
Differential Amino Acid, Carbohydrate and Lipid Metabolism Perpetuations Involved in a Subtype of Rheumatoid Arthritis with Chinese Medicine Cold Pattern

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Differential Metabolites and Canonical Pathways Involved in Rheumatoid Arthritis (RA) Cold and Heat Patterns
2.2. Comparison Analysis between Cold and Heat Patterns in Amino Acids Metabolism
2.3. Comparison Analysis between Cold and Heat Patterns in Carbohydrates Metabolism
2.4. Comparison Analysis between Cold and Heat Patterns in Lipid Metabolism
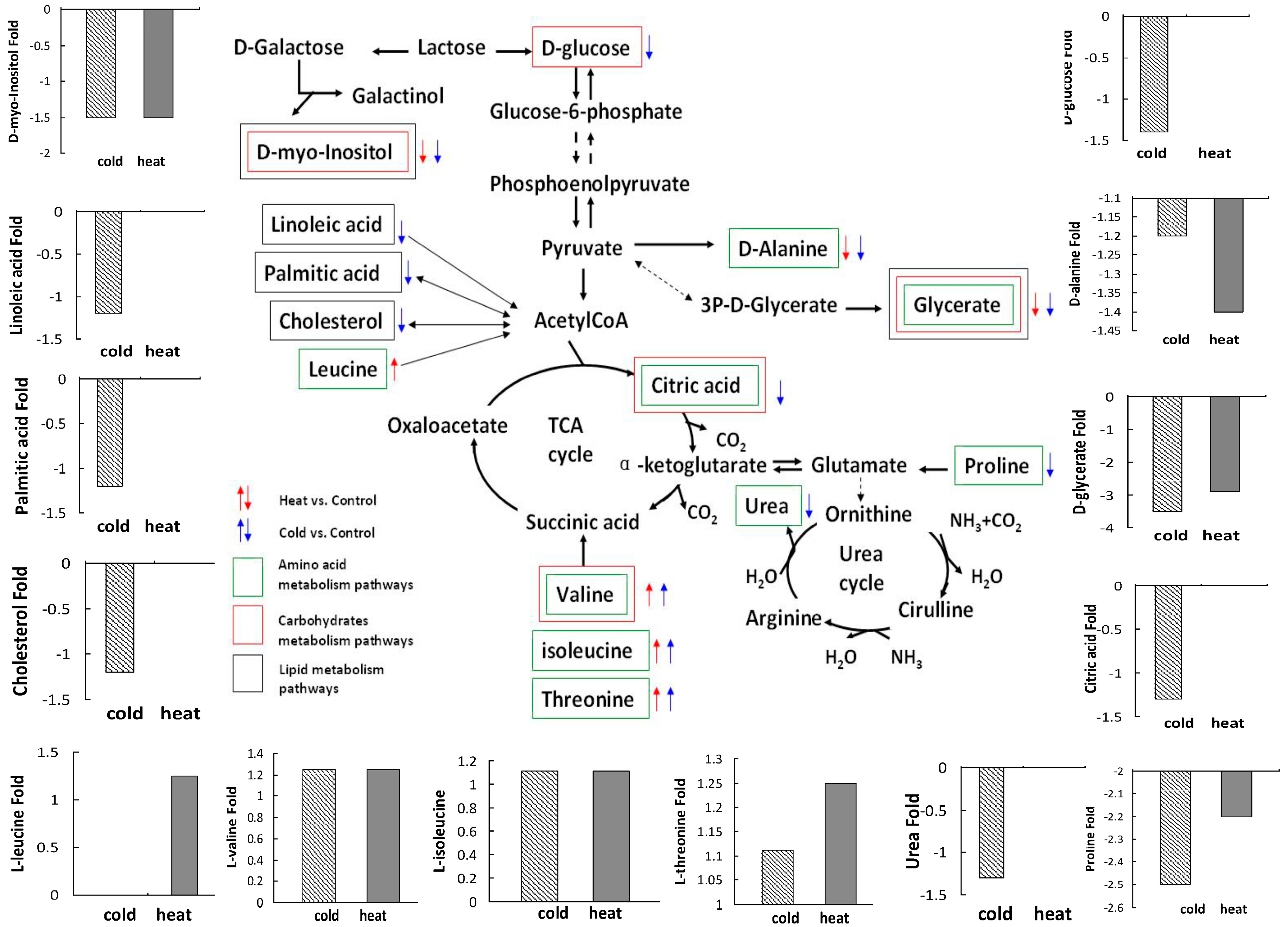
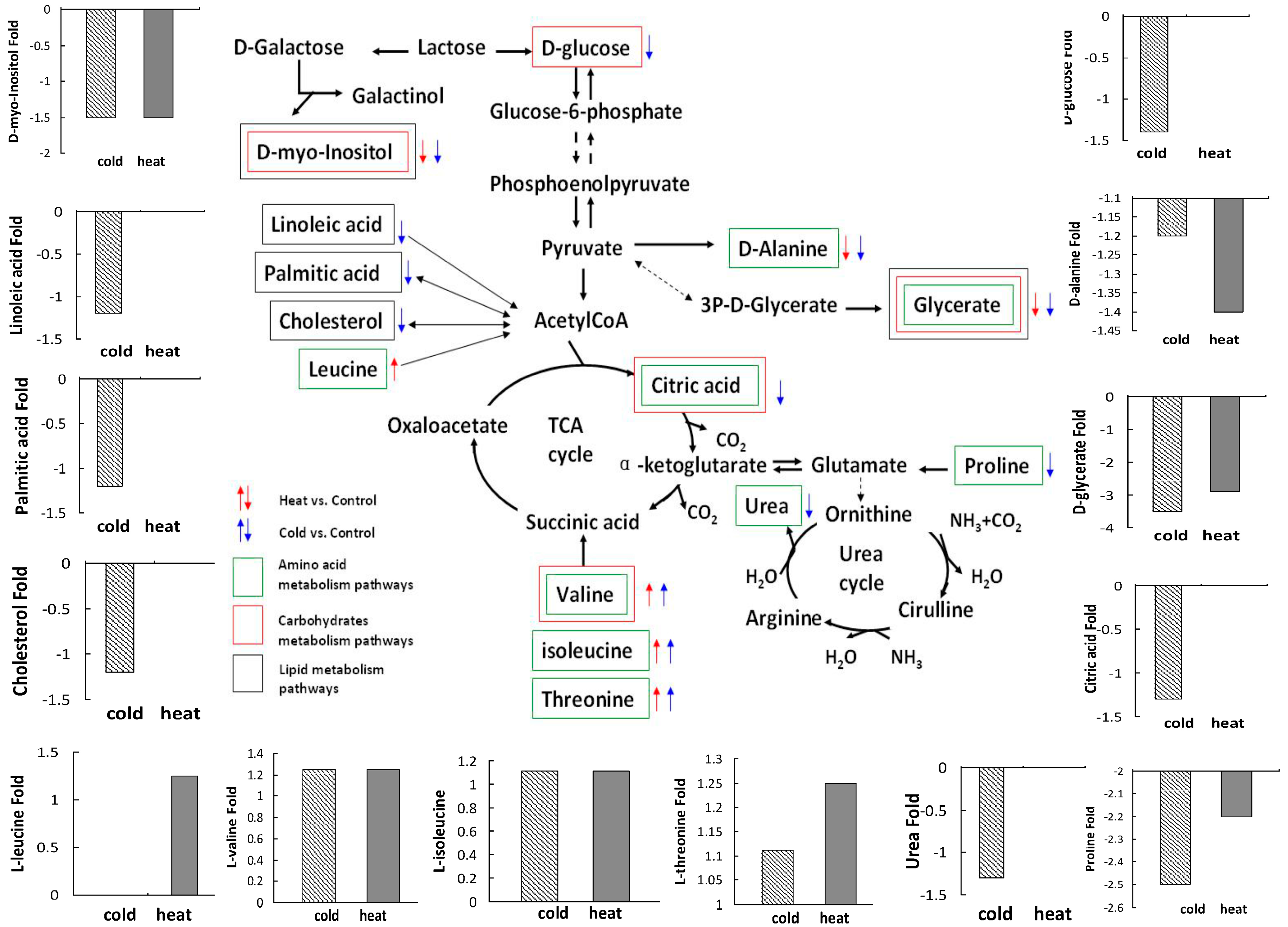
2.5. Integrative Analysis in Amino Acids, Carbohydrates and Lipid Metabolism between Cold and Heat Patterns
3. Discussion
4. Materials and Methods
4.1. Chemicals
4.2. Patients and Sample Preparation
4.3. LC/MS and GC/MS Analysis
4.4. Data Analysis
4.5. Pathway Analysis Using Ingenuity Pathways Analysis Software
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Goldbach-Mansky, R.; Wilson, M.; Fleischmann, R.; Olsen, N.; Silverfield, J.; Kempf, P.; Kivitz, A.; Sherrer, Y.; Pucino, F.; Csako, G.; et al. Comparison of Tripterygium wilfordii Hook F. versus sulfasalazine in the treatment of rheumatoid arthritis: A randomized trial. Ann. Intern. Med. 2009, 151, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Zha, Q.; Chang, A.; He, Y.; Lu, A. Pattern differentiation in traditional chinese medicine can help define specific indications for biomedical therapy in the treatment of rheumatoid arthritis. J. Altern. Complement. Med. 2009, 15, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Zha, Q.L.; Zhang, C.; Lu, C.; Yan, X.P.; Zhu, W.H.; Liu, W.; Tu, S.H.; Hou, L.P.; Wang, C.W.; et al. Predicting and verifying outcome of Tripterygium wilfordii Hook F. based therapy in rheumatoid arthritis: From open to double-blinded randomized trial. Sci. Rep. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Lu, A.P.; Jia, H.W.; Xiao, C.; Lu, Q.P. Theory of traditional chinese medicine and therapeutic method of diseases. World J. Gastroenterol. 2004, 10, 1854–1856. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.Y. Therapeutic wisdom in traditional chinese medicine: A perspective from modern science. Trends Pharmacol. Sci. 2005, 26, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Lu, C.; Zhang, C.; Yang, J.; Tan, Y.; Lu, A.; Chan, K. Syndrome differentiation in modern research of traditional chinese medicine. J. Ethnopharmacol. 