The Association of Periodontitis and Peripheral Arterial Occlusive Disease—A Systematic Review


 ,
,
Abstract
:1. Introduction
2. Results
2.1. Association between PD or Tooth Loss and PAOD
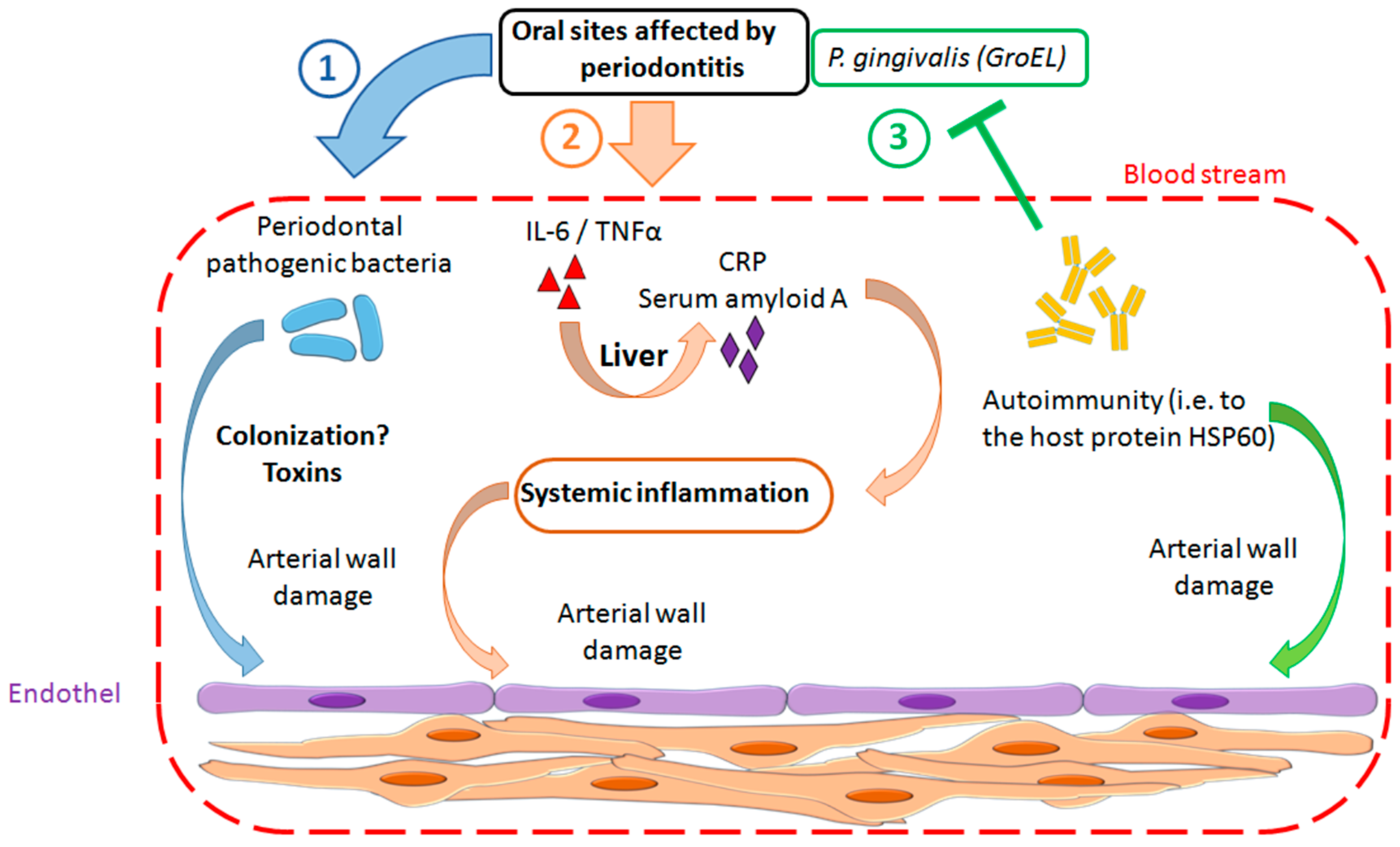
2.2. Pathomechanism
3. Discussion
4. Methods
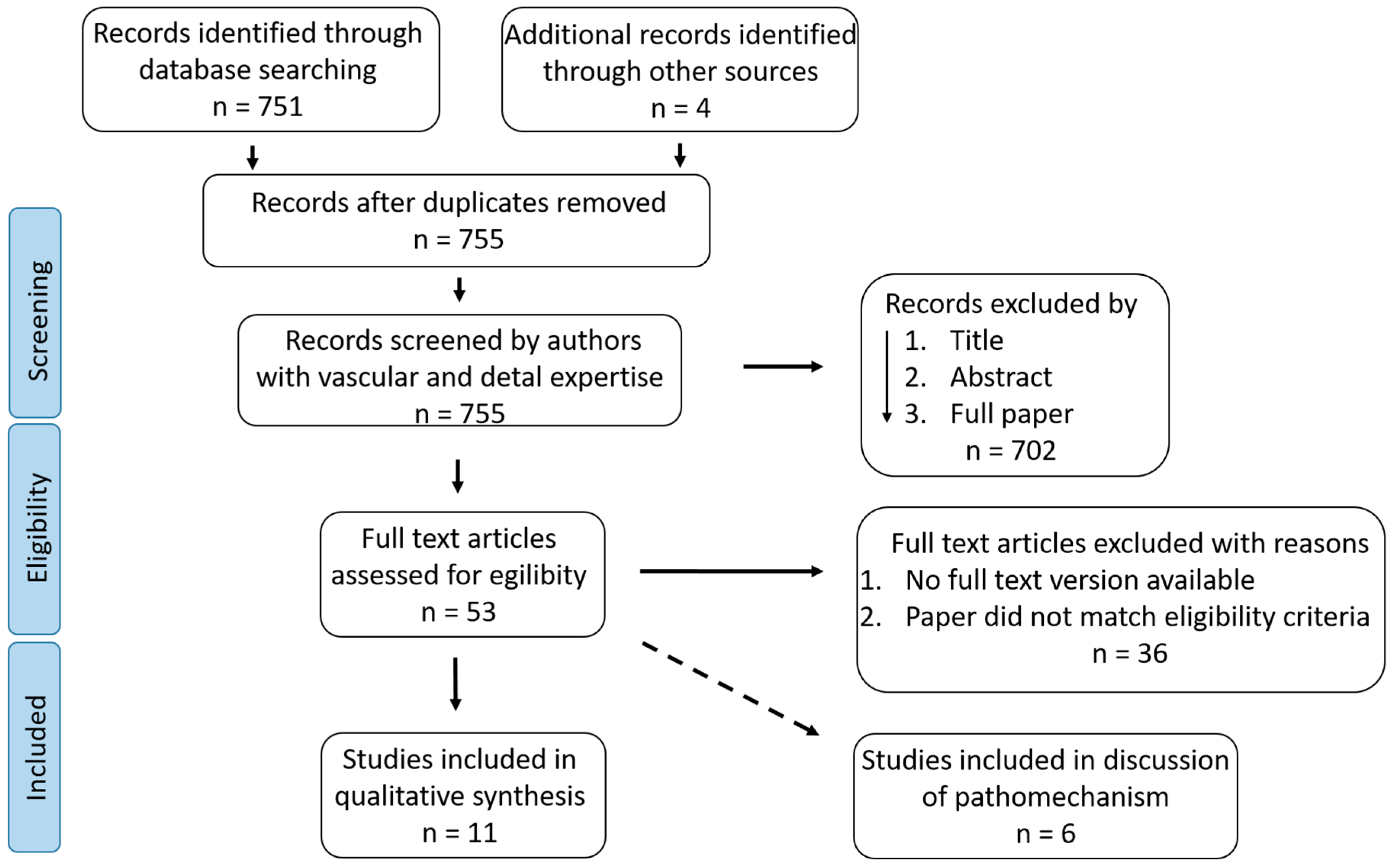
4.1. Literature Search
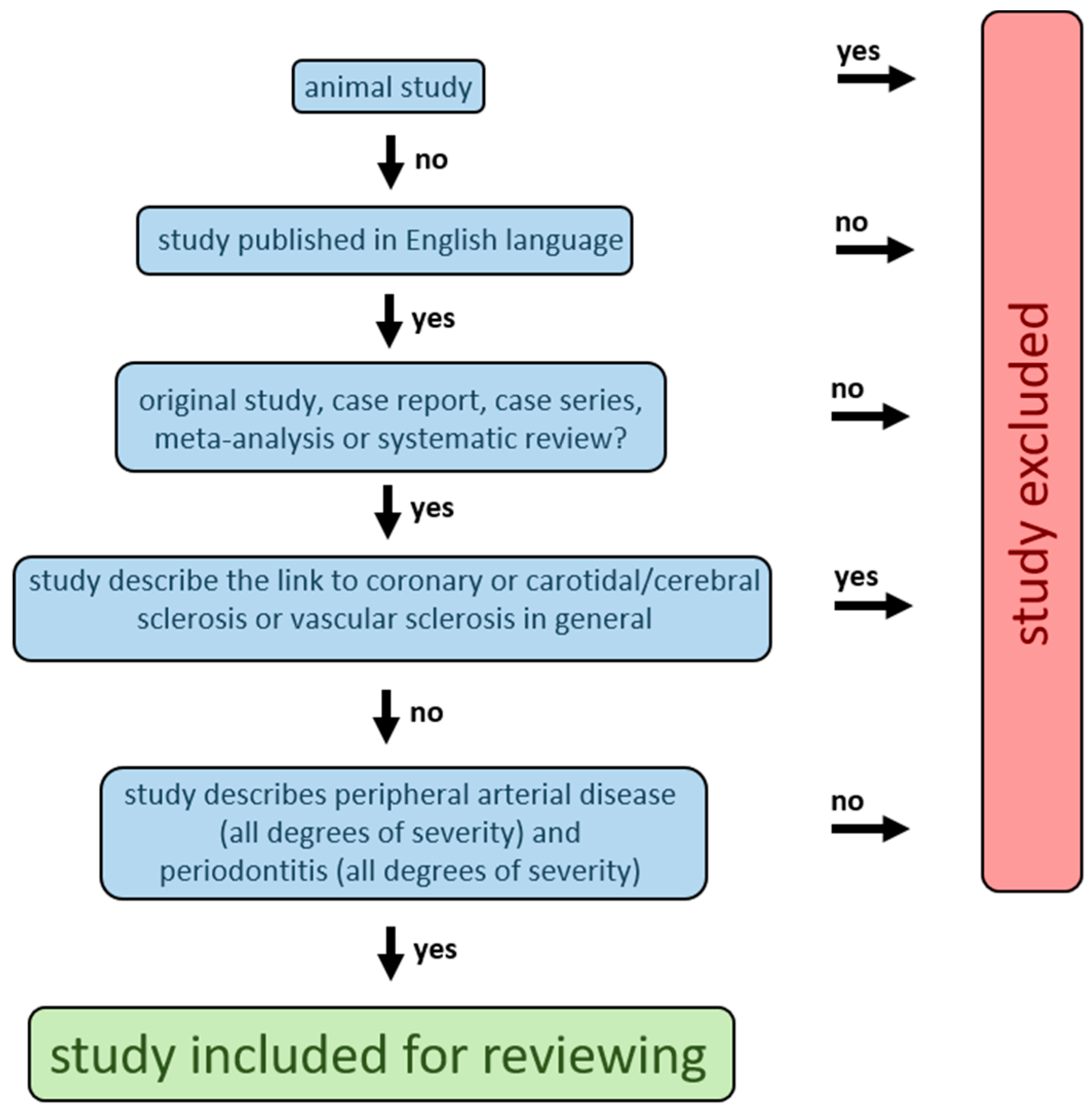
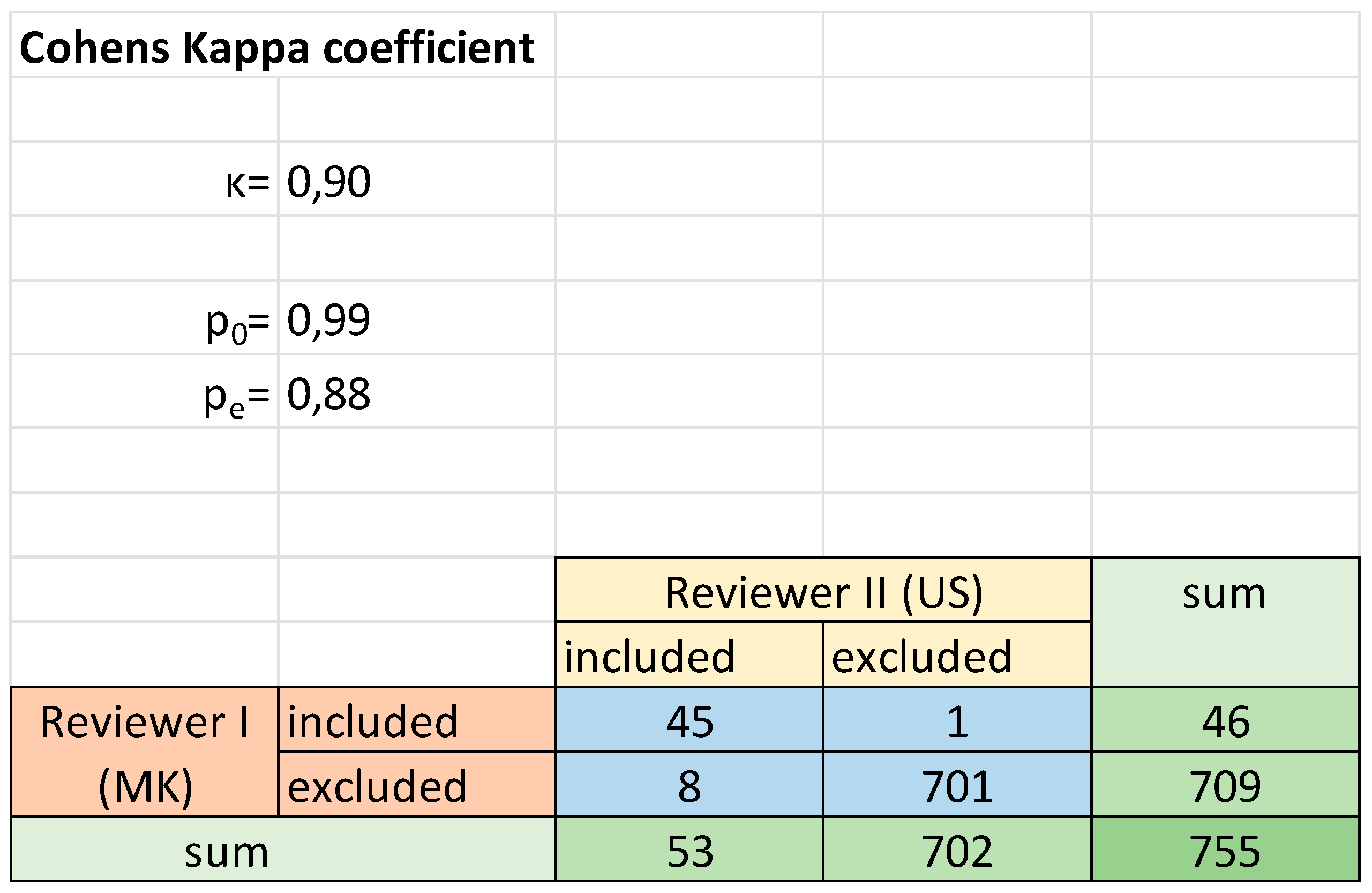
4.2. Study Selection and Data Extraction
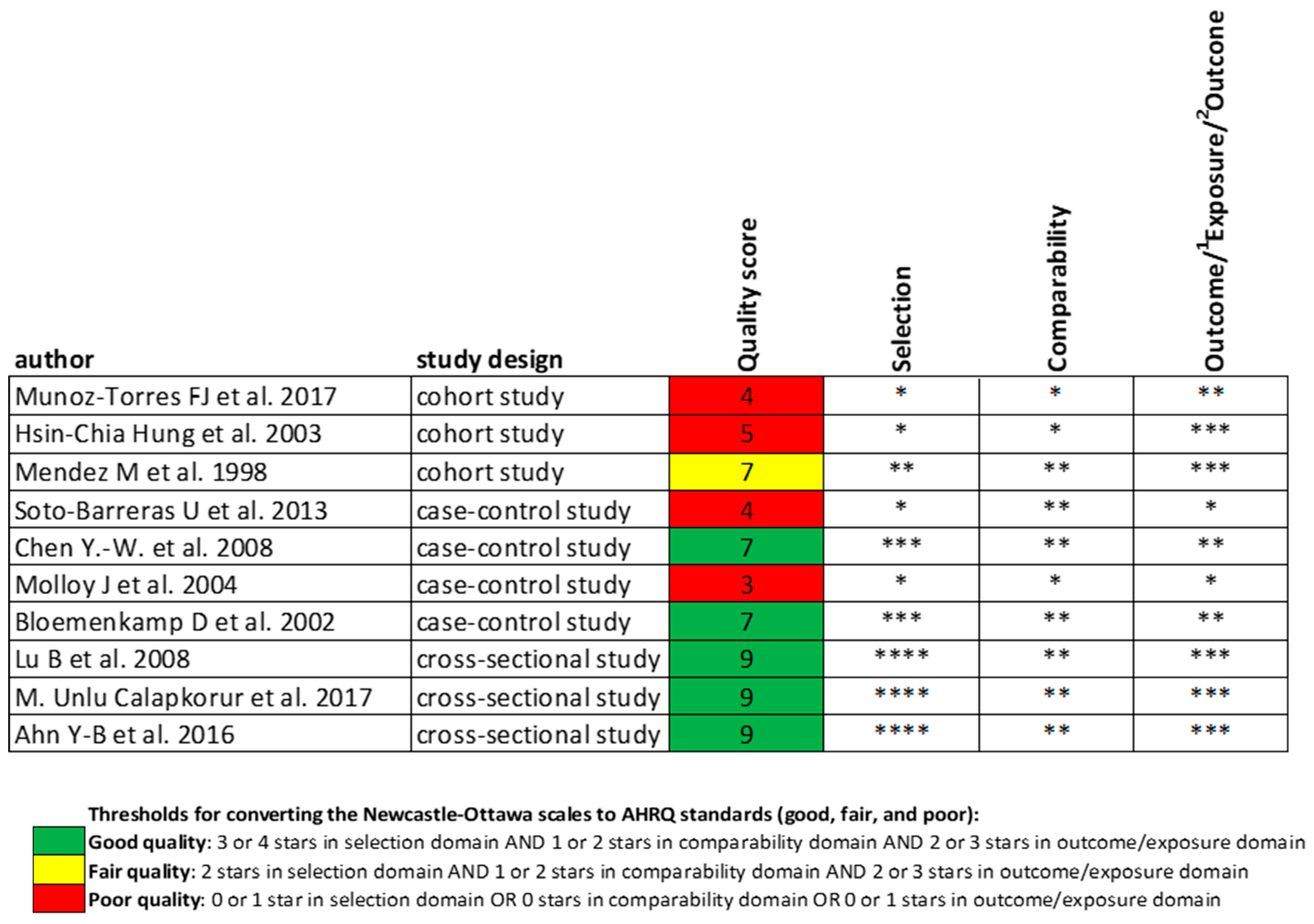
4.3. Quality Assessment
5. Conclusions
Supplementary Materials
Funding
Conflicts of Interest
Appendix A

References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Sampson, U.K.A.; Fowkes, F.G.R.; McDermott, M.M.; Criqui, M.H.; Aboyans, V.; Norman, P.E.; Forouzanfar, M.H.; Naghavi, M.; Song, Y.; Harrell, F.E., Jr.; et al. Global and Regional Burden of Death and Disability from Peripheral Artery Disease: 21 World Regions, 1990 to 2010. Glob. Heart 2014, 9, 145–158. [Google Scholar] [CrossRef]
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Creager, M.A. The Crisis of Vascular Disease and the Journey to Vascular Health. Circulation 2016, 133, 2593–2598. [Google Scholar] [CrossRef] [PubMed]
- Malyar, N.; Fürstenberg, T.; Wellmann, J.; Meyborg, M.; Lüders, F.; Gebauer, K.; Bunzemeier, H.; Roeder, N.; Reinecke, H. Recent trends in morbidity and in-hospital outcomes of in-patients with peripheral arterial disease: A nationwide population-based analysis. Eur. Heart J. 2013, 34, 2706–2714. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef] [PubMed]
