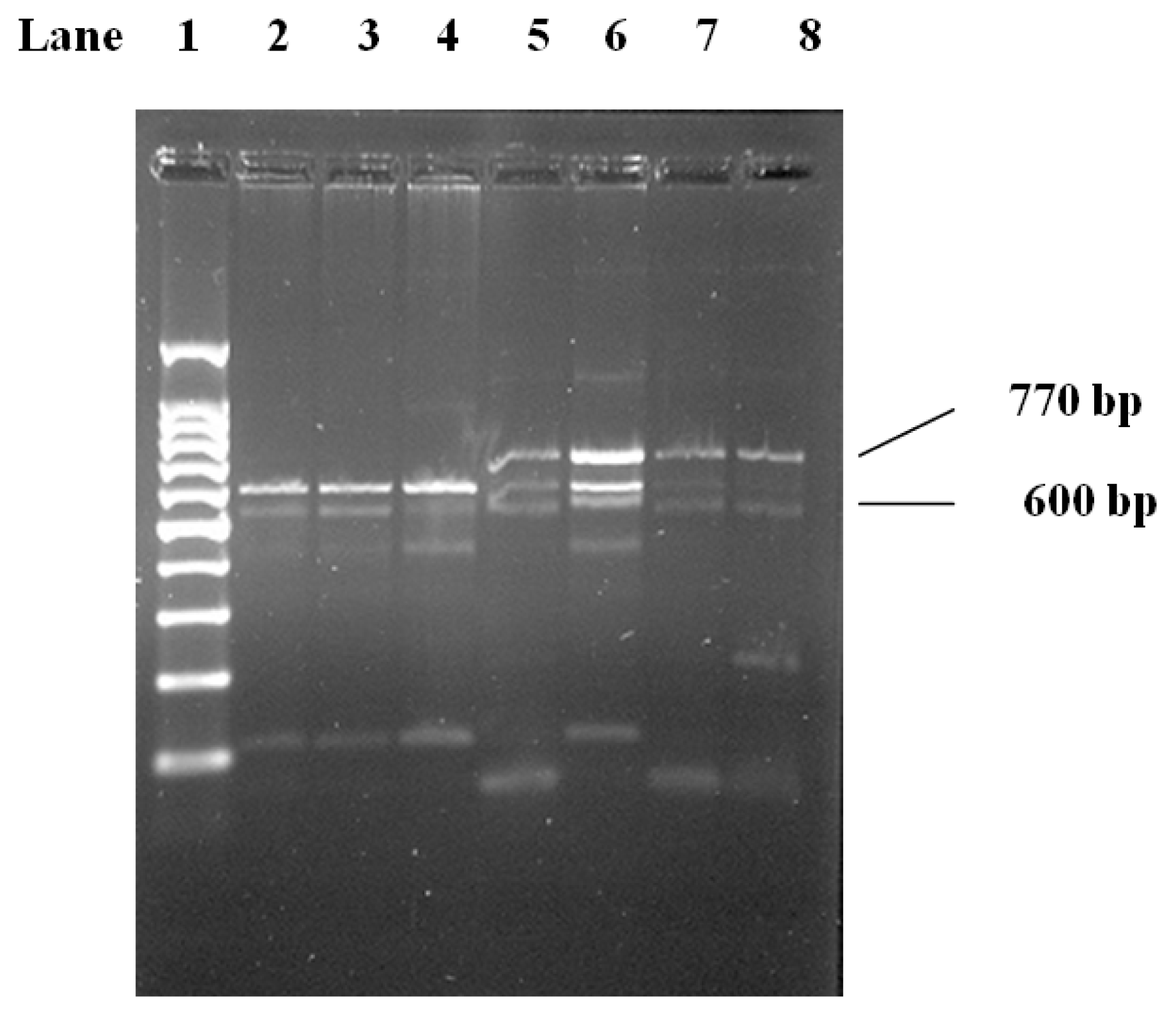
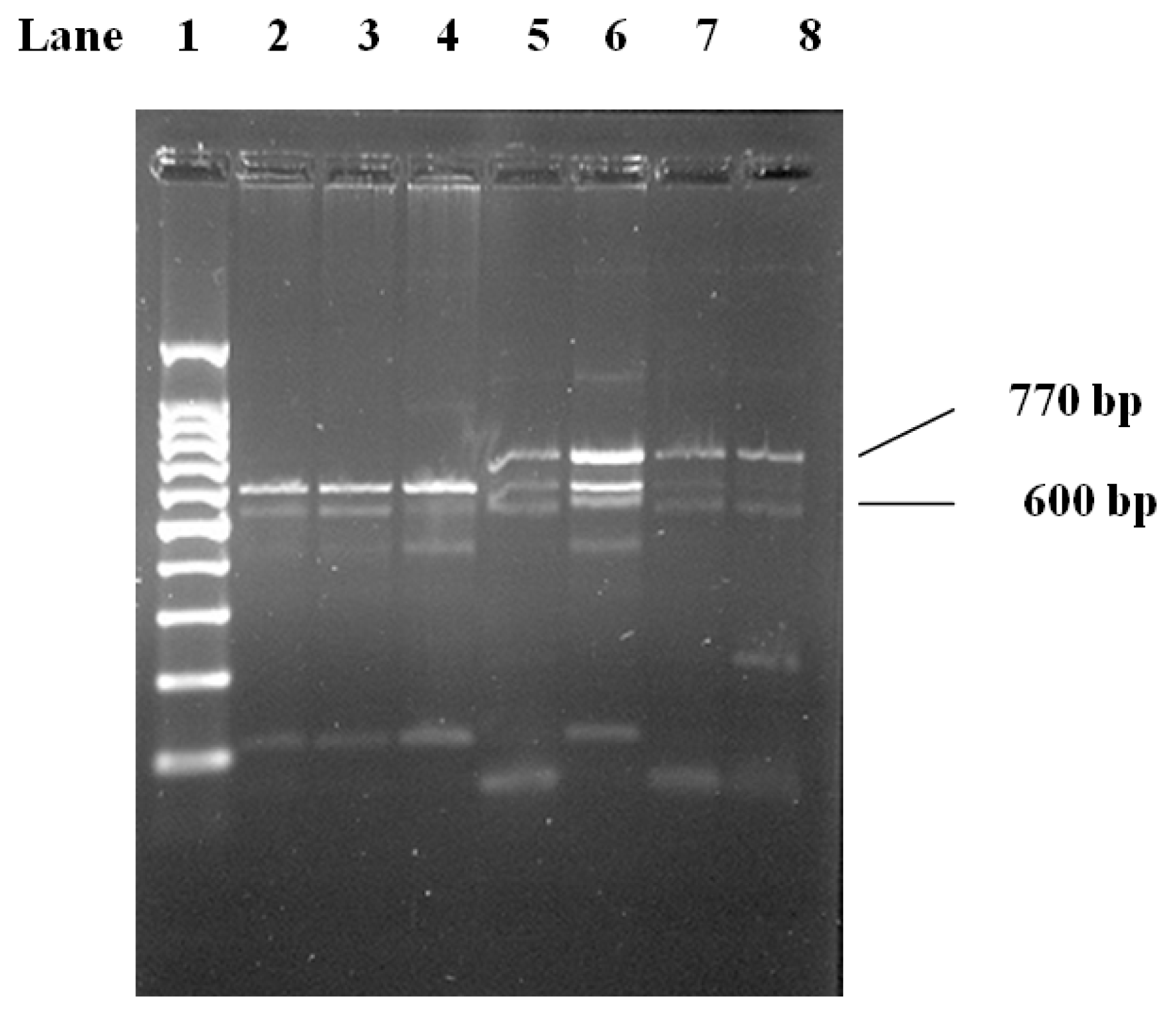
Genotype frequencies did not deviate from Hardy-Weinberg expectations in both controls and CAD group. The genotype distribution and the allele frequency for LPL gene polymorphisms are summarized in
Table 2. H
+ and H
− alleles did not differ significantly between CAD group and controls. For the
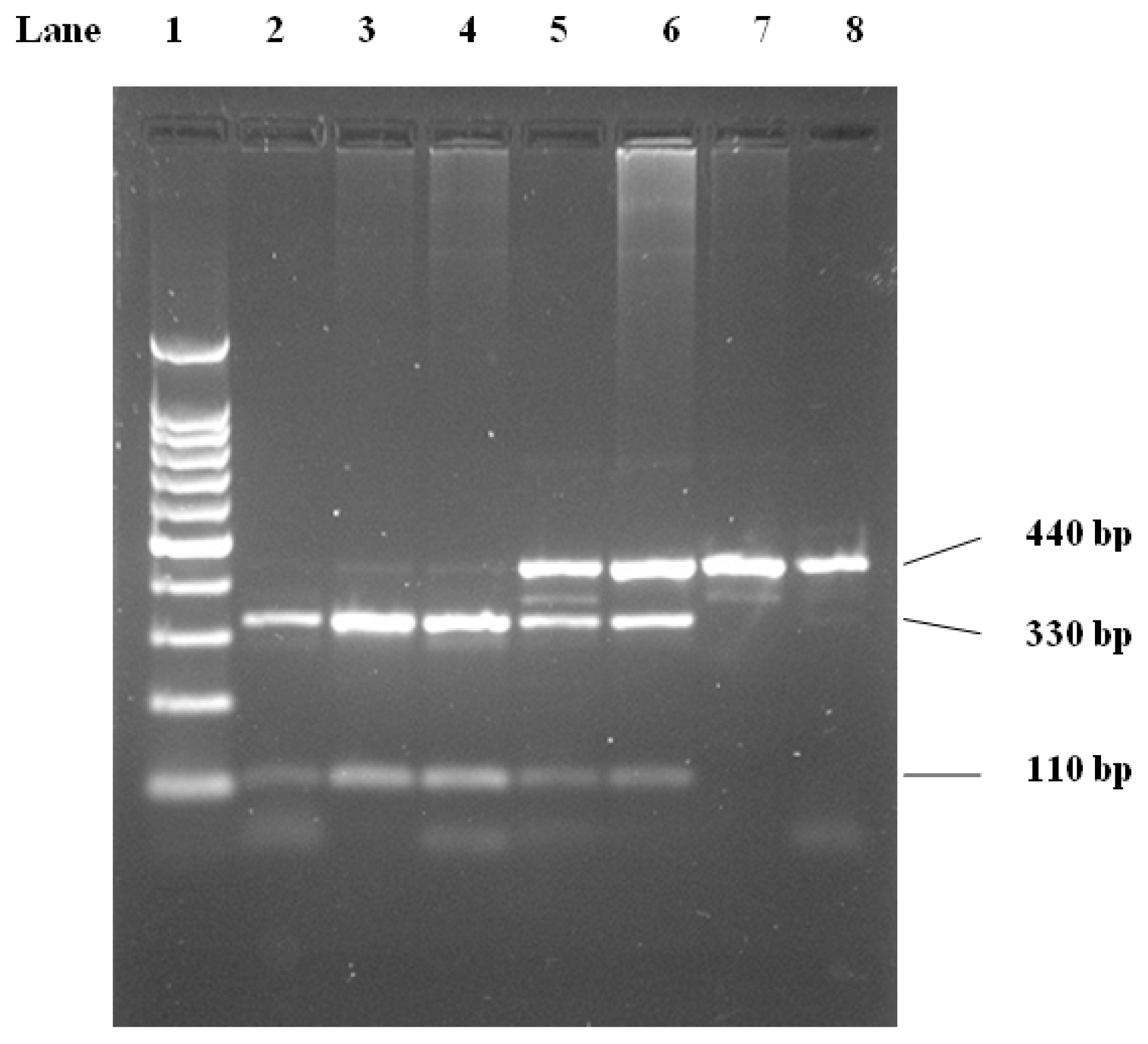
HindIII genotype, within the CAD group (
n = 120), the frequencies of the H
+H
+ found in 61 individuals (50.8%), whereas 52 (44.3%) carried the H
−/H
+ genotype, and 6 (5%) carried the H
−/H
− genotype. Within the control group (n = 65), the H
+/H
+ genotype was found in 29 (44.6%), whereas 23 (35.4%) carried the H
−/H
+ genotype, and 13.0 (20%) carried the H
−H
− genotype. the distribution of
