

Treatment of Osteoporosis in Men on Androgen Deprivation Therapy in Japan
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Data Collection
3. Results
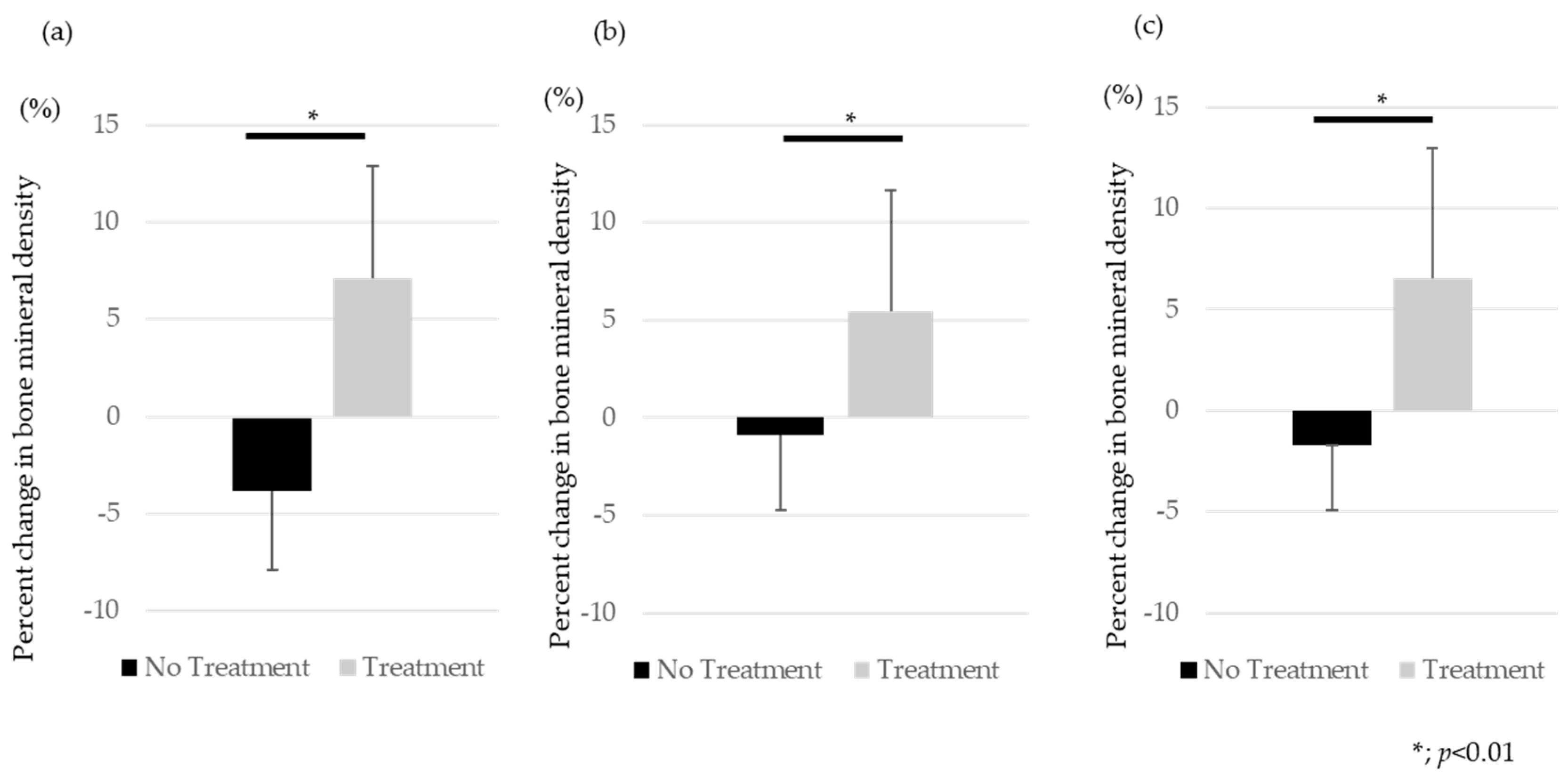
3.1. Change in BMD
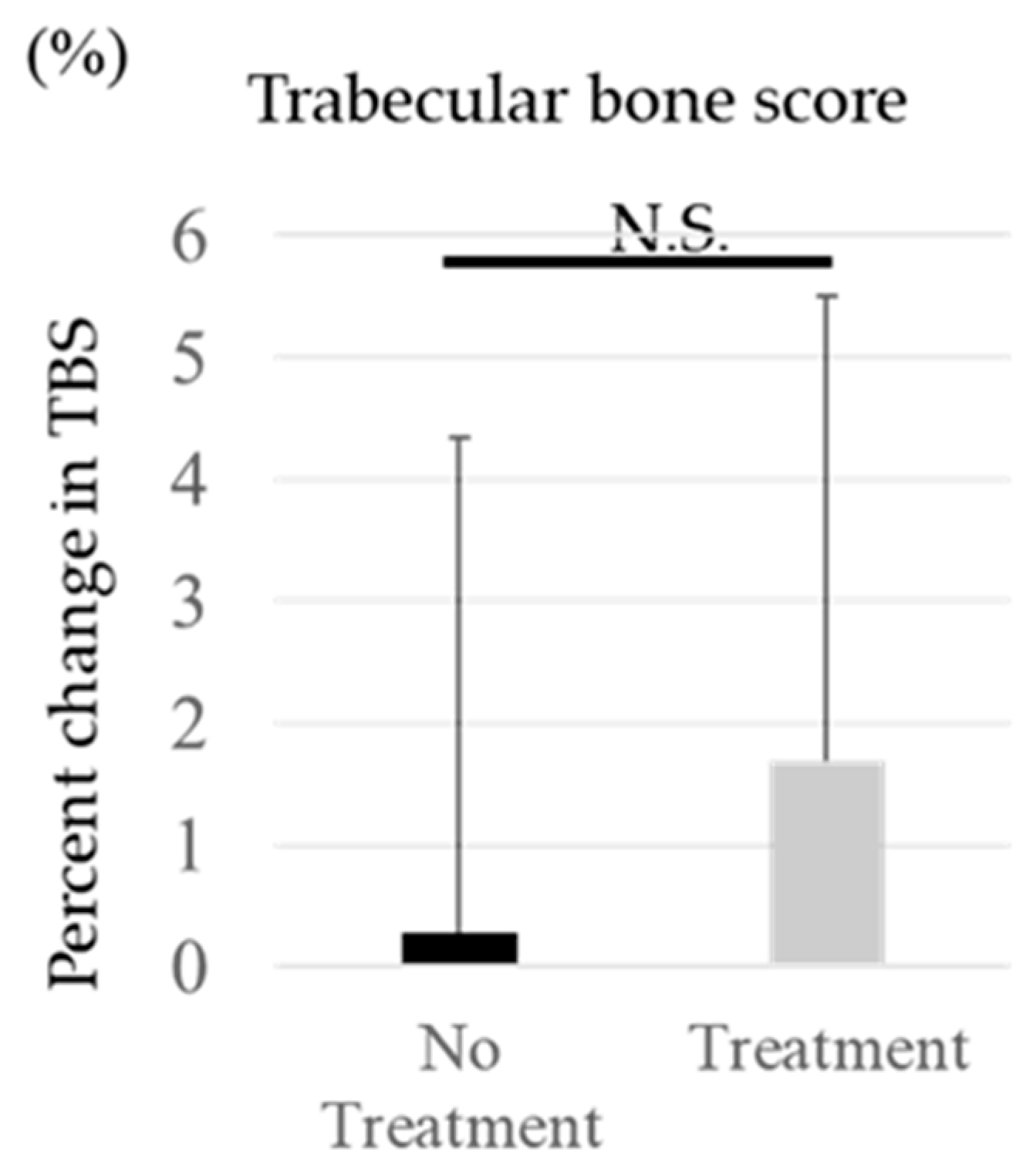
3.2. Change in TBS
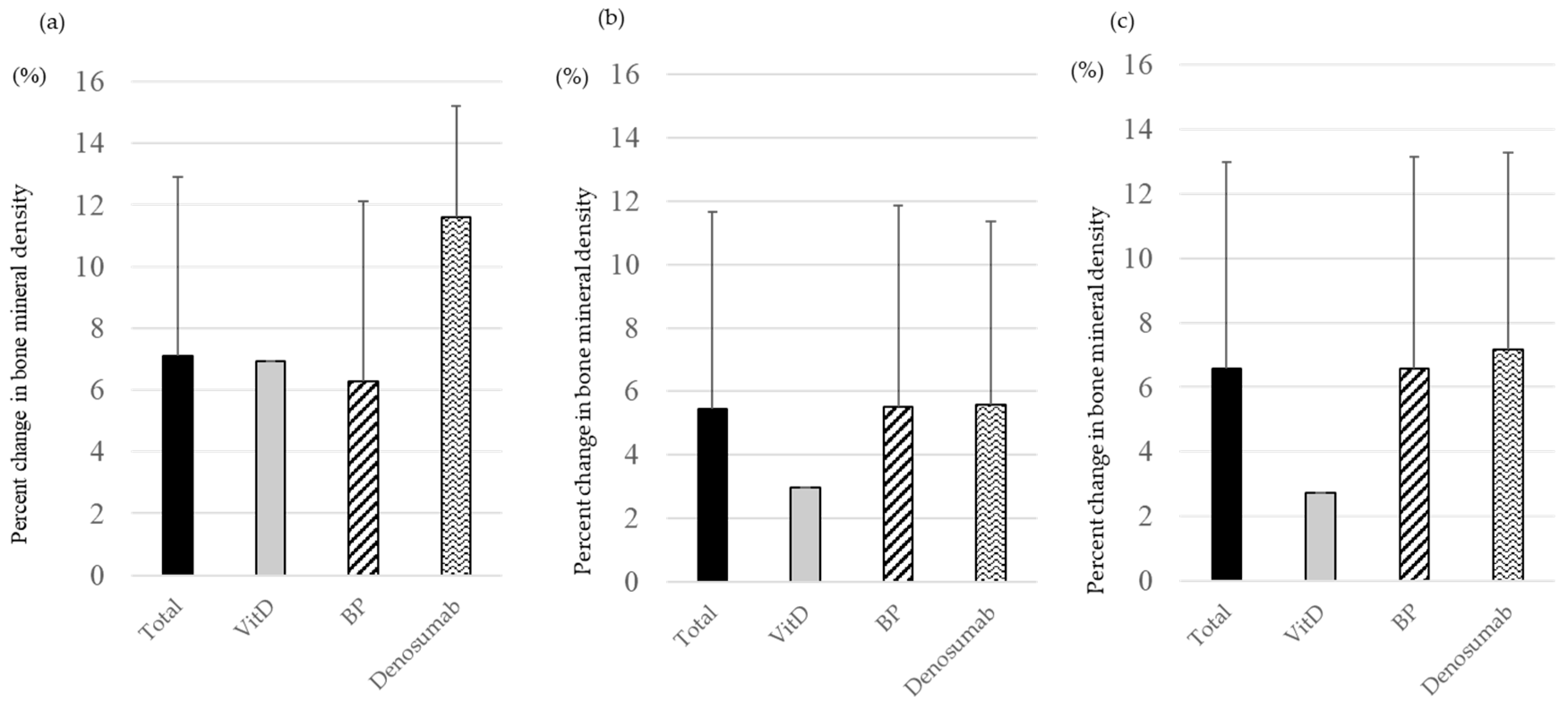
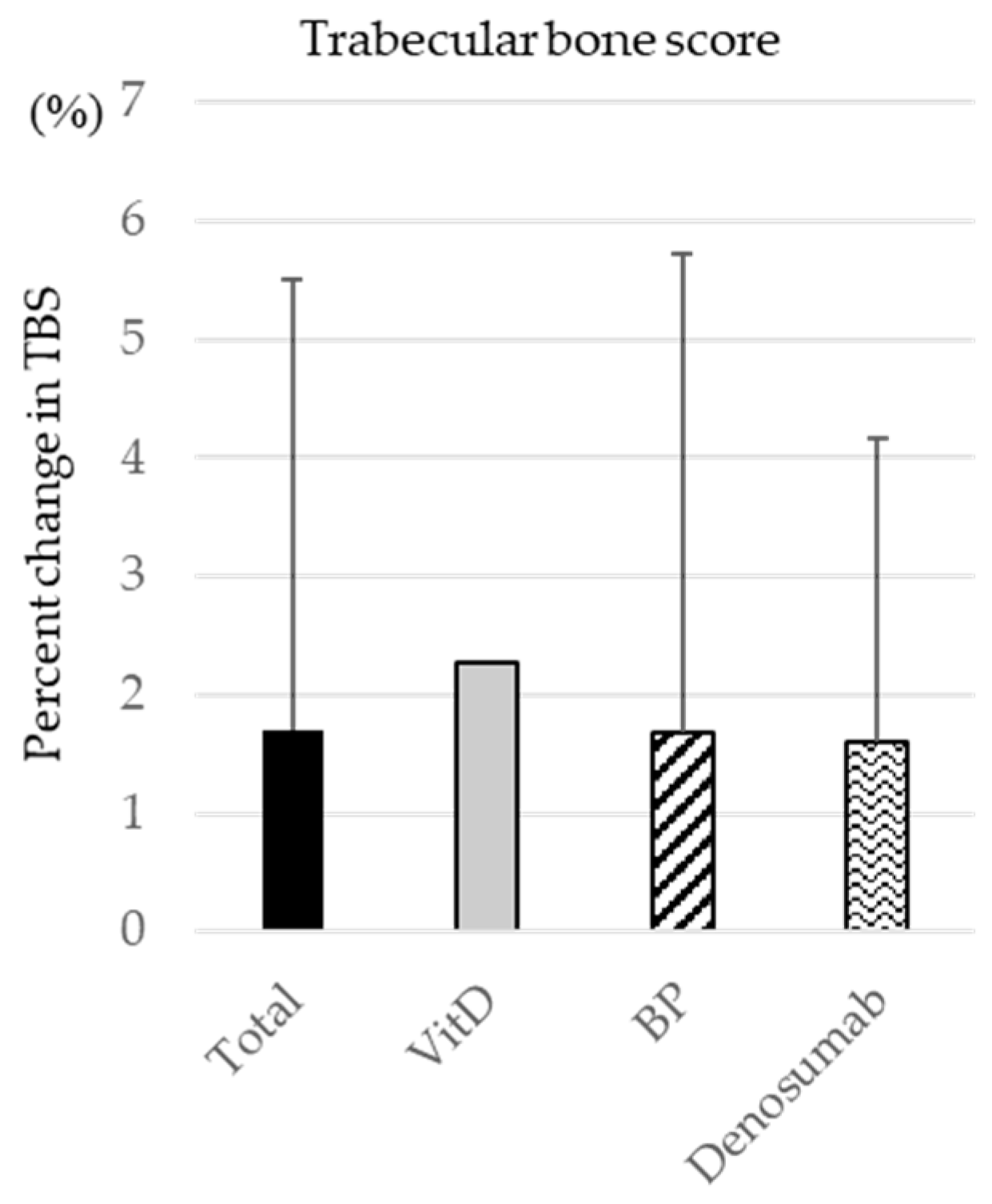
3.3. Change in BMD and TBS by Drug Type
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yanagisawa, T.; Rajwa, P.; Thibault, C.; Gandaglia, G.; Mori, K.; Kawada, T.; Fukuokaya, W.; Shim, S.R.; Mostafaei, H.; Motlagh, R.S.; et al. Androgen Receptor Signaling Inhibitors in Addition to Docetaxel with Androgen Deprivation Therapy for Metastatic Hormone-sensitive Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2022, 82, 584–598. [Google Scholar] [CrossRef]
- Sharifi, N.; Gulley, J.L.; Dahut, W.L. Androgen deprivation therapy for prostate cancer. JAMA 2005, 294, 238–244. [Google Scholar] [CrossRef]
- Isbarn, H.; Boccon-Gibod, L.; Carroll, P.R.; Montorsi, F.; Schulman, C.; Smith, M.R.; Sternberg, C.N.; Studer, U.E. Androgen deprivation therapy for the treatment of prostate cancer: Consider both benefits and risks. Eur. Urol. 2009, 55, 62–75. [Google Scholar] [CrossRef]
- Shahinian, V.B.; Kuo, Y.F.; Freeman, J.L.; Goodwin, J.S. Risk of fracture after androgen deprivation for prostate cancer. N. Engl. J. Med. 2005, 352, 154–164. [Google Scholar] [CrossRef]