2012, 140, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Lu, A.; Wang, Y. Symptomatic comparison in efficacy on patients with benign prostatic hyperplasia treated with two therapeutic approaches. Complement. Ther. Med. 2010, 18, 21–27. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Lu, A.; Lu, C.; Zha, Y.; Yan, X.; Song, Y.; Zeng, S.; Liu, W.; Zhu, W.; Su, L.; et al. Symptom combinations assessed in traditional chinese medicine and its predictive role in ACR20 efficacy response in rheumatoid arthritis. Am. J. Chin. Med. 2008, 36, 675–683. [Google Scholar] [CrossRef] [PubMed]
- De Seny, D.; Fillet, M.; Meuwis, M.A.; Geurts, P.; Lutteri, L.; Ribbens, C.; Bours, V.; Wehenkel, L.; Piette, J.; Malaise, M.; et al. Discovery of new rheumatoid arthritis biomarkers using the surface-enhanced laser desorption/ionization time-of-flight mass spectrometry proteinchip approach. Arthritis Rheum. 2005, 52, 3801–3812. [Google Scholar] [CrossRef] [PubMed]
- Garnero, P.; Delmas, P.D. Noninvasive techniques for assessing skeletal changes in inflammatory arthritis: Bone biomarkers. Curr. Opin. Rheumatol. 2004, 16, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.; Wu, J.; Kuhn, E.; Chin, W.; Chang, B.; Jones, M.D.; O'Neil, S.; Clauser, K.R.; Karl, J.; Hasler, F.; et al. Use of mass spectrometry to identify protein biomarkers of disease severity in the synovial fluid and serum of patients with rheumatoid arthritis. Arthritis Rheum. 2004, 50, 3792–3803. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Pedrera, C.; Barbarroja, N.; Villalba, J.M. Novel biomarkers of atherosclerosis and cardiovascular risk in autoimmune diseases: Genomics and proteomics approaches. Proteom. Clin. Appl. 2009, 3, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Xiao, C.; Chen, G.; Jiang, M.; Zha, Q.; Yan, X.; Kong, W.; Lu, A. Cold and heat pattern of rheumatoid arthritis in traditional chinese medicine: Distinct molecular signatures indentified by microarray expression profiles in CD4-positive T cell. Rheumatol. Int. 2012, 32, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Van Wietmarschen, H.; Yuan, K.; Lu, C.; Gao, P.; Wang, J.; Xiao, C.; Yan, X.; Wang, M.; Schroen, J.; Lu, A.; et al. Systems biology guided by Chinese medicine reveals new markers for sub-typing rheumatoid arthritis patients. J. Clin. Rheumatol. 