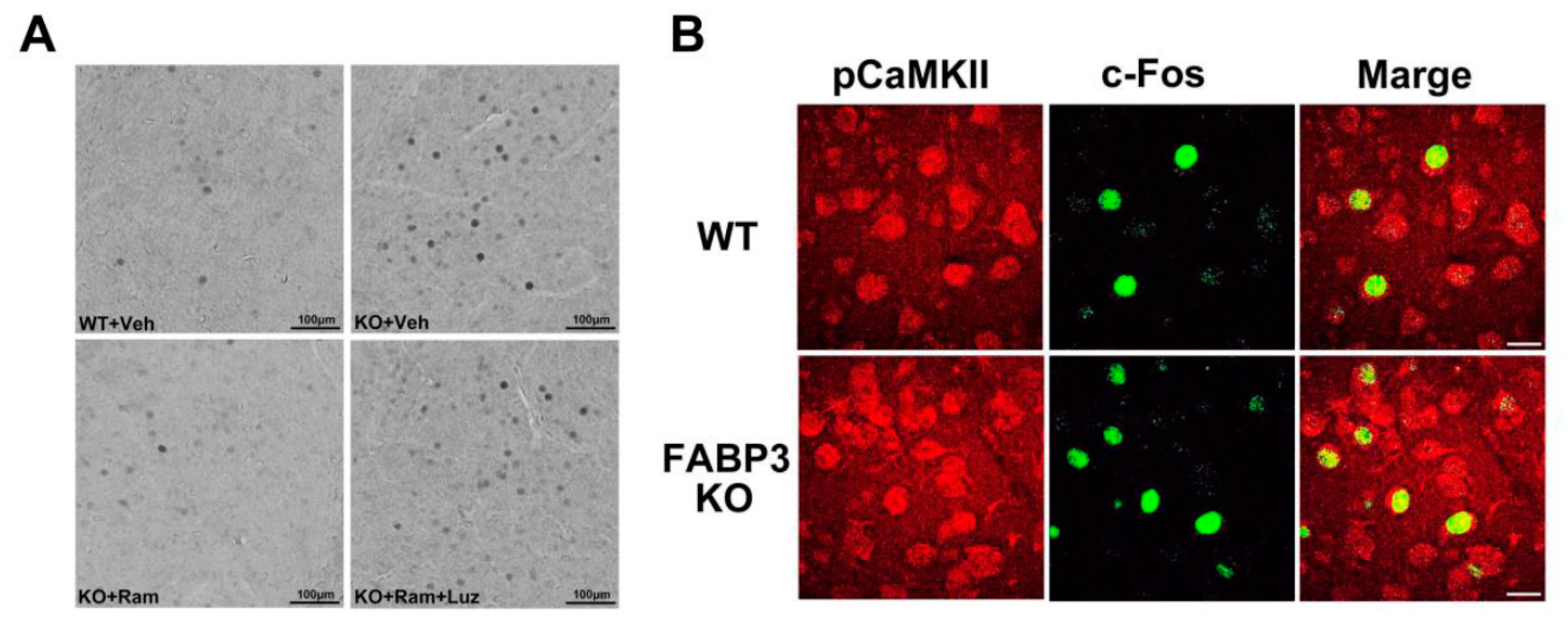
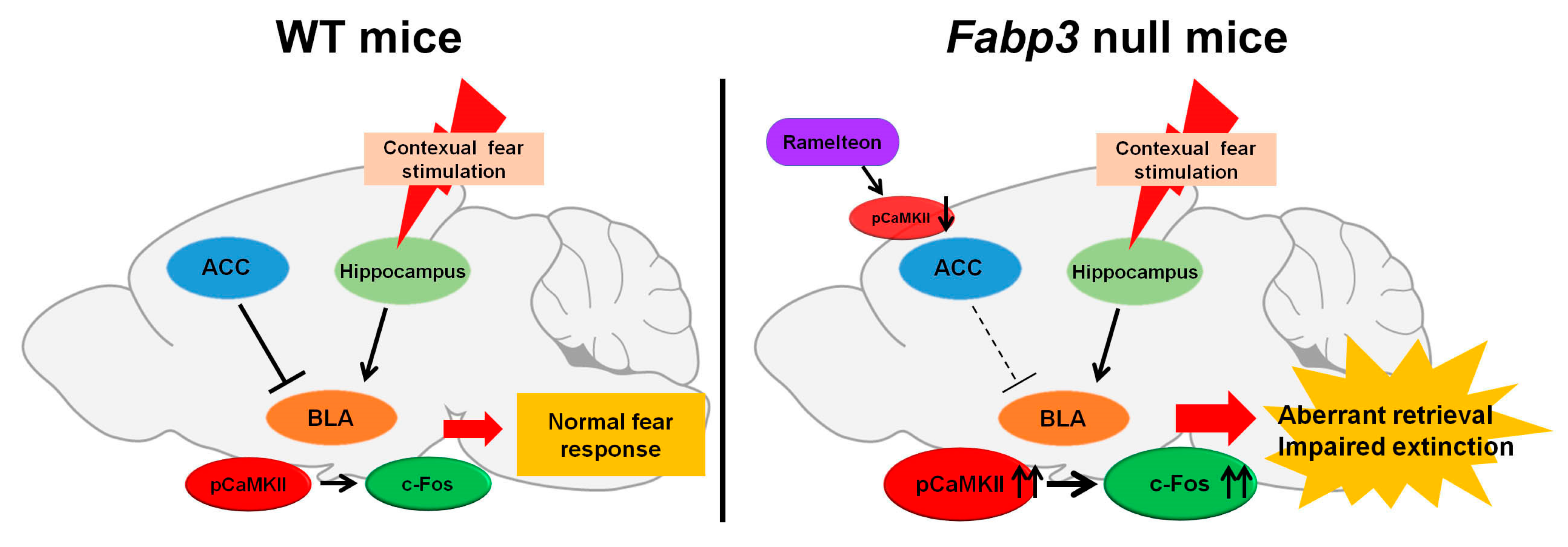
6. Impaired Fear Extinction Process in Fabp3 Null Mice
7. Potential Efficacy of Melatonin Receptor Agonist for PTSD Symptom
8. Conclusions
Funding
Conflicts of Interest
Abbreviations
| ACC | anterior cingulated cortex |
| BLA | basolateral amygdala |
| CaMKII | calcium/calmodulin-dependent protein kinase II |
| CBT | cognitive behavioral therapy |
| Cdk5 | cyclin-dependent kinase 5 |
| DG | dentate gyrus |
| EMDR | eye movement desensitization and reprocessing |
| FABP | fatty acid binding protein |
| fMRI | functional magnetic resonance imaging |
| GABA | γ-aminobutyric acid |
| HPA | hypothalamo-pituitary-adrenal |
| 5-HT | serotonin |
| IRT | imagery rehearsal therapy |
| LCPUFA | long-chain polyunsaturated fatty acid |
| MRI | magnetic resonance imaging |
| NMDA | N-methyl-d-aspartate |
| PFC | prefrontal cortex |
| PTSD | Post-traumatic stress disorder |
| QOL | quality of life |
| SNRI | serotonin and noradrenaline reuptake inhibitor |
| SPS | Single prolonged stress |
| SSRI | selective serotonin reuptake inhibitor |
| WT | wild-type |
References
- Foa, E.B.; Gillihan, S.J.; Bryant, R.A. Challenges and Successes in Dissemination of Evidence-Based Treatments for Posttraumatic Stress: Lessons Learned From Prolonged Exposure Therapy for PTSD. Psychol. Sci. Public Interest 2013, 14, 65–111. [Google Scholar] [CrossRef] [PubMed]
- Javidi, H.; Yadollahie, M. Post-traumatic Stress Disorder. Int. J. Occup. Environ Med. 2012, 3, 2–9. [Google Scholar] [PubMed]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.B.; Smith, S.M.; Chou, S.P.; Saha, T.D.; Jung, J.; Zhang, H.; Pickering, R.P.; Ruan, W.J.; Huang, B.; Grant, B.F. The epidemiology of DSM-5 posttraumatic stress disorder in the United States: Results from the National Epidemiologic Survey on Alcohol and Related Conditions-III. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1137–1148. [Google Scholar] [CrossRef]
- Kawakami, N.; Tsuchiya, M.; Umeda, M.; Koenen, K.C.; Kessler, R.C. World Mental Health Survey Japan. Trauma and posttraumatic stress disorder in Japan: Results from the World Mental Health Japan Survey. J. Psychiatr. Res. 2014, 53, 157–165. [Google Scholar] [CrossRef]
- Fullerton, C.S.; Ursano, R.J.; Wang, L. Acute stress disorder, posttraumatic stress disorder, and depression in disaster or rescue workers. Am. J. Psychiatry 2004, 161, 1370–1376. [Google Scholar] [CrossRef]
- Matsubara, C.; Murakami, H.; Imai, K.; Mizoue, T.; Akashi, H.; Miyoshi, C.; Nakasa, T. Prevalence and Risk Factors for Post-Traumatic Stress Reaction Among Resident Survivors of the Tsunami That Followed the Great East Japan Earthquake, March 11, 2011. Disaster Med. Public Health Prep. 2016, 10, 746–753. [Google Scholar] [CrossRef]
- Schlenger, W.E.; Caddell, J.M.; Ebert, L.; Jordan, B.K.; Rourke, K.M.; Wilson, D.; Thalji, L.; Dennis, J.M.; Fairbank, J.A.; Kulka, R.A. Psychological reactions to terrorist attacks: Findings from the National Study of Americans’ Reactions to September 11. JAMA 2002, 288, 581–588. [Google Scholar] [CrossRef]
- Turner, S.W.; Thompson, J.; Rosser, R.M. The Kings Cross fire: Psychological reactions. J. Trauma Stress 1995, 8, 419–427. [Google Scholar] [CrossRef]
- Havenaar, J.M.; Rumyantzeva, G.M.; van den Brink, W.; Poelijoe, N.W.; van den Bout, J.; van Engeland, H.; Koeter, M.W. Long-term mental health effects of the Chernobyl disaster: An epidemiologic survey in two former Soviet regions. Am. J. Psychiatry 1997, 154, 1605–1607. [Google Scholar] [CrossRef]
- Ressler, K.J.; Mayberg, H.S. Targeting abnormal neural circuits in mood and anxiety disorders: From the laboratory to the clinic. Nat. Neurosci. 2007, 10, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Waltman, S.H.; Shearer, D.; Moore, B.A. Management of Post-Traumatic Nightmares: A Review of Pharmacologic and Nonpharmacologic Treatments Since 2013. Curr. Psychiatry Rep. 2018, 20, 108. [Google Scholar] [CrossRef] [PubMed]
- Bremner, J.D.; Scott, T.M.; Delaney, R.C.; Southwick, S.M.; Mason, J.W.; Johnson, D.R.; Innis, R.B.; McCarthy, G.; Charney, D.S. Deficits in short-term memory in posttraumatic stress disorder. Am. J. Psychiatry 1993, 150, 1015–1019. [Google Scholar] [CrossRef] [PubMed]
- Vasterling, J.J.; Duke, L.M.; Brailey, K.; Constans, J.I.; Allain, A.N., Jr.; Sutker, P.B. Attention, learning, and memory performances and intellectual resources in Vietnam veterans: PTSD and no disorder comparisons. Neuropsychology 2002, 16, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Moser, D.A.; Aue, T.; Suardi, F.; Kutlikova, H.; Cordero, M.I.; Rossignol, A.S.; Favez, N.; Rusconi Serpa, S.; Schechter, D.S. Violence-related PTSD and neural activation when seeing emotionally charged male-female interactions. Soc. Cogn. Affect. Neurosci. 2015, 10, 645–653. [Google Scholar] [CrossRef]
- Yu, B.; Cui, S.Y.; Zhang, X.Q.; Cui, X.Y.; Li, S.J.; Sheng, Z.F.; Cao, Q.; Huang, Y.L.; Xu, Y.P.; Lin, Z.G.; et al. Different neural circuitry is involved in physiological and psychological stress-induced PTSD-like “nightmares” in rats. Sci. Rep. 2015, 5, 15976. [Google Scholar] [CrossRef]
- Paintain, E.; Cassidy, S. First-line therapy for post-traumatic stress disorder: A systematic review of cognitive behavioural therapy and psychodynamic approaches. Couns. Psychother. Res. 2018, 18, 237–250. [Google Scholar] [CrossRef]
- Forman-Hoffman, V.; Middleton, J.C.; Feltner, C.; Gaynes, B.N.; Weber, R.P.; Bann, C.; Viswanathan, M.; Lohr, K.N.; Baker, C.; Green, J. Psychological and Pharmacological Treatments for Adults With Posttraumatic Stress Disorder: A Systematic Review Update; Report No.: 18-EHC011-EF; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2018.
- Milad, M.R.; Quirk, G.J. Neurons in medial prefrontal cortex signal memory for fear extinction. Nature 2002, 420, 70–74. [Google Scholar] [CrossRef]
- Parsons, R.G.; Ressler, K.J. Implications of memory modulation for post-traumatic stress and fear disorders. Nat. Neurosci. 2013, 16, 146–153. [Google Scholar] [CrossRef]
- Wilensky, A.E.; Schafe, G.E.; Kristensen, M.P.; LeDoux, J.E. Rethinking the fear circuit: The central nucleus of the amygdala is required for the acquisition, consolidation, and expression of Pavlovian fear conditioning. J. Neurosci. 2006, 26, 12387–12396. [Google Scholar] [CrossRef]