- Berruti, A.; Dogliotti, L.; Terrone, C.; Cerutti, S.; Isaia, G.; Tarabuzzi, R.; Reimondo, G.; Mari, M.; Ardissone, P.; De Luca, S.; et al. Changes in bone mineral density, lean body mass and fat content as measured by dual energy x-ray absorptiometry in patients with prostate cancer without apparent bone metastases given androgen deprivation therapy. J. Urol. 2002, 167, 2361–2367; discussion 7. [Google Scholar] [CrossRef]
- Morote, J.; Morin, J.P.; Orsola, A.; Abascal, J.M.; Salvador, C.; Trilla, E.; Raventos, C.X.; Cecchini, L.; Encabo, G.; Reventos, J. Prevalence of osteoporosis during long-term androgen deprivation therapy in patients with prostate cancer. Urology 2007, 69, 500–504. [Google Scholar] [CrossRef]
- Takahashi, S. Management of cancer treatment-induced bone loss (CTIBL) in patients with breast cancer or prostate cancer. J. Bone Miner. Metab. 2023, 41, 307–316. [Google Scholar] [CrossRef]
- Meng, M.V.; Grossfeld, G.D.; Sadetsky, N.; Mehta, S.S.; Lubeck, D.P.; Carroll, P.R. Contemporary patterns of androgen deprivation therapy use for newly diagnosed prostate cancer. Urology 2002, 60 (Suppl. S1), 7–11; discussion 11–12. [Google Scholar]
- Yoshimura, N.; Iidaka, T.; Horii, C.; Muraki, S.; Oka, H.; Kawaguchi, H.; Nakamura, K.; Akune, T.; Tanaka, S. Trends in osteoporosis prevalence over a 10-year period in Japan: The ROAD study 2005–2015. J. Bone Miner. Metab. 2022, 40, 829–838. [Google Scholar] [CrossRef]