HindIII demonstrated that CAD patients had lower H
−H
− frequency compared to the control group and higher H
+H
−, H
+H
+ frequencies compared to the control group
Table 3. Odds Ratios were 4.5 and 4.6 respectively when compared with (H
−H
−) genotype. Individuals with homozygous (H
+H
+) or (H
+H
−) genotype were at much higher risk of developing CAD compared to the (H
−H
−) genotype (
p < 0.005),
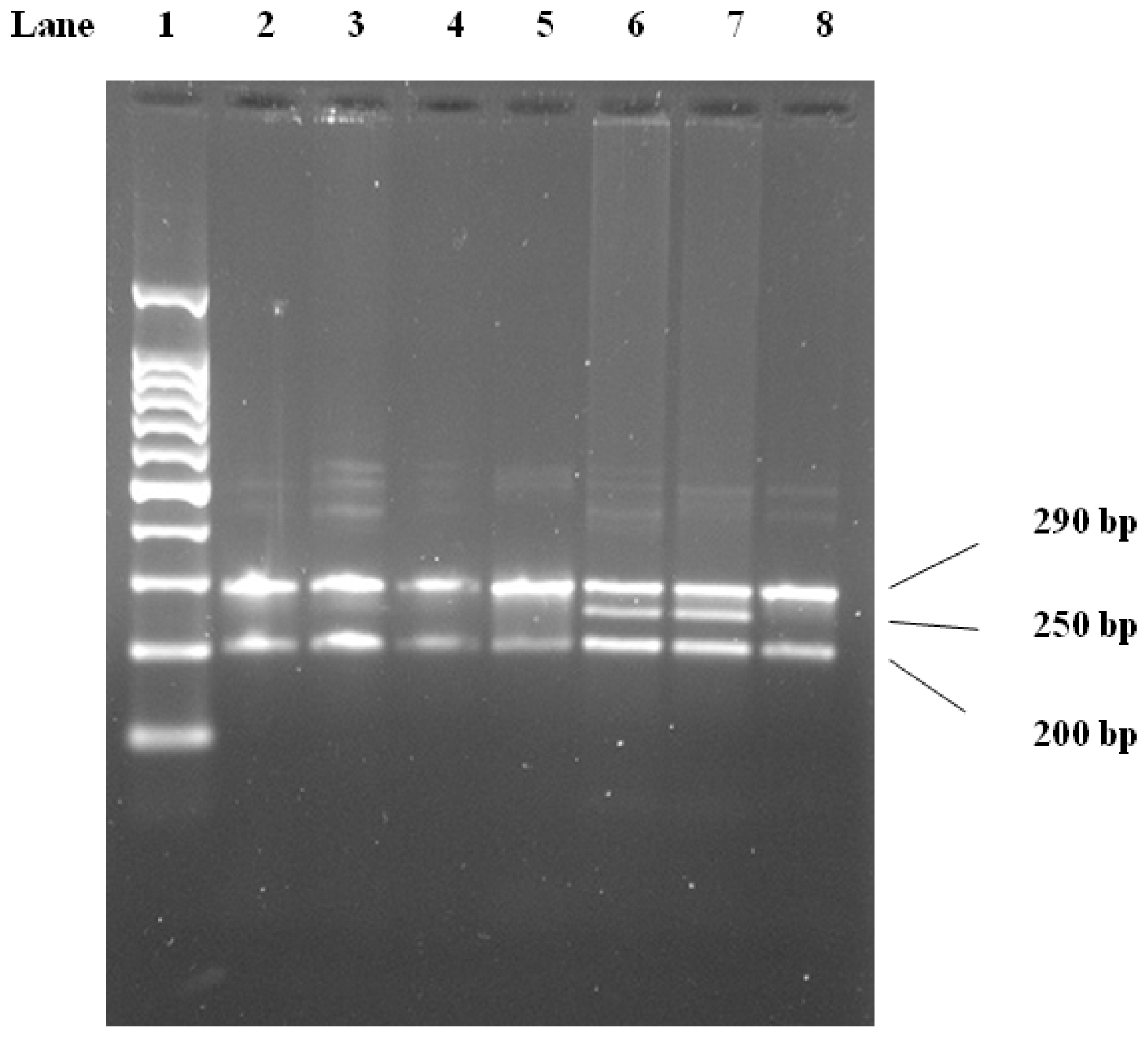
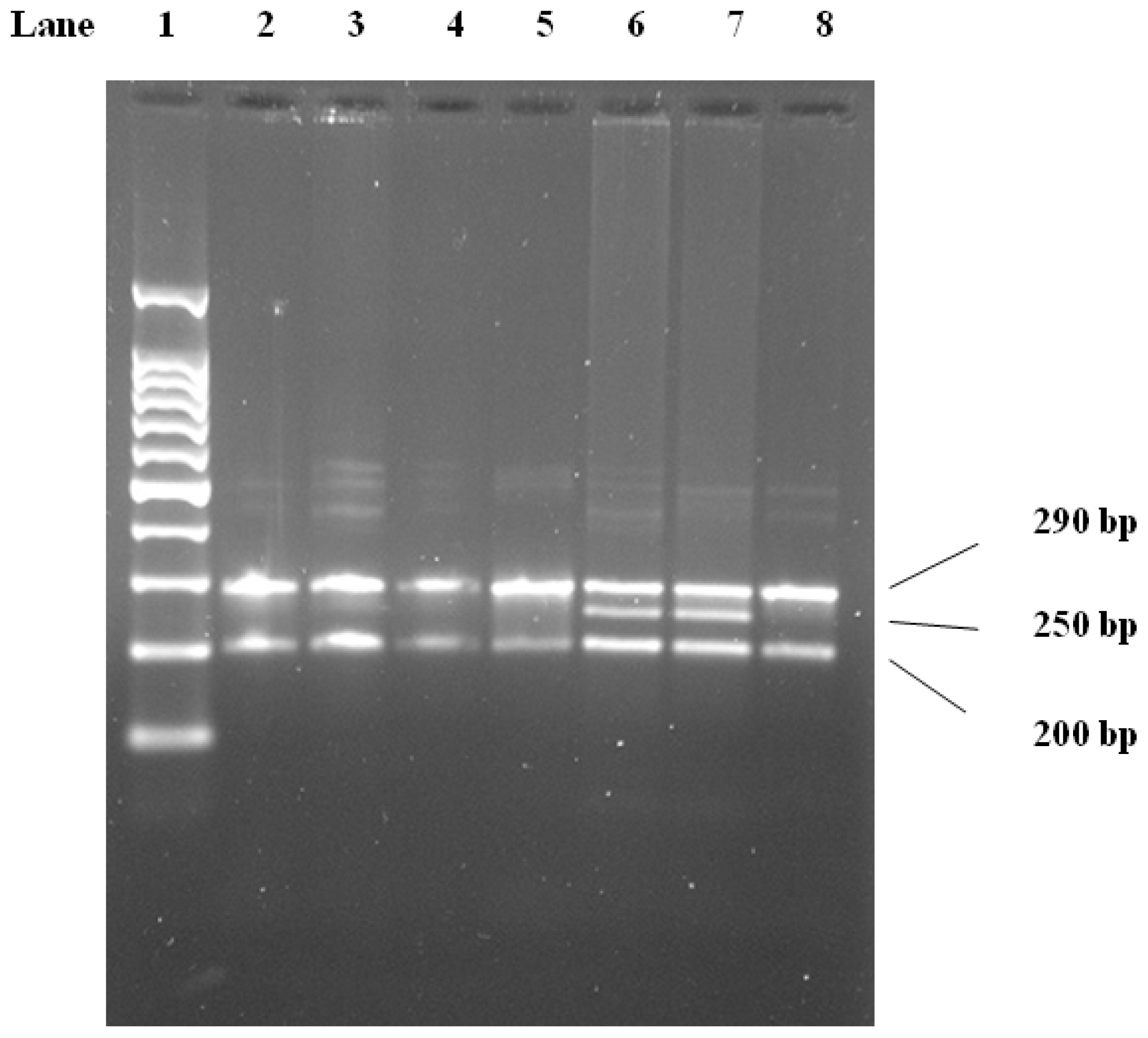
Table 4. For the
PvuII genotype, within the CAD group (
n = 120), the frequencies of the P
+P
+ found in 50 (41.7%), whereas 52 (43.2%) carried the P
−P
+ genotype, and 18 (15%) carried the P
−P
− genotype. Within the control group (
n = 65), the P
+P
+ was found in 25 (38.5%), 28 (43.0%) carried the P
−P
+ genotype, and 12.0 (18.5%) carried the P
−P
− genotype. The distribution of
