Harmful Effects and Potential Benefits of Anti-Tumor Necrosis Factor (TNF)-α on the Liver

 ,
,
Abstract
:1. Introduction
2. Methods
3. Chronic Viral Hepatitis
3.1. Hepatitis C
3.2. Hepatitis B
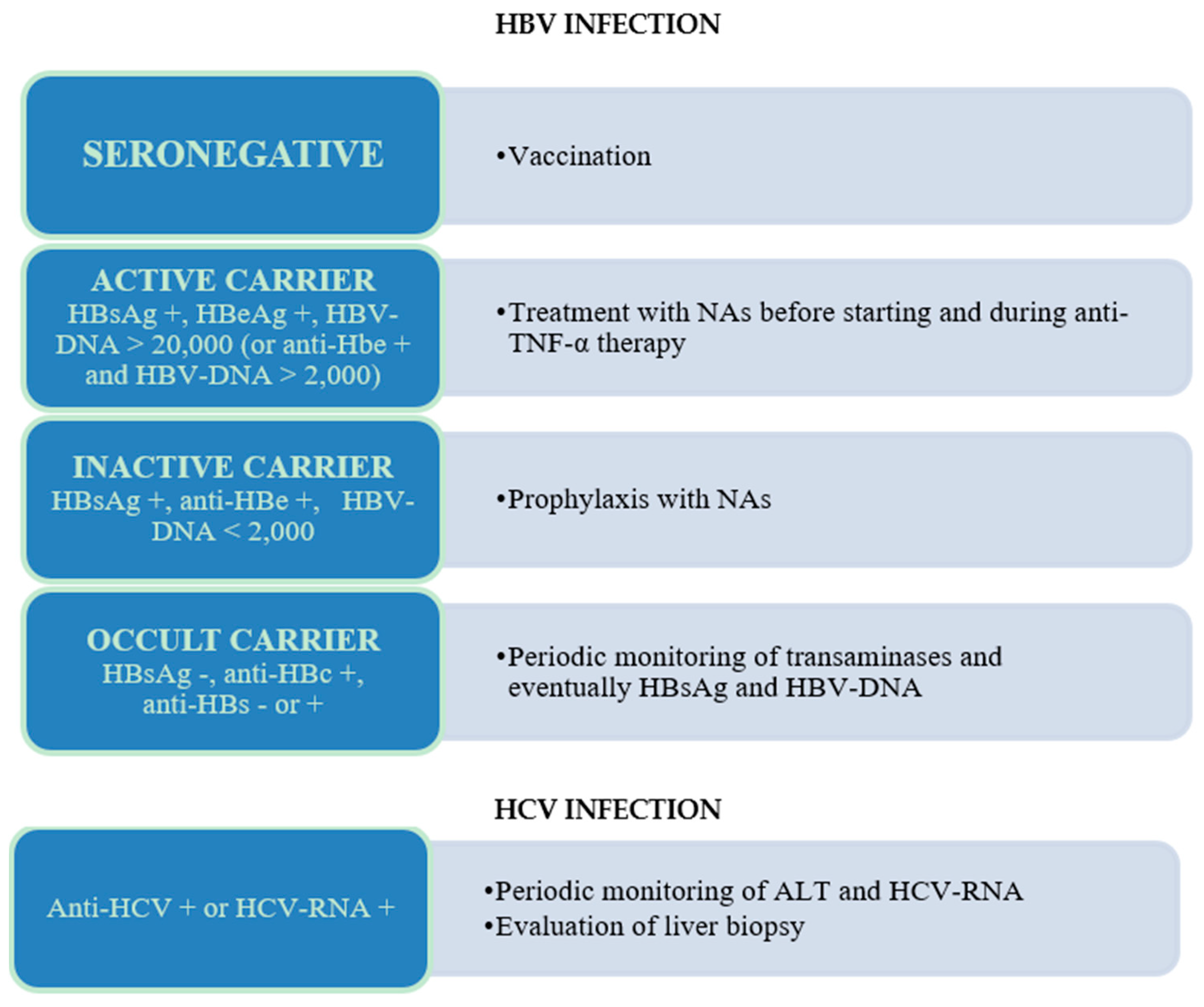
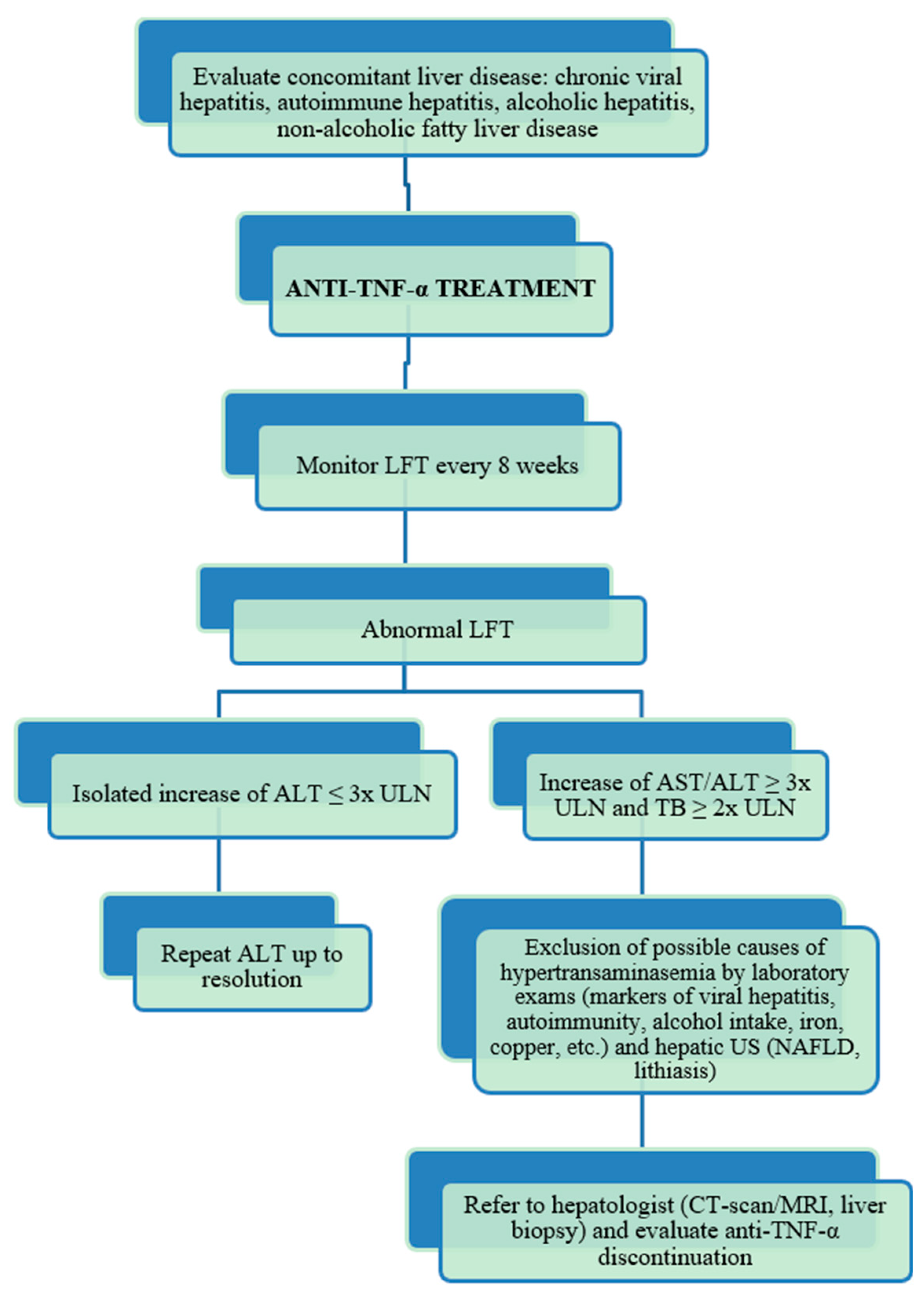
3.3. Recommendations for the Management of Patients with Hepatitis B Virus (HBV) or Hepatitis C Virus (HCV) Infection in Therapy with Anti-Tumor Necrosis Factor (Anti-TNF-α) Agents
4. Liver-Transplanted Patients
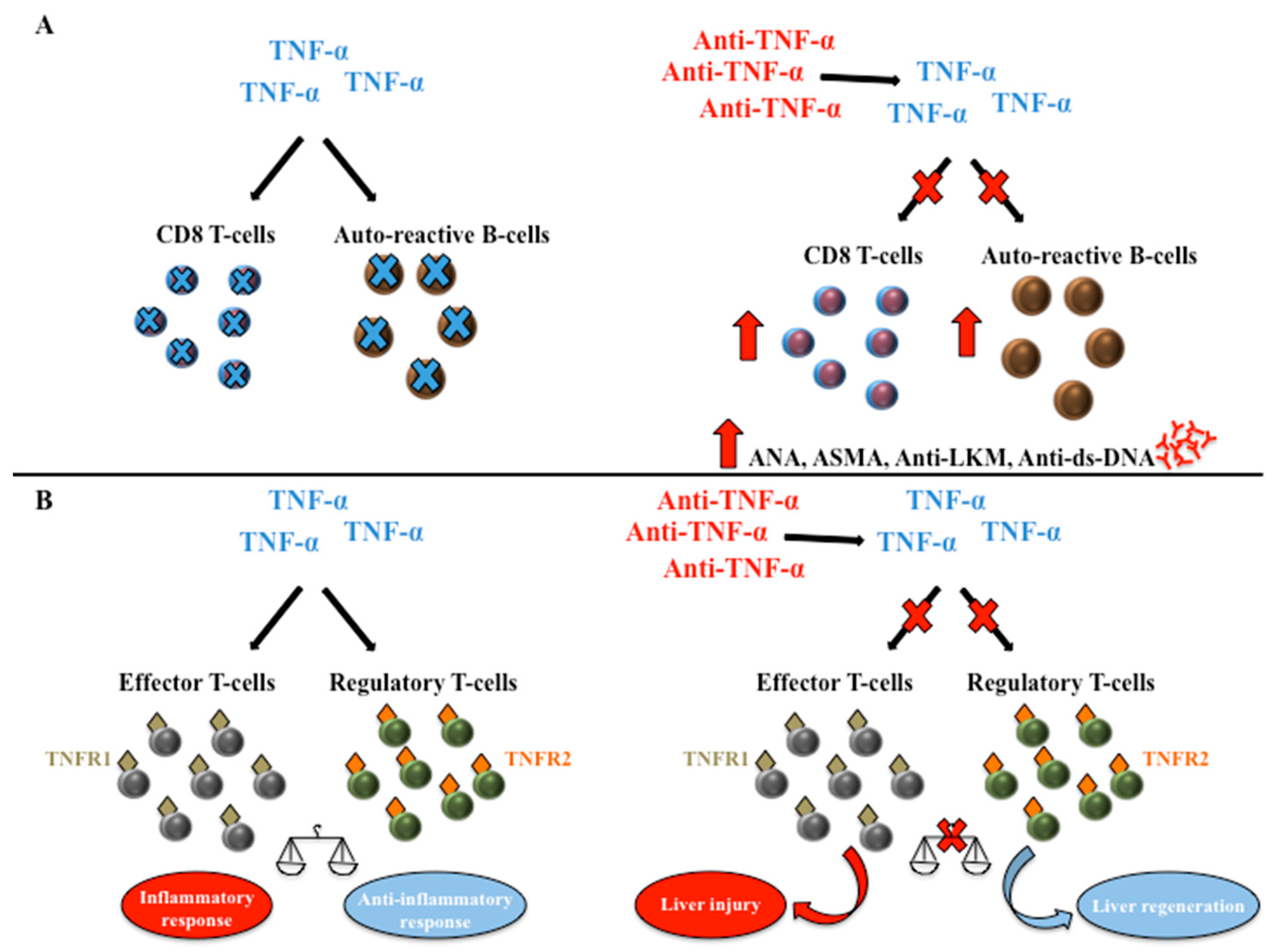
5. Anti-TNF-α Liver Toxicity
6. Potential Beneficial Effects of Anti-TNF-α on Liver Diseases
6.1. Alcoholic Hepatitis (AH)
6.2. Non-Alcoholic Fatty Liver Disease (NAFLD)
6.3. Autoimmune Hepatitis (AIH)
6.4. Primary Biliary Cholangitis (PBC)
7. Conclusions
Acknowledgments
Conflicts of Interest
Abbreviations
| IBD | Inflammatory Bowel Diseases |
| CD | Crohn’s Disease |
| UC | Ulcerative Colitis |
| TNF-α | Tumor Necrosis Factor |
| RA | Rheumatoid Arthritis |
| JIA | Juvenile Idiopathic Arthritis |
| AS | Ankylosing Spondylitis |
| PsA | Psoriatic Arthritis |
| IFX | Infliximab |
| ADA | Adalimumab |
| CER | Certolizumab Pegol |
| ETA | Etanercept |
| GOL | Golimumab |
| Ig | Immunoglobulin |
| HBV | Hepatitis B Virus |
| HCV | Hepatitis C Virus |
| AH | Alcoholic Hepatitis |
| NAFLD | Non-Alcoholic Fatty Liver Disease |
| AIH | Autoimmune Hepatitis |
| PBC | Primary Biliary Cholangitis |
| ECCO | European Crohn’s and Colitis Organization |
| ALT | Alanine Aminotransferase |
| IFN | Interferon |
| LT | Liver Transplantation |
| FDA | Food and Drug Administration |
| MMF | Mycophenolate Mofetil |
| DILI | Drug Induced Liver Injury |
| CRP | C-reactive protein |
| NASH | Non-Alcoholic Steatohepatitis |
| TNFR | TNF Receptor |
References
- Papadakis, K.A.; Targan, S.R. Tumor necrosis factor: Biology and therapeutic inhibitors. Gastroenterology 2000, 119, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- Nesbitt, A.; Fossati, G.; Bergin, M.; Stephens, P.; Stephens, S.; Foulkes, R.; Brown, D.; Robinson, M.; Bourne, T. Mechanism of action of certolizumab pegol (CDP870): In vitro comparison with other anti-tumor necrosis factor alpha agents. Inflamm. Bowel Dis. 2007, 13, 1323–1332. [Google Scholar] [CrossRef] [PubMed]
- Weaver, A.L. Differentiating the new rheumatoid arthritis biologic therapies. J. Clin. Rheumatol. 2003, 9, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Mocci, G.; Bonizzi, M.; Felice, C.; Andrisani, G.; De Vitis, I.; Guidi, L.; Gasbarrini, A. Use of infliximab in particular clinical settings: Management based on current evidence. Am. J. Gastroenterol. 2009, 104, 1575–1586. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.E.; Parisi, I.; Despott, E.J.; Burroughs, A.K.; O’Beirne, J.; Conte, D.; Hamilton, M.I.; Murray, C.D. Anti-tumour necrosis factor agent and liver injury: Literature review, recommendations for management. World J. Gastroenterol. 2014, 20, 17352–17359. [Google Scholar] [CrossRef] [PubMed]
- Ghabril, M.; Bonkovsky, H.L.; Kum, C.; Davern, T.; Hayashi, P.H.; Kleiner, D.E.; Serrano, J.; Rochon, J.; Fontana, R.J.; Bonacini, M.; et al. Liver injury from tumor necrosis factor-alpha antagonists: Analysis of thirty-four cases. Clin. Gastroenterol. Hepatol. 2013, 11, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Cassano, N.; Vestita, M.; Apruzzi, D.; Vena, G.A. Alcohol, psoriasis, liver disease, and anti-psoriasis drugs. Int. J. Dermatol. 2011, 50, 1323–1331. [Google Scholar] [CrossRef] [PubMed]
- Levitsky, J.; Mailliard, M.E. Diagnosis and therapy of alcoholic liver disease. Semin. Liver Dis. 2004, 24, 233–247. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zheng, L.; Sheng, C.; Cheng, X.; Qing, L.; Qu, S. Systematic review on the treatment of pentoxifylline in patients with non-alcoholic fatty liver disease. Lipids Health Dis. 2011, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulou, D.; Dimitroulas, T.; Akriviadis, E.; Garyfallos, A. Infliximab as a treatment option for patients with rheumatoid arthritis and primary biliary cirrhosis. Rheumatol. Int. 2015, 35, 1913–1916. [Google Scholar] [CrossRef] [PubMed]
- Weiler-Normann, C.; Schramm, C.; Quaas, A.; Wiegard, C.; Glaubke, C.; Pannicke, N.; Moller, S.; Lohse, A.W. Infliximab as a rescue treatment in difficult-to-treat autoimmune hepatitis. J. Hepatol. 2013, 58, 529–534. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Easl clinical practice guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar]
- Ellerin, T.; Rubin, R.H.; Weinblatt, M.E. Infections and anti-tumor necrosis factor alpha therapy. Arthritis Rheum. 2003, 48, 3013–3022. [Google Scholar] [CrossRef] [PubMed]
- Schluter, D.; Deckert, M. The divergent role of tumor necrosis factor receptors in infectious diseases. Microbes Infect. 2000, 2, 1285–1292. [Google Scholar] [CrossRef]