- Quirk, G.J.; Russo, G.K.; Barron, J.L.; Lebron, K. The role of ventromedial prefrontal cortex in the recovery of extinguished fear. J. Neurosci. 2000, 20, 6225–6231. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Fanselow, M.S. Modality-specific retrograde amnesia of fear. Science 1992, 256, 675–677. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.J.; Fanselow, M.S. Pre-training prevents context fear conditioning deficits produced by hippocampal NMDA receptor blockade. Neurobiol. Learn Mem. 2003, 80, 123–129. [Google Scholar] [CrossRef]
- Sotres-Bayon, F.; Sierra-Mercado, D.; Pardilla-Delgado, E.; Quirk, G.J. Gating of Fear in Prelimbic Cortex by Hippocampal and Amygdala Inputs. Neuron 2012, 76, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Tovote, P.; Fadok, J.P.; Lüthi, A. Neuronal circuits for fear and anxiety. Nat. Rev. Neurosci. 2015, 16, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Klavir, O.; Prigge, M.; Sarel, A.; Paz, R.; Yizhar, O. Manipulating fear associations via optogenetic modulation of amygdala inputs to prefrontal cortex. Nat. Neurosci. 2017, 20, 836–844. [Google Scholar] [CrossRef]
- Kitayama, N.; Vaccarino, V.; Kutner, M.; Weiss, P.; Bremner, J.D. Magnetic resonance imaging (MRI) measurement of hippocampal volume in posttraumatic stress disorder: A meta-analysis. J. Affect. Disord. 2005, 88, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Yamasue, H.; Kasai, K.; Iwanami, A.; Ohtani, T.; Yamada, H.; Abe, O.; Kuroki, N.; Fukuda, R.; Sadamatsu, M.; Sasaki, T.; et al. Voxel-based analysis of MRI reveals anterior cingulate gray-matter volume reduction in posttraumatic stress disorder due to terrorism. Proc. Natl. Acad. Sci. USA 2003, 100, 9039–9043. [Google Scholar] [CrossRef]
- O’Doherty, D.C.; Chitty, K.M.; Saddiqui, S.; Bennett, M.R.; Lagopoulos, J. A systematic review and meta-analysis of magnetic resonance imaging measurement of structural volumes in posttraumatic stress disorder. Psychiatry Res. 2015, 232, 1–33. [Google Scholar] [CrossRef]
- Rauch, S.L.; Shin, L.M.; Phelps, E.A. Neurocircuitry models of posttraumatic stress disorder and extinction: Human neuroimaging research-past, present, and future. Biol. Psychiatry 2006, 60, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Logue, M.W.; van Rooij, S.J.H.; Dennis, E.L.; Davis, S.L.; Hayes, J.P.; Stevens, J.S.; Densmore, M.; Haswell, C.C.; Ipser, J.; Koch, S.B.J.; et al. Smaller Hippocampal Volume in Posttraumatic Stress Disorder: A Multisite ENIGMA-PGC Study: Subcortical Volumetry Results From Posttraumatic Stress Disorder Consortia. Biol. Psychiatry 2018, 83, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Shin, L.M.; Wright, C.I.; Cannistraro, P.A.; Wedig, M.M.; McMullin, K.; Martis, B.; Macklin, M.L.; Lasko, N.B.; Cavanagh, S.R.; Krangel, T.S.; et al. A functional magnetic resonance imaging study of amygdala and medial prefrontal cortex responses to overtly presented fearful faces in posttraumatic stress disorder. Arch Gen. Psychiatry 2005, 62, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Rauch, S.L.; Whalen, P.J.; Shin, L.M.; McInerney, S.C.; Macklin, M.L.; Lasko, N.B.; Orr, S.P.; Pitman, R.K. Exaggerated amygdala response to masked facial stimuli in posttraumatic stress disorder: A functional MRI study. Biol. Psychiatry 2000, 47, 769–776. [Google Scholar] [CrossRef]
- Shin, L.M.; Whalen, P.J.; Pitman, R.K.; Bush, G.; Macklin, M.L.; Lasko, N.B.; Orr, S.P.; McInerney, S.C.; Rauch, S.L. An fMRI study of anterior cingulate function in posttraumatic stress disorder. Biol. Psychiatry 2001, 50, 932–942. [Google Scholar] [CrossRef]
- Patel, R.; Spreng, R.N.; Shin, L.M.; Girard, T.A. Neurocircuitry models of posttraumatic stress disorder and beyond: A meta-analysis of functional neuroimaging studies. Neurosci. Biobehav. Rev. 2012, 36, 2130–2142. [Google Scholar] [CrossRef] [PubMed]
- Lanius, R.A.; Frewen, P.A.; Tursich, M.; Jetly, R.; McKinnon, M.C. Restoring large-scale brain networks in PTSD and related disorders: A proposal for neuroscientifically-informed treatment interventions. Eur. J. Psychotraumatol. 2015, 6, 27313. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.P.; Hayes, S.M.; Mikedis, A.M. Quantitative meta-analysis of neural activity in posttraumatic stress disorder. Biol. Mood Anxiety Disord. 2012, 2, 9. [Google Scholar] [CrossRef] [PubMed]
- Koch, S.B.; van Zuiden, M.; Nawijn, L.; Frijling, J.L.; Veltman, D.J.; Olff, M. Aberrant resting-state brain activity in posttraumatic stress disorder: A meta-analysis and systematic review. Depress. Anxiety 2016, 33, 592–605. [Google Scholar] [CrossRef]
- Bremner, J.D.; Staib, L.H.; Kaloupek, D.; Southwick, S.M.; Soufer, R.; Charney, D.S. Neural correlates of exposure to traumatic pictures and sound in Vietnam combat veterans with and without posttraumatic stress disorder: A positron emission tomography study. Biol. Psychiatry 1999, 45, 806–816. [Google Scholar] [CrossRef]
- Feng, P.; Feng, T.; Chen, Z.; Lei, X. Memory consolidation of fear conditioning: Bi-stable amygdala connectivity with dorsal anterior cingulate and medial prefrontal cortex. Soc. Cogn. Affect. Neurosci. 2014, 9, 1730–1737. [Google Scholar] [CrossRef]
- Jeon, D.; Kim, S.; Chetana, M.; Jo, D.; Ruley, H.E.; Lin, S.Y.; Rabah, D.; Kinet, J.P.; Shin, H.S. Observational fear learning involves affective pain system and Cav1.2 Ca2+ channels in ACC. Nat. Neurosci. 2010, 13, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Mátyás, F.; Lee, J.; Shin, H.S.; Acsády, L. The fear circuit of the mouse forebrain: Connections between the mediodorsal thalamus, frontal cortices and basolateral amygdala. Eur. J. Neurosci. 2014, 39, 1810–1823. [Google Scholar] [CrossRef] [PubMed]