- Hernlund, E.; Svedbom, A.; Ivergård, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jönsson, B.K.; Kanis, J.A. Osteoporosis in the European Union: Medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch. Osteoporos. 2013, 8, 136. [Google Scholar] [CrossRef] [PubMed]
- Wright, N.C.; Looker, A.C.; Saag, K.G.; Curtis, J.R.; Delzell, E.S.; Randall, S.; Dawson-Hughes, B. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J. Bone Miner. Res. 2014, 29, 2520–2526. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.C.; Leslie, W.D.; Resch, H.; Lamy, O.; Lesnyak, O.; Binkley, N.; McCloskey, E.V.; A Kanis, J.; Bilezikian, J.P. Trabecular bone score: A noninvasive analytical method based upon the DXA image. J. Bone Miner. Res. 2014, 29, 518–530. [Google Scholar] [CrossRef] [PubMed]
- Russell, N.; Grossmann, M. Management of bone and metabolic effects of androgen deprivation therapy. Urol. Oncol. 2021, 39, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, H.; Daneshmand, S. Androgen deprivation therapy for prostate cancer: Long-term safety and patient outcomes. Patient Relat. Outcome Meas. 2014, 5, 63–70. [Google Scholar]
- Greenspan, S.L.; Coates, P.; Sereika, S.M.; Nelson, J.B.; Trump, D.L.; Resnick, N.M. Bone loss after initiation of androgen deprivation therapy in patients with prostate cancer. J. Clin. Endocrinol. Metab. 2005, 90, 6410–6417. [Google Scholar] [CrossRef] [PubMed]
