1. Introduction
In the current study, we evaluate whether 5-aminulevulinic acid (5-ALA) may improve various components of mood among study participants with prediabetes using two questionnaires entitled Psychosocial Depressive Symptoms Questionnaire and the Perceived Stress Scale (See
Supplementary Materials). Prediabetes or intermediate hyperglycemia is a high-risk state for the development of diabetes [
1]. According to an American Diabetes Association panel of experts, up to 70 percent of prediabetic individuals will ultimately develop diabetes [
1]. Prediabetes is defined by glycemic variables (e.g., blood glucose concentrations) that are higher than normal limits, but lower than the diagnostic criteria for diabetes [
1]. The most effective diabetes prevention method in prediabetic individuals is lifestyle modification [
1]. This finding is supported by evidence showing a 40 to 70 percent relative-risk reduction for diabetes development [
1]. Lifestyle modifications include reducing body weight and moderate daily exercise [
2].
However, despite the benefits of lifestyle change, diabetes prevalence continues to increase [
3]. In the U.S., diabetes affects 25.8 million Americans [
4]. That is, more than 1 in 10 adults have diabetes and the prevalence of diabetes continues to rise in adults [
3,
4,
5]. In fact, over the last 30 years the prevalence has increased by 176 percent [
3]. This increase may be related to the many emotional health obstacles a prediabetic adult faces when it comes to maintaining an exercise routine and a healthy eating plan. Some examples of these emotional health obstacles are fatigue, poor sleep, mood swings, irritability, anxiety and depression [
6,
7]. Finding a solution to treat these emotional health issues may help prediabetic individuals maintain the healthy lifestyle modifications necessary to prevent the development of diabetes.
A potential treatment for prediabetic emotional health issues, such as mood, is 5-ALA. This natural compound is a heme precursor in mammals and a chlorophyll precursor in plants (See
Figure 1) [
8,
9]. Many common foods contain 5-ALA such as spinach, green peppers, tomatoes, bananas, and ground beef [
10]. In previous publications, using the same study design and group of participants, previous authors reported that the administration of 5-ALA improves sleep [
11] and reduces two hour post-oral glucose tolerance test (OGTT) glucose levels [
12]. Specifically, Rodriguez and colleagues (2012) reported that among individuals taking 5-ALA for 12 weeks, two hour post–OGTT glucose levels declined significantly compared to those not taking the supplement (
p = 0.02) [
12]. The relationship was greater among those with glucose measurements greater than 140 mg/dL (
p = 0.005 and
p = 0.02 for the low and high dose groups, respectively) [
12]. Similar trends were observed for Hemoglobin A1c but results were of borderline significance (
p = 0.07) [
12]. More recently, other studies have confirmed the beneficial effect of 5-ALA on glucose metabolism [
13,
14,
15,
16]. The health applications of 5-ALA, something that is currently not fully understood, is critical in designing the most effective wellness and diabetes prevention program.
In this study, our first aim is to perform an integrative literature review of the relationship between the administration of 5-ALA with mood and coping ability. The second aim is to determine the relationship between 15 mg and 50 mg 5-ALA and mood and coping ability using the Psychosocial Depressive Symptoms (PDS) and Perceived Stress Scale (PSS) Questionnaires. The final aim is to determine if a dose-dependent relationship exists between 5-ALA, mood, and coping ability.
2. Materials and Methods
2.1. Study Design
This research study uses previously collected data from the Prediabetes and Supplement Study (PASS). The PASS is a double-blinded randomized parallel-group comparison prospective study using participants residing on Oahu, Hawaii. Recruitment of study participants utilized IRB-approved local newspaper advertisements, flyers, television and radio advertising, referrals from local physicians, and local seminars and community programs. The study group includes 154 participants, both men and women, between the ages of 40 to 70 years old. All enrolled participants signed the IRB-approved informed consent. The selection of study participants was based on the strict inclusion and exclusion criteria provided in
Table 1. For further details on study design, please see the paper by Rodriguez and colleagues [
12].
2.2. Procedures
Potential participants were first screened and if eligible, consented at the initial visit. If eligible, participants were enrolled and asked to take a nutritional supplement (5-ALA) once a day for 90 days. The participants were randomly allocated to the following three study groups described in
Table 2: control group (
n = 51), 15 mg low dose of 5-ALA (
n = 50), and 50 mg high dose of 5-ALA (
n = 53). As described in
Table 2, the control group was given a placebo capsule of identical size and color. The 5-ALA supplement used in this study contains the following components: (1) 5-ALA, (2) sodium ferrous citrate (SFC), and (3) corn starch as a filler [
12]. For further information about the 5-ALA supplement used, please review the paper by Rodriguez and colleagues [
12].
Table 3 describes the administration of the 5-ALA supplement. Participants were required to report for periodic physical exams the initial screening visit and every four weeks thereafter (Week 4, 8, 12, and 16). During these periodic check-ups, blood samples were collected. Blood samples were sent to the Diagnostic Laboratory Services of Hawaii for analysis.
2.3. Data Collection Tools
Table 4 and
Table 5 describe the study procedures. Study participants were interviewed about diet, smoking status, and exercise or physical activity. The Prediabetes and Supplement Study (PASS) assessment tool, adapted from the Honolulu Heart Study [
17], was used to assess lifestyle and physical activity. The Perceived Stress Scale (PSS) was used to measure stress [
18]. A calibrated digital precision scale and a stadiometer were used to measure the participant’s weight and height, respectively. Body mass index (BMI) was calculated using weight (kg) divided by height (m
2). A calibrated digital sphygmomanometer was used to measure blood pressure. The average of two measurements was used to estimate systolic and diastolic pressures. Finally, blood was collected at the initial visit and at the 12 week visit. The oral glucose tolerance test (OGTT) was also performed at the 12 week visit. For this test, participants fasted for 10 h prior to blood collection. The Diagnostic Laboratory Services of Hawaii performed the standardized blood analyses.