- Hamburg, N.M.; Creager, M.A. Pathophysiology of Intermittent Claudication in Peripheral Artery Disease. Circ. J. 2017, 81, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Taleb, S. Inflammation in atherosclerosis. Arch. Cardiovasc. Dis. 2016, 109, 708–715. [Google Scholar] [CrossRef]
- Miao, C.-Y.; Li, Z.-Y. The role of perivascular adipose tissue in vascular smooth muscle cell growth. Br. J. Pharmacol. 2012, 165, 643–658. [Google Scholar] [CrossRef] [Green Version]
- Armitage, G.C. Periodontal diagnoses and classification of periodontal diseases. Periodontol. 2000 2004, 34, 9–21. [Google Scholar] [CrossRef]
- Matarese, G.; Ramaglia, L.; Fiorillo, L.; Cervino, G.; Lauritano, F.; Isola, G. Implantology and Periodontal Disease: The Panacea to Problem Solving? Open Dent. J. 2017, 11, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Thornton-Evans, G.; Eke, P.; Wei, L.; Palmer, A.; Moeti, R.; Hutchins, S.; Borrell, L.N. Periodontitis among adults aged ≥30 years—United States, 2009–2010. MMWR Suppl. 2013, 62, 129–135. [Google Scholar] [PubMed]
- Ferlazzo, N.; Currò, M.; Zinellu, A.; Caccamo, D.; Isola, G.; Ventura, V.; Carru, C.; Matarese, G.; Ientile, R. Influence of MTHFR Genetic Background on p16 and MGMT Methylation in Oral Squamous Cell Cancer. Int. J. Mol. Sci. 2017, 18, 724. [Google Scholar] [CrossRef] [PubMed]
- Cury, E.Z.; Santos, V.R.; da Silva Maciel, S.; Gonçalves, T.E.D.; Zimmermann, G.S.; Mota, R.M.S.; Figueiredo, L.C.; Duarte, P.M. Lipid parameters in obese and normal weight patients with or without chronic periodontitis. Clin. Oral Investig. 