- Duman, R.S.; Girgenti, M.J. Molecular and cellular studies of PTSD: Postmortem transcriptome analysis and novel therapeutic targets. J. Neurosci. Res. 2019, 97, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Myers, K.M.; Davis, M. Mechanisms of fear extinction. Mol. Psychiatry 2007, 12, 120–150. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.J.; Francis, J.; Friedlander, J.; Banks-Williams, L.; Lande, R.G.; Taylor, P.; Blair, J.; McLellan, J.; Law, W.; Tarpley, V.; et al. Improvement in cerebral function with treatment of posttraumatic stress disorder. Ann. N. Y. Acad. Sci. 2010, 1208, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Szeszko, P.R.; Yehuda, R. Magnetic resonance imaging predictors of psychotherapy treatment response in post-traumatic stress disorder: A role for the salience network. Psychiatry Res. 2019, 277, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, J.C.; Hand, A.; Jarnecke, A.M.; Moran-Santa Maria, M.M.; Brady, K.T.; Joseph, J.E. Effects of oxytocin on working memory and executive control system connectivity in posttraumatic stress disorder. Exp. Clin. Psychopharmacol. 2018, 26, 391–402. [Google Scholar] [CrossRef]
- Bossini, L.; Tavanti, M.; Lombardelli, A.; Calossi, S.; Polizzotto, N.R.; Galli, R.; Vatti, G.; Pieraccini, F.; Castrogiovanni, P. Changes in hippocampal volume in patients with post-traumatic stress disorder after sertraline treatment. J. Clin. Psychopharmacol. 2007, 27, 233–235. [Google Scholar] [CrossRef]
- Vermetten, E.; Vythilingam, M.; Southwick, S.M.; Charney, D.S.; Bremner, J.D. Long-term treatment with paroxetine increases verbal declarative memory and hippocampal volume in posttraumatic stress disorder. Biol. Psychiatry 2003, 54, 693–702. [Google Scholar] [CrossRef]
- Letizia, B.; Andrea, F.; Paolo, C. Neuroanatomical changes after eye movement desensitization and reprocessing (EMDR) treatment in posttraumatic stress disorder. J. Neuropsychiatry Clin. Neurosci. 2007, 19, 475–476. [Google Scholar] [CrossRef]
- Nardo, D.; Högberg, G.; Looi, J.C.; Larsson, S.; Hällström, T.; Pagani, M. Gray matter density in limbic and paralimbic cortices is associated with trauma load and EMDR outcome in PTSD patients. J. Psychiatry Res. 2010, 44, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Felmingham, K.; Whitford, T.J.; Kemp, A.; Hughes, G.; Peduto, A.; Williams, L.M. Rostral anterior cingulate volume predicts treatment response to cognitive-behavioural therapy for posttraumatic stress disorder. J. Psychiatry Neurosci. 2008, 33, 142–146. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Clinical Excellence (NICE). Post-Traumatic Stress Disorder: Management (CG26); National Institute for Health and Clinical Excellence: Manchester, UK, 2005. [Google Scholar]
- Kar, N. Cognitive behavioral therapy for the treatment of post-traumatic stress disorder: A review. Neuropsychiatry Dis. Treat. 2011, 7, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Schnitzlein, C.W.; Wolf, J.P.; Vythilingam, M.; Rasmusson, A.M.; Hoge, C.W. Psychotherapy versus pharmacotherapy for posttraumatic stress disorder: Systemic review and meta-analyses to determine first-line treatments. Depress. Anxiety 2016, 33, 792–806. [Google Scholar] [CrossRef] [PubMed]
- Resick, P.A.; Nishith, P.; Weaver, T.L.; Astin, M.C.; Feuer, C.A. A comparison of cognitive-processing therapy with prolonged exposure and a waiting condition for the treatment of chronic posttraumatic stress disorder in female rape victims. J. Consult. Clin. Psychol. 2002, 70, 867–879. [Google Scholar] [CrossRef] [PubMed]
- Asukai, N.; Saito, A.; Tsuruta, N.; Kishimoto, J.; Nishikawa, T. Efficacy of exposure therapy for Japanese patients with posttraumatic stress disorder due to mixed traumatic events: A randomized controlled study. J. Trauma Stress 2010, 23, 744–750. [Google Scholar] [CrossRef]
- Monson, C.M.; Fredman, S.J.; Macdonald, A.; Pukay-Martin, N.D.; Resick, P.A.; Schnurr, P.P. Effect of cognitive-behavioral couple therapy for PTSD: A randomized controlled trial. JAMA 2012, 308, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Hollifield, M.; Sinclair-Lian, N.; Warner, T.D.; Hammerschlag, R. Acupuncture for posttraumatic stress disorder: A randomized controlled pilot trial. J. Nerv. Ment. Dis. 2007, 195, 504–513. [Google Scholar] [CrossRef]
- Ehlers, A.; Hackmann, A.; Grey, N.; Wild, J.; Liness, S.; Albert, I.; Deale, A.; Stott, R.; Clark, D.M. A randomized controlled trial of 7-day intensive and standard weekly cognitive therapy for PTSD and emotion-focused supportive therapy. Am. J. Psychiatry 2014, 171, 294–304. [Google Scholar] [CrossRef]
- Ter Heide, F.J.; Mooren, T.M.; van de Schoot, R.; de Jongh, A.; Kleber, R.J. Eye movement desensitisation and reprocessing therapy v. stabilisation as usual for refugees: Randomised controlled trial. Br. J. Psychiatry 2016, 209, 311–318. [Google Scholar] [CrossRef]
- Carlson, J.G.; Chemtob, C.M.; Rusnak, K.; Hedlund, N.L.; Muraoka, M.Y. Eye movement desensitization and reprocessing (EDMR) treatment for combat-related posttraumatic stress disorder. J. Trauma Stress 1998, 11, 3–24. [Google Scholar] [CrossRef] [PubMed]
- van der Kolk, B.A.; Spinazzola, J.; Blaustein, M.E.; Hopper, J.W.; Hopper, E.K.; Korn, D.L.; Simpson, W.B. A randomized clinical trial of eye movement desensitization and reprocessing (EMDR), fluoxetine, and pill placebo in the treatment of posttraumatic stress disorder: Treatment effects and long-term maintenance. J. Clin. Psychiatry 2007, 68, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Krakow, B.; Hollifield, M.; Johnston, L.; Koss, M.; Schrader, R.; Warner, T.D.; Tandberg, D.; Lauriello, J.; McBride, L.; Cutchen, L.; et al. Imagery rehearsal therapy for chronic nightmares in sexual assault survivors with posttraumatic stress disorder: A randomized controlled trial. JAMA 2001, 286, 537–545. [Google Scholar] [CrossRef]
- Boden, M.T.; Kimerling, R.; Jacobs-Lentz, J.; Bowman, D.; Weaver, C.; Carney, D.; Walser, R.; Trafton, J.A. Seeking Safety treatment for male veterans with a substance use disorder and post-traumatic stress disorder symptomatology. Addiction 2012, 107, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Galovski, T.E.; Blain, L.M.; Mott, J.M.; Elwood, L.; Houle, T. Manualized therapy for PTSD: Flexing the structure of cognitive processing therapy. J. Consult. Clin. Psychol. 2012, 80, 968–981. [Google Scholar] [CrossRef] [PubMed]
- Martenyi, F.; Brown, E.B.; Zhang, H.; Prakash, A.; Koke, S.C. Fluoxetine versus placebo in posttraumatic stress disorder. J. Clin. Psychiatry 2002, 63, 199–206. [Google Scholar] [CrossRef]