2.4. Questionnaires
The two questionnaires used in this study were the Psychological Depressive Symptoms (PDS) Questionnaire and the Perceived Stress Scale (PSS). These questionnaires are included in
Supplementary Materials. The Psychological Depressive Symptoms questionnaire is a part of the Prediabetes and Supplement Study (PASS) assessment tool, adapted from the Honolulu Heart Study [
17]. The Psychological Depressive Symptoms Questionnaire was designed to measure self-perception of mood. The Perceived Stress Scale, designed by Dr. Sheldon Cohen, is the most widely used psychological tool to measure self-perception of stress [
18]. The questions in the PSS ask the respondent about his or her feelings during the last month regarding certain situations in one’s life [
18]. For each situation, the PSS is designed to measure the degree to which a situation is considered stressful [
18]. Furthermore, since the questions of both questionnaires are written in a general nature, they are relatively free of content specific to any sub-population group [
18]. For both questionnaires, participants were asked about their thoughts and feelings during the last month towards each question. The answer choice options for both questionnaires were: “never,” “almost never,” “sometimes,” “fairly often,” and “very often.”
2.5. Literature Review Procedures
This literature review was focused on clinical trials, cross-sectional, case-control, and prospective cohort studies on the relationship between administrations of 5-ALA with mood and coping ability. A systematic search was conducted up to March 2018 using the PubMed database (MEDLINE, National Library of Medicine, Bethesda, MD, USA). To build a better query in PubMed, MeSH (Medical Subheadings) was utilized. MeSH is the National Library of Medicine controlled vocabulary thesaurus used for indexing articles for PubMed. In PubMed, the MeSH terms used were “5-ALA” or “5 5-aminolevulinic acid” along with other key words: “Prediabetes”, “Hyperglycemia”, “Diabetes”, “Mood”, “Coping”, “Emotional Health”, and “Psychological Health”. The search included both animal and human studies. The search was restricted to articles in English. All full-text studies were considered. This initial search resulted in zero articles. A further search was done using a list of relevant publications provided by SBI Pharmaceuticals Co., Ltd. This search resulted in zero articles. A final search using the above search terms was done using the Google Internet search engine and this also resulted in zero articles.
2.6. Statistical Analyses
Descriptive and inferential statistics were used to evaluate relationships between and among variables. The statistical programs utilized were SAS software, version 10 (SAS Institute Inc., Cary, NC, USA) and GraphPad Prism software, version 6 (GraphPad Software Inc., La Jolla, CA, USA). For the inferential tests, statistical significance was defined as p < 0.05. Using Prism software, a two-way ANOVA was performed to compare age