
Paraneoplastic Syndromes in Hepatocellular Carcinoma, Epidemiology, and Survival: A Retrospective Seven Years Study

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Diagnosis of Hepatocellular Carcinoma
2.3. Laboratory Testing
2.4. Definition of Paraneoplastic Syndromes
2.5. Statistical Analysis
3. Results
3.1. Frequency of Paraneoplastic Syndromes in Individuals with Hepatocellular Carcinoma
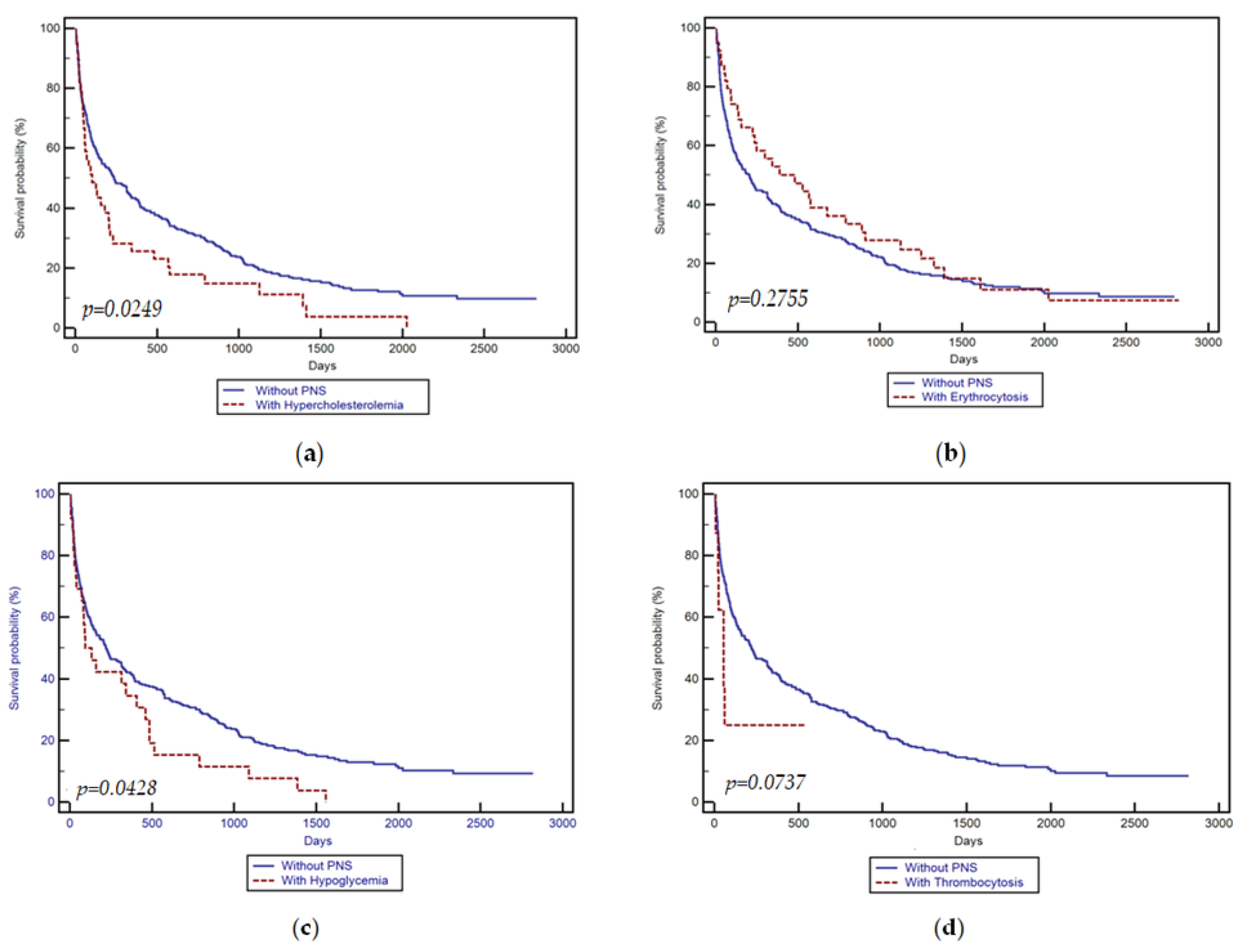
3.2. Patients’ Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, K.A.; Soerjomataram, I. Global burden of primary liver cancer in 2020 and predictions to 2040. J. Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef]
- Rumgay, H.; Ferlay, J.; de Martel, C.; Georges, D.; Ibrahim, A.S.; Zheng, R.; Wei, W.; Lemmens, V.E.P.P.; Soerjomataram, I. Global, regional and national burden of primary liver cancer by subtype. Eur. J. Cancer 2022, 161, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef] [PubMed]
- Sangiovanni, A.; Prati, G.M.; Fasani, P.; Ronchi, G.; Romeo, R.; Manini, M.; Del Ninno, E.; Morabito, A.; Colombo, M. The natural history of compensated cirrhosis due to hepatitis C virus: A 17-year cohort study of 214 patients. Hepatology 2006, 43, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.C.; Hwang, S.J.; Wu, J.C.; Li, C.P.; Hsiao, L.T.; Lai, C.R.; Chiang, J.H.; Lui, W.Y.; Chang, F.Y.; Lee, S.D. Paraneoplastic syndromes in patients with hepatocellular carcinoma in Taiwan. Cancer 1999, 86, 799–804. [Google Scholar] [CrossRef]
- Chang, P.E.; Ong, W.C.; Lui, H.F.; Tan, C.K. Epidemiology and prognosis of paraneoplastic syndromes in hepatocellular carcinoma. ISRN Oncol. 2013, 2013, 684026. [Google Scholar] [CrossRef]
- Huh, U.Y.; Kim, J.H.; Kim, B.H.; Nam, K.D.; Jang, J.Y.; Kim, N.H.; Lee, S.K.; Joo, K.R.; Dong, S.H.; Kim, H.J.; et al. The incidence and clinical significance of paraneoplastic syndromes in patients with hepatocellular carcinoma. Korean J. Hepatol. 2005, 11, 275–283. (In Korean) [Google Scholar]