PvuII polymorphism demonstrated that CAD patients had higher P
+P
−, P
−P
−, P
+P
+ frequencies compared with controls,
Table 3. The odds ratios of
PvuII genotype P
−P
− vs. P
−P
+ and P
+P
+ genotypes (95% CI) is 1.26 (90.53–2.99) and 1.33 (0.56–3.20) respectively, hence showing no significant association with CAD disease
Table 5. In previous studies, the prevalence rate of the LPL-
HindIII (H
+H
+) genotype was implicated as the most common genotype associated with CAD. Shimo-Nakanishi
et al. (2001) [
17] demonstrated that
HindIII polymorphism is associated with increased risk of atherothrombotic infarction. Likewise, Chamberlain
et al. (1989) [
30] indicated that there were differences in frequencies of both
HindIII and
PvuII alleles between Whites and Japanese populations, the statistical analysis for the LPL-
HindIII genotypes indicates significant differences in the distribution of these genotypes between the control groups and the CAD groups, which in agreement with previous reported study [
20]. Several studies have investigated the possibility that the LPL
-HindIII and the LPL-
PvuII polymorphisms are associated with the severity of CAD in various populations [
1,
14,
16,
19,
20,
31–
36]. However, limited data are available concerning the Saudi population [
21], which has not adequately defined the association between LPL polymorphism and CAD. While a large number of studies have found the LPL-
HindIII (H
+H
+) genotype to be associated with CAD, the finding from the association studies with LPL-
PvuII polymorphisms have been inconsistent [
14,
15,
19,
33,
35]. For example, Thorne
et al. (1990) [
15] reported an increase in the LPL-
HindIII (H