and gender in the three groups. Using SAS software, an ordered logistic regression or proportional odds model was used to analyze the association between the dose groups (control, 15 mg, and 50 mg) and responses to the Psychosocial Depressive Symptoms (PDS) Questionnaire and Perceived Stress Scale (PSS). The appropriateness of the proportional odds model was tested using scored p-values.
4. Discussion
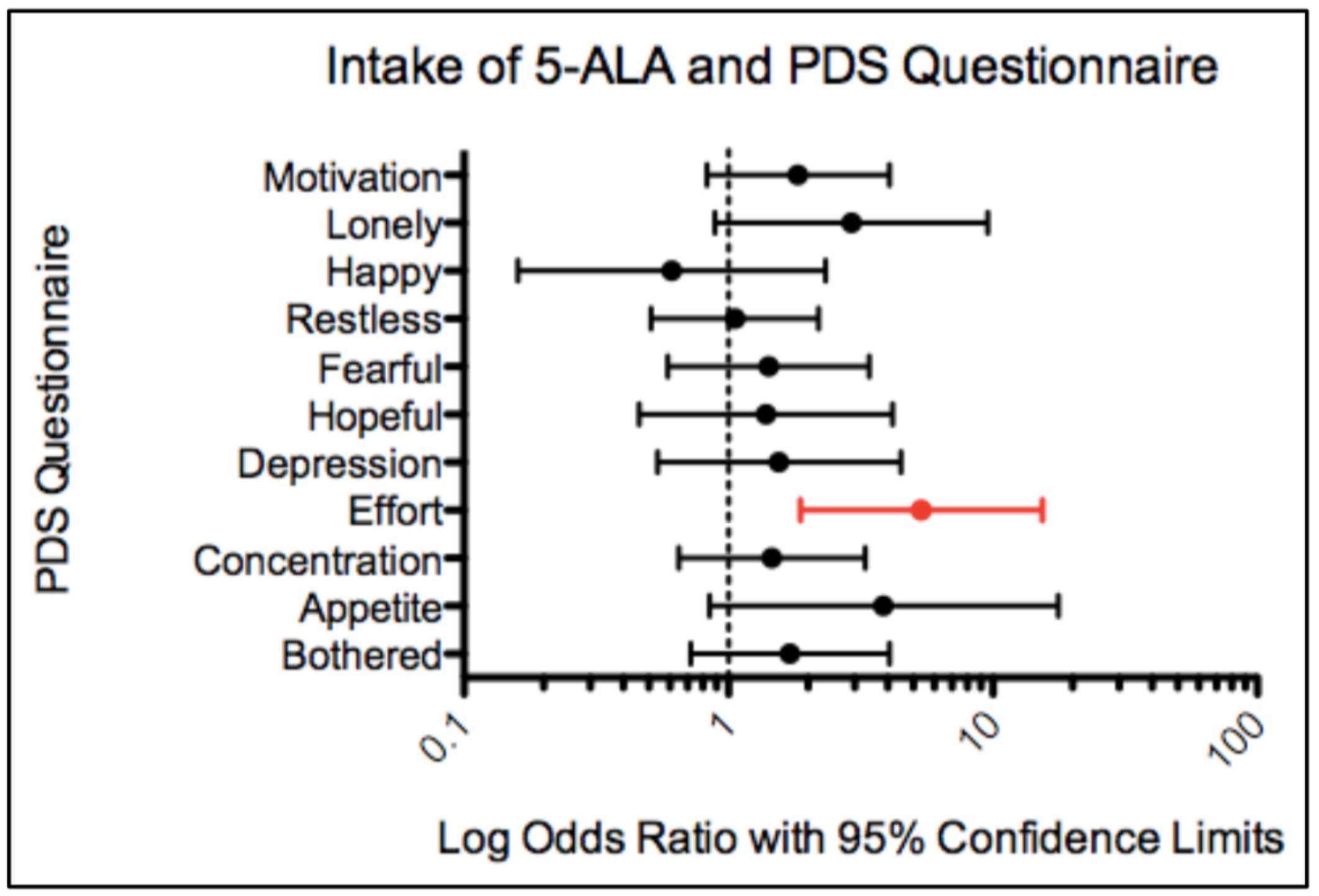
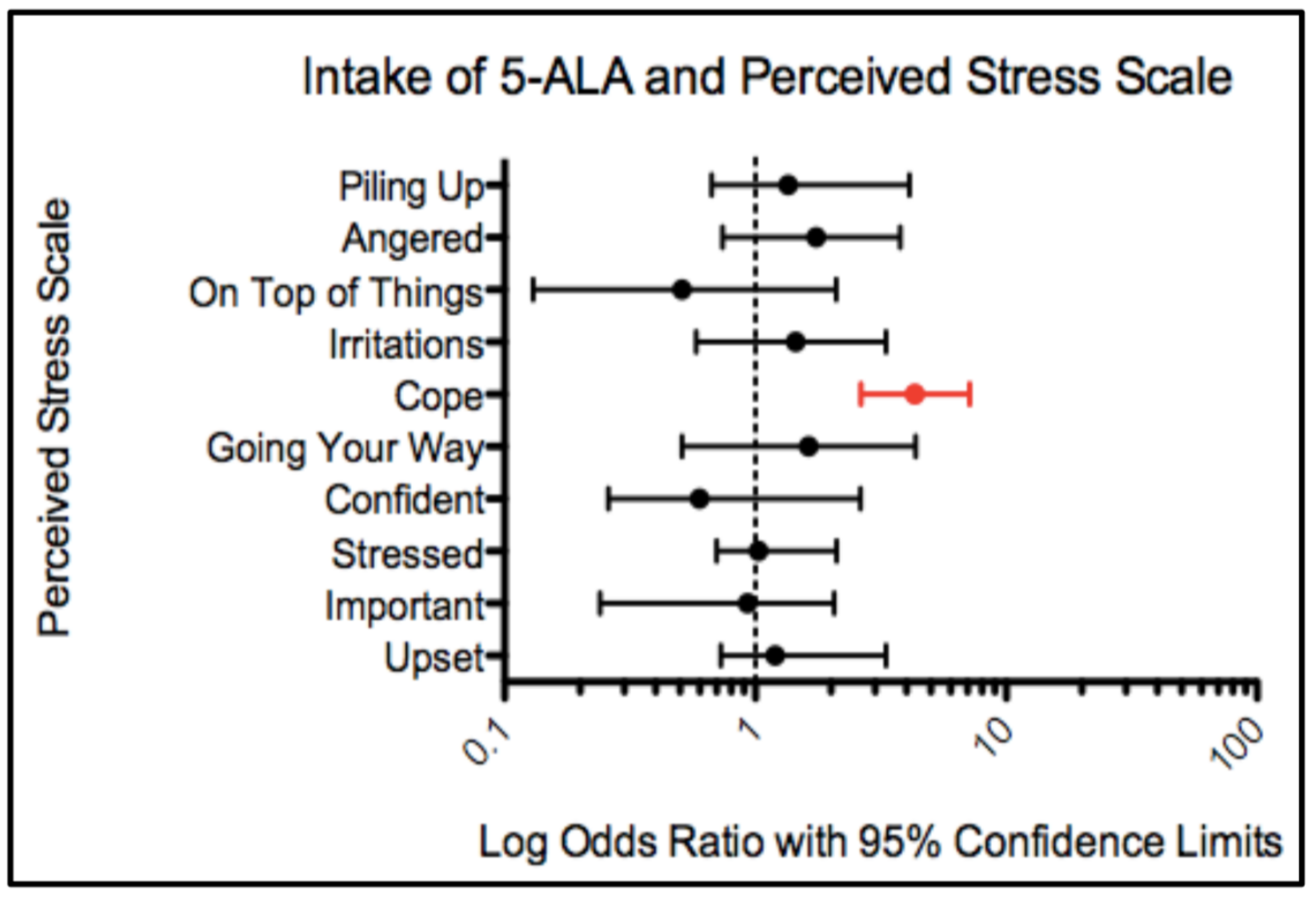
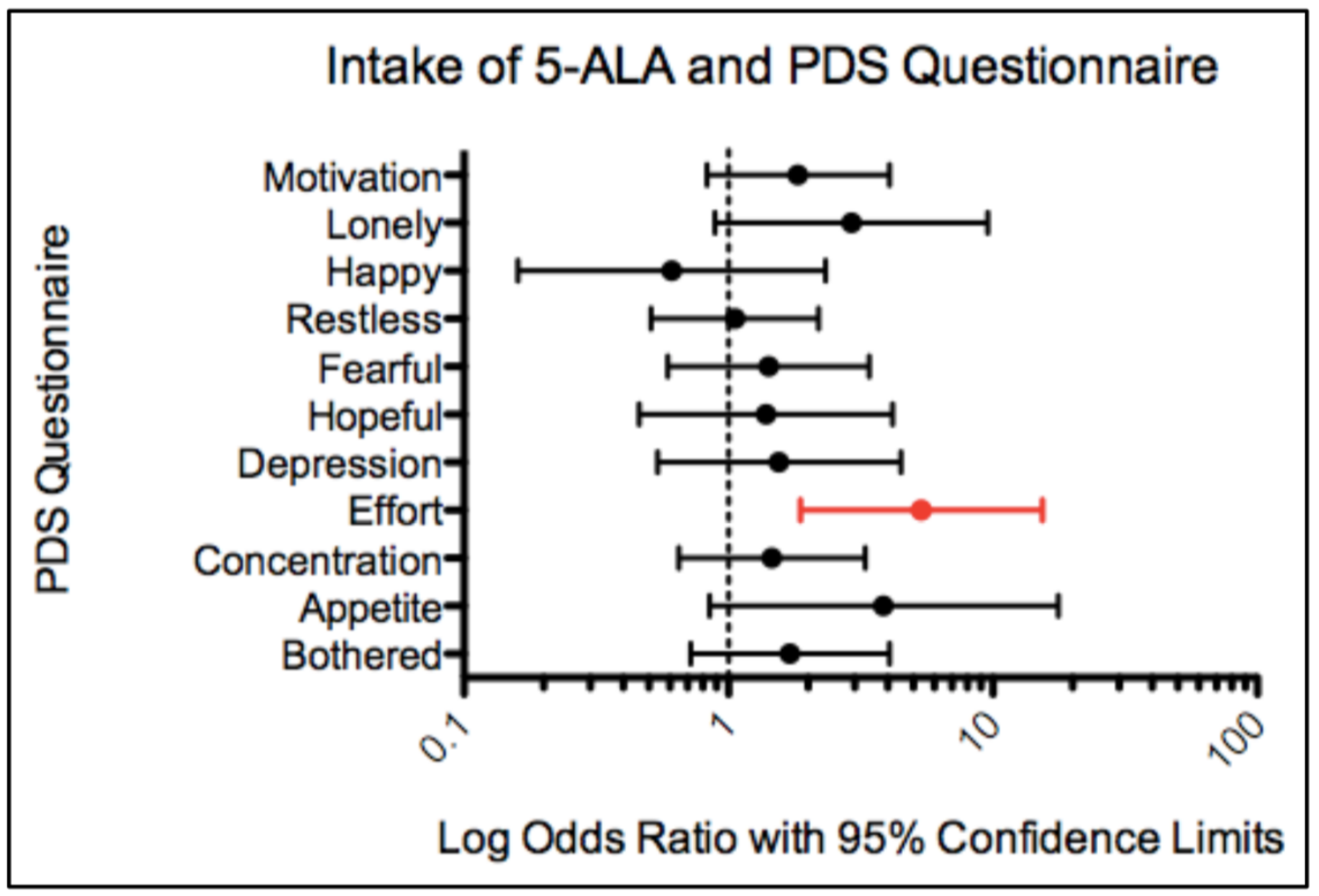
To summarize, the three specific aims of this study were met. First, we completed an integrative literature review that resulted in zero articles published on the relationship between the administration of 5-ALA and mood and coping ability. To the best of our knowledge, this is the first study to report the effect of 5-ALA intake on mood and coping ability in prediabetic middle aged and older adults. Second, utilizing the Psychological Depressive Symptoms (PDS) Questionnaire and the Perceived Stress Scale (PSS), the intake of 5-ALA was significantly associated with improved coping ability and improved self-perception of effort spent. Finally, a dose-dependent relationship was found for the effect of 5-ALA intake on measures of effort, loneliness, and coping ability. The 50 mg dose was more effective than the 15 mg dose in improving these measures. Overall, the intake of 5-ALA improved mood and coping ability in a population of prediabetic middle aged and older adults.