- Feng, X.-Z.; Zhong, J.-H.; Qi, Y.-P.; Wei, T.; Xiang, B.-D.; Yuan, W.-P. Paraneoplastic Syndrome May be a Favorable Prognostic Factor in Patients with Hepatocellular Carcinoma Following Hepatectomy. World J. Surg. Surg. Res. 2019, 2, 1124. [Google Scholar]
- Bárdos, D.; Molnár, M.J.; Dudás, I.; Tuza, S.; Szijártó, A.; Hahn, O. Polymyositis and rhabdomyolysis caused by hepatocellular carcinoma—Case report and literature review. Ann Med. Surg. 2021, 65, 102269. [Google Scholar] [CrossRef]
- Arguedas, M.R.; McGuire, B.M. Hepatocellular carcinoma presenting with chronic inflammatory demyelinating polyradiculoneuropathy. Dig. Dis. Sci. 2000, 45, 2369–2373. [Google Scholar] [CrossRef]
- Regino, C.A.; López-Montoya, V.; López-Urbano, F.; Alvarez, J.C.; Roman-Gonzalez, A. Paraneoplastic Hypoglycemia in Hepatocarcinoma: Case Report and Literature Review. Cureus 2020, 12, e12013. [Google Scholar] [CrossRef] [PubMed]
- Qu, Q.; Wang, S.; Chen, S.; Zhou, L.; Rui, J.A. Prognostic role and significance of paraneoplastic syndromes in hepatocellular carcinoma. Am. Surg. 2014, 80, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Ong, Y.; Huey, C.W.T.; Shelat, V.G. Paraneoplastic syndromes in hepatocellular carcinoma: A review. Expert. Rev. Gastroenterol. Hepatol. 2022, 16, 449–471. [Google Scholar] [CrossRef] [PubMed]
- Ülger, Y.; Delik, A. Paraneoplastic syndrome frequency and prognostic effect in hepatocellular carcinoma patients. Eur. J. Gastroenterol. Hepatol. 2022, 34, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Al-Showbaki, L.; Toubasi, A.A.; Jaber, D.Z.; Shdifat, M.A.; Al-Maani, N.; Qudah, O.; Fararjeh, F.; Amir, E. Paraneoplastic Cutaneous Manifestations of Hepatocellular Carcinoma. A Systematic Review and Meta-analysis. J. Cancer 2024, 15, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- FactSheetsbyPopulation-Globocan-IARC. n.d. Available online: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx (accessed on 1 February 2024).
