
Childhood Diarrhea Determinants in Sub-Saharan Africa: A Cross Sectional Study of Tiko-Cameroon

Abstract
:1. Introduction
2. Method and Materials
2.1. Study Design and Setting
2.2. Sample Size and Sampling
2.3. Data Collection and Quality Control
2.4. Data Analysis
2.5. Ethical Consideration
3. Results
Characteristics of Subjects

{kind=link}
{kind=link}
| Characteristics | Health Area | Total (N = 602) | ||
|---|---|---|---|---|
| Holforth (N = 283) | Likomba (N = 166) | Tiko Town (N = 153) | ||
| Mother/Caretaker | ||||
| ≤24 years | 79 (27.9) | 42 (25.5) | 37 (24.2) | 158 (26.3) |
| 25–34 years | 100 (35.3) | 75 (45.5) | 70 (45.8) | 245 (40.8) |
| 35 years and plus | 104 (36.7) | 48 (29.1) | 46 (30.1) | 198 (198) |
| Marital status | ||||
| Single | 41 (14.5) | 21 (12,7) | 20 (13.1) | 82 (13.6) |
| Married | 213 (75.3) | 137 (82.5) | 116 (75.8) | 466 (77.4) |
| Divorce | 03 (1.1) | 01 (0.6) | 02 (1.3) | 06 (1.0) |
| Widow(er) | 26 (9.2) | 07 (4.2) | 15 (1.8) | 48 (8.0) |
| Household head’s Education level | ||||
| No level | 19 (6.7) | 5 (3.0) | 03 (2.0) | 27 (4.5) |
| Primary | 107 (37.8) | 73 (44.0) | 66 (43.1) | 246 (40.9) |
| Secondary | 86 (30.4) | 51 (30.7) | 57 (37.3) | 194 (32.2) |
| Tertiary | 71 (25.1) | 37 (22.3) | 27 (17.6) | 135 (22.4) |
| Socio-professional Category | ||||
| Unskilled worker | 108 (38.2) | 97 (58.4) | 63 (41.2) | 268 (44.5) |
| Skilled worker | 67 (23.7) | 46 (27.7) | 36 (23.5) | 149 (24.8) |
| Senior skill worker | 15 (5.3) | 05 (3.0) | 03 (2.0) | 23 (3.8) |
| Head of an Enterprise | 10 (3.5) | 01 (0.6) | 0 (0) | 11 (1.8) |
| Student | 0 (0) | 02 (1.2) | 01 (0.7) | 3 (0.5) |
| Unemployed | 04 (1.4) | 0 (0) | 03 (2.0) | 7 (1.2) |
| Other | 79 (27.9) | 15 (9.0) | 47 (30.7) | 14 (23.4) |
| No. of Children <10years in the household | ||||
| 1 | 98 (34.6) | 98 (60) | 55 (35.9) | 213 (35.4) |
| 2 | 103 (36.4) | 52 (31.3) | 61 (39.9) | 216 (35.9) |
| 3–4 | 69 (24.4) | 46 (27.7) | 31 (20.3) | 146 (24.3) |