- van Oostwaard, M.M.; van den Bergh, J.P.; van de Wouw, Y.; Janssen-Heijnen, M.; de Jong, M.; Wyers, C.E. High prevalence of vertebral fractures at initiation of androgen deprivation therapy for prostate cancer. J. Bone Oncol. 2023, 38, 100465. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Jeon, Y.J.; Bak, J.K.; Yoo, B.N.; Park, J.W.; Ha, Y.C.; Lee, Y.K. Association of Androgen Deprivation Therapy with Osteoporotic Fracture in Patients with Prostate Cancer with Low Tumor Burden Using a Retrospective Population-Based Propensity-Score-Matched Cohort. Cancers 2023, 15, 2822. [Google Scholar] [CrossRef] [PubMed]
- Oefelein, M.G.; Ricchiuti, V.; Conrad, W.; Resnick, M.I. Skeletal fractures negatively correlate with overall survival in men with prostate cancer. J. Urol. 2002, 168, 1005–1007. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, W.; Huang, X.; Lin, R.; Wu, J.; Zhang, X. Effect of Diphosphonates on Bone Mineral Density in Men Receiving Androgen Deprivation Therapy for Prostate Cancer. Clin. Genitourin. Cancer 2018, 16, e1243–e1250. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, S.L.; Nelson, J.B.; Trump, D.L.; Resnick, N.M. Effect of once-weekly oral alendronate on bone loss in men receiving androgen deprivation therapy for prostate cancer: A randomized trial. Ann. Intern. Med. 2007, 146, 416–424. [Google Scholar] [CrossRef]
- Bruder, J.M.; Ma, J.Z.; Wing, N.; Basler, J.; Katselnik, D. Effects of alendronate on bone mineral density in men with prostate cancer treated with androgen deprivation therapy. J. Clin. Densitom. 2006, 9, 431–437. [Google Scholar] [CrossRef]