+H
+) genotypic frequencies in patients with coronary atherosclerosis in Japanese population whereas Peacok
et al. (1992) [
33] observed no differences in either LPL-
HindIII or LPL-
PvuII allelic frequencies in young survivors of myocardial infarction in Spanish population. Ukkola
et al. (1995) [
35] found reductions in various measures of ischemic heart disease in non-insulin-dependent diabetics who were LPL-
PvuII (P
+P
+), but noted increases in those who were LPL-
HindIII (H
−H
−) in Canadian adult population. In contrast, Gerdes
et al. (1995) [
34] found the LPL-
HindIII (H
+H
+) genotype to be positively associated with a family history of premature ischemic heart disease in a group of Danish men. Similarly, Mattu
et al. (1994) [
32] found an association between the LPL-
HindIII H
+H
+ genotype and CAD, but not between the LPL-
PvuII (P
+P
+) genotype and CAD in native Brazilian population. On the other hand, Wang
et al. (1996) [
14] reported an association between the extent, but not occurrence of CAD and the LPL-
PvuII (P
+P
+) genotype. However, in the same study, Wang
et al. (1996) [
14] found no association between the LPL-
HindIII genotype and CAD. Interestingly, Gambino
et al. (1999) [
31] found a striking association between the LPL-
HindIII (H
+H
+) genotype and multi-vessel disease in an Italian group of young survivors of myocardial infarction. Also it has been reported that Anderson
et al. (1999) [
1] found a moderate association between the LPL-
HindIII (H
+H
+) genotype and CAD, whereas the LPL
-PvuII (P
−P
−) genotype was modestly associated with CAD. In summary, the relevance of these genotypes may vary among different populations.