| ≥5 | 13 (4.6) | 8 (4.8) | 06 (3.9) | 27 (4.5) |
| Month average salary (U.S. Dollars) | ||||
| <100 | 101 (35.7) | 46 (27.7) | 41 (26.8) | 188 (31.2) |
| 100–200 | 115 (40.6) | 87 (52.4) | 87 (56.9) | 289 (48.0) |
| 201–1000 | 64 (22.6) | 33 (19.9) | 25 (16.3) | 122 (20.3) |
| >1000 | 3 (1.1) | 0 (0.0) | 0 (0.0) | 3 (0.5) |
| Total | 283 (100) | 166 (100) | 153 (100) | 602 (100) |
| Characteristics | Health Area | Total (N = 602) | ||
|---|---|---|---|---|
| Holforth (N = 283) | Likomba (N = 166) | Tiko Town (N = 153) | ||
| Habitat quality | ||||
| Clean/security zone | 168 (59.4) | 52 (31.3) | 99 (64.7) | 319 (53.0) |
| Dirty | 108 (38.4) | 111 (66.9) | 53 (34.6) | 272 (45.2) |
| Swampy zone | 7 (2.5) | 3 (1.8) | 1 (0.7) | 11 (1.8) |
| Water source for laundry and cooking | ||||
| Tap pipe borne inside the household | 33 (11.7) | 15 (9) | 17 (11.1) | 65 (10.8) |
| Tap pipe borne outside the household | 24 (8.5) | 130 (78.3) | 13 (8.5) | 167 (27.7) |
| Tap public and other collective pipe borne | 3 (1.1) | 13 (7.8) | 9 (5.9) | 25 (4.2) |
| Covered or equipped well sources | 65 (23) | 1 (0.6) | 54 (35.3) | 120 (19.9) |
| Stream/rain water/non-equipped well sources | 158 (55.8) | 7 (4.2) | 60 (39.3) | 225 (37.4) |
| Water source for drinking | ||||
| Tap pipe borne inside/outside the household | 106 (37.4) | 130 (78.3) | 90 (58.8) | 326 (54.2) |
| Tap public pipe borne | 17 (6.0) | 2 (1.2) | 0.0 (0) | 19 (3.2) |
| Mineral water | 65 (23) | 11 (6.6) | 53 (34.6) | 129 (21.4) |
| Other * | 95 (33.6) | 23 (13.9) | 10 (6.6) | 128 (20.7) |
| Duration from Child’s water source | ||||
| 0 mins | 48 (17.0) | 23 (13.9) | 23 (15.0) | 94 (15.6) |
| 1–5 mins | 30 (10.6) | 104 (62.7) | 44 (28.8) | 178 (29.6) |
| 6–15 mins | 50 (17.7) | 21 (12.7) | 24 (15.7) | 95 (15.8) |
| 16–30 mins | 54 (19.1) | 11 (6.6) | 38 (24.8) | 103 (17.1) |
| 31–60 mins | 26 (9.2) | 7 (4.2) | 21 (13.7) | 54 (9.0) |
| >60 mins | 75 (26.5) | 0 (0) | 3 (2.0) | 78 (13) |
| Child’s toilet | ||||