2018, 22, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Aarabi, G.; Heydecke, G.; Seedorf, U. Roles of Oral Infections in the Pathomechanism of Atherosclerosis. Int. J. Mol. Sci. 2018, 19, 1978. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.V.; Scott, T.; LaMorte, W.; Vokonas, P.; Menzoian, J.O.; Garcia, R. An Association between Periodontal Disease and Peripheral Vascular Disease. Am. J. Surg. 1998, 176, 153–157. [Google Scholar] [CrossRef]
- Hung, H.-C.; Willett, W.; Merchant, A.; Rosner, B.A.; Ascherio, A.; Joshipura, K.J. Oral Health and Peripheral Arterial Disease. Circulation 2003, 107, 1152–1157. [Google Scholar] [CrossRef] [Green Version]
- Lu, B.; Parker, D.; Eaton, C.B. Relationship of periodontal attachment loss to peripheral vascular disease: An analysis of NHANES 1999–2002 data. Atherosclerosis 2008, 200, 199–205. [Google Scholar] [CrossRef]
- Muñoz-Torres, F.J.; Mukamal, K.J.; Pai, J.K.; Willett, W.; Joshipura, K.J. Relationship between Tooth Loss and Peripheral Arterial Disease among Women. J. Clin. Periodontol. 2017, 44, 989–995. [Google Scholar] [CrossRef]
- Yang, S.; Zhao, L.S.; Cai, C.; Shi, Q.; Wen, N.; Xu, J. Association between periodontitis and peripheral artery disease: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2018, 18, 141. [Google Scholar] [CrossRef]
- Soto-Barreras, U.; Olvera-Rubio, J.O.; Loyola-Rodríguez, J.P.; Reyes-Macías, J.F.; Martinez-Martinez, R.E.; Patiño-Marin, N.; Martinez-Castanon, G.-A.; Aradillas-García, C.; Little, J.W. Peripheral Arterial Disease Associated with Caries and Periodontal Disease. J. Periodontol. 