- Theis, V.S.; Rhodes, J.M. Review article: Minimizing tuberculosis during anti-tumour necrosis factor-alpha treatment of inflammatory bowel disease. Aliment. Pharm. Ther. 2008, 27, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Rahier, J.F.; Magro, F.; Abreu, C.; Armuzzi, A.; Ben-Horin, S.; Chowers, Y.; Cottone, M.; de Ridder, L.; Doherty, G.; Ehehalt, R.; et al. Second European evidence-based consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel disease. J. Crohn’s Colitis 2014, 8, 443–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanini, S.; Easterbrook, P.J.; Zumla, A.; Ippolito, G. Hepatitis C: Global epidemiology and strategies for control. Clin. Microbiol. Infect. 2016, 22, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Chuang, E.; Del Vecchio, A.; Smolinski, S.; Song, X.Y.; Sarisky, R.T. Biomedicines to reduce inflammation but not viral load in chronic HCV—What’s the sense? Trends Biotechnol. 2004, 22, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Freeman, A.J.; Marinos, G.; Ffrench, R.A.; Lloyd, A.R. Immunopathogenesis of hepatitis C virus infection. Immunol. Cell Biol. 2001, 79, 515–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, J.; Pei, X.; Xu, W.; Wang, C.; Zhang, X.; Wu, J.; Zhao, W. The relationship between tumor necrosis factor-alpha polymorphisms and hepatitis C virus infection: A systematic review and meta-analysis. Ren. Fail. 2011, 33, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.R.; Lim, H.L.; Marousis, C.G.; Fang, J.W.; Davis, G.L.; Shen, L.; Urdea, M.S.; Kolberg, J.A.; Lau, J.Y. Activation of tumor necrosis factor-alpha system in chronic hepatitis C virus infection. Digest. Dis. Sci. 1997, 42, 2487–2494. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, R.; Ishimura, N.; Ishihara, S.; Chowdhury, A.; Morlyama, N.; Nogami, C.; Miyake, T.; Niigaki, M.; Tokuda, A.; Satoh, S.; et al. Intrahepatic expression of pro-inflammatory cytokine mRNAs and interferon efficacy in chronic hepatitis C. Liver 1996, 16, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Zein, N.N.; Etanercept Study Group. Etanercept as an adjuvant to interferon and ribavirin in treatment-naive patients with chronic hepatitis c virus infection: A phase 2 randomized, double-blind, placebo-controlled study. J. Hepatol. 2005, 42, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Brunasso, A.M.; Puntoni, M.; Gulia, A.; Massone, C. Safety of anti-tumour necrosis factor agents in patients with chronic hepatitis c infection: A systematic review. Rheumatology 2011, 50, 1700–1711. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.V.; Blonski, W.; Buchner, A.M.; Reddy, K.R.; Lichtenstein, G.R. The influence of anti-TNF therapy on the course of chronic hepatitis C virus infection in patients with inflammatory bowel disease. Digest. Dis. Sci. 2013, 58, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Loras, C.; Gisbert, J.P.; Saro, M.C.; Piqueras, M.; Sanchez-Montes, C.; Barrio, J.; Ordas, I.; Montserrat, A.; Ferreiro, R.; Zabana, Y.; et al. Impact of surveillance of hepatitis B and hepatitis C in patients with inflammatory bowel disease under anti-TNF therapies: Multicenter prospective observational study (repentina 3). J. Crohn’s Colitis 2014, 8, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.; Caso, F.; Atteno, M.; Giannitti, C.; Spadaro, A.; Ramonda, R.; Vezzu, M.; Del Puente, A.; Morisco, F.; Fiocco, U.; et al. Long-term safety of anti-TNF-alpha in PSA patients with concomitant HCV infection: A retrospective observational multicenter study on 15 patients. Clin. Rheumatol. 2014, 33, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Ballanti, E.; Conigliaro, P.; Chimenti, M.S.; Kroegler, B.; Di Muzio, G.; Guarino, M.D.; Triggianese, P.; Gigliucci, G.; Novelli, L.; Barbato, C.; et al. Use of anti-tumor necrosis factor alpha therapy in patients with concurrent rheumatoid arthritis and hepatitis B or hepatitis C: A retrospective analysis of 32 patients. Drug Dev. Res. 2014, 75, S42–S45. [Google Scholar] [CrossRef] [PubMed]
- Salvi, M.; Macaluso, L.; Luci, C.; Mattozzi, C.; Paolino, G.; Aprea, Y.; Calvieri, S.; Richetta, A.G. Safety and efficacy of anti-tumor necrosis factors alpha in patients with psoriasis and chronic hepatitis C. World J. Clin. Cases 2016, 4, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.M.; Cheng, T.T.; Lin, J.C.; Chen, C.J. Tumor necrosis factor-alpha antagonist therapy for concomitant rheumatoid arthritis and hepatitis C virus infection: A case series study. Clin. Rheumatol. 2015, 34, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- Vauloup, C.; Krzysiek, R.; Greangeot-Keros, L.; Wendling, D.; Goupille, P.; Brault, R.; Brousse, C.; Mariette, X.; Emilie, D. Effects of tumor necrosis factor antagonist treatment on hepatitis C-related immunological abnormalities. Eur. Cytokine Netw. 2006, 17, 290–293. [Google Scholar] [PubMed]