| Portable toilet/bucket | 171 (60.4) | 130 (78.3) | 100 (65.4) | 401 (66.6) |
| Main toilet | 62 (21.9) | 17 (10.2) | 34 (22.2) | 113 (18.8) |
| On soil around the compound/diapers/stream | 50 (17.7) | 19 (11.4) | 19 (12.4) | 88 (14.6) |
| Child’s water storage container | ||||
| Pot/Basin | 31 (11.0) | 52 (31.1) | 33 (21.6) | 116 (19.3) |
| Gallon/bottle | 252 (89) | 114 (68.7) | 120 (78.4) | 486 (80.7) |
| Total | 283 (100) | 166 (100) | 153 (100) | 602 (100) |
| Characteristics | Health Area | Total (N = 602) | ||
|---|---|---|---|---|
| Holforth (N = 283) | Likomba (N = 166) | Tiko Town (N = 153) | ||
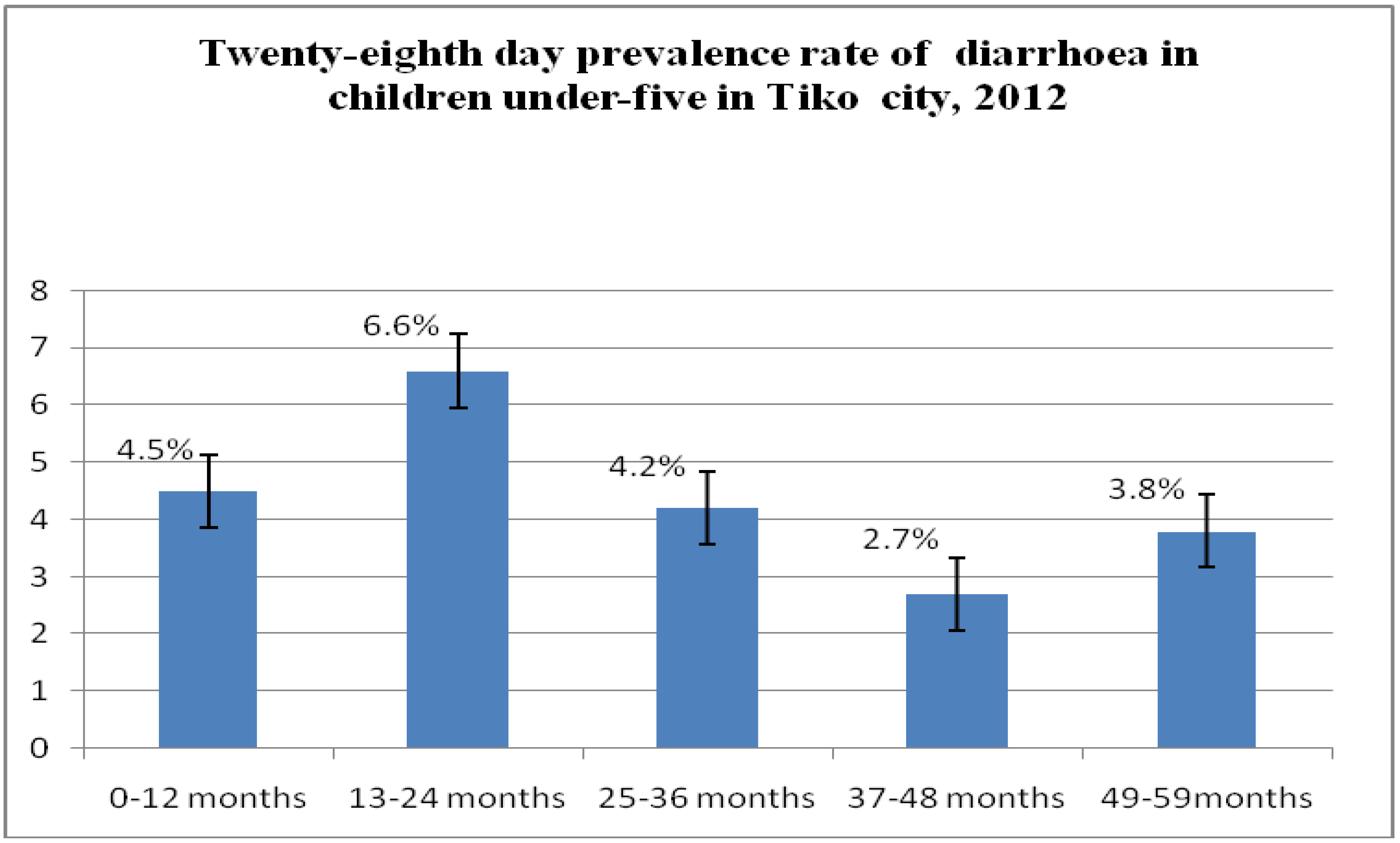
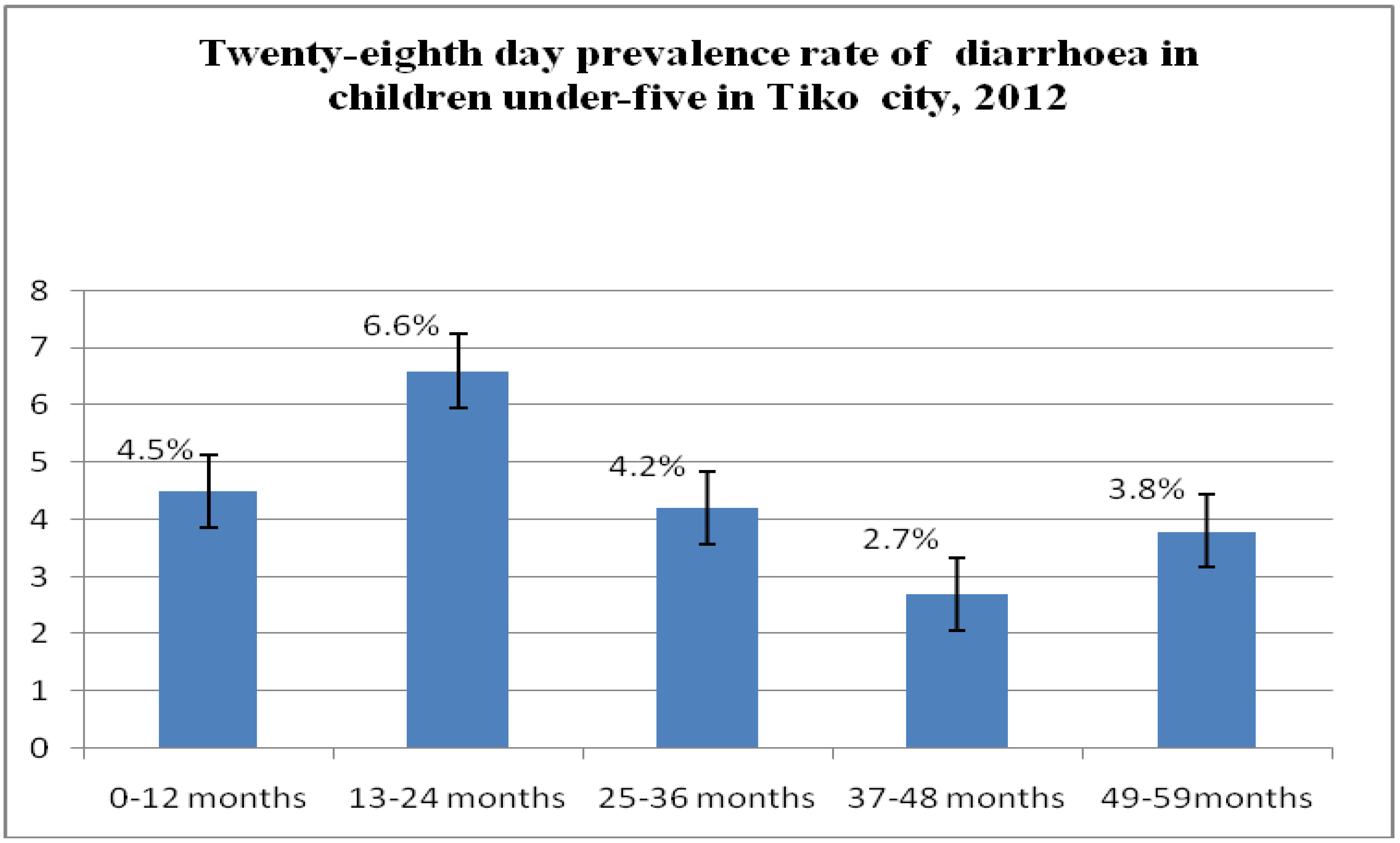
| Watery stool 3–4 times in past Four (4) weeks | ||||
| Yes | 73 (25.8) | 36 (21.7) | 34 (22.2) | 143 (23.8) |
| No | 210 (74.2) | 130 (78.3) | 119 (77.8) | 459 (76.2) |
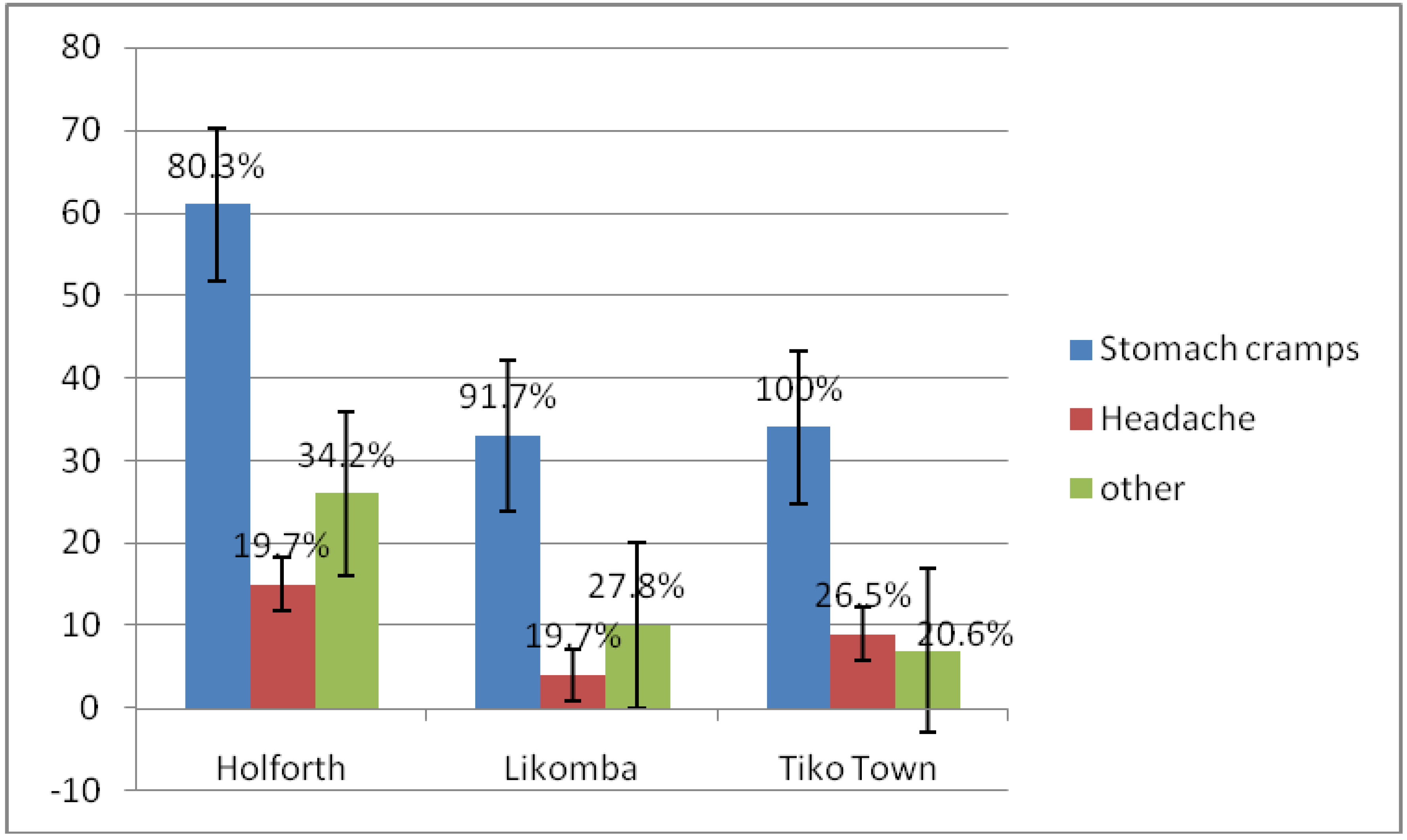
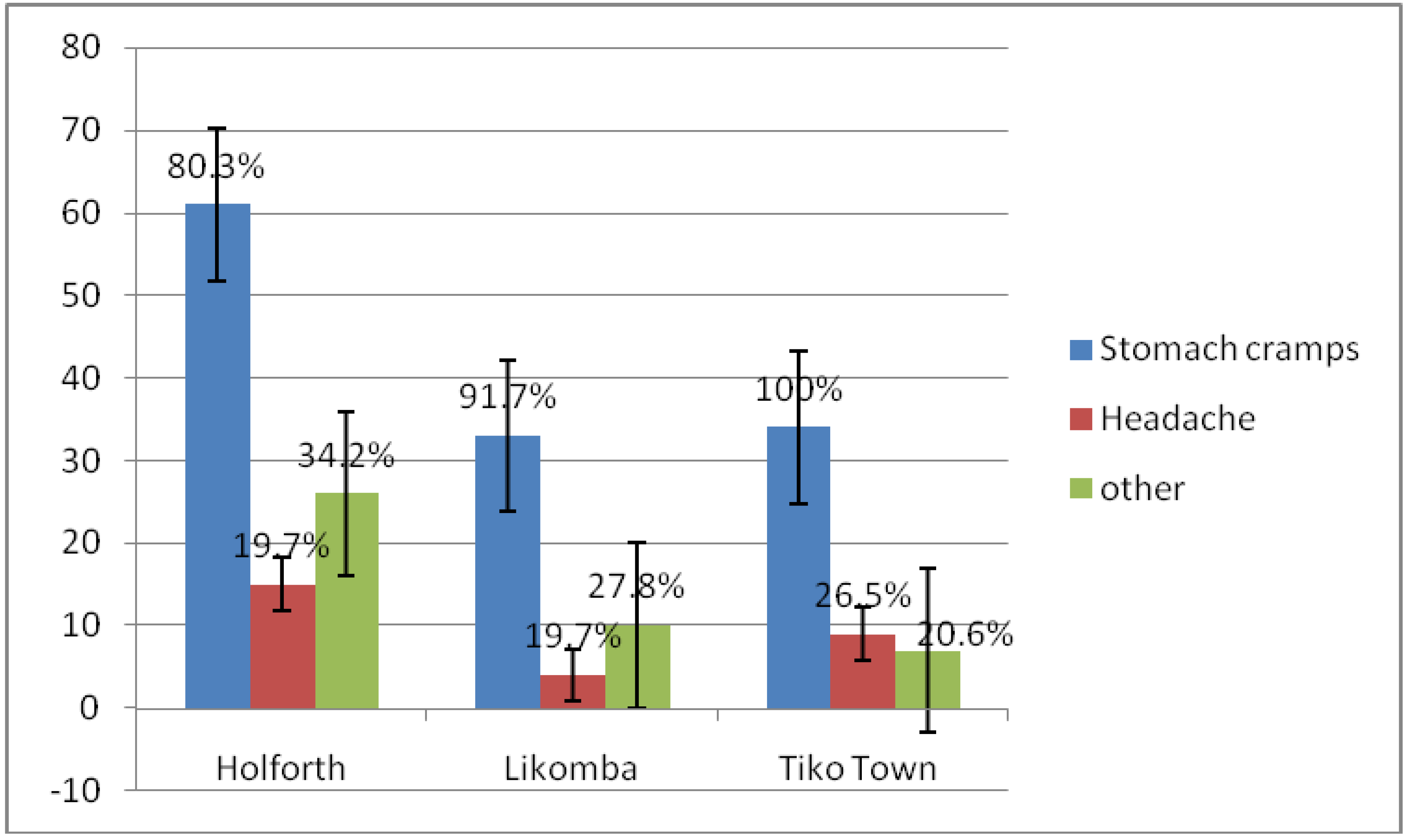
| Symptoms | ||||
| Stomach cramps | 61 (80.3) | 33 (91.7) | 34 (100) | 128 (87.7) |
| Headache | 15 (19.7) | 4 (19.7) | 9 (26.5) | 28 (19.2) |
| Other * | 26 (34.2) | 10 (27.8) | 7 (20.6) | 43 (29.5) |
| Duration of diarrhea | ||||
| 1–2 days | 43 (56.6) | 20 (55.6) | 17 (50.0) | 80 (54.8) |
| 3–5days | 18 (23.7) | 11 (30.6) | 12 (35.3) | 41 (28.1) |
| >5 days | 15 (19.7) | 5 (13.9) | 5 (14.7) | 25 (47.1) |
| Health seeking behavior | ||||
| No treatment | 42 (57.5) | 21 (58.8) | 16 (47.1) | 79 (55.2) |
| Medical center/pharmacy | 18 (24.7) | 11 (30.6) | 09 (26.5) | 38 (26.6) |
| Home care | 08 (11.0) | 03 (08.3) | 07 (20.5) | 18 (12.6) |
| Traditional | 05 (06.8) | 01 (02.8) | 02 (05.9) | 08 (06.0) |
| Characteristics | Proportion | OR | p at 95% CI |
|---|---|---|---|
| Number of children in household | *** | *** | |
| 1 | 23.8 | Ref | p < 0.05 |
| 2 | 37.8 | 1.222 *** | |
| 3–4 | 30.8 | 0.577 | |
| ≥5 | 7.7 | 0.626 | |
| Child’s toilet | *** | *** | p < 0.05 |
| Portable toilet/bucket | 72.0 | Ref | |