2013, 84, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Çalapkorur, M.U.; Alkan, B.A.; Tasdemir, Z.; Akcali, Y.; Saatci, E. Association of peripheral arterial disease with periodontal disease: Analysis of inflammatory cytokines and an acute phase protein in gingival crevicular fluid and serum. J. Periodontal Res. 2017, 52, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Bloemenkamp, D.G.; van den Bosch, M.A.; Mali, W.P.; Tanis, B.C.; Rosendaal, F.R.; Kemmeren, J.M.; Algra, A.; Visseren, F.L.; Van Der Graaf, Y. Novel risk factors for peripheral arterial disease in young women. Am. J. Med. 2002, 113, 462–467. [Google Scholar] [CrossRef]
- Molloy, J.; Wolff, L.F.; Lopez-Guzman, A.; Hodges, J.S. The association of periodontal disease parameters with systemic medical conditions and tobacco use. J. Clin. Periodontol. 2004, 31, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.-B.; Shin, M.-S.; Han, D.-H.; Sukhbaatar, M.; Kim, M.-S.; Shin, H.-S.; Kim, H.-D. Periodontitis is associated with the risk of subclinical atherosclerosis and peripheral arterial disease in Korean adults. Atherosclerosis 2016, 251, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-W.; Umeda, M.; Nagasawa, T.; Takeuchi, Y.; Huang, Y.; Inoue, Y.; Iwai, T.; Izumi, Y.; Ishikawa, I. Periodontitis May Increase the Risk of Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Armingohar, Z.; Jørgensen, J.J.; Kristoffersen, A.K.; Abesha-Belay, E.; Olsen, I. Bacteria and bacterial DNA in atherosclerotic plaque and aneurysmal wall biopsies from patients with and without periodontitis. J. Oral Microbiol. 2014, 6, 23408. [Google Scholar] [CrossRef]