- Chu, C.W.; Hwang, S.J.; Luo, J.C.; Tsay, S.H.; Li, C.P.; Chang, F.Y.; Lee, S.D.; Lui, W.Y.; Chiang, J.H. Manifestations of hypercholesterolaemia, hypoglycaemia, erythrocytosis and hypercalcaemia in patients with hepatocellular carcinoma: Report of two cases. J. Gastroenterol. Hepatol. 1999, 14, 807–810. [Google Scholar] [CrossRef]
- Attali, P.; Houssin, D.; Roche, A.; Buffet, C.; Bismuth, H.; Etienne, J.P. Hepatic arterial embolization for malignant hypercalcemia in hepatocellular carcinoma. Dig. Dis. Sci. 1984, 29, 466–469. [Google Scholar] [CrossRef]
- Sohda, T.; Iwata, K.; Hirano, G.; Sakurai, K.; Yokoyama, K.; Morihara, D.; Takeyama, Y.; Irie, M.; Shakado, S.; Sakisaka, S. 3-Hydroxyl-3-methylglutaryl-coenzyme A reductase is up regulated in hepatocellular carcinoma associated with paraneoplastic hypercholesterolemia. Med. Mol. Morphol. 2013, 46, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Reddy, D.N.; Kiat, T.C. Refractory Hypoglycemia Presenting as First Manifestation of Advanced Hepatocellular Carcinoma. ACG Case Rep. J. 2014, 2, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Zini, E.; Glaus, T.M.; Minuto, F.; Arvigo, M.; Hauser, B.; Reusch, C.E. Paraneoplastic hypoglycemia due to an insulin-like growth factor type-II secreting hepatocellular carcinoma in a dog. J. Vet. Intern. Med. 2007, 21, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Sakisaka, S.; Watanabe, M.; Tateishi, H.; Harada, M.; Shakado, S.; Mimura, Y.; Gondo, K.; Yoshitake, M.; Noguchi, K.; Hino, T.; et al. Erythropoietin production in hepatocellular carcinoma cells associated with polycythemia: Immunohistochemical evidence. Hepatology 1993, 18, 1357–1362. [Google Scholar] [CrossRef] [PubMed]
- Trotter, J.F.; Cohn, A.; Grant, R. Erythrocytosis in a patient with hepatocellular carcinoma. J. Clin. Gastroenterol. 2002, 35, 365–366. [Google Scholar] [CrossRef] [PubMed]
- Lok, S.; Kaushansky, K.; Holly, R.D.; Kuijper, J.L.; Lofton-Day, C.E.; Oort, P.J.; Grant, F.J.; Heipel, M.D.; Burkhead, S.K.; Kramer, J.M.; et al. Cloning and expression of murine thrombopoietin cDNA and stimulation of platelet production in vivo. Nature 1994, 369, 565–568. [Google Scholar] [CrossRef]