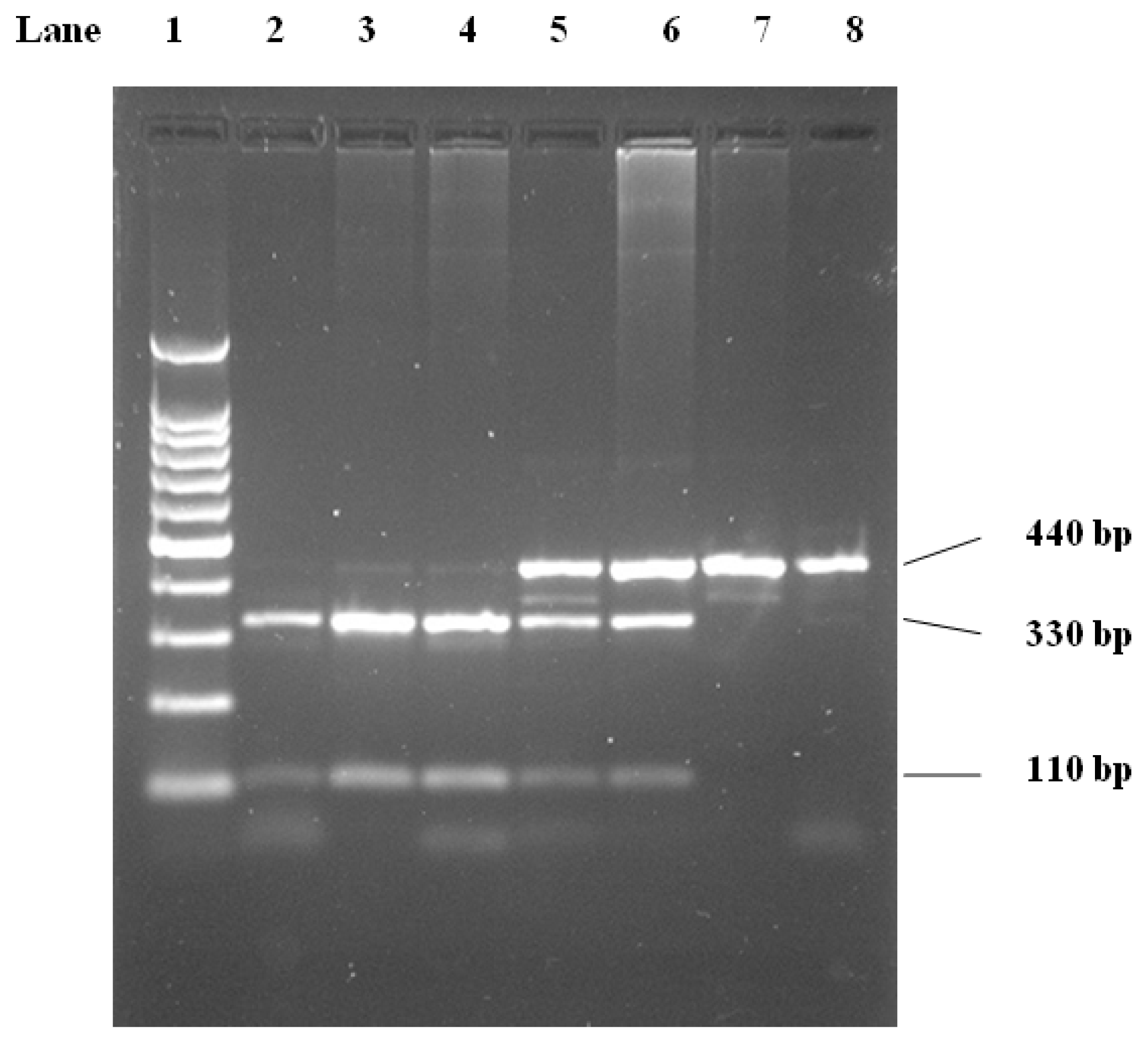
For the Ser447Ter genotype, within the CAD group (
n = 120), the frequencies of the CC found in 100 (83.3%), whereas 20 (16.7%) carried the CG genotype. Within the control group (
n = 65), the CC was found in 57 (87.7%) and 8 (12.3%) carried the CG genotype. We did not get any GG genotypes in the control or any patients for this gene. The homozygote of G allele was incorporated with the heterozygote due to the low frequency of GG, higher frequencies of CC and CG genotypes in the CAD group
Table 3. OR of CC
vs. CG+GG (95% CI) is 1.43 from 0.59 to 3.44, which is insignificant,
Table 4. Interestingly, no GG genotype was observed in the CAD and control groups in the distribution of Ser447Ter polymorphism in the present study. However, we found for the first time in Saudi populations new genotype frequencies of Ser447-Ter mutations of the LPL gene between the CAD patients and the healthy controls. In previous reported studies, the frequency of the Ser447-Ter genotype of GG and CG was significantly lower in a group of Japanese CAD patients than in the control [
37], representing a significantly low risk of CAD. Also Shimo-Nakanishi
et al. (2001) [
17] found that Ser447 Stop mutations of the LPL gene are a novel genetic marker for low risk of atherothrombotic cerebral infarction. Kozaki
et al. (1993) [
37] originally found an approximately 2-fold increase in the enzymatic activity of LPL resulting from the Ser447-Ter mutations at the carboxy terminal of LPL transfected and expressed
in vitro, conflicting results that demonstrated that Ser447-Ter mutations might have either no or an inverse effect on LPL function may have been caused by different methodology.