- Figuero, E.; Lindahl, C.; Marín, M.J.; Renvert, S.; Herrera, D.; Ohlsson, O.; Wetterling, T.; Sanz, M. Quantification of Periodontal Pathogens in Vascular, Blood, and Subgingival Samples from Patients with Peripheral Arterial Disease or Abdominal Aortic Aneurysms. J. Periodontol. 2014, 85, 1182–1193. [Google Scholar] [CrossRef]
- Armingohar, Z.; Jørgensen, J.J.; Kristoffersen, A.K.; Schenck, K.; Dembic, Z. Polymorphisms in the interleukin-10 gene and chronic periodontitis in patients with atherosclerotic and aortic aneurysmal vascular diseases. J. Oral Microbiol. 2015, 7, 26051. [Google Scholar] [CrossRef]
- Nishida, E.; Aino, M.; Kobayashi, S.-I.; Okada, K.; Ohno, T.; Kikuchi, T.; Hayashi, J.-I.; Yamamoto, G.; Hasegawa, Y.; Mitani, A. Serum Amyloid A Promotes E-Selectin Expression via Toll-Like Receptor 2 in Human Aortic Endothelial Cells. Mediat. Inflamm. 2016, 2016, 7150509. [Google Scholar] [CrossRef]
- Choi, J.-I.; Chung, S.-W.; Kang, H.-S.; Rhim, B.Y.; Kim, S.-J.; Kim, S.-J. Establishment of Porphyromonas gingivalis Heat-shock-protein-specific T-cell Lines from Atherosclerosis Patients. J. Dent. Res. 2002, 81, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Tse, H.F.; Yiu, K.H.; Li, L.S.W.; Jin, L. Effect of periodontal treatment on circulating CD34+ cells and peripheral vascular endothelial function: A randomized controlled trial. J. Clin. Periodontol. 2011, 38, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Leng, W.-D.; Zeng, X.-T.; Kwong, J.S.; Hua, X.-P. Periodontal disease and risk of coronary heart disease: An updated meta-analysis of prospective cohort studies. Int. J. Cardiol. 