2009, 15, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Toms, T.E.; Panoulas, V.F.; Smith, J.P.; Douglas, K.M.; Metsios, G.S.; Stavropoulos-Kalinoglou, A.; Kitas, G.D. Rheumatoid arthritis susceptibility genes associate with lipid levels in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2011, 70, 1025–1032. [Google Scholar] [CrossRef] [PubMed]
- Kawashiri, S.Y.; Kawakami, A.; Yamasaki, S.; Imazato, T.; Iwamoto, N.; Fujikawa, K.; Aramaki, T.; Tamai, M.; Nakamura, H.; Ida, H.; et al. Effects of the anti-interleukin-6 receptor antibody, tocilizumab, on serum lipid levels in patients with rheumatoid arthritis. Rheumatol. Int. 2011, 31, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Glocker, M.O.; Guthke, R.; Kekow, J.; Thiesen, H.J. Rheumatoid arthritis, a complex multifactorial disease: On the way toward individualized medicine. Med. Res. Rev. 2006, 26, 63–87. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; Wilson, I.D. Opinion: Understanding ‘global’ systems biology: Metabonomics and the continuum of metabolism. Nat. Rev. Drug Discov. 2003, 2, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; Connelly, J.; Lindon, J.C.; Holmes, E. Metabonomics: A platform for studying drug toxicity and gene function. Nat. Rev. Drug. Discov. 2002, 1, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Madsen, R.K.; Lundstedt, T.; Gabrielsson, J.; Sennbro, C.J.; Alenius, G.M.; Moritz, T.; Rantapaa-Dahlqvist, S.; Trygg, J. Diagnostic properties of metabolic perturbations in rheumatoid arthritis. Arthritis Res. Ther. 2011, 13, R19. [Google Scholar] [CrossRef] [PubMed]
- Van Wietmarschen, H.A.; Dai, W.; van der Kooij, A.J.; Reijmers, T.H.; Schroen, Y.; Wang, M.; Xu, Z.; Wang, X.; Kong, H.; Xu, G.; et al. Characterization of rheumatoid arthritis subtypes using symptom profiles, clinical chemistry and metabolomics measurements. PLoS ONE 2012, 7, e44331. [Google Scholar] [CrossRef] [PubMed]
- Lao, Y.M.; Jiang, J.G.; Yan, L. Application of metabonomic analytical techniques in the modernization and toxicology research of traditional chinese medicine. Br. J. Pharmacol. 2009, 157, 1128–1141. [Google Scholar] [CrossRef] [PubMed]