- Schlaak, J.F.; Tully, G.; Lohr, H.F.; Gerken, G.; Meyer zum Buschenfelde, K.H. HBV-specific immune defect in chronic hepatitis B (CHB) is correlated with a dysregulation of pro- and anti-inflammatory cytokines. Clin. Exp. Immunol. 1999, 115, 508–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guidotti, L.G.; Chisari, F.V. Noncytolytic control of viral infections by the innate and adaptive immune response. Annu. Rev. Immunol. 2001, 19, 65–91. [Google Scholar] [CrossRef] [PubMed]
- Herbein, G.; O’Brien, W.A. Tumor necrosis factor (TNF)-α and TNF receptors in viral pathogenesis. Proc. Soc. Exp. Biol. Med. 2000, 223, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Kasahara, S.; Ando, K.; Saito, K.; Sekikawa, K.; Ito, H.; Ishikawa, T.; Ohnishi, H.; Seishima, M.; Kakumu, S.; Moriwaki, H. Lack of tumor necrosis factor alpha induces impaired proliferation of hepatitis B virus-specific cytotoxic T lymphocytes. J. Virol. 2003, 77, 2469–2476. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, H.T.; Tsai, H.F.; Chyuan, I.T.; Liao, H.J.; Chen, C.J.; Chen, P.J.; Hsu, P.N. Tumor necrosis factor-alpha induced by hepatitis B virus core mediating the immune response for hepatitis B viral clearance in mice model. PLoS ONE 2014, 9, e103008. [Google Scholar] [CrossRef] [PubMed]
- Longo, F.; Hebuterne, X.; Tran, A.; Staccini, P.; Hastier, P.; Schneider, S.; Benzaken, S.; Tirtaine, C.; Rampal, P. prevalence of hepatitis C in patients with chronic inflammatory bowel disease in the region of nice and evaluation of risk factors. Gastroenterol. Clin. Biol. 2000, 24, 77–81. [Google Scholar] [PubMed]
- Biancone, L.; Pavia, M.; Del Vecchio Blanco, G.; D’Inca, R.; Castiglione, F.; De Nigris, F.; Doldo, P.; Cosco, F.; Vavassori, P.; Bresci, G.P.; et al. Hepatitis B and C virus infection in crohn’s disease. Inflamm. Bowel Dis. 2001, 7, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Chevaux, J.B.; Nani, A.; Oussalah, A.; Venard, V.; Bensenane, M.; Belle, A.; Gueant, J.L.; Bigard, M.A.; Bronowicki, J.P.; Peyrin-Biroulet, L. Prevalence of hepatitis B and C and risk factors for nonvaccination in inflammatory bowel disease patients in northeast france. Inflamm. Bowel Dis. 2010, 16, 916–924. [Google Scholar] [CrossRef] [PubMed]
- Loras, C.; Saro, C.; Gonzalez-Huix, F.; Minguez, M.; Merino, O.; Gisbert, J.P.; Barrio, J.; Bernal, A.; Gutierrez, A.; Piqueras, M.; et al. Prevalence and factors related to hepatitis B and C in inflammatory bowel disease patients in Spain: A nationwide, multicenter study. Am. J. Gastroenterol. 2009, 104, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Felice, C.; Marzo, M.; Andrisani, G.; Armuzzi, A.; Covino, M.; Mocci, G.; Pugliese, D.; De Vitis, I.; Gasbarrini, A.; et al. Prevalence and natural history of hepatitis B and C infections in a large population of IBD patients treated with anti-tumor necrosis factor-alpha agents. J. Crohn’s Colitis 2013, 7, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Lalazar, G.; Rund, D.; Shouval, D. Screening, prevention and treatment of viral hepatitis B reactivation in patients with haematological malignancies. Br. J. Haematol. 2007, 136, 699–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeo, W.; Johnson, P.J. Diagnosis, prevention and management of hepatitis B virus reactivation during anticancer therapy. Hepatology 2006, 43, 209–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raimondo, G.; Pollicino, T.; Cacciola, I.; Squadrito, G. Occult hepatitis B virus infection. J. Hepatol. 2007, 46, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Perez-Alvarez, R.; Diaz-Lagares, C.; Garcia-Hernandez, F.; Lopez-Roses, L.; Brito-Zeron, P.; Perez-de-Lis, M.; Retamozo, S.; Bove, A.; Bosch, X.; Sanchez-Tapias, J.M.; et al. Hepatitis B virus (HBV) reactivation in patients receiving tumor necrosis factor (TNF)-targeted therapy: Analysis of 257 cases. Medicine 2011, 90, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G. Prophylaxis with lamivudine of hepatitis B virus reactivation in chronic HbsAg carriers with hemato-oncological neoplasias treated with chemotherapy. Leuk. Lymphoma 2003, 44, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.C.; Wu, M.J.; Cheng, C.H.; Chen, C.H.; Shu, K.H.; Lian, J.D. Lamivudine is effective for the treatment of reactivation of hepatitis B virus and fulminant hepatic failure in renal transplant recipients. Am. J. Kidney Dis. 2001, 38, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wang, B.; Yu, L.; Liu, C.; Wu, Z.; Pan, C.E. Lamivudine in prevention and treatment of recurrent HBV after liver transplantation. Hepatobiliary Pancreat. Dis. Int. 2004, 3, 504–507. [Google Scholar] [PubMed]