- Abbas, H.; Hanif, S.; Tariq, H.; Chilimuri, S. Thrombocytosis as a Rare Paraneoplastic Syndrome Occurring in Hepatocellular Carcinoma: A Case Report. Gastroenterol. Res. 2019, 12, 96–99. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | PNS Positive n = 97 | PNS Negative n = 281 | p Value |
|---|---|---|---|
| Mean age (years) | 64.18 ± 8.35 | 66.96 ± 8.83 | 0.0070 |
| Gender (%) | |||
| Females | 17.5% (17) | 33.5% (94) | 0.0043 |
| Males | 82.5% (80) | 66.5% (187) | 0.0043 |
| BMI (kg/m2) | 25.5 (18.6–31.4) | 22.5 (18.4–31.3) | 0.6126 |
| cACLD as the underlying disease (%) | |||
| Yes | 90.7% (88) | 96.1% (270) | 0.0741 |
| No | 9.3% (9) | 3.9% (11) | 0.0741 |
| Child–Pugh grade (%) | |||
| A [5–6] | 44.3% (39/88) | 35.6% (96/270) | 0.1817 |
| B [7–9] | 23.9% (21/88) | 39.3% (106/270) | 0.0127 |
| C [10–15] | 31.8% (28/88) | 25.1% (68/270) | 0.2737 |
| Etiology (%) | |||
| ALD | 22.7% (22) | 18.1% (51) | 0.4004 |
| HBV | 27.8% (27) | 17.1% (48) | 0.0331 |
| HBV + HCV | 0% (0) | 2.2% (6) | 0.3131 |
| HBV + HDV | 3.1% (3) | 5.3% (15) | 0.5469 |
| HCV | 33% (32) | 46.6% (131) | 0.0269 |
| MASLD | 13.4% (13) | 10.7% (30) | 0.5918 |
| Number of HCC lesions | |||
| 1 lesion | 41.2% (40) | 52.7% (148) | 0.0665 |
| 2 lesions | 7.2% (7) | 12.1% (34) | 0.2506 |
| 3 lesions | 0% (0) | 1.1% (3) | 0.7014 |
| Multiple lesions | 45.4% (44) | 29.5% (83) | 0.0063 |
| Infiltrative (diffuse) | 6.2% (6) | 4.6% (13) | 0.7242 |
| HCC stage (BCLC) (%) | |||
| A | 12.4% (12) | 14.9% (42) | 0.6608 |
| B | 27.8% (27) | 33.5% (94) | 0.3622 |
| C | 30.9% (30) | 27.4% (77) | 0.5967 |
| D | 28.9% (28) | 24.2% (68) | 0.4345 |
| PVT (%) | 41.2% (40) | 30.6% (86) | 0.0743 |
| Benign | 2.5% (1/40) | 10.5% (10/86) | 0.2337 |
| Malignant | 97.5% (39/40) | 89.5% (77/86) | 0.2337 |
| Patients’ comorbidities | |||
| Arterial hypertension | 44.3% (43) | 37% (104) | 0.2498 |
| Other cardiac pathology | 22.7% (22) | 21% (59) | 0.8350 |
| Diabetes mellitus | 37.2% (46) | 29.2% (82) | 0.1807 |
| Chronic kidney disease | 8.3% (8) | 4.3% (12) | 0.2112 |
| Laboratory Data | ||||
|---|---|---|---|---|
| Parameters | PNS Positive n = 97 | PNS Negative n = 281 | p Value | Normal Range Values |
| FBG (mg/dL) | 109 (45–269) | 116 (67–477) | 0.0092 | 75–110 md/dL |
| Total cholesterol (mg/dL) | 171 (45–523) | 138 (19–216) | <0.0001 | 0–199 mg/dL |
| Platelet count (×103/µL) | 166 (36–971) | 120 (37–392) | <0.0001 | 150–400 × 103/µL |