- Ishizaka, K.; Machida, T.; Kobayashi, S.; Kanbe, N.; Kitahara, S.; Yoshida, K. Preventive effect of risedronate on bone loss in men receiving androgen-deprivation therapy for prostate cancer. Int. J. Urol. 2007, 14, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Gleason, D.M.; Murray, R.; Tchekmedyian, S.; Venner, P.; Lacombe, L.; Chin, J.L.; Vinholes, J.J.; Goas, J.A.; Zheng, M. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer. J. Natl. Cancer Inst. 2004, 96, 879–882. [Google Scholar] [CrossRef]
- Smith, M.R.; Egerdie, B.; Toriz, N.H.; Feldman, R.; Tammela, T.L.; Saad, F.; Heracek, J.; Szwedowski, M.; Ke, C.; Kupic, A.; et al. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N. Engl. J. Med. 2009, 361, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Morton, R.A.; Barnette, K.G.; Sieber, P.R.; Malkowicz, S.B.; Rodriguez, D.; Hancock, M.L.; Steiner, M.S. Toremifene to reduce fracture risk in men receiving androgen deprivation therapy for prostate cancer. J. Urol. 2013, 189 (Suppl. Sl), S45–S50. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Fallon, M.A.; Lee, H.; Finkelstein, J.S. Raloxifene to prevent gonadotropin-releasing hormone agonist-induced bone loss in men with prostate cancer: A randomized controlled trial. J. Clin. Endocrinol. Metab. 2004, 89, 3841–3846. [Google Scholar] [CrossRef]