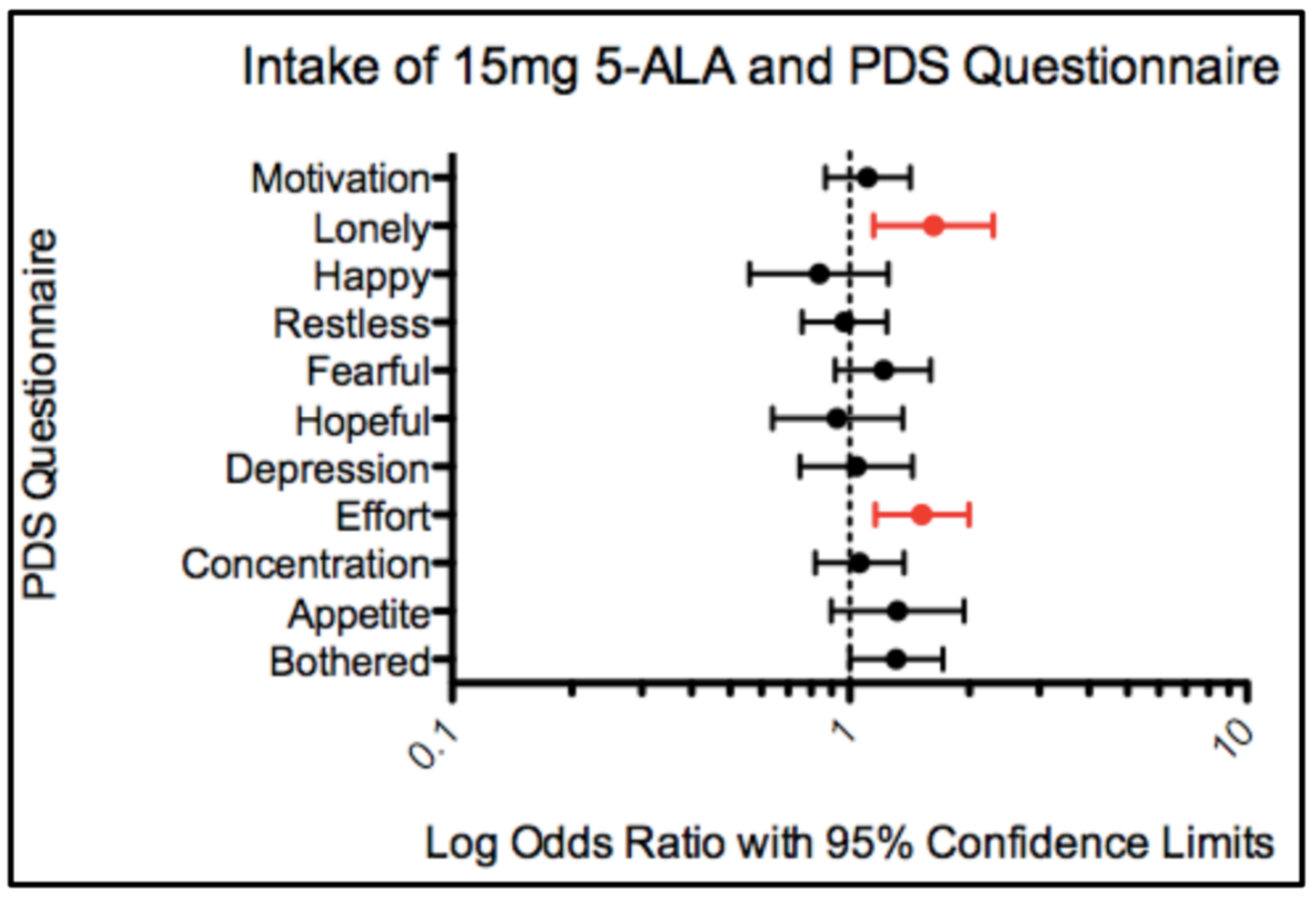
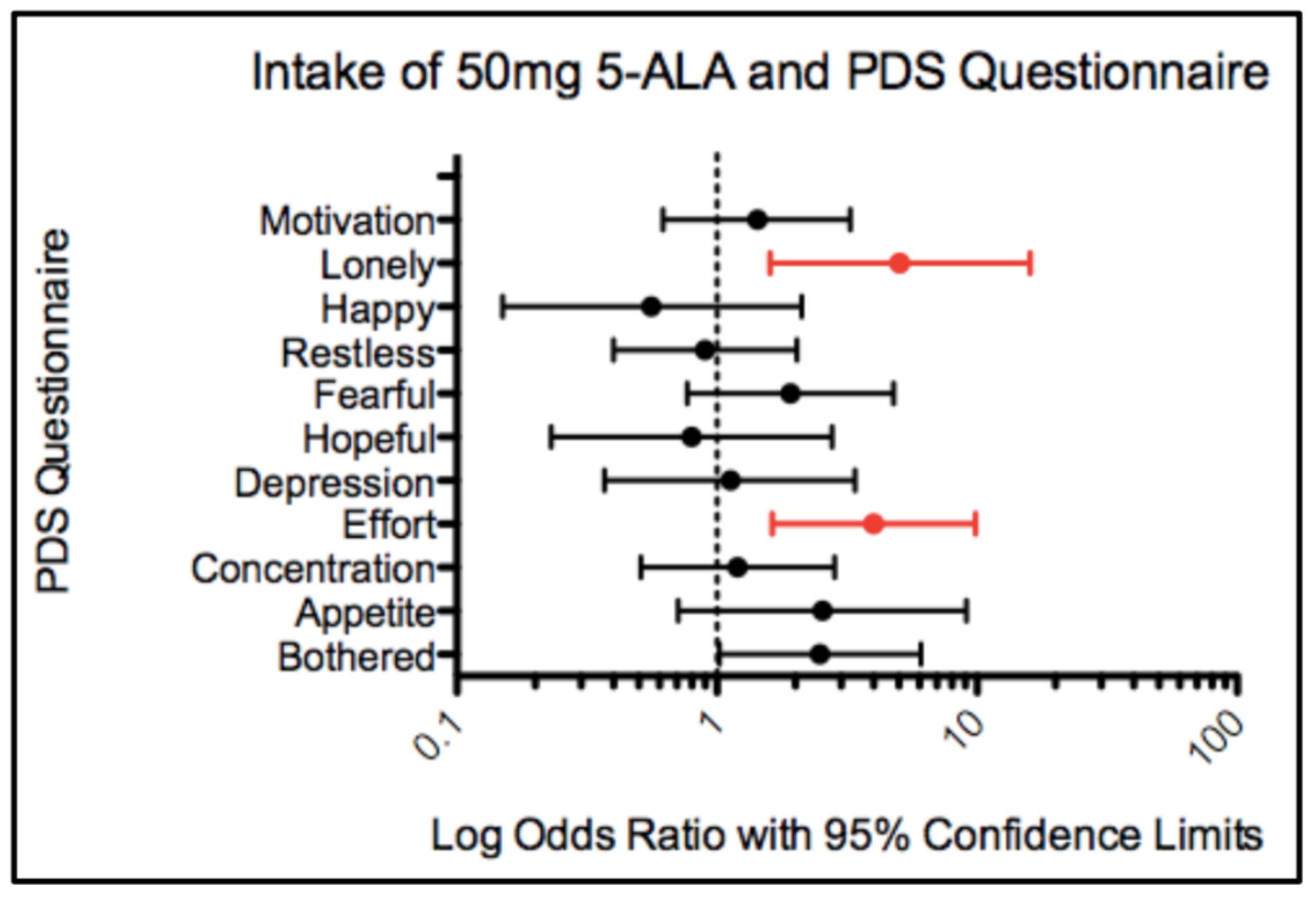
According to the Psychological Depressive Symptoms questionnaire, the intake of 5-ALA after 12 weeks improved self-perception of effort spent (See
Supplementary Materials, PDS Question 4: “I felt that everything I did was an effort”). Compared to the participants’ answers at Week 1 (no 5-ALA), the intake of the 15 mg and 50 mg of 5-ALA significantly improved their perception of effort spent by 1.5 and 4.0 times, respectively. An improvement in self-perception of effort spent is important in helping prevent the development of diabetes. This is because while the most effective diabetes prevention strategy is lifestyle modification [
1], for some individuals the task of maintaining healthy lifestyle changes may feel like an enormous effort or task.
The Psychological Depressive Symptoms questionnaire also revealed that the intake of 5-ALA significantly improved self-perception of loneliness (See
Supplementary Materials, PDS Question 10: “I felt lonely”). Compared to the participants’ answers at Week 1 (no 5-ALA), 15 mg and 50 mg of 5-ALA significantly improved their perception of feeling alone by 1.6 and 5.1 times, respectively. Interestingly, it has been shown that loneliness depends on perception rather than social situation [