- Liu, C.J.; Lai, M.Y.; Lee, P.H.; Chou, N.K.; Chu, S.H.; Chen, P.J.; Kao, J.H.; Jen, Y.M.; Chen, D.S. Lamivudine treatment for hepatitis B reactivation in HbsAg carriers after organ transplantation: A 4-year experience. J. Gastroenterol. Hepatol. 2001, 16, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Navarro, R.; Concha-Garzon, M.J.; Castano, C.; Casal, C.; Guiu, A.; Dauden, E. Outcome of patients with serology suggestive of past hepatitis B virus infection during antitumor necrosis factor therapy for psoriasis. Int. J. Dermatol. 2014, 53, 909–911. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Notarnicola, A.; Lopalco, G.; Viggiani, M.T.; Sebastiani, F.; Covelli, M.; Iannone, F.; Avolio, A.W.; Di Leo, A.; Cantarini, L.; et al. Safety of long-term biologic therapy in rheumatologic patients with a previously resolved hepatitis B viral infection. Hepatology 2015, 62, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vigano, M.; Degasperi, E.; Aghemo, A.; Lampertico, P.; Colombo, M. Anti-TNF drugs in patients with hepatitis B or C virus infection: Safety and clinical management. Expert Opin. Biol. Ther. 2012, 12, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.S.; McMahon, B.J. Chronic hepatitis B: Update 2009. Hepatology 2009, 50, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.; Angelucci, E.; Andreone, P.; Brunetto, M.; Bruno, R.; Burra, P.; Caraceni, P.; Daniele, B.; Di Marco, V.; Fabrizi, F.; et al. Prophylaxis and treatment of hepatitis B in immunocompromised patients. Digest. Liver Dis. 2007, 39, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Liang, R. How I treat and monitor viral hepatitis B infection in patients receiving intensive immunosuppressive therapies or undergoing hematopoietic stem cell transplantation. Blood 2009, 113, 3147–3153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL clinical practice guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar]
- Sands, B.E.; Cuffari, C.; Katz, J.; Kugathasan, S.; Onken, J.; Vitek, C.; Orenstein, W. Guidelines for immunizations in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2004, 10, 677–692. [Google Scholar] [CrossRef] [PubMed]
- Melmed, G.Y.; Ippoliti, A.F.; Papadakis, K.A.; Tran, T.T.; Birt, J.L.; Lee, S.K.; Frenck, R.W.; Targan, S.R.; Vasiliauskas, E.A. Patients with inflammatory bowel disease are at risk for vaccine-preventable illnesses. Am. J. Gastroenterol. 2006, 101, 1834–1840. [Google Scholar] [CrossRef] [PubMed]
- Vida Perez, L.; Gomez Camacho, F.; Garcia Sanchez, V.; Iglesias Flores, E.M.; Castillo Molina, L.; Cerezo Ruiz, A.; Casais Juanena, L.; De Dios Vega, J.F. Adequate rate of response to hepatitis B virus vaccination in patients with inflammatory bowel disease. Med. Clin. 2009, 132, 331–335. [Google Scholar]
- Gisbert, J.P.; Villagrasa, J.R.; Rodriguez-Nogueiras, A.; Chaparro, M. Efficacy of hepatitis B vaccination and revaccination and factors impacting on response in patients with inflammatory bowel disease. Am. J. Gastroenterol. 2012, 107, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Filipec Kanizaj, T.; Mijic, M. Inflammatory bowel disease in liver transplanted patients. World J. Gastroenterol. 2017, 23, 3214–3227. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, A.; Alameel, T.; Dale, C.H.; Levstik, M.; Chande, N. The safety and efficacy of antitumour necrosis factor-alpha therapy for inflammatory bowel disease in patients post liver transplantation: A case series. Aliment. Pharmacol. Ther. 2012, 36, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Mohabbat, A.B.; Sandborn, W.J.; Loftus, E.V., Jr.; Wiesner, R.H.; Bruining, D.H. Anti-tumour necrosis factor treatment of inflammatory bowel disease in liver transplant recipients. Aliment. Pharmacol. Ther. 2012, 36, 569–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westerouen van Meeteren, M.J.; Hayee, B.; Inderson, A.; van der Meulen, A.E.; Altwegg, R.; van Hoek, B.; Pageaux, G.P.; Stijnen, T.; Stein, D.; Maljaars, P.W.J. Safety of anti-TNF treatment in liver transplant recipients: A systematic review and meta-analysis. J. Crohn’s Colitis 2017, 11, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- DeFilippis, E.M.; Kumar, S. Clinical presentation and outcomes of autoimmune hepatitis in inflammatory bowel disease. Digest. Dis. Sci. 2015, 60, 2873–2880. [Google Scholar] [CrossRef] [PubMed]
- FDA. Briefing Document. Safety Alerts for Drugs, Biologics Medical Devices, and Dietary Supplements. Remicade (Infliximab). 2004. Available online: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=103772 (accessed on 3 June 2018).
- Mancini, S.; Amorotti, E.; Vecchio, S.; Ponz de Leon, M.; Roncucci, L. Infliximab-related hepatitis: Discussion of a case and review of the literature. Intern. Emerg. Med. 2010, 5, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Tobon, G.J.; Canas, C.; Jaller, J.J.; Restrepo, J.C.; Anaya, J.M. Serious liver disease induced by infliximab. Clin. Rheumatol. 2007, 26, 578–581. [Google Scholar] [CrossRef] [PubMed]
- Ierardi, E.; Valle, N.D.; Nacchiero, M.C.; De Francesco, V.; Stoppino, G.; Panella, C. Onset of liver damage after a single administration of infliximab in a patient with refractory ulcerative colitis. Clin. Drug Investig. 2006, 26, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, K.M.; Riis, L.; Madsen, O.R. Toxic hepatitis induced by infliximab in a patient with rheumatoid arthritis with no relapse after switching to etanercept. Clin. Rheumatol. 2009, 28, 1001–1003. [Google Scholar] [CrossRef] [PubMed]