| Main toilet | 7.7 | 0.528 * | |
| Other * | 20.3 | 0.194 *** | |
| Child’s water storage container | *** | *** | |
| Pot/Basin | 28.0 | Ref | p < 0.05 |
| Gallon/bottle | 72.0 | 0.429 *** | |
| Do you think your source of Water is safe? | *** | ** | |
| Yes | 63.6 | Ref | p < 0.05 |
| No | 36.4 | 1.849 ** |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
References
- Pond, K.; Rueedi, J.; Pedley, S. Microrisk: Pathogens in Drinking Water Sources; Robens Centre for Public and Environmental Health: Guildford, UK, 2004. [Google Scholar]
- Bryce, J.; Boschi-Pinto, C.; Shibuya, K.; Black, R.E. WHO estimates of the causes of death in children. Lancet 2005, 365, 1147–1152. [Google Scholar] [CrossRef]
- UNICEF/WHO. Diarrhea: Why Children are Still Dying and What Can be Done; World Health Organisation: Geneva, Switzerland, 2009. [Google Scholar]
- Boschi-Pinto, C.; Velebitb, L.; Shibuyac, K. Estimating child mortality due to diarrhea in developing countries. Bull. World Health Organ. 2008, 86, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Kosek, M.; Bern, C.; Guerrant, R.L. The global burden of diarrheal disease, as estimated from studies published between 1992 and 2000. Bull. World Health Organ. 2003, 8, 197–204. [Google Scholar]
- Woldemichael, G. Diarrheal morbidity among young children in Eritrea: Environmental and socioeconomic determinants. J. Health Popul. Nutr. 2001, 19, 83–90. [Google Scholar]
- World Health Organization. Child Health Research Project: Childhood Diarrhea in Sub-Saharan Africa; World Health Organisation: Geneva, Switzerland, 1998. [Google Scholar]
- Black, R.E.; Cousens, S.; Johnson, H.L.; Lawn, J.E.; Rudan, I.; Bassani, D.G.; Jha, P.; Campbell, H.; Walker, C.F.; Cibulskis, R.; et al. Global, regional, and national causes of child mortality in 2008: A systematic analysis. Lancet 2010, 375, 1969–1987. [Google Scholar] [CrossRef]
- Bouree, P. Tropical diarrhea: Consequences of poverty. Presse Med. 2007, 36, 683–685. [Google Scholar] [PubMed]