- Pollizzi, K.N.; Powell, J.D. Integrating canonical and metabolic signalling programmes in the regulation of t cell responses. Nat. Rev. Immunol. 2014, 14, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Trang, L.E.; Furst, P.; Odeback, A.C.; Lovgren, O. Plasma amino acids in rheumatoid arthritis. Scand. J. Rheumatol. 1985, 14, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Shet, K.; Siddiqui, S.M.; Yoshihara, H.; Kurhanewicz, J.; Ries, M.; Li, X. High-resolution magic angle spinning nmr spectroscopy of human osteoarthritic cartilage. NMR Biomed. 2012, 25, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Fu, P.; Ke, B.; Wang, S.; Li, M.; Han, L.; Peng, C.; Zhang, W.; Liu, R. Metabolomic analysis of biochemical changes in the plasma and urine of collagen-induced arthritis in rats after treatment with huang-lian-jie-du-tang. J. Ethnopharmacol. 2014, 154, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Ma, T.; Gu, J.; Liang, X.; Li, S. Imbalanced network biomarkers for traditional chinese medicine syndrome in gastritis patients. Sci. Rep. 2013, 3, 1543. [Google Scholar] [CrossRef] [PubMed]
- Nikolac Perkovic, M.; Pucic Bakovic, M.; Kristic, J.; Novokmet, M.; Huffman, J.E.; Vitart, V.; Hayward, C.; Rudan, I.; Wilson, J.F.; Campbell, H.; et al. The association between galactosylation of immunoglobulin g and body mass index. Prog. Neuropsychopharmacol. Biol. Psychiatry. 2014, 48, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Girardi, E.; Holdom, M.D.; Davies, A.M.; Sutton, B.J.; Beavil, A.J. The crystal structure of rabbit IGG-FC. Biochem. J. 2009, 417, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Chang, X.; Wei, C. Glycolysis and rheumatoid arthritis. Int. J. Rheum. Dis. 2011, 14, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 2001, 285, 2486–2497. [Google Scholar]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the national cholesterol education program (ncep) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Solomon, D.H.; Goodson, N.J.; Katz, J.N.; Weinblatt, M.E.; Avorn, J.; Setoguchi, S.; Canning, C.; Schneeweiss, S. Patterns of cardiovascular risk in rheumatoid arthritis. Ann. Rheum. Dis. 2006, 65, 1608–1612. [Google Scholar] [CrossRef] [PubMed]
- Maradit-Kremers, H.; Crowson, C.S.; Nicola, P.J.; Ballman, K.V.; Roger, V.L.; Jacobsen, S.J.; Gabriel, S.E. Increased unrecognized coronary heart disease and sudden deaths in rheumatoid arthritis: A population-based cohort study. Arthritis Rheum. 2005, 52, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Lazarevic, M.B.; Vitic, J.; Myones, B.L.; Mladenovic, V.; Nanusevic, N.; Skosey, J.L.; Swedler, W.I. Antilipoprotein antibodies in rheumatoid arthritis. Semin. Arthritis Rheum. 1993, 22, 385–391. [Google Scholar] [CrossRef]