- Haennig, A.; Bonnet, D.; Thebault, S.; Alric, L. Infliximab-induced acute hepatitis during Crohn’s disease therapy: Absence of cross-toxicity with adalimumab. Gastroenterol. Clin. Biol. 2010, 34, e7–e8. [Google Scholar] [CrossRef] [PubMed]
- Germano, V.; Picchianti Diamanti, A.; Baccano, G.; Natale, E.; Onetti Muda, A.; Priori, R.; Valesini, G. Autoimmune hepatitis associated with infliximab in a patient with psoriatic arthritis. Ann. Rheum. Dis. 2005, 64, 1519–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozorio, G.; McGarity, B.; Bak, H.; Jordan, A.S.; Lau, H.; Marshall, C. Autoimmune hepatitis following infliximab therapy for ankylosing spondylitis. Med. J. Aust. 2007, 187, 524–526. [Google Scholar] [PubMed]
- Doyle, A.; Forbes, G.; Kontorinis, N. Autoimmune hepatitis during infliximab therapy for Crohn’s disease: A case report. J. Crohn’s Colitis 2011, 5, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, K.; Chitturi, S.; Brown, M.; Pavli, P. Infliximab-induced autoimmune hepatitis in Crohn’s disease treated with budesonide and mycophenolate. Inflamm. Bowel Dis. 2011, 17, E149–E150. [Google Scholar] [CrossRef] [PubMed]
- Adar, T.; Mizrahi, M.; Pappo, O.; Scheiman-Elazary, A.; Shibolet, O. Adalimumab-induced autoimmune hepatitis. J. Clin. Gastroenterol. 2010, 44, e20–e22. [Google Scholar] [CrossRef] [PubMed]
- Coffin, C.S.; Fraser, H.F.; Panaccione, R.; Ghosh, S. Liver diseases associated with anti-tumor necrosis factor-alpha (TNF-α) use for inflammatory bowel disease. Inflamm. Bowel Dis. 2011, 17, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Cravo, M.; Silva, R.; Serrano, M. Autoimmune hepatitis induced by infliximab in a patient with Crohn’s disease with no relapse after switching to adalimumab. BioDrugs 2010, 24, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Goldfeld, D.A.; Verna, E.C.; Lefkowitch, J.; Swaminath, A. Infliximab-induced autoimmune hepatitis with successful switch to adalimumab in a patient with Crohn’s disease: The index case. Digest. Dis. Sci. 2011, 56, 3386–3388. [Google Scholar] [CrossRef] [PubMed]
- Borman, M.A.; Urbanski, S.; Swain, M.G. Anti-TNF-induced autoimmune hepatitis. J. Hepatol. 2014, 61, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Bjornsson, E.S.; Gunnarsson, B.I.; Grondal, G.; Jonasson, J.G.; Einarsdottir, R.; Ludviksson, B.R.; Gudbjornsson, B.; Olafsson, S. Risk of drug-induced liver injury from tumor necrosis factor antagonists. Clin. Gastroenterol. Hepatol. 2015, 13, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Bjornsson, E.S.; Bergmann, O.M.; Bjornsson, H.K.; Kvaran, R.B.; Olafsson, S. Incidence, presentation, and outcomes in patients with drug-induced liver injury in the general population of Iceland. Gastroenterology 2013, 144, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Bjornsson, E.S. Hepatotoxicity by drugs: The most common implicated agents. Int. J. Mol. Sci. 2016, 17, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksson, C.; Engstrand, S.; Sundqvist, K.G.; Rantapaa-Dahlqvist, S. Autoantibody formation in patients with rheumatoid arthritis treated with anti-TNF alpha. Ann. Rheum. Dis. 2005, 64, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Marques, M.; Magro, F.; Cardoso, H.; Carneiro, F.; Portugal, R.; Lopes, J.; Costa Santos, C. Infliximab-induced lupus-like syndrome associated with autoimmune hepatitis. Inflamm. Bowel. Dis. 2008, 14, 723–725. [Google Scholar] [CrossRef] [PubMed]
- Diehl, A.M. Cytokine regulation of liver injury and repair. Immunol. Rev. 2000, 174, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Oppenheim, J.J. Contrasting effects of TNF and anti-TNF on the activation of effector t cells and regulatory t cells in autoimmunity. FEBS Lett. 2011, 585, 3611–3618. [Google Scholar] [CrossRef] [PubMed]
- Menghini, V.V.; Arora, A.S. Infliximab-associated reversible cholestatic liver disease. Mayo Clin. Proc. 2001, 76, 84–86. [Google Scholar] [CrossRef] [PubMed]
- Kinnunen, U.; Farkkila, M.; Makisalo, H. A case report: Ulcerative colitis, treatment with an antibody against tumor necrosis factor (infliximab), and subsequent liver necrosis. J. Crohn’s Colitis 2012, 6, 724–727. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Cummings, O.W.; Hartley, M.P.; Filomena, C.A.; Cho, W.K. Hepatocellular carcinoma occurring in a patient with Crohn’s disease treated with both azathioprine and infliximab. Digest. Dis. Sci. 2006, 51, 952–955. [Google Scholar] [CrossRef] [PubMed]
- Fathalla, B.M.; Goldsmith, D.P.; Pascasio, J.M.; Baldridge, A. Development of autoimmune hepatitis in a child with systemic-onset juvenile idiopathic arthritis during therapy with etanercept. J. Clin. Rheumatol. 2008, 14, 297–298. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.; Akai, Y.; Koyama, S.; Ikenaka, Y.; Saito, Y. A case of autoimmune hepatitis exacerbated by the administration of etanercept in the patient with rheumatoid arthritis. Clin. Rheumatol. 2008, 27, 1063–1066. [Google Scholar] [CrossRef] [PubMed]