- Bhandari, N.; Mazumder, S.; Taneja, S.; Dube, B.; Agarwal, R.C.; Mahalanabis, D.; Fontaine, O.; Black, R.E.; Bhan, M.K. Effectiveness of zinc supplementation plus oral rehydration salts compared with oral rehydration salts alone as a treatment for acute diarrhea in a primary care setting: A cluster randomized trial. Pediatrics 2008, 121, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, S.; Bahl, R.; Sharma, P.K.; Kumar, G.T.; Saxena, S.K.; Bhan, M.K. Zinc with oral rehydration therapy reduces stool output and duration of diarrhea in hospitalized children: A randomized controlled trial. J. Pediatr. Gastroenterol. Nutr. 2004, 38, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Fischer Walker, C.L.; Fontaine, O.; Young, M.W.; Black, R.E. Zinc and low osmolarity oral rehydration salts for diarrhea: A renewed call to action. Bull. World Health Organ. 2009, 87, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Ram, P.K.; Choi, M.; Blum, L.S.; Wamae, A.W.; Mintz, E.D.; Bartlett, A.V. Declines in case management of diarrhea among children less than five years old. Bull. World Health Organ. 2008, 86. [Google Scholar] [CrossRef]
- UNICEF & WHO. Ending Preventable Child Deaths from Pneumonia and Diarrhea by 2025: The integrated Global Action Plan for Pneumonia and Diarrhea (GAPPD); World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- United Nations Children’s Fund, UNICEF. Levels and Trends in Child Mortality. Available online: http://www.childinfo.org/files/Child_Mortality_Report_2010.pdf (accessed on 15 April 2013).
- Yongsi, H.B.; Gerard, S.; Thouez, J.P. Health risks associated with faces cleansing methods in Yaounde, Cameroon. Nat. Sci. Soc. 2008, 16, 3–12. [Google Scholar]
- Demographic and Health Surveys. Enquête Démographique et de Santé et à Indicateurs Multiples EDS-MICS 2011; National Institute of Statistics: Yaoundé, Cameroon, 2011. (in French)