- van der Kolk, B.A.; Dreyfuss, D.; Michaels, M.; Shera, D.; Berkowitz, R.; Fisler, R.; Saxe, G. Fluoxetine in posttraumatic stress disorder. J. Clin. Psychiatry 1994, 55, 517–522. [Google Scholar] [PubMed]
- Martenyi, F.; Brown, E.B.; Caldwell, C.D. Failed efficacy of fluoxetine in the treatment of posttraumatic stress disorder: Results of a fixed-dose, placebo-controlled study. J. Clin. Psychopharmacol. 2007, 27, 166–170. [Google Scholar] [CrossRef]
- Marshall, R.D.; Beebe, K.L.; Oldham, M.; Zaninelli, R. Efficacy and safety of paroxetine treatment for chronic PTSD: A fixed-dose, placebo-controlled study. Am. J. Psychiatry 2001, 158, 1982–1988. [Google Scholar] [CrossRef]
- Tucker, P.; Zaninelli, R.; Yehuda, R.; Ruggiero, L.; Dillingham, K.; Pitts, C.D. Paroxetine in the treatment of chronic posttraumatic stress disorder: Results of a placebo-controlled, flexible-dosage trial. J. Clin. Psychiatry 2001, 62, 860–868. [Google Scholar] [CrossRef]
- Brady, K.; Pearlstein, T.; Asnis, G.M.; Baker, D.; Rothbaum, B.; Sikes, C.R.; Farfel, G.M. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: A randomized controlled trial. JAMA 2000, 283, 1837–1844. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.R.; Rothbaum, B.O.; van der Kolk, B.A.; Sikes, C.R.; Farfel, G.M. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch. Gen. Psychiatry 2001, 58, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Zohar, J.; Amital, D.; Miodownik, C.; Kotler, M.; Bleich, A.; Lane, R.M.; Austin, C. Double-blind placebo-controlled pilot study of sertraline in military veterans with posttraumatic stress disorder. J. Clin. Psychopharmacol. 2002, 22, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.; Rothbaum, B.O.; Tucker, P.; Asnis, G.; Benattia, I.; Musgnung, J.J. Venlafaxine extended release in posttraumatic stress disorder: A sertraline- and placebo-controlled study. J. Clin. Psychopharmacol. 2006, 26, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.; Baldwin, D.; Stein, D.J.; Kuper, E.; Benattia, I.; Ahmed, S.; Pedersen, R.; Musgnung, J. Treatment of posttraumatic stress disorder with venlafaxine extended release: A 6-month randomized controlled trial. Arch. Gen. Psychiatry 2006, 63, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Kosten, T.R.; Frank, J.B.; Dan, E.; McDougle, C.J.; Giller, E.L., Jr. Pharmacotherapy for posttraumatic stress disorder using phenelzine or imipramine. J. Nerv. Ment. Dis. 1991, 179, 366–370. [Google Scholar] [CrossRef]
- Davidson, J.; Kudler, H.; Smith, R.; Mahorney, S.L.; Lipper, S.; Hammett, E.; Saunders, W.B.; Cavenar, J.O., Jr. Treatment of posttraumatic stress disorder with amitriptyline and placebo. Arch. Gen. Psychiatry 1990, 47, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.R.; Weisler, R.H.; Butterfield, M.I.; Casat, C.D.; Connor, K.M.; Barnett, S.; van Meter, S. Mirtazapine vs. placebo in posttraumatic stress disorder: A pilot trial. Biol. Psychiatry 2003, 53, 188–191. [Google Scholar] [CrossRef]
- Becker, M.E.; Hertzberg, M.A.; Moore, S.D.; Dennis, M.F.; Bukenya, D.S.; Beckham, J.C. A placebo-controlled trial of bupropion SR in the treatment of chronic posttraumatic stress disorder. J. Clin. Psychopharmacol. 2007, 27, 193–197. [Google Scholar] [CrossRef]
- Hamner, M.B.; Faldowski, R.A.; Ulmer, H.G.; Frueh, B.C.; Huber, M.G.; Arana, G.W. Adjunctive risperidone treatment in post-traumatic stress disorder: A preliminary controlled trial of effects on comorbid psychotic symptoms. Int. Clin. Psychopharmacol. 2003, 18, 1–8. [Google Scholar] [CrossRef]
- Reich, D.B.; Winternitz, S.; Hennen, J.; Watts, T.; Stanculescu, C. A preliminary study of risperidone in the treatment of posttraumatic stress disorder related to childhood abuse in women. J. Clin. Psychiatry 2004, 65, 1601–1606. [Google Scholar] [CrossRef] [PubMed]
- Krystal, J.H.; Rosenheck, R.A.; Cramer, J.A.; Vessicchio, J.C.; Jones, K.M.; Vertrees, J.E.; Horney, R.A.; Huang, G.D.; Stock, C. Veterans, Affairs, Cooperative, Study, No. 504 Group. Adjunctive risperidone treatment for antidepressant-resistant symptoms of chronic military service-related PTSD: A randomized trial. JAMA 2011, 306, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Kline, N.A.; Matloff, J.L. Adjunctive olanzapine for SSRI-resistant combat-related PTSD: A double-blind, placebo-controlled study. Am. J. Psychiatry 2002, 159, 1777–1779. [Google Scholar] [CrossRef] [PubMed]
- Carey, P.; Suliman, S.; Ganesan, K.; Seedat, S.; Stein, D.J. Olanzapine monotherapy in posttraumatic stress disorder: Efficacy in a randomized, double-blind, placebo-controlled study. Hum. Psychopharmacol. 2012, 27, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Lambert, M.T. Aripiprazole in the management of post-traumatic stress disorder symptoms in returning Global War on Terrorism veterans. Int. Clin. Psychopharmacol. 2006, 21, 185–187. [Google Scholar] [CrossRef]
- Hamner, M.B.; Brodrick, P.S.; Labbate, L.A. Gabapentin in PTSD: A retrospective, clinical series of adjunctive therapy. Ann. Clin. Psychiatry 2001, 13, 141–146. [Google Scholar] [CrossRef]
- Raskind, M.A.; Peskind, E.R.; Kanter, E.D.; Petrie, E.C.; Radant, A.; Thompson, C.E.; Dobie, D.J.; Hoff, D.; Rein, R.J.; Straits-Tröster, K.; et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: A placebo-controlled study. Am. J. Psychiatry 2003, 160, 371–373. [Google Scholar] [CrossRef]
- Raskind, M.A.; Peterson, K.; Williams, T.; Hoff, D.J.; Hart, K.; Holmes, H.; Homas, D.; Hill, J.; Daniels, C.; Calohan, J.; et al. A trial of prazosin for combat trauma PTSD with nightmares in active-duty soldiers returned from Iraq and Afghanistan. Am. J. Psychiatry 2013, 170, 1003–1010. [Google Scholar] [CrossRef]
- Raskind, M.A.; Peskind, E.R.; Chow, B.; Harris, C.; Davis-Karim, A.; Holmes, H.A.; Hart, K.L.; McFall, M.; Mellman, T.A.; Reist, C.; et al. Trial of Prazosin for Post-Traumatic Stress Disorder in Military Veterans. N. Engl. J. Med. 2018, 378, 507–517. [Google Scholar] [CrossRef]
- Tucker, P.; Trautman, R.P.; Wyatt, D.B.; Thompson, J.; Wu, S.C.; Capece, J.A.; Rosenthal, N.R. Efficacy and safety of topiramate monotherapy in civilian posttraumatic stress disorder: A randomized, double-blind, placebo-controlled study. J. Clin. Psychiatry 2007, 68, 201–206. [Google Scholar] [CrossRef]