19]. Often patients withdraw from family and friend support because they feel isolated or different from other people [
20]. Some diabetic patients contribute the feeling of isolation with the responsibilities that come with their condition (i.e., diet restriction, checking blood glucose, insulin shots, etc.) [
20]. Improving self-perception of loneliness is an important first step in preventing diabetes because prediabetic adults who have help from family, friends, and a community of similar patients are more likely to maintain a healthier lifestyle [
21].
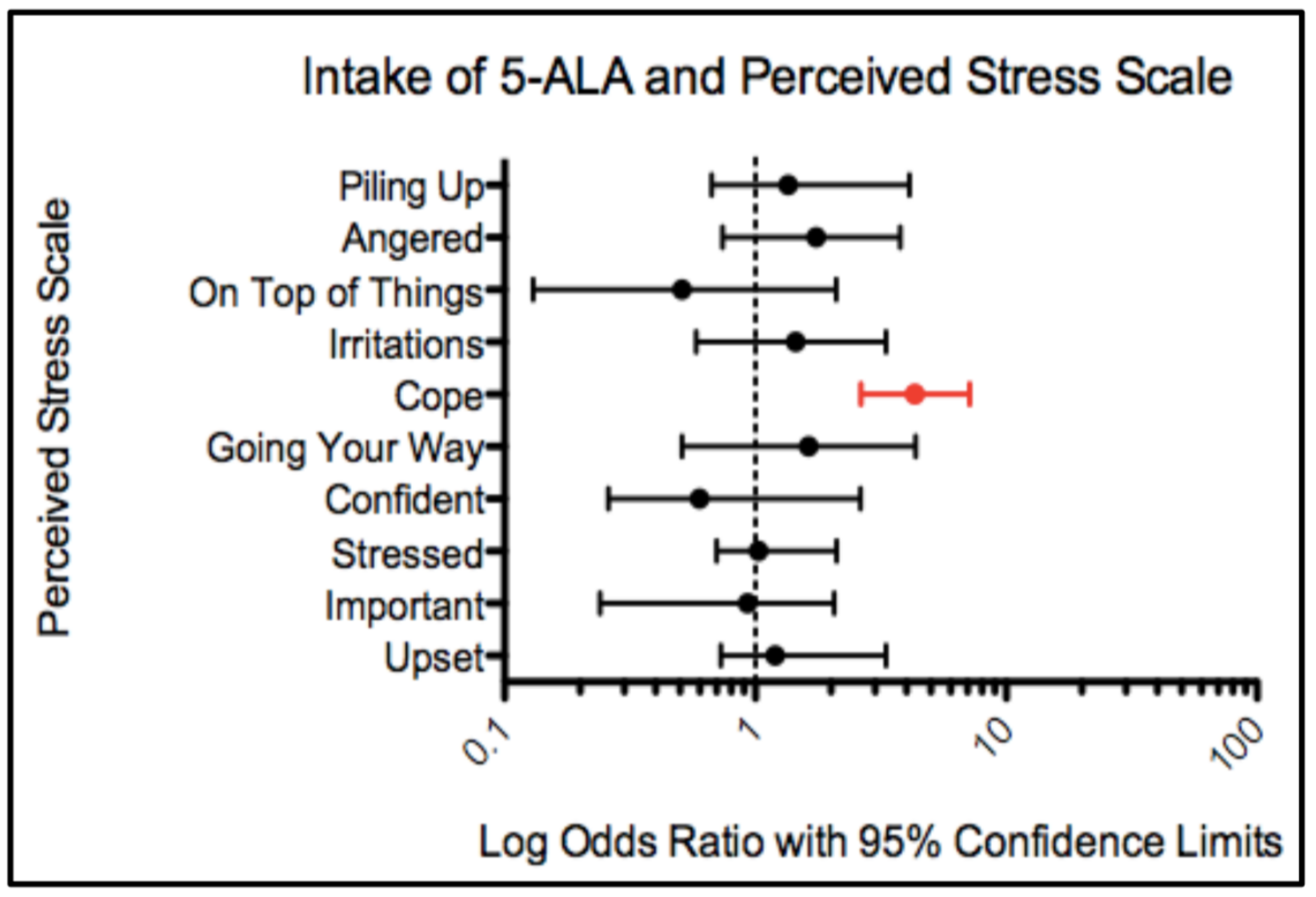
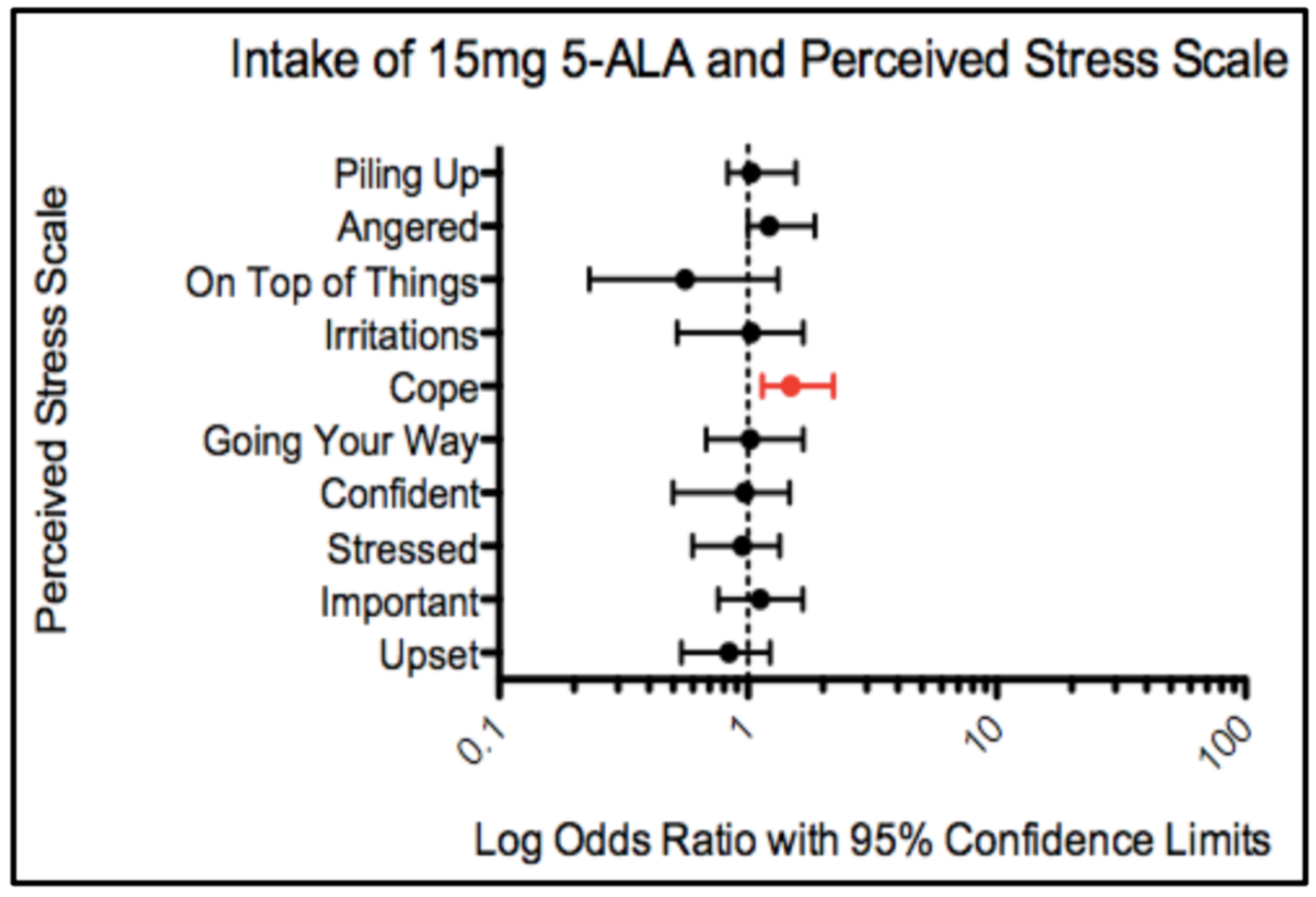
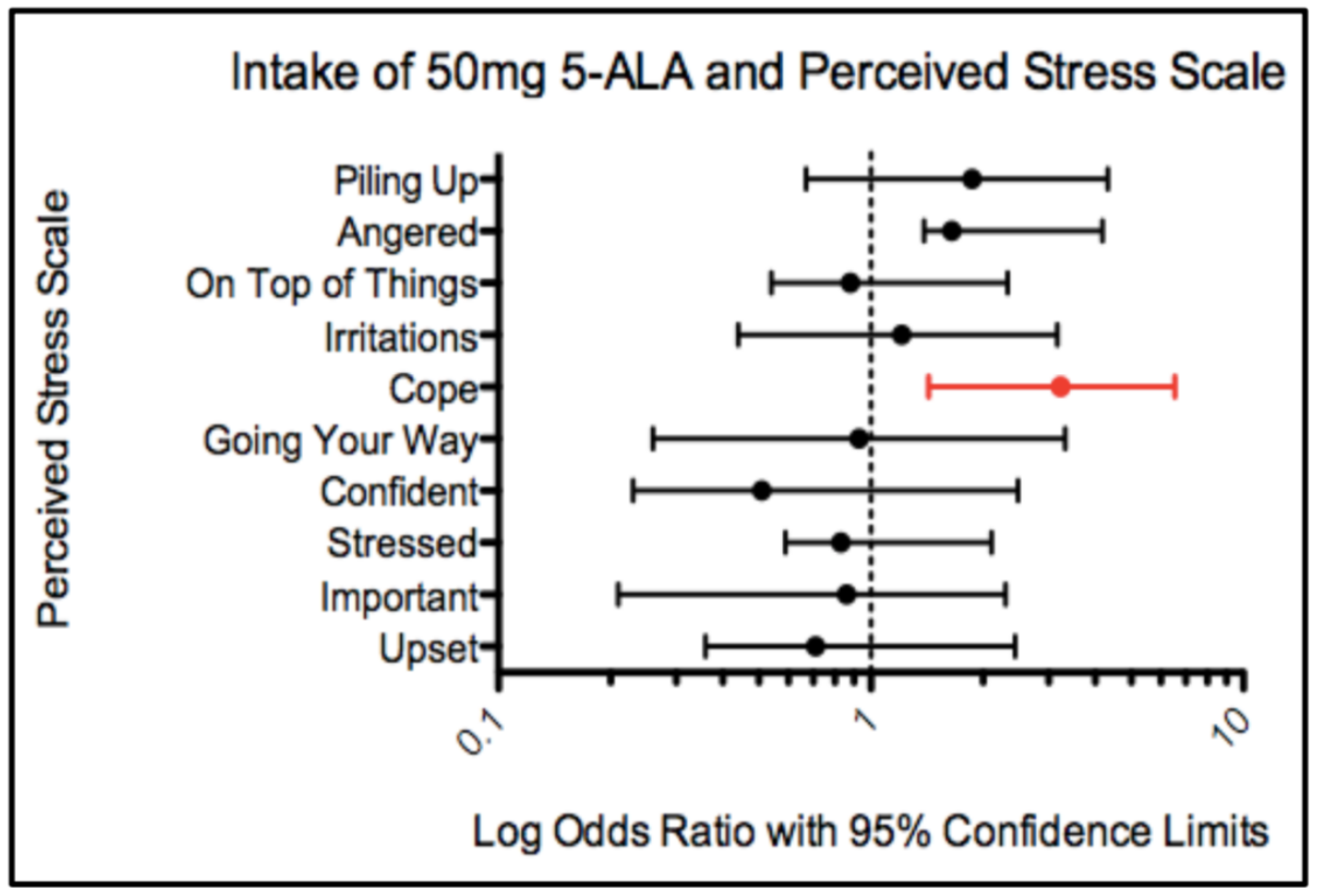
The Perceived Stress Scale (PSS) revealed that coping ability was improved in a group of prediabetic adults (See
Supplementary Materials, PSS Question 6: “How often have you found that you could not cope with all the things that you had to do?”). Compared to the participants’ answers at Week 1 (no 5-ALA), 15 mg and 50 