- Parekh, R.; Kaur, N. Liver injury secondary to anti-TNF-α therapy in inflammatory bowel disease: A case series and review of the literature. Case Rep. Gastrointest. Med. 2014, 2014, 956463. [Google Scholar] [CrossRef] [PubMed]
- Shelton, E.; Chaudrey, K.; Sauk, J.; Khalili, H.; Masia, R.; Nguyen, D.D.; Yajnik, V.; Ananthakrishnan, A.N. New onset idiosyncratic liver enzyme elevations with biological therapy in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2015, 41, 972–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, J.B.; Bonacini, M.; Ghabril, M.; Foureau, D.; Bonkovsky, H.L. Hepatotoxicity associated with the use of anti-TNF-alpha agents. Drug Saf. 2016, 39, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.; Lopes, S.; Magro, F.; Cardoso, H.; Horta e Vale, A.M.; Marques, M.; Mariz, E.; Bernardes, M.; Lopes, J.; Carneiro, F.; et al. Autoimmune hepatitis and anti-tumor necrosis factor alpha therapy: A single center report of 8 cases. World J. Gastroenterol. 2015, 21, 7584–7588. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.M.; Ahn, J. Review article: The diagnosis and management of alcoholic hepatitis. Aliment. Pharmacol. Ther. 2009, 30, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Hardison, W.G.; Lee, F.I. Prognosis in acute liver disease of the alcoholic patient. N. Engl. J. Med. 1966, 275, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Tilg, H.; Diehl, A.M. Cytokines in alcoholic and nonalcoholic steatohepatitis. N. Engl. J. Med. 2000, 343, 1467–1476. [Google Scholar] [CrossRef] [PubMed]
- McClain, C.J.; Barve, S.; Deaciuc, I.; Kugelmas, M.; Hill, D. Cytokines in alcoholic liver disease. Semin. Liver Dis. 1999, 19, 205–219. [Google Scholar] [CrossRef] [PubMed]
- McClain, C.J.; Song, Z.; Barve, S.S.; Hill, D.B.; Deaciuc, I. Recent advances in alcoholic liver disease. Iv. Dysregulated cytokine metabolism in alcoholic liver disease. Am. J. Physiol. Gastrointest. Liver Physiol. 2004, 287, G497–G502. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Talavera, J.C.; Merrill, W.W.; Groszmann, R.J. Tumor necrosis factor alpha: A major contributor to the hyperdynamic circulation in prehepatic portal-hypertensive rats. Gastroenterology 1995, 108, 761–767. [Google Scholar] [CrossRef]
- Yin, M.; Wheeler, M.D.; Kono, H.; Bradford, B.U.; Gallucci, R.M.; Luster, M.I.; Thurman, R.G. Essential role of tumor necrosis factor alpha in alcohol-induced liver injury in mice. Gastroenterology 1999, 117, 942–952. [Google Scholar] [CrossRef]
- Iimuro, Y.; Gallucci, R.M.; Luster, M.I.; Kono, H.; Thurman, R.G. Antibodies to tumor necrosis factor alfa attenuate hepatic necrosis and inflammation caused by chronic exposure to ethanol in the rat. Hepatology 1997, 26, 1530–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McClain, C.J.; Cohen, D.A. Increased tumor necrosis factor production by monocytes in alcoholic hepatitis. Hepatology 1989, 9, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Khoruts, A.; Stahnke, L.; McClain, C.J.; Logan, G.; Allen, J.I. Circulating tumor necrosis factor, interleukin-1 and interleukin-6 concentrations in chronic alcoholic patients. Hepatology 1991, 13, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Barve, A.; Khan, R.; Marsano, L.; Ravindra, K.V.; McClain, C. Treatment of alcoholic liver disease. Ann. Hepatol. 2008, 7, 5–15. [Google Scholar] [PubMed]
- Menachery, J.; Duseja, A. Treatment of decompensated alcoholic liver disease. Int. J. Hepatol. 2011, 2011, 219238. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, M.A.; Cabre, E.; Lorenzo-Zuniga, V.; Montoliu, S.; Planas, R.; Gassull, M.A. Combining steroids with enteral nutrition: A better therapeutic strategy for severe alcoholic hepatitis? Results of a pilot study. Eur. J. Gastroenterol. Hepatol. 2004, 16, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- Mathurin, P.; Mendenhall, C.L.; Carithers, R.L., Jr.; Ramond, M.J.; Maddrey, W.C.; Garstide, P.; Rueff, B.; Naveau, S.; Chaput, J.C.; Poynard, T. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis (AH): Individual data analysis of the last three randomized placebo controlled double blind trials of corticosteroids in severe ah. J. Hepatol. 2002, 36, 480–487. [Google Scholar] [CrossRef]
- McCullough, A.J.; O’Connor, J.F. Alcoholic liver disease: Proposed recommendations for the American college of gastroenterology. Am. J. Gastroenterol. 1998, 93, 2022–2036. [Google Scholar] [CrossRef] [PubMed]
- Mathurin, P.; O’Grady, J.; Carithers, R.L.; Phillips, M.; Louvet, A.; Mendenhall, C.L.; Ramond, M.J.; Naveau, S.; Maddrey, W.C.; Morgan, T.R. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis: Meta-analysis of individual patient data. Gut 2011, 60, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Taieb, J.; Mathurin, P.; Elbim, C.; Cluzel, P.; Arce-Vicioso, M.; Bernard, B.; Opolon, P.; Gougerot-Pocidalo, M.A.; Poynard, T.; Chollet-Martin, S. Blood neutrophil functions and cytokine release in severe alcoholic hepatitis: Effect of corticosteroids. J. Hepatol. 2000, 32, 579–586. [Google Scholar] [CrossRef]