2015, 201, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, L.L.; Fu, R.; Buckley, D.I.; Freeman, M.; Helfand, M. Periodontal Disease and Coronary Heart Disease Incidence: A Systematic Review and Meta-analysis. J. Gen. Intern. Med. 2008, 23, 2079–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shultis, W.A.; Weil, E.J.; Looker, H.C.; Curtis, J.M.; Shlossman, M.; Genco, R.J.; Knowler, W.C.; Nelson, R.G. Effect of Periodontitis on Overt Nephropathy and End-Stage Renal Disease in Type 2 Diabetes. Diabetes Care 2007, 30, 306–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saremi, A.; Nelson, R.G.; Tulloch-Reid, M.; Hanson, R.L.; Sievers, M.L.; Taylor, G.W.; Shlossman, M.; Bennett, P.H.; Genco, R.; Knowler, W.C. Periodontal disease and mortality in type 2 diabetes. Diabetes Care 2005, 28, 27–32. [Google Scholar] [CrossRef]
- Jeffcoat, M.K.; Geurs, N.C.; Reddy, M.S.; Cliver, S.P.; Goldenberg, R.L.; Hauth, J.C. Periodontal infection and preterm birth: Results of a prospective study. J. Am. Dent. Assoc. 2001, 132, 875–880. [Google Scholar] [CrossRef]
- Offenbacher, S.; Katz, V.; Fertik, G.; Collins, J.; Boyd, D.; Maynor, G.; McKaig, R.; Beck, J. Periodontal Infection as a Possible Risk Factor for Preterm Low Birth Weight. J. Periodontol. 1996, 67, 1103–1113. [Google Scholar] [CrossRef]
- Belkin, N.; Damrauer, S.M. Peripheral Arterial Disease Genetics: Progress to Date and Challenges Ahead. Curr. Cardiol. Rep. 2017, 19, 131. [Google Scholar] [CrossRef]