mg of 5-ALA after 12 weeks significantly improved coping ability by 1.5 and 3.2 times, respectively. Diabetes is a stressful, incurable disease that is associated with a higher incidence of depression and anxiety [
22]. For prediabetic adults, the ability to cope with the threat of developing diabetes is important to minimize stress so they can focus on changing their lifestyle.
The mechanism for how 5-ALA improved mood and coping ability is beyond the scope of this project. However, there are a few possible mechanisms for improvement in mood and coping ability as a result of 5-ALA intake. In a previous study using a murine model, researchers found that regular administration of 5-ALA raised brain serotonin levels [
23]. Another study also suggested that 5-ALA might improve mood through its influence on neuroactive substances such as tryptophan, serotonin and melatonin [
10]. Researchers hypothesized that an increase in serotonin levels may correspond with improvements in mood, calmness, irritability, and coping abilities [
23]. In addition, using the same study design and cohort as the current study, Perez and colleagues (2013) reported an improvement in sleep as a result of 5-ALA intake [
10]. The authors suggest that improvement in sleep as a result of 5-ALA intake may be related to a boost in cellular metabolism [
10]. It is well accepted that sleep and mood are closely linked [
24]. Poor sleep is associated with irritability and stress, while adequate sleep is associated with enhanced well-being [
24]. Improvement in sleep in prediabetic adults may increase the energy needed to cope with the possibility of being diagnosed with diabetes. Also, improved sleep may help prediabetic adults feel less alone. A previous study found that people who feel lonely experience more sleep disruptions compared to those who do not feel lonely [
19].
In conclusion, we report that after 12 weeks of taking 5-ALA, self-perception of effort spent, loneliness, and coping ability were improved in a group of prediabetic middle aged and older adults. Improved mood and coping ability may allow prediabetic individuals to overcome the emotional obstacles preventing them from maintaining a healthy lifestyle and ultimately, help them stop the development of diabetes.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}