| RBC (×106/µL) | 4.55 (2.6–7.2) | 3.92 (1.6–5) | <0.0001 | 4–5.5 × 106/µL |
| AFP levels (ng/mL) | 218.7 (1.6–91,797) | 45.5 (10–100,000) | 0.0117 | 0–7.51 ng/ml |
| PNS | Child–Pugh A | Child–Pugh B | Child–Pugh C | p Value |
|---|---|---|---|---|
| PNS (+), n (%) | 39 (44.3%) | 21 (23.9%) | 28 (31.8%) | p < 0.0001 |
| PNS (−), n (%) | 96 (35.6%) | 106 (39.3%) | 68 (25.1%) | |
| PNS (+) group | ||||
| Hypoglycemia | 5 (12.8%) | 5 (23.8%) | 14 (50%) | |
| Hypercholesterolemia | 20 (51.3%) | 8 (38%) | 10 (35.7%) | |
| Thrombocytosis | 2 (5.1%) | 4 (19.1%) | 3 (10.7%) | |
| Erythrocytosis | 12 (30.8%) | 4 (19.1%) | 1 (3.6%) | |
| PNS | ALD | HBV | HCV | Mixed Etiology | MASLD |
|---|---|---|---|---|---|
| PNS (+), n (%) | 22 (22.7%) | 27 (27.8%) | 32 (33%) | 3 (3.1%) | 13 (13.4%) |
| PNS (−), n (%) | 51 (18.1%) | 48 (17.1%) | 131 (46.6%) | 21 (7.5%) | 30 (10.7%) |
| PNS group | |||||
| Hypoglycemia | 7 (31.8%) | 4 (14.8%) | 9 (28.1%) | 2 (66.7%) | 4 (30.8%) |
| Hypercholesterolemia | 10 (45.5%) | 14 (51.8%) | 12 (37.5%) | 1 (33.3) | 4 (30.8%) |
| Thrombocytosis | 3 (13.6%) | 3 (11.2%) | 4 (12.5%) | 0 | 3 (23.1%) |
| Erythrocytosis | 2 (9.1%) | 6 (22.2%) | 7 (21.9%) | 0 | 2 (15.3%) |
| Variables | OR | 95% CI | p Value |
|---|---|---|---|
| Albuminlevels (g/dL) | 4.21 | 1.56–18.92 | 0.035 |
| PLT values (103/µL) | 1.09 | 1.00–1.22 | 0.086 |
| Total bilirubin (mg/dL) | 1.37 | 1.09–1.88 | 0.026 |
| AFP levels (ng/mL) | 1.71 | 1.11–2.23 | <0.0001 |
| Presence of diabetes mellitus | 2.88 | 1.96–4.31 | 0.038 |
| INR | 1.11 | 0.89–1.98 | 0.541 |
| Child–Pugh C | 1.43 | 0.98–2.23 | 0.063 |
| BCLC stage | 0.94 | 0.79–1.22 | 0.231 |
| MELD | 0.88 | 0.81–1.12 | 0.32 |
| Tumor size < 2 cm | 0.91 | 0.87–1.33 | 0.0013 |
| Tumor size < 5 cm | 2.28 | 1.76–3.02 | <0.0001 |
| PNS+ | Hypoglycemia | Erythrocytosis | Hypercholesterolemia | Thrombocytosis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Albumin levels (g/dL) | 3.61 | 1.96–16.42 | 0.0745 | 2.21 | 1.11–11.92 | 0.231 | 4.55 | 2.11–13.28 | 0.031 | 4.21 | 1.56–18.92 | 0.035 |
| PLT values (103/µL) | 1.06 | 1.00–1.19 | 0.076 | 1.14 | 1.03–1.36 | 0.125 | 1.31 | 1.04–1.32 | 0.066 | 1.28 | 0.90–1.92 | 0.126 |
| Total bilirubin (mg/dL) | 2.31 | 1.92–4.88 | 0.263 | 1.07 | 1.01–1.83 | 0.021 | 1.57 | 1.33–2.88 | 0.082 | 1.70 | 0.98–2.13 | 0.034 |