- Mathurin, P.; Duchatelle, V.; Ramond, M.J.; Degott, C.; Bedossa, P.; Erlinger, S.; Benhamou, J.P.; Chaput, J.C.; Rueff, B.; Poynard, T. Survival and prognostic factors in patients with severe alcoholic hepatitis treated with prednisolone. Gastroenterology 1996, 110, 1847–1853. [Google Scholar] [CrossRef] [PubMed]
- Spahr, L.; Rubbia-Brandt, L.; Frossard, J.L.; Giostra, E.; Rougemont, A.L.; Pugin, J.; Fischer, M.; Egger, H.; Hadengue, A. Combination of steroids with infliximab or placebo in severe alcoholic hepatitis: A randomized controlled pilot study. J. Hepatol. 2002, 37, 448–455. [Google Scholar] [CrossRef]
- Naveau, S.; Chollet-Martin, S.; Dharancy, S.; Mathurin, P.; Jouet, P.; Piquet, M.A.; Davion, T.; Oberti, F.; Broet, P.; Emilie, D.; et al. A double-blind randomized controlled trial of infliximab associated with prednisolone in acute alcoholic hepatitis. Hepatology 2004, 39, 1390–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tilg, H.; Jalan, R.; Kaser, A.; Davies, N.A.; Offner, F.A.; Hodges, S.J.; Ludwiczek, O.; Shawcross, D.; Zoller, H.; Alisa, A.; et al. Anti-tumor necrosis factor-alpha monoclonal antibody therapy in severe alcoholic hepatitis. J. Hepatol. 2003, 38, 419–425. [Google Scholar] [CrossRef]
- Mookerjee, R.P.; Sen, S.; Davies, N.A.; Hodges, S.J.; Williams, R.; Jalan, R. Tumour necrosis factor alpha is an important mediator of portal and systemic haemodynamic derangements in alcoholic hepatitis. Gut 2003, 52, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Kumar, A.; Sharma, B.C.; Sarin, S.K. Infliximab monotherapy for severe alcoholic hepatitis and predictors of survival: An open label trial. J. Hepatol. 2009, 50, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Boetticher, N.C.; Peine, C.J.; Kwo, P.; Abrams, G.A.; Patel, T.; Aqel, B.; Boardman, L.; Gores, G.J.; Harmsen, W.S.; McClain, C.J.; et al. A randomized, double-blinded, placebo-controlled multicenter trial of etanercept in the treatment of alcoholic hepatitis. Gastroenterology 2008, 135, 1953–1960. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, N.; Younossi, Z.M. Nonalcoholic fatty liver disease: A practical approach to evaluation and management. Clin. Liver Dis. 2009, 13, 249–266. [Google Scholar] [CrossRef] [PubMed]
- Browning, J.D.; Horton, J.D. Molecular mediators of hepatic steatosis and liver injury. J. Clin. Investig. 2004, 114, 147–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Browning, J.D.; Szczepaniak, L.S.; Dobbins, R.; Nuremberg, P.; Horton, J.D.; Cohen, J.C.; Grundy, S.M.; Hobbs, H.H. Prevalence of hepatic steatosis in an urban population in the united states: Impact of ethnicity. Hepatology 2004, 40, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Williams, R. Global challenges in liver disease. Hepatology 2006, 44, 521–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falck-Ytter, Y.; Younossi, Z.M.; Marchesini, G.; McCullough, A.J. Clinical features and natural history of nonalcoholic steatosis syndromes. Semin. Liver Dis. 2001, 21, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Perseghin, G.; Petersen, K.; Shulman, G.I. Cellular mechanism of insulin resistance: Potential links with inflammation. Int. J. Obes. Relat. Metab. Disord. 2003, 27, S6–S11. [Google Scholar] [CrossRef] [PubMed]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Investig. 2006, 116, 1793–1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diehl, A.M.; Li, Z.P.; Lin, H.Z.; Yang, S.Q. Cytokines and the pathogenesis of non-alcoholic steatohepatitis. Gut 2005, 54, 303–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomita, K.; Tamiya, G.; Ando, S.; Ohsumi, K.; Chiyo, T.; Mizutani, A.; Kitamura, N.; Toda, K.; Kaneko, T.; Horie, Y.; et al. Tumour necrosis factor alpha signalling through activation of Kupffer cells plays an essential role in liver fibrosis of non-alcoholic steatohepatitis in mice. Gut 2006, 55, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Cai, D.; Yuan, M.; Frantz, D.F.; Melendez, P.A.; Hansen, L.; Lee, J.; Shoelson, S.E. Local and systemic insulin resistance resulting from hepatic activation of IKK-β and NF-κ. Nat. Med. 2005, 11, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Koca, S.S.; Bahcecioglu, I.H.; Poyrazoglu, O.K.; Ozercan, I.H.; Sahin, K.; Ustundag, B. The treatment with antibody of TNF-α reduces the inflammation, necrosis and fibrosis in the non-alcoholic steatohepatitis induced by methionine- and choline-deficient diet. Inflammation 2008, 31, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Barbuio, R.; Milanski, M.; Bertolo, M.B.; Saad, M.J.; Velloso, L.A. Infliximab reverses steatosis and improves insulin signal transduction in liver of rats fed a high-fat diet. J. Endocrinol. 2007, 194, 539–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schramm, C.; Schneider, A.; Marx, A.; Lohse, A.W. Adalimumab could suppress the activity of non alcoholic steatohepatitis (NASH). Z. Gastroenterol. 2008, 46, 1369–1371. [Google Scholar] [CrossRef] [PubMed]