- Yeh, M.S.; Mari, J.J.; Costa, M.C.; Andreoli, S.B.; Bressan, R.A.; Mello, M.F. A double-blind randomized controlled trial to study the efficacy of topiramate in a civilian sample of PTSD. CNS Neurosci. Ther. 2011, 17, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Jetly, R.; Heber, A.; Fraser, G.; Boisvert, D. The efficacy of nabilone, a synthetic cannabinoid, in the treatment of PTSD-associated nightmares: A preliminary randomized, double-blind, placebo-controlled cross-over design study. Psychoneuroendocrinology 2015, 51, 585–588. [Google Scholar] [CrossRef] [PubMed]
- Gunduz-Cinar, O.; Flynn, S.; Brockway, E.; Kaugars, K.; Baldi, R.; Ramikie, T.S.; Cinar, R.; Kunos, G.; Patel, S.; Holmes, A. Fluoxetine Facilitates Fear Extinction Through Amygdala Endocannabinoids. Neuropsychopharmacology 2016, 41, 1598–1609. [Google Scholar] [CrossRef] [PubMed]
- Deschaux, O.; Spennato, G.; Moreau, J.L.; Garcia, R. Chronic treatment with fluoxetine prevents the return of extinguished auditory-cued conditioned fear. Psychopharmacology 2011, 215, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Bentefour, Y.; Rakibi, Y.; Bennis, M.; Ba-M’hamed, S.; Garcia, R. Paroxetine treatment, following behavioral suppression of PTSD-like symptoms in mice, prevents relapse by activating the infralimbic cortex. Eur. Neuropsychopharmacol. 2016, 26, 195–207. [Google Scholar] [CrossRef]
- Alvarez-Ricartes, N.; Oliveros-Matus, P.; Mendoza, C.; Perez-Urrutia, N.; Echeverria, F.; Iarkov, A.; Barreto, G.E.; Echeverria, V. Intranasal Cotinine Plus Krill Oil Facilitates Fear Extinction, Decreases Depressive-Like Behavior, and Increases Hippocampal Calcineurin A Levels in Mice. Mol. Neurobiol. 2018, 55, 7949–7960. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.H.; Shi, H.S.; Zhu, W.L.; Wu, P.; Sun, L.L.; Si, J.J.; Liu, M.M.; Zhang, Y.; Suo, L.; Yang, J.L. Venlafaxine facilitates between-session extinction and prevents reinstatement of auditory-cue conditioned fear. Behav. Brain Res. 2012, 230, 268–273. [Google Scholar] [CrossRef]
- Kakui, N.; Yokoyama, F.; Yamauchi, M.; Kitamura, K.; Imanishi, T.; Inoue, T.; Koyama, T. Anxiolytic-like profile of mirtazapine in rat conditioned fear stress model: Functional significance of 5-hydroxytryptamine 1A receptor and alpha1-adrenergic receptor. Pharmacol. Biochem. Behav. 2009, 92, 393–398. [Google Scholar] [CrossRef]
- An, Y.; Inoue, T.; Kitaichi, Y.; Nakagawa, S.; Wang, C.; Chen, C.; Song, N.; Kusumi, I. Combined treatment with subchronic lithium and acute intracerebral mirtazapine microinjection into the median raphe nucleus exerted an anxiolytic-like effect synergistically. Eur. J. Pharmacol. 2016, 783, 112–116. [Google Scholar] [CrossRef]
- Sun, T.; He, W.; Hu, G.; Li, M. Anxiolytic-like property of risperidone and olanzapine as examined in multiple measures of fear in rats. Pharmacol. Biochem. Behav. 2010, 95, 298–307. [Google Scholar] [CrossRef]
- Milstein, J.A.; Elnabawi, A.; Vinish, M.; Swanson, T.; Enos, J.K.; Bailey, A.M.; Kolb, B.; Frost, D.O. Olanzapine treatment of adolescent rats causes enduring specific memory impairments and alters cortical development and function. PLoS ONE 2013, 8, e57308. [Google Scholar] [CrossRef] [PubMed]
- Ganella, D.E.; Lee-Kardashyan, L.; Luikinga, S.J.; Nguyen, D.L.D.; Madsen, H.B.; Zbukvic, I.C.; Coulthard, R.; Lawrence, A.J.; Kim, J.H. Aripiprazole Facilitates Extinction of Conditioned Fear in Adolescent Rats. Front. Behav. Neurosci. 2017, 11, 76. [Google Scholar] [CrossRef] [PubMed]
- Dubrovina, N.I.; Zinov’eva, D.V. Effects of activation and blockade of dopamine receptors on the extinction of a passive avoidance reaction in mice with a depressive-like state. Neurosci. Behav. Physiol. 2010, 40, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, L.B.; Klein, S.; Prinssen, E.P. Defensive-like behaviors induced by ultrasound: Further pharmacological characterization in Lister-hooded rats. Psychopharmacology 2007, 194, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Gazarini, L.; Stern, C.A.; Carobrez, A.P.; Bertoglio, L.J. Enhanced noradrenergic activity potentiates fear memory consolidation and reconsolidation by differentially recruiting α1- and β-adrenergic receptors. Learn. Mem. 2013, 20, 210–219. [Google Scholar] [CrossRef]
- Lucas, E.K.; Wu, W.C.; Roman-Ortiz, C.; Clem, R.L. Prazosin during fear conditioning facilitates subsequent extinction in male C57Bl/6N mice. Psychopharmacology 2018, 236, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Schmidt do Prado-Lima, P.A.; Perrenoud, M.F.; Kristensen, C.H.; Cammarota, M.; Izquierdo, I. Topiramate diminishes fear memory consolidation and extinguishes conditioned fear in rats. J. Psychiatry Neurosci. 2011, 36, 250–255. [Google Scholar] [CrossRef][Green Version]
- Rau, V.; DeCola, J.P.; Fanselow, M.S. Stress-induced enhancement of fear learning: An animal model of posttraumatic stress disorder. Neurosci. Biobehav. Rev. 2005, 29, 1207–1223. [Google Scholar] [CrossRef]
- Liberzon, I.; Krstov, M.; Young, E.A. Stress-restress: Effects on ACTH and fast feedback. Psychoneuroendocrinology 1997, 22, 443–453. [Google Scholar] [CrossRef]
- Vanderheyden, W.M.; George, S.A.; Urpa, L.; Kehoe, M.; Liberzon, I.; Poe, G.R. Sleep alterations following exposure to stress predict fear-associated memory impairments in a rodent model of PTSD. Exp. Brain Res. 2015, 233, 2335–2346. [Google Scholar] [CrossRef]
- Han, F.; Jiang, J.; Ding, J.; Liu, H.; Xiao, B.; Shi, Y. Change of Rin1 and Stathmin in the animal model of traumatic stresses. Front. Behav. Neurosci. 2017, 11, 62. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, Y.; Morinobu, S.; Takahashi, T.; Yamawaki, S. Single prolonged stress increases contextual freezing and the expression of glycine transporter 1 and vesicle-associated membrane protein 2 mRNA in the hippocampus of rats. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2007, 31, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.M.; Schreiber, W.B.; Stanfield, B.R.; Knox, D. Inhibiting corticosterone synthesis during fear memory formation exacerbates cued fear extinction memory deficits within the single prolonged stress model. Behav. Brain Res. 2015, 287, 182–186. [Google Scholar] [CrossRef]