| AFP levels (ng/mL) | 1.91 | 1.21–2.23 | <0.0001 | 2.11 | 1.18–2.98 | 0.062 | 1.41 | 1.18–2.56 | 0.013 | 2.01 | 1.61–2.83 | 0.138 |
| Presence of Diabetes mellitus | 1.88 | 1.16–3.45 | 0.038 | 1.58 | 1.16–2.21 | 0.038 | 2.45 | 1.56–3.91 | 0.026 | 2.48 | 1.64–2.91 | 0.098 |
| INR | 1.41 | 0.89–1.68 | 0.671 | 1.01 | 0.59–1.34 | 0.741 | 1.13 | 0.59–1.48 | 0.0944 | 1.18 | 0.90–1.82 | 0.431 |
| Child–Pugh C | 1.23 | 1.08–2.43 | 0.163 | 1.52 | 1.11–2.36 | 0.083 | 1.43 | 1.28–1.88 | 0.098 | 1.53 | 1.13–1.94 | 0.103 |
| BCLC stage | 0.89 | 0.69–1.11 | 0.411 | 0.92 | 0.81–1.33 | 0.201 | 0.94 | 0.59–1.72 | 0.093 | 0.98 | 0.89–1.67 | 0.181 |
| MELD | 0.98 | 0.84–1.11 | 0.32 | 1.07 | 0.73–1.52 | 0.212 | 1.16 | 0.81–1.63 | 0.412 | 0.91 | 0.61–1.62 | 0.323 |
| Tumor size < 5 cm | 1.98 | 1.46–3.12 | 0.0531 | 2.18 | 1.91–3.43 | 0.0712 | 2.59 | 1.86–3.91 | <0.0001 | 2.63 | 1.99–4.02 | <0.0001 |
| Survival Time (Days) | Subjects without Paraneoplastic Syndromes n = 281 | Subjects with Paraneoplastic Syndromes n = 97 | ||
|---|---|---|---|---|
| Survival Proportion | Standard Error | Survival Proportion | Standard Error | |
| 30 days | 0.794 | 0.0241 | 0.814 | 0.0395 |
| 60 days | 0.719 | 0.0268 | 0.670 | 0.0477 |
| 90 days | 0.654 | 0.2840 | 0.576 | 0.0530 |
| 183 days | 0.539 | 0.0298 | 0.481 | 0.0510 |
| 365 days | 0.436 | 0.0300 | 0.365 | 0.0454 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burciu, C.; Sirli, R.; Bende, R.; Vuletici, D.; Miutescu, B.; Moga, T.; Bende, F.; Popescu, A.; Sporea, I.; Koppandi, O.; et al. Paraneoplastic Syndromes in Hepatocellular Carcinoma, Epidemiology, and Survival: A Retrospective Seven Years Study. Medicina 2024, 60, 552. https://doi.org/10.3390/medicina60040552
Burciu C, Sirli R, Bende R, Vuletici D, Miutescu B, Moga T, Bende F, Popescu A, Sporea I, Koppandi O, et al. Paraneoplastic Syndromes in Hepatocellular Carcinoma, Epidemiology, and Survival: A Retrospective Seven Years Study. Medicina. 2024; 60(4):552. https://doi.org/10.3390/medicina60040552
Chicago/Turabian StyleBurciu, Calin, Roxana Sirli, Renata Bende, Deiana Vuletici, Bogdan Miutescu, Tudor Moga, Felix Bende, Alina Popescu, Ioan Sporea, Oana Koppandi, and et al. 2024. "Paraneoplastic Syndromes in Hepatocellular Carcinoma, Epidemiology, and Survival: A Retrospective Seven Years Study" Medicina 60, no. 4: 552. https://doi.org/10.3390/medicina60040552