Haplotype frequencies for the
HindIII,
PvuII and Ser447Ter alleles were estimated for controls and patients (
Table 6). A score for each haplotype (Hap-score) was calculated and the
P-value was obtained for the significance of each Hap-score. The haplotypes −/−/C, +/−/C, −/−/G, −/+/C, −/+/G, +/−/G, +/+/C and +/+/G are the most common in the CAD patients group. There were differences between the CAD group and control group with regards to the haplotype distribution. Comparison of the common haplotype frequencies between the CAD patients group and control group revealed a significant increase in the frequency of the most common haplotype in those with CAD. This also suggests an increase in the frequency of less common haplotypes among some cases. Haplotypes −/−/G and +/+/C were associated with a significantly increased risk factor of CAD (
p = 0.06, 0.04 respectively).
Table 6 Shows that combined genotypes may play an important role in the process of atherogenesis. It has been proposed that the H
−allele is a marker either for a mutation that alters an amino acid within LPL, causing enzyme activity or lipid binding to be more efficient, or possibly for a sequence change within the promoter, causing higher levels of LPL expression [
20]. The frequencies of H
−/C and P
−/C were significantly higher in CI patients than in controls, and the H
−/P
−/C combined genotype was the most common genotype of
HindIII/
PvuII/Ser447Ter combined genotypes in the cerebral infarction group.
P−allele is more frequent and G allele is less frequent in cerebral infarction (CI) patients than in controls. The data also provide strong evidence of an association between polymorphisms in the LPL gene with lipid levels. Moreover, H
−/C and P
−/C mutations, especially H
−/P
−/C mutation of the LPL gene, are relevant to CI.
PvuII polymorphism is a risk factor for CI while Ser447Ter mutation is a protective factor, indicating that the LPL polymorphism remains a useful genetic marker for predicting CI risk in the Chinese [
19]. Goodarzi
et al. 2003 [
38] showed no differences between cases and controls, in comparison of genotype frequencies except for a modestly significant difference for the 8393 (
HindIII) variant (
p = 0.05). However, comparison of the common haplotype frequencies between the Mexican-Americans with and without coronary artery disease revealed a significant decrease in the frequency of the most common haplotype in those with disease. Goodarzi
et al. 2003 found that six markers in the 3′ end of
LPL allowed us to distinguish the most common haplotypes occurring in two major U.S. ethnic groups, Hispanic and non-Hispanic Caucasians. The allele and haplotype frequencies were different between the Mexican-Americans and non-Hispanic Caucasians. Furthermore, within the Mexican-Americans, there were positive and negative associations of particular haplotypes with coronary artery disease, suggesting a role of this gene in contributing to CAD in this population. In comparing two different ethnic groups, Goodarzi
et al. 2003 [
38] found several differences in the allele and haplotype frequencies observed in the 3′
LPL markers. Such differences may affect the results of association studies conducted in different populations.


{kind=link}
{kind=link}
{kind=link}