- Dunn, W.B.; Broadhurst, D.; Begley, P.; Zelena, E.; Francis-McIntyre, S.; Anderson, N.; Brown, M.; Knowles, J.D.; Halsall, A.; Haselden, J.N.; et al. Procedures for large-scale metabolic profiling of serum and plasma using gas chromatography and liquid chromatography coupled to mass spectrometry. Nat. Protoc. 2011, 6, 1060–1083. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.; Lu, C.; Zhang, F.; Sang, P.; Yang, D.; Li, X.; Kong, H.; Yin, P.; Tian, J.; Lu, X.; et al. Integrated gc-ms and lc-ms plasma metabonomics analysis of ankylosing spondylitis. Analyst 2008, 133, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhao, X.; Fritsche, J.; Yin, P.; Schmitt-Kopplin, P.; Wang, W.; Lu, X.; Haring, H.U.; Schleicher, E.D.; Lehmann, R.; et al. Practical approach for the identification and isomer elucidation of biomarkers detected in a metabonomic study for the discovery of individuals at risk for diabetes by integrating the chromatographic and mass spectrometric information. Anal. Chem. 2008, 80, 1280–1289. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aziz, H.O.; Takasaki, I.; Tabuchi, Y.; Nomoto, K.; Murai, Y.; Tsuneyama, K.; Takano, Y. High-density oligonucleotide microarrays and functional network analysis reveal extended lung carcinogenesis pathway maps and multiple interacting genes in NNK [4-(methylnitrosamino)-1-(3-pyridyle)-1-butanone] induced CD1 mouse lung tumor. J. Cancer Res. Clin. Oncol. 2007, 133, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Calvano, S.E.; Xiao, W.; Richards, D.R.; Felciano, R.M.; Baker, H.V.; Cho, R.J.; Chen, R.O.; Brownstein, B.H.; Cobb, J.P.; Tschoeke, S.K.; et al. A network-based analysis of systemic inflammation in humans. Nature 2005, 437, 1032–1037. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Chen, J.Y. Discovery of pathway biomarkers from coupled proteomics and systems biology methods. BMC Genom. 2010, 11, S12. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No. | Pathway | Molecules | Cold Pattern vs. Healthy Control | Heat Pattern vs. Healthy Control | ||||
|---|---|---|---|---|---|---|---|---|
| Fold | Regulations | p Value | Fold | Regulations | p Value | |||
| 1 | Aminoacyl-tRNA biosynthesis | l-isoleucine | 1.11 | ↑ | 5.94 × 10−7 | 1.11 | ↑ | 4.21 × 10−8 |