- Zoladz, P.R.; Conrad, C.D.; Fleshner, M.; Diamond, D.M. Acute episodes of predator exposure in conjunction with chronic social instability as an animal model of post-traumatic stress disorder. Stress 2008, 11, 259–281. [Google Scholar] [CrossRef] [PubMed]
- Zoladz, P.R.; Fleshner, M.; Diamond, D.M. Psychosocial animal model of PTSD produces a long-lasting traumatic memory, an increase in general anxiety and PTSD-like glucocorticoid abnormalities. Psychoneuroendocrinology 2012, 37, 1531–1545. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.; Zohar, J. An animal model of posttraumatic stress disorder: The use of cut-off behavioral criteria. Ann. N. Y. Acad. Sci. 2004, 1032, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Daskalakis, N.P.; Yehuda, R.; Diamond, D.M. Animal models in translational studies of PTSD. Psychoneuroendocrinology 2013, 38, 1895–1911. [Google Scholar] [CrossRef]
- Maren, S.; Holmes, A. Stress and Fear Extinction. Neuropsychopharmacology 2016, 41, 58–79. [Google Scholar] [CrossRef]
- Parks, C.L.; Robinson, P.S.; Sibille, E.; Shenk, T.; Toth, M. Increased anxiety of mice lacking the serotonin1A receptor. Proc. Natl. Acad. Sci. USA 1998, 95, 10734–10739. [Google Scholar] [CrossRef]
- Holmes, A.; Yang, R.J.; Lesch, K.P.; Crawley, J.N.; Murphy, D.L. Mice lacking the serotonin transporter exhibit 5-HT(1A) receptor-mediated abnormalities in tests for anxiety-like behavior. Neuropsychopharmacology 2003, 28, 2077–2088. [Google Scholar] [CrossRef]
- Klemenhagen, K.C.; Gordon, J.A.; David, D.J.; Hen, R.; Gross, C.T. Increased fear response to contextual cues in mice lacking the 5-HT1A receptor. Neuropsychopharmacology 2006, 31, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Wellman, C.L.; Izquierdo, A.; Garrett, J.E.; Martin, K.P.; Carroll, J.; Millstein, R.; Lesch, K.P.; Murphy, D.L.; Holmes, A. Impaired stress-coping and fear extinction and abnormal corticolimbic morphology in serotonin transporter knock-out mice. J. Neurosci. 2007, 27, 684–691. [Google Scholar] [CrossRef]
- Adamec, R.; Burton, P.; Blundell, J.; Murphy, D.L.; Holmes, A. Vulnerability to mild predator stress in serotonin transporter knockout mice. Behav. Brain Res. 2006, 170, 126–140. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, K.X.; Czesak, M.; Deria, M.; Le François, B.; Albert, P.R. Region-specific regulation of 5-HT1A receptor expression by Pet-1-dependent mechanisms in vivo. J. Neurochem. 2011, 116, 1066–1076. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, T.J.; Fyodorov, D.V.; Wegman, L.J.; Lelutiu, N.B.; Pehek, E.A.; Yamamoto, B.; Silver, J.; Weeber, E.J.; Sweatt, J.D.; Deneris, E.S. Pet-1 ETS gene plays a critical role in 5-HT neuron development and is required for normal anxiety-like and aggressive behavior. Neuron 2003, 37, 233–247. [Google Scholar] [CrossRef]
- Wellman, C.L.; Camp, M.; Jones, V.M.; MacPherson, K.P.; Ihne, J.; Fitzgerald, P.; Maroun, M.; Drabant, E.; Bogdan, R.; Hariri, A.R.; et al. Convergent effects of mouse Pet-1 deletion and human PET-1 variation on amygdala fear and threat processing. Exp. Neurol. 2013, 250, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Wang, Y.; Pattwell, S.; Jing, D.; Liu, T.; Zhang, Y.; Bath, K.G.; Lee, F.S.; Chen, Z.Y. Variant BDNF Val66Met polymorphism affects extinction of conditioned aversive memory. J. Neurosci. 2009, 29, 4056–4064. [Google Scholar] [CrossRef] [PubMed]
- Somerville, L.H.; Voss, H.U.; Glover, G.; Ballon, D.J.; Liston, C.; Teslovich, T.; Van Kempen, T.; Lee, F.S.; Casey, B.J. A genetic variant BDNF polymorphism alters extinction learning in both mouse and human. Science 2010, 327, 863–866. [Google Scholar] [CrossRef]
- Thoeringer, C.K.; Henes, K.; Eder, M.; Dahlhoff, M.; Wurst, W.; Holsboer, F.; Deussing, J.M.; Moosmang, S.; Wotjak, C.T. Consolidation of remote fear memories involves Corticotropin-Releasing Hormone (CRH) receptor type 1-mediated enhancement of AMPA receptor GluR1 signaling in the dentate gyrus. Neuropsychopharmacology 2012, 37, 787–796. [Google Scholar] [CrossRef]
- Verma, D.; Tasan, R.O.; Herzog, H.; Sperk, G. NPY controls fear conditioning and fear extinction by combined action on Y₁ and Y₂ receptors. Br. J. Pharmacol. 2012, 166, 1461–1473. [Google Scholar] [CrossRef]
- Joseph, A.; Tang, M.; Mamiya, T.; Chen, Q.; Yang, L.L.; Jiao, J.; Yu, N.; Tang, Y.P. Temporal association of elevated cholecystokininergic tone and adolescent trauma is critical for posttraumatic stress disorder-like behavior in adult mice. Proc. Natl. Acad. Sci. USA 2013, 110, 6589–6594. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N. Nutrition and cognitive function. Brain Dev. 1997, 19, 165–170. [Google Scholar] [CrossRef]
- Sakayori, N.; Kikkawa, T.; Tokuda, H.; Kiryu, E.; Yoshizaki, K.; Kawashima, H.; Yamada, T.; Arai, H.; Kang, J.X.; Katagiri, H.; et al. Maternal dietary imbalance between omega-6 and omega-3 polyunsaturated fatty acids impairs neocortical development via epoxy metabolites. Stem Cells 2016, 34, 470–482. [Google Scholar] [CrossRef] [PubMed]
- Arvindakshan, M.; Ghate, M.; Ranjekar, P.K.; Evans, D.R.; Mahadik, S.P. Supplementation with a combination of omega-3 fatty acids and antioxidants (vitamins E and C) improves the outcome of schizophrenia. Schizophr. Res. 2003, 62, 195–204. [Google Scholar] [CrossRef]
- Vancassel, S.; Durand, G.; Barthélémy, C.; Lejeune, B.; Martineau, J.; Guilloteau, D.; Andrès, C.; Chalon, S. Plasma fatty acid levels in autistic children. Prostaglandins Leukot. Essent. Fatty Acids 2011, 65, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, M.; Takashima, N.; Matsumata, M.; Ikegami, S.; Kontani, M.; Hara, Y.; Kawashima, H.; Owada, Y.; Kiso, Y.; Yoshikawa, T.; et al. Arachidonic acid drives postnatal neurogenesis and elicits a beneficial effect on prepulse inhibition, a biological trait of psychiatric illnesses. PLoS ONE 2009, 4, e5085. [Google Scholar] [CrossRef] [PubMed]
- de Vries, G.J.; Mocking, R.; Lok, A.; Assies, J.; Schene, A.; Olff, M. Fatty acid concentrations in patients with posttraumatic stress disorder compared to healthy controls. J. Affect. Disord. 2016, 205, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, Y.; Nishi, D.; Nakaya, N.; Sone, T.; Hamazaki, K.; Hamazaki, T.; Koido, Y. Attenuating posttraumatic distress with omega-3 polyunsaturated fatty acids among disaster medical assistance team members after the Great East Japan Earthquake: The APOP randomized controlled trial. BMC Psychiatry 2011, 11, 132. [Google Scholar] [CrossRef]