- Schramm, C.; Weiler-Normann, C.; Wiegard, C.; Hellweg, S.; Muller, S.; Lohse, A.W. Treatment response in patients with autoimmune hepatitis. Hepatology 2010, 52, 2247–2248. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manns, M.P.; Woynarowski, M.; Kreisel, W.; Lurie, Y.; Rust, C.; Zuckerman, E.; Bahr, M.J.; Gunther, R.; Hultcrantz, R.W.; Spengler, U.; et al. Budesonide induces remission more effectively than prednisone in a controlled trial of patients with autoimmune hepatitis. Gastroenterology 2010, 139, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Hennes, E.M.; Oo, Y.H.; Schramm, C.; Denzer, U.; Buggisch, P.; Wiegard, C.; Kanzler, S.; Schuchmann, M.; Boecher, W.; Galle, P.R.; et al. Mycophenolate mofetil as second line therapy in autoimmune hepatitis? Am. J. Gastroenterol. 2008, 103, 3063–3070. [Google Scholar] [CrossRef] [PubMed]
- De Boer, N.K.; van Nieuwkerk, C.M.; Aparicio Pages, M.N.; de Boer, S.Y.; Derijks, L.J.; Mulder, C.J. Promising treatment of autoimmune hepatitis with 6-thioguanine after adverse events on azathioprine. Eur. J. Gastroenterol. Hepatol. 2005, 17, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Kanzler, S.; Gerken, G.; Dienes, H.P.; Meyer zum Buschenfelde, K.H.; Lohse, A.W. Cyclophosphamide as alternative immunosuppressive therapy for autoimmune hepatitis—Report of three cases. Z. Gastroenterol. 1997, 35, 571–578. [Google Scholar] [PubMed]
- Malekzadeh, R.; Nasseri-Moghaddam, S.; Kaviani, M.J.; Taheri, H.; Kamalian, N.; Sotoudeh, M. Cyclosporin a is a promising alternative to corticosteroids in autoimmune hepatitis. Dig. Dis. Sci. 2001, 46, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Larsen, F.S.; Vainer, B.; Eefsen, M.; Bjerring, P.N.; Adel Hansen, B. Low-dose tacrolimus ameliorates liver inflammation and fibrosis in steroid refractory autoimmune hepatitis. World J. Gastroenterol. 2007, 13, 3232–3236. [Google Scholar] [CrossRef] [PubMed]
- Rajanayagam, J.; Lewindon, P.J. Infliximab as rescue therapy in paediatric autoimmune hepatitis. J. Hepatol. 2013, 59, 908–909. [Google Scholar] [CrossRef] [PubMed]
- Akberova, D.; Kiassov, A.P.; Abdulganieva, D. Serum cytokine levels and their relation to clinical features in patients with autoimmune liver diseases. J. Immunol. Res. 2017, 2017, 9829436. [Google Scholar] [CrossRef] [PubMed]
- Diamantis, I.; Boumpas, D.T. Autoimmune hepatitis: Evolving concepts. Autoimmun. Rev. 2004, 3, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Jalan, R.; Fernandez, J.; Wiest, R.; Schnabl, B.; Moreau, R.; Angeli, P.; Stadlbauer, V.; Gustot, T.; Bernardi, M.; Canton, R.; et al. Bacterial infections in cirrhosis: A position statement based on the EASL special conference 2013. J. Hepatol. 2014, 60, 1310–1324. [Google Scholar] [CrossRef] [PubMed]
- Spadaro, A.; Scrivo, R.; Riccieri, V.; Valesini, G. Effect of tumor necrosis factor alpha antagonists in a patient with rheumatoid arthritis and primary biliary cirrhosis. Joint Bone Spine 2008, 75, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Ogata, A.; Terabe, F.; Nakanishi, K.; Kawai, M.; Kuwahara, Y.; Hirano, T.; Arimitsu, J.; Hagihara, K.; Shima, Y.; Narazaki, M.; et al. Etanercept improved primary biliary cirrhosis associated with rheumatoid arthritis. Joint Bone Spine 2009, 76, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Del Ross, T.; Ruffatti, A.; Floreani, A.; Hoxha, A.; Punzi, L. The efficacy of adalimumab in psoriatic arthritis concomitant to overlapping primary biliary cholangitis and primary sclerosing cholangitis: A case report. BMC Musculoskelet. Disord. 2016, 17, 485. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Harmful Effects of Anti-TNF-α Agents | Potential Beneficial Effects of Anti TNF-α Agents |
|---|---|
Reactivation of HBV infection
|
|
Hepatotoxicity
|
|
| |
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopetuso, L.R.; Mocci, G.; Marzo, M.; D’Aversa, F.; Rapaccini, G.L.; Guidi, L.; Armuzzi, A.; Gasbarrini, A.; Papa, A. Harmful Effects and Potential Benefits of Anti-Tumor Necrosis Factor (TNF)-α on the Liver. Int. J. Mol. Sci. 2018, 19, 2199. https://doi.org/10.3390/ijms19082199
Lopetuso LR, Mocci G, Marzo M, D’Aversa F, Rapaccini GL, Guidi L, Armuzzi A, Gasbarrini A, Papa A. Harmful Effects and Potential Benefits of Anti-Tumor Necrosis Factor (TNF)-α on the Liver. International Journal of Molecular Sciences. 2018; 19(8):2199. https://doi.org/10.3390/ijms19082199
Chicago/Turabian StyleLopetuso, Loris Riccardo, Giammarco Mocci, Manuela Marzo, Francesca D’Aversa, Gian Lodovico Rapaccini, Luisa Guidi, Alessandro Armuzzi, Antonio Gasbarrini, and Alfredo Papa. 2018. "Harmful Effects and Potential Benefits of Anti-Tumor Necrosis Factor (TNF)-α on the Liver" International Journal of Molecular Sciences 19, no. 8: 2199. https://doi.org/10.3390/ijms19082199