- National Institute of Statistics. Bureau Central des Recensements et des Etudes de la Population. La population du Cameroun en 2010; National Institute of Statistics: Yaoundé, Cameroon, 2010.
- Amin, M.E. Social Sciences Research: Conception, Methodology and Analysis Includes Bibliographical References and Indexes; Makerere University Printer: Kampala, Uganda, 2005. [Google Scholar]
- Majowicz, S.E.; Hall, G.; Scallan, E.; Adak, G.K.; Gauci, C.; Jones, T.F.; O’Brien, S.O.; Henao, O.; Sockett, P.N. A common, symptom-based case definition for gastroenteritis. Epidemiol. Infect. 2008, 136, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; Wiley: New York, NY, USA, 2000; pp. 92–95. [Google Scholar]
- Clark, S.; Berrang-Ford, L.; Lwasa, S.; Namanya, D.B.; Edge, V.L.; IHACC Research Team; Harper, S. The burden and determinants of self-reported acute gastrointestinal illness in an indigenous Batwa Pygmy population in Southwestern Uganda. Epidemiol. Infect. 2015, 143, 2287–2298. [Google Scholar] [CrossRef] [PubMed]
- Gaigbe, T.V. Seasonality and cause of infant deaths in Yaounde. Ann. IFORD 1988, 12, 97–126. [Google Scholar]
- Ako, A.A.; Nkeng, G.E.; Takem, G.E. Water quality and occurrence of water-borne diseases in the Douala 4th District, Cameroon. Water Sci. Technol. 2009, 59, 2321–2329. [Google Scholar] [CrossRef] [PubMed]
- Mihrete, T.S.; Alemie, G.A.; Teferra, A.S. Determinants of childhood among under five children in Benishangul Gumuz Regional State, North West Ethiopia. BMC Pediatr. 2014, 14. [Google Scholar] [CrossRef]
- Page, A.; Hustatache, S.; Luquero, F.; Djibo, A.; Laouali, M.; Grais, R. Health care seeking behavior for diarrhea in children under 5 in rural Niger: Results of a cross-sectional survey. BMC Public Health 2011, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilgwan, C.S.; Okolo, S.N. Prevalence of diarrhea disease and risk factors in Jos University Teaching Hospital, Nigeria. Ann. Afr. Med. 2012, 11, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Yongsi, H.B. Pathogenic microorganisms associated with childhood diarrhea in low-and-middle income countries: Case study of Yaoundé—Cameroon. Int. J. Environ. Res. Public Health 2008, 5, 213–229. [Google Scholar] [CrossRef] [PubMed]