- Aarabi, G.; Zeller, T.; Heydecke, G.; Munz, M.; Schãfer, A.; Seedorf, U. Roles of the Chr.9p21.3 ANRIL Locus in Regulating Inflammation and Implications for Anti-Inflammatory Drug Target Identification. Front. Cardiovasc. Med. 2018, 5, 47. [Google Scholar] [CrossRef] [Green Version]
- Jaff, M.R.; Dale, R.A.; Creager, M.A.; Lipicky, R.J.; Constant, J.; Campbell, L.A.; Hiatt, W.R. Anti-Chlamydial Antibiotic Therapy for Symptom Improvement in Peripheral Artery Disease. Prospective Evaluation of Rifalazil Effect on Vascular Symptoms of Intermittent Claudication and Other Endpoints in Chlamydia pneumoniae Seropositive Patients (PROVIDENCE-1). Circulation 2009, 119, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Joensen, J.B.; Juul, S.; Henneberg, E.; Thomsen, G.; Ostergaard, L.; Lindholt, J.S. Can long-term antibiotic treatment prevent progression of peripheral arterial occlusive disease? A large, randomized, double-blinded, placebo-controlled trial. Atherosclerosis 2008, 196, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 23 July 2015).
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, A. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref | Study Design | Strength of the Association between PD or Tooth Lost and PAOD | Participants | Limitations |
|---|---|---|---|---|
| [20] | systematic review and meta-analysis | RR = 1.70 (95% CI: 1.3–2.3; p = 0.01) * WMD = 3.75 (95% CI: 1.3–6.2; p = 0.003) | 4.307 | |
| [22] | cross-sectional study | OR = 5.8 (95% CI: 1.5–21.9; p = 0.009) | 60 | |
| [19] | cohort study | HR = 1.3 (95% CI: 1.0–1.7) | 79.663 | no adjustment for smoking |
| only women | ||||