- Matsuoka, Y. Clearance of fear memory from the hippocampus through neurogenesis by omega-3 fatty acids: A novel preventive strategy for posttraumatic stress disorder? Biopsychosoc. Med. 2011, 5, 3. [Google Scholar] [CrossRef]
- Matsuoka, Y.; Nishi, D.; Yonemoto, N.; Hamazaki, K.; Hashimoto, K.; Hamazaki, T. Omega-3 fatty acids for secondary prevention of posttraumatic stress disorder after accidental injury: An open-label pilot study. J. Clin. Psychopharmacol. 2010, 30, 217–219. [Google Scholar] [CrossRef]
- Kitamura, T.; Saitoh, Y.; Takashima, N.; Murayama, A.; Niibori, Y.; Ageta, H.; Sekiguchi, M.; Sugiyama, H.; Inokuchi, K. Adult neurogenesis modulates the hippocampus-dependent period of associative fear memory. Cell 2009, 139, 814–827. [Google Scholar] [CrossRef] [PubMed]
- Jansen, D.; Zerbi, V.; Arnoldussen, I.A.; Wiesmann, M.; Rijpma, A.; Fang, X.T.; Dederen, P.J.; Mutsaers, M.P.; Broersen, L.M.; Lütjohann, D.; et al. Effects of specific multi-nutrient enriched diets on cerebral metabolism, cognition and neuropathology in AβPPswe-PS1dE9 mice. PLoS ONE 2013, 8, e75393. [Google Scholar] [CrossRef]
- Kawakita, E.; Hashimoto, M.; Shido, O. Docosahexaenoic acid promotes neurogenesis in vitro and in vivo. Neuroscience 2006, 139, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.Z.; Li, X.; Godbout, R. A novel fatty acid-binding protein (FABP) gene resulting from tandem gene duplication in mammals: Transcription in rat retina and testis. Genomics 2008, 92, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Furuhashi, M.; Hotamisligil, G.S. Fatty acid-binding proteins: Role in metabolic diseases and potential as drug targets. Nat. Rev. Drug Discov. 2008, 7, 489–503. [Google Scholar] [CrossRef] [PubMed]
- Owada, Y.; Yoshimoto, T.; Kondo, H. Spatio-temporally differential expression of genes for three members of fatty acid binding proteins in developing and mature rat brains. J. Chem. Neuroanat. 1996, 12, 113–122. [Google Scholar] [CrossRef]
- Matsumata, M.; Sakayori, N.; Maekawa, M.; Owada, Y.; Yoshikawa, T.; Osumi, N. The effects of Fabp7 and Fabp5 on postnatal hippocampal neurogenesis in the mouse. Stem Cells 2012, 30, 1532–1543. [Google Scholar] [CrossRef] [PubMed]
- Owada, Y.; Abdelwahab, S.A.; Kitanaka, N.; Sakagami, H.; Takano, H.; Sugitani, Y.; Sugawara, M.; Kawashima, H.; Kiso, Y.; Mobarakeh, J.I.; et al. Altered emotional behavioral responses in mice lacking brain-type fatty acid-binding protein gene. Eur. J. Neurosci. 2006, 24, 175–187. [Google Scholar] [CrossRef]
- Gerstner, J.R.; Perron, I.J.; Riedy, S.M.; Yoshikawa, T.; Kadotani, H.; Owada, Y.; Van Dongen, H.P.A.; Galnte, R.J.; Dickinson, K.; Yin, J.C.P.; et al. Normal sleep requires the astrocyte brain-type fatty acid binding protein FABP7. Sci. Adv. 2017, 3, e1602663. [Google Scholar] [CrossRef]
- Takeuchi, Y.; Fukunaga, K. Differential subcellular localization of two dopamine D2 receptor isoforms in transfected NG108-15 cells. J. Neurochem. 2003, 85, 1064–1074. [Google Scholar] [CrossRef]
- Shioda, N.; Yamamoto, Y.; Watanabe, M.; Binas, B.; Owada, Y.; Fukunaga, K. Heart-type fatty acid binding protein regulates dopamine D2 receptor function in mouse brain. J. Neurosci. 2010, 30, 3146–3155. [Google Scholar] [CrossRef] [PubMed]
- Shioda, N.; Yabuki, Y.; Kobayashi, Y.; Onozato, M.; Owada, Y.; Fukunaga, K. FABP3 protein promotes α-synuclein oligomerization associated with 1-methyl-1,2,3,6-tetrahydropiridine-induced neurotoxicity. J. Biol. Chem. 2014, 289, 18957–18965. [Google Scholar] [CrossRef] [PubMed]
- Shimamoto, C.; Ohnishi, T.; Maekawa, M.; Watanabe, A.; Ohba, H.; Arai, R.; Iwayama, Y.; Hisano, Y.; Toyota, T.; Toyoshima, M.; et al. Functional characterization of FABP3, 5 and 7 gene variants identified in schizophrenia and autism spectrum disorder and mouse behavioral studies. Hum. Mol. Genet. 2014, 23, 6495–6511. [Google Scholar] [CrossRef] [PubMed]
- Yabuki, Y.; Takahata, I.; Matsuo, K.; Owada, Y.; Fukunaga, K. Ramelteon Improves Post-traumatic Stress Disorder-Like Behaviors Exhibited by Fatty Acid-Binding Protein 3 Null Mice. Mol. Neurobiol. 2018, 55, 3577–3591. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Kida, H.; Kagawa, Y.; Yasumoto, Y.; Miyazaki, H.; Islam, A.; Ogata, M.; Yanagawa, Y.; Mitsushima, D.; Fukunaga, K.; et al. FABP3 in the Anterior Cingulate Cortex Modulates the Methylation Status of the Glutamic Acid Decarboxylase67 Promoter Region. J. Neurosci. 2018, 38, 10411–10423. [Google Scholar] [CrossRef] [PubMed]
- Amaral, O.B.; Roesler, R. Targeting the NMDA receptor for fear-related disorders. Recent Pat. CNS Drug Discov. 2008, 3, 166–178. [Google Scholar] [CrossRef]
- Burgos-Robles, A.; Vidal-Gonzalez, I.; Santini, E.; Quirk, G.J. Consolidation of fear extinction requires NMDA receptor-dependent bursting in the ventromedial prefrontal cortex. Neuron 2007, 53, 871–880. [Google Scholar] [CrossRef]
- Lerea, L.S.; Butler, L.S.; McNamara, J.O. NMDA and non-NMDA receptor-mediated increase of c-fos mRNA in dentate gyrus neurons involves calcium influx via different routes. J. Neurosci. 1992, 12, 2973–2981. [Google Scholar] [CrossRef]
- Comai, S.; Gobbi, G. Unveiling the role of melatonin MT2 receptors in sleep, anxiety and other neuropsychiatric diseases: A novel target in psychopharmacology. J. Psychiatry Neurosci. 2014, 39, 6–21. [Google Scholar] [CrossRef]
- Doyen, C.; Mighiu, D.; Kaye, K.; Colineaux, C.; Beaumanoir, C.; Mouraeff, Y.; Rieu, C.; Paubel, P.; Contejean, Y. Melatonin in children with autistic spectrum disorders: Recent and practical data. Eur. Child Adolesc. Psychiatry 2011, 20, 231–239. [Google Scholar] [CrossRef]
- Huang, F.; Yang, Z.; Liu, X.; Li, C.Q. Melatonin facilitates extinction, but not acquisition or expression, of conditional cued fear in rats. BMC Neurosci. 2014, 15, 86. [Google Scholar] [CrossRef][Green Version]