| l-leucine | N.S | N.S | 1.25 | ↑ | ||||
| l-threonine | 1.11 | ↑ | 1.25 | ↑ | ||||
| l-valine | 1.25 | ↑ | 1.25 | ↑ | ||||
| l-proline | 2.5 | ↓ | N.S | N.S | ||||
| 2 | Valine, leucine and isoleucine biosynthesis | l-isoleucine | 1.11 | ↑ | 1.87 × 10−4 | 1.11 | ↑ | 1.54 × 10−7 |
| l-leucine | N.S | N.S | 1.25 | ↑ | ||||
| l-valine | 1.25 | ↑ | 1.25 | ↑ | ||||
| 3 | Urea cycle and metabolism of amino groups | l-proline | 2.5 | ↓ | 1.31 × 10−3 | N.S | N.S | N.S |
| Urea | 1.3 | ↓ | N.S | N.S | N.S | |||
| 4 | Alanine and aspartate metabolism | d-alanine | 1.2 | ↓ | 1.50 × 10−3 | 1.4 | ↓ | 3.21 × 10−2 |
| Citric acid | 1.3 | ↓ | N.S | N.S | ||||
| 5 | Valine, leucine and isoleucine degradation | l-isoleucine | 1.11 | ↑ | 3.26 × 10−3 | 1.11 | ↑ | 1.23 × 10−5 |
| l-leucine | N.S | N.S | 1.25 | ↑ | ||||
| l-valine | 1.25 | ↑ | 1.25 | ↑ | ||||
| 6 | Glycine, serine and threonine metabolism | d-glyceric acid | 3.5 | ↓ | 4.96 × 10−3 | 2.9 | ↓ | 1.53 × 10−3 |
| l-threonine | 1.11 | ↑ | 1.25 | ↑ | ||||
| 7 | Arginine and proline metabolism | l-proline | 2.5 | ↓ | N.S | N.S | N.S | |
| Urea | 1.3 | ↓ | N.S | N.S | N.S | |||
| 8 | Glutamate metabolism | Citric acid | 1.3 | ↓ | 5.91 × 10−2 | N.S | N.S | N.S |
| No. | Pathway | Molecules | Cold Pattern vs. Healthy Control | Heat Pattern vs. Healthy Control | ||||
|---|---|---|---|---|---|---|---|---|
| Fold | Regulations | p Value | Fold | Regulations | p Value | |||
| 1 | Glyoxylate and dicarboxylate metabolism | Citric acid | 1.3 | ↓ | 9.38 × 10−4 | N.S | N.S | N.S |
| d-glyceric acid | 3.5 | ↓ | 2.9 | ↓ | 2.55 × 10−2 | |||
| 2 | Galactose metabolism | myo-inositol | 1.5 | ↓ | 1.80 × 10−3 | 1.5 | ↓ | 3.52 × 10−2 |
| d-glucose | 1.4 | ↓ | N.S | N.S | ||||
| 3 | Inositol metabolism | myo-inositol | 1.5 | ↓ | 1.02 × 10−2 | 1.5 | ↓ | 5.77 × 10−3 |
| 4 | Citrate cycle | Citric acid | 1.3 | ↓ | 4.48 × 10−2 | N.S | N.S | N.S |
| 5 | Pentose phosphate pathway | d-glucose | 1.4 | ↓ | 4.39 × 10−2 | N.S | N.S | N.S |
| 6 | Propanoate metabolism | l-valine | 1.25 | ↑ | 7.57 × 10−2 | 1.25 | ↑ | 4.33 × 10−2 |
| 7 | Starch and sucrose metabolism | d-glucose | 1.4 | ↓ | 8.18 × 10−2 | N.S | N.S | N.S |
| 8 | Glycolysis/gluconeogenesis | d-glucose | 1.4 | ↓ | 9.38 × 10−2 | N.S | N.S | N.S |
| No. | Pathway | Molecules | Cold Pattern vs. Healthy Control | Heat Pattern vs. Healthy Control | ||||
|---|---|---|---|---|---|---|---|---|