| [25] | cross-sectional study | OR = 2.0 (95% CI: 1.0–3.9; p = 0.036) | 1.343 | |
| [21] | case-control study | OR = 8.2 (95% CI: 1.2–35.2; p = 0.031) | 60 | |
| [26] | case-control study | OR = 5.5 (95% CI: 1.6–18.9; p = 0.007) | 57 | |
| [18] | cross-sectional study | OR = 2.3 (95% CI: 1.2–4.2; p = 0.004) | 3.585 | |
| [24] | case-control study | **vascular disease p-value 0.014; **vascular surgery p-value 0.001 | 2.006 | |
| [17] | cohort study | RR = 1.41 (95% CI: 1.1–1.8) | 45.136 | only men |
| [23] | case-control study | OR = 3.0 (95% CI: 1.4–6.3) | 687 | only women |
| [16] | cohort study | OR = 2.27 (95% CI: 1.3–3.9; p = 0.003) | 1.110 | only men |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaschwich, M.; Behrendt, C.-A.; Heydecke, G.; Bayer, A.; Debus, E.S.; Seedorf, U.; Aarabi, G. The Association of Periodontitis and Peripheral Arterial Occlusive Disease—A Systematic Review. Int. J. Mol. Sci. 2019, 20, 2936. https://doi.org/10.3390/ijms20122936
Kaschwich M, Behrendt C-A, Heydecke G, Bayer A, Debus ES, Seedorf U, Aarabi G. The Association of Periodontitis and Peripheral Arterial Occlusive Disease—A Systematic Review. International Journal of Molecular Sciences. 2019; 20(12):2936. https://doi.org/10.3390/ijms20122936
Chicago/Turabian StyleKaschwich, Mark, Christian-Alexander Behrendt, Guido Heydecke, Andreas Bayer, Eike Sebastian Debus, Udo Seedorf, and Ghazal Aarabi. 2019. "The Association of Periodontitis and Peripheral Arterial Occlusive Disease—A Systematic Review" International Journal of Molecular Sciences 20, no. 12: 2936. https://doi.org/10.3390/ijms20122936