- Tang, H.; Di, W.; Qi, H.; Liu, J.; Yu, J.; Cai, J.; Lai, B.; Ding, G.; Cheng, P. Age-Related Changes in Trabecular Bone Score and Bone Mineral Density in Chinese Men: A Cross-Sectional and Longitudinal Study. Clin. Interv. Aging 2022, 17, 429–437. [Google Scholar] [CrossRef]
- Hans, D.; Goertzen, A.L.; Krieg, M.A.; Leslie, W.D. Bone microarchitecture assessed by TBS predicts osteoporotic fractures independent of bone density: The Manitoba study. J. Bone Miner. Res. 2011, 26, 2762–2769. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment (n = 33) | No Treatment (n = 33) | p Value | |
|---|---|---|---|
| Age (y.o.) | 76.2 ± 7.7 | 76.0 ± 7.6 | 0.203 |
| BMI (kg/m2) | 22.4 ± 3.3 | 23.4 ± 4.0 | 0.226 |
| Bone Metabolic Markers | |||
| TRACP 5b | 480.3 ± 170.3 | 457.5 ± 224.0 | 0.246 |
| P1NP | 58.9 ± 16.1 | 56.1 ± 18.5 | 0.086 |
| BAP | 15.6 ± 7.0 | 15.1 ± 8.7 | 0.062 |
| 25(OH)D | 17.5 ± 6.5 | 24.3 ± 8.3 | 0.016 * |
| No Treatment | Treatment | ||||
|---|---|---|---|---|---|
| Before Follow Up | 1 Year Later | Before Treatment | 1 Year Later | ||
| BMD (g/cm2) | Lumber spine | 1.025 ± 0.170 | 0.982 ± 0.162 | 0.799 ± 0.169 | 0.845 ± 0.171 |
| Femoral neck | 0.693 ± 0.087 | 0.683 ± 0.081 | 0.555 ± 0.066 | 0.564 ± 0.067 | |
| Total hip | 0.878 ± 0.092 | 0.859 ± 0.084 | 0.695 ± 0.084 | 0.707 ± 0.086 | |
| Trabecular bone score | 1.310 ± 0.063 | 1.313 ± 0.072 | 1.242 ± 0.074 | 1.263 ± 0.080 | |
| Bone Mineral Density (g/cm2) | TBS | |||||||
|---|---|---|---|---|---|---|---|---|
| Lumber Spine | Femoral Neck | Total Hip | ||||||