| Fold | Regulations | p Value | Fold | Regulations | p Value | |||
| 1 | Fatty acid biosynthesis | Palmitic acid | 1.2 | ↓ | 1.76 × 10−2 | N.S | N.S | N.S |
| 2 | Fatty acid elongation in mitochondria | Palmitic acid | 1.2 | ↓ | 4.12 × 10−2 | N.S | N.S | N.S |
| 3 | Biosynthesis of steroids | cholesterol | 1.2 | ↓ | 5.2 × 10−2 | N.S | N.S | N.S |
| 4 | C21-steroid hormone metabolism | cholesterol | 1.2 | ↓ | 5.2 × 10−2 | N.S | N.S | N.S |
| 5 | Linoleic acid metabolism | Linoleic Acid | 1.2 | ↓ | 6.43 × 10−2 | N.S | N.S | N.S |
| 6 | Bile acid metabolism | Linoleic Acid | 1.2 | ↓ | 7.4 × 10−2 | N.S | N.S | N.S |
| 7 | Glycerolipid metabolism | d-glyceric acid | 3.5 | ↓ | 9.8 × 10−2 | 2.9 | ↓ | 5.64 × 10−2 |
| 8 | Fatty acid metabolism | Palmitic acid | 1.2 | ↓ | 1.28 × 10−1 | N.S | N.S | N.S |
| 9 | Inositol phosphate metabolism | myo-inositol | 1.5 | ↓ | 1.44 × 10−1 | 1.5 | ↓ | 8.4 × 10−2 |
| Item | RA with Cold Pattern (n = 28) | RA with Heat Pattern (n = 29) |
|---|---|---|
| Age, mean (S.D.), years | 46.7 (9.7) | 42.0 (1.7) |
| RA disease duration, mean (S.D.), years | 1.5 (0.9) | 1.3 (1.1) |
| ESR, mean (S.D.), mm/h | 20.2 (10.3) | 21.5 (9.6) |
| RF, positive, n (%) | 14 (50) | 16 (55.2) |
| DAS28-ESR, mean (S.D.) | 2.3 (0.6) | 2.3 (0.5) |
| Anti-CCP, positive, n (%) | 19 (67.9) | 21 (72.4) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, H.; Niu, X.; Gu, Y.; Lu, C.; Xiao, C.; Yue, K.; Zhang, G.; Pan, X.; Jiang, M.; Tan, Y.; et al. Differential Amino Acid, Carbohydrate and Lipid Metabolism Perpetuations Involved in a Subtype of Rheumatoid Arthritis with Chinese Medicine Cold Pattern. Int. J. Mol. Sci. 2016, 17, 1757. https://doi.org/10.3390/ijms17101757
Guo H, Niu X, Gu Y, Lu C, Xiao C, Yue K, Zhang G, Pan X, Jiang M, Tan Y, et al. Differential Amino Acid, Carbohydrate and Lipid Metabolism Perpetuations Involved in a Subtype of Rheumatoid Arthritis with Chinese Medicine Cold Pattern. International Journal of Molecular Sciences. 2016; 17(10):1757. https://doi.org/10.3390/ijms17101757
Chicago/Turabian StyleGuo, Hongtao, Xuyan Niu, Yan Gu, Cheng Lu, Cheng Xiao, Kevin Yue, Ge Zhang, Xiaohua Pan, Miao Jiang, Yong Tan, and et al. 2016. "Differential Amino Acid, Carbohydrate and Lipid Metabolism Perpetuations Involved in a Subtype of Rheumatoid Arthritis with Chinese Medicine Cold Pattern" International Journal of Molecular Sciences 17, no. 10: 1757. https://doi.org/10.3390/ijms17101757