
GSTM1 and GSTP1 Polymorphisms Affect Outcome in Colorectal Adenocarcinoma

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Patient Selection
2.2. Study Design
2.3. Peripheral Blood Collection and Assay
2.4. Statistical Analysis
3. Results
3.1. GST Genotypes and Survival