| Before Treatment | 1 Year Later | Before Treatment | 1 Year Later | Before Treatment | 1 Year Later | Before Treatment | 1 Year Later | |
| Vitamin D | 0.759 | 0.778 | 0.522 | 0.543 | 0.648 | 0.655 | 1.272 | 1.301 |
| Bisphosphonate | 0.829 ± 0.150 | 0.866 ± 0.160 | 0.568 ± 0.064 | 0.577 ± 0.064 | 0.712 ± 0.078 | 0.724 ± 0.079 | 1.253 ± 0.070 | 1.274 ± 0.079 |
| Denosumab | 0.644 ± 0.179 | 0.740 ± 0.183 | 0.492 ± 0.036 | 0.493 ± 0.031 | 0.614 ± 0.067 | 0.621 ± 0.071 | 1.181 ± 0.064 | 1.199 ± 0.053 |
| Total | 0.799 ± 0.169 | 0.845 ± 0.171 | 0.555 ± 0.066 | 0.564 ± 0.067 | 0.695 ± 0.084 | 0.707 ± 0.086 | 1.242 ± 0.074 | 1.263 ± 0.080 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimoto, H.; Inui, A.; Mifune, Y.; Yamaura, K.; Bando, Y.; Okamura, Y.; Hara, T.; Terakawa, T.; Kuroda, R. Treatment of Osteoporosis in Men on Androgen Deprivation Therapy in Japan. Medicina 2024, 60, 551. https://doi.org/10.3390/medicina60040551
Nishimoto H, Inui A, Mifune Y, Yamaura K, Bando Y, Okamura Y, Hara T, Terakawa T, Kuroda R. Treatment of Osteoporosis in Men on Androgen Deprivation Therapy in Japan. Medicina. 2024; 60(4):551. https://doi.org/10.3390/medicina60040551
Chicago/Turabian StyleNishimoto, Hanako, Atsuyuki Inui, Yutaka Mifune, Kohei Yamaura, Yukari Bando, Yasuyoshi Okamura, Takuto Hara, Tomoaki Terakawa, and Ryosuke Kuroda. 2024. "Treatment of Osteoporosis in Men on Androgen Deprivation Therapy in Japan" Medicina 60, no. 4: 551. https://doi.org/10.3390/medicina60040551