- Arif, A.; Naheed, R. Socio-economic determinants of diarrhea morbidity in Pakistan. Acad. Res. Int. 2012, 2, 398–432. [Google Scholar]
- El-Gilany, A.H.; Hammad, S. Epidemiology of diarrheal diseases among children under age 5 years in Dakahlia, Egypt. East. Mediterr. Health J. 2005, 11, 762–775. [Google Scholar] [PubMed]
- Diouf, K.; Tabatabai, P.; Rudolph, J.; Marx, M. Diarrhea prevalence in children under five years of age in rural Burundi: An assessment of social and behavioral factors at the household level. Glob. Health Action 2014, 7. [Google Scholar] [CrossRef]
- Amy Quinn, A.B. Likelihood in Ghanaian Children: A Study of the Association between Diarrhea and Water and Sanitation Infrastructure. Master Thesis, Georgetown Public Policy Institute, Washington, DC, USA, 2009. [Google Scholar]
- Greene, L.E.; Freeman, M.C.; Akoko, D.; Saboori, S.; Moe, C.; Rheingans, R. Impact of a school-based hygiene promotion and sanitation intervention on pupil hand contamination in Western Kenya: A cluster randomized trial. Am. J. Trop. Med. Hyg. 2012, 87, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Ansari, M.; Ibrahim, M.I.; Hassali, M.A.; Shankar, P.R.; Koirala, A.; Thapa, N.J. Mothers’ beliefs and barriers about childhood diarrhea and its management in Morang district, Nepal. BMC Res. Notes 2012, 5. [Google Scholar] [CrossRef] [PubMed]
- Teklemariam, S.; Getaneh, T.; Bekele, F. Environmental determinants of diarrhea morbidity in under-five children, Keffa-Sheka Zone, Southwest Ethiopia. Ethiop. Med. J. 2000, 38, 27–34. [Google Scholar] [PubMed]
- Lindstrand, A.; Bergstrom, S.; Rosling, H.; Rubenson, B.; Stenson, B.; Tylleskar, T. Global Health—An Introductory Textbook; Narayana Press: Copenhagen, Denmark, 2006; p. 325. [Google Scholar]