- Nishiyama, K.; Shintani, Y.; Hirai, K.; Yoshikubo, S. Molecular cloning and pharmacological characterization of monkey MT1 and MT2 melatonin receptors showing high affinity for the agonist ramelteon. J. Pharmacol. Exp. Ther. 2009, 330, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Lacoste, B.; Angeloni, D.; Dominguez-Lopez, S.; Calderoni, S.; Mauro, A.; Fraschini, F.; Descarries, L.; Gobbi, G. Anatomical and cellular localization of melatonin MT1 and MT2 receptors in the adult rat brain. J. Pineal Res. 2015, 58, 397–417. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Yabuki, Y.; Moriguchi, S.; Fukunaga, K.; Mao, P.J.; Hong, L.J.; Lu, Y.M.; Wang, R.; Ahmed, M.M.; Liao, M.H.; et al. Melatonin reverses the decreases in hippocampal protein serine/threonine kinases observed in an animal model of autism. J. Pineal Res. 2014, 56, 1–11. [Google Scholar] [CrossRef]
- Zeng, W.; Mak, D.O.; Li, Q.; Shin, D.M.; Foskett, J.K.; Muallem, S. A new mode of Ca2+ signaling by G protein-coupled receptors: Gating of IP3 receptor Ca2+ release channels by Gbetagamma. Curr. Biol. 2003, 13, 872–876. [Google Scholar] [CrossRef]
- Domínguez-Alonso, A.; Valdés-Tovar, M.; Solís-Chagoyán, H.; Benítez-King, G. Melatonin stimulates dendrite formation and complexity in the hilar zone of the rat hippocampus: Participation of the Ca++/Calmodulin complex. Int. J. Mol. Sci. 2015, 16, 1907–1927. [Google Scholar] [CrossRef]
- Fukunaga, K.; Yabuki, Y.; Takahata, I.; Matsuo, K. Neurological mechanism and therapeutic strategy for posttraumatic stress disorders. Nihon Yakurigaku Zasshi 2018, 152, 194–201. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ho, A.K.; Chik, C.L. Modulation of Aanat gene transcription in the rat pineal gland. J. Neurochem. 2010, 112, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.L.; Ressler, K.J.; Lu, K.T.; Davis, M. Facilitation of conditioned fear extinction by systemic administration or intra-amygdala infusions of D-cycloserine as assessed with fear-potentiated startle in rats. J. Neurosci. 2002, 22, 2343–2351. [Google Scholar] [CrossRef]
- Ledgerwood, L.; Richardson, R.; Cranney, J. D-cycloserine facilitates extinction of learned fear: Effects on reacquisition and generalized extinction. Biol. Psychiatry 2005, 57, 841–847. [Google Scholar] [CrossRef]
- Attari, A.; Rajabi, F.; Maracy, M.R. D-cycloserine for treatment of numbing and avoidance in chronic post traumatic stress disorder: A randomized, double blind, clinical trial. J. Res. Med. Sci. 2014, 19, 592–598. [Google Scholar] [PubMed]
- Shukla, M.; Govitrapong, P.; Boontem, P.; Reiter, R.J.; Satayavivad, J. Mechanisms of Melatonin in Alleviating Alzheimer’s Disease. Curr. Neuropharmacol. 2017, 15, 1010–1031. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, A.C.; Barton, C.A.; Briggs, N.; Kennaway, D.J. The relationship between urinary melatonin metabolite excretion and posttraumatic symptoms following traumatic injury. J. Affect. Disord. 2010, 127, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Agorastos, A.; Linthorst, A.C. Potential pleiotropic beneficial effects of adjuvant melatonergic treatment in posttraumatic stress disorder. J. Pineal Res. 2016, 61, 3–26. [Google Scholar] [CrossRef] [PubMed]
- R T Ramirez, R.; Poling, M.I.; deCourten, J.F.; Chamberlain, R.L. Potential positive feedback loop of pineal cyst and posttraumatic stress disorder. Med. Hypotheses 2017, 100, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Alvira, D.; Tajes, M.; Verdaguer, E.; Acuña-Castroviejo, D.; Folch, J.; Camins, A.; Pallas, M. Inhibition of the cdk5/p25 fragment formation may explain the antiapoptotic effects of melatonin in an experimental model of Parkinson’s disease. J. Pineal Res. 2006, 40, 251–258. [Google Scholar] [CrossRef]
- Sase, A.S.; Lombroso, S.I.; Santhumayor, B.A.; Wood, R.R.; Lim, C.J.; Neve, R.L.; Heller, E.A. Sex-Specific Regulation of Fear Memory by Targeted Epigenetic Editing of Cdk5. Biol. Psychiatry 2019, 85, 623–634. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Treatment | Effects on PTSD Symptoms | Animal Models |
|---|---|---|
| SSRI | ||
| Fluoxetine | Improvement [64,68,69], Not effective [70] | Facilitation of fear extinction [95,96] |
| Paroxetine | Improvement [71,72] | Prevention of PTSD symptoms reactivation [97] |
| Sertraline | Improvement [73,74,75] | No effect on fear extinction [98] |
| SNRI | ||
| Venlafaxine | Improvement [76,77] | Facilitation of fear extinction [99] |
| Anti-depressant | ||
| Mirtazapine | Improvement [80], Not effective [18] | Relief of fear response [100,101] |
| Bupropion | Not effective [81] | Relief of fear response [100] |
| Antipsychotics | ||
| Risperidone | Improvement [82,83,84] | Facilitation of fear extinction [102] |
| Olanzapine | Improvement [85,86] | Relief of fear response [102], deficits of fear extinction [103] |
| Aripiprazole | Improvement [87] | Facilitation of fear extinction [104] |
| Sulpiride | No data | Facilitation of fear extinction [105] |
| Other drugs | ||
| Gabapentin (Calcium blocker) | Improvement [88] | Relief of anxiety response [106] |
| Prazosin (Alpha blocker) | Improvement [89,90], Not effective [91] | Relief of fear response [107], facilitation of fear extinction [108] |
| Topiramate (Anticonvulsant) | Improvement [92,93] | Facilitation of fear extinction [109] |
| Nabilone (Cannabinoid) | Improvement [94] | No data |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yabuki, Y.; Fukunaga, K. Clinical Therapeutic Strategy and Neuronal Mechanism Underlying Post-Traumatic Stress Disorder (PTSD). Int. J. Mol. Sci. 2019, 20, 3614. https://doi.org/10.3390/ijms20153614
Yabuki Y, Fukunaga K. Clinical Therapeutic Strategy and Neuronal Mechanism Underlying Post-Traumatic Stress Disorder (PTSD). International Journal of Molecular Sciences. 2019; 20(15):3614. https://doi.org/10.3390/ijms20153614
Chicago/Turabian StyleYabuki, Yasushi, and Kohji Fukunaga. 2019. "Clinical Therapeutic Strategy and Neuronal Mechanism Underlying Post-Traumatic Stress Disorder (PTSD)" International Journal of Molecular Sciences 20, no. 15: 3614. https://doi.org/10.3390/ijms20153614
APA StyleYabuki, Y., & Fukunaga, K. (2019). Clinical Therapeutic Strategy and Neuronal Mechanism Underlying Post-Traumatic Stress Disorder (PTSD). International Journal of Molecular Sciences, 20(15), 3614. https://doi.org/10.3390/ijms20153614