- Motarjemi, Y.; Käferstein, F.; Moy, G.; Quevedo, F. Contaminated weaning food: A major risk factor for diarrhea and associated malnutrition. Bull. World Health Organ. 1993, 71, 79–92. [Google Scholar] [PubMed]
- Root, G.P.M. Sanitation, community environment and childhood diarrhea in rural Zimbabwe. J. Health Popul. Nutr. 2001, 19, 73–82. [Google Scholar] [PubMed]
- Ghosh, S.; Sengupta, P.G.; Gupta, D.N.; Mondal, S.K.; Goswami, M.; Bhattacharya, S.K.; Sircar, B.K. Maternal knowledge on risk behavioural practices and its association with diarrhea in a rural community of West Bengal, India. J. Commun. Dis. 1998, 30, 251–255. [Google Scholar] [PubMed]
- Nkrumah, B.; Nguah, S.B. Giardia lamblia: A major parasitic cause of childhood diarrhea in patients attending a district hospital in Ghana. Parasit. Vectors 2011, 4. [Google Scholar] [CrossRef] [PubMed]
- Bezatu, M.; Yemane, B.; Alemayehu, W. Prevalence of diarrhea and associated risk factors among children under-five years of age in Eastern Ethiopia: A cross-sectional study. Open J. Prev. Med. 2013, 3, 446–453. [Google Scholar]
- Jalan, J.; Ravallion, M. Does piped water reduce diarrheal disease for children in rural India? J. Econom. 2001, 152, 153–173. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tambe, A.B.; Nzefa, L.D.; Nicoline, N.A. Childhood Diarrhea Determinants in Sub-Saharan Africa: A Cross Sectional Study of Tiko-Cameroon. Challenges 2015, 6, 229-243. https://doi.org/10.3390/challe6020229
Tambe AB, Nzefa LD, Nicoline NA. Childhood Diarrhea Determinants in Sub-Saharan Africa: A Cross Sectional Study of Tiko-Cameroon. Challenges. 2015; 6(2):229-243. https://doi.org/10.3390/challe6020229
Chicago/Turabian StyleTambe, Ayuk Betrand, Leonie Dapi Nzefa, and Nchang Allo Nicoline. 2015. "Childhood Diarrhea Determinants in Sub-Saharan Africa: A Cross Sectional Study of Tiko-Cameroon" Challenges 6, no. 2: 229-243. https://doi.org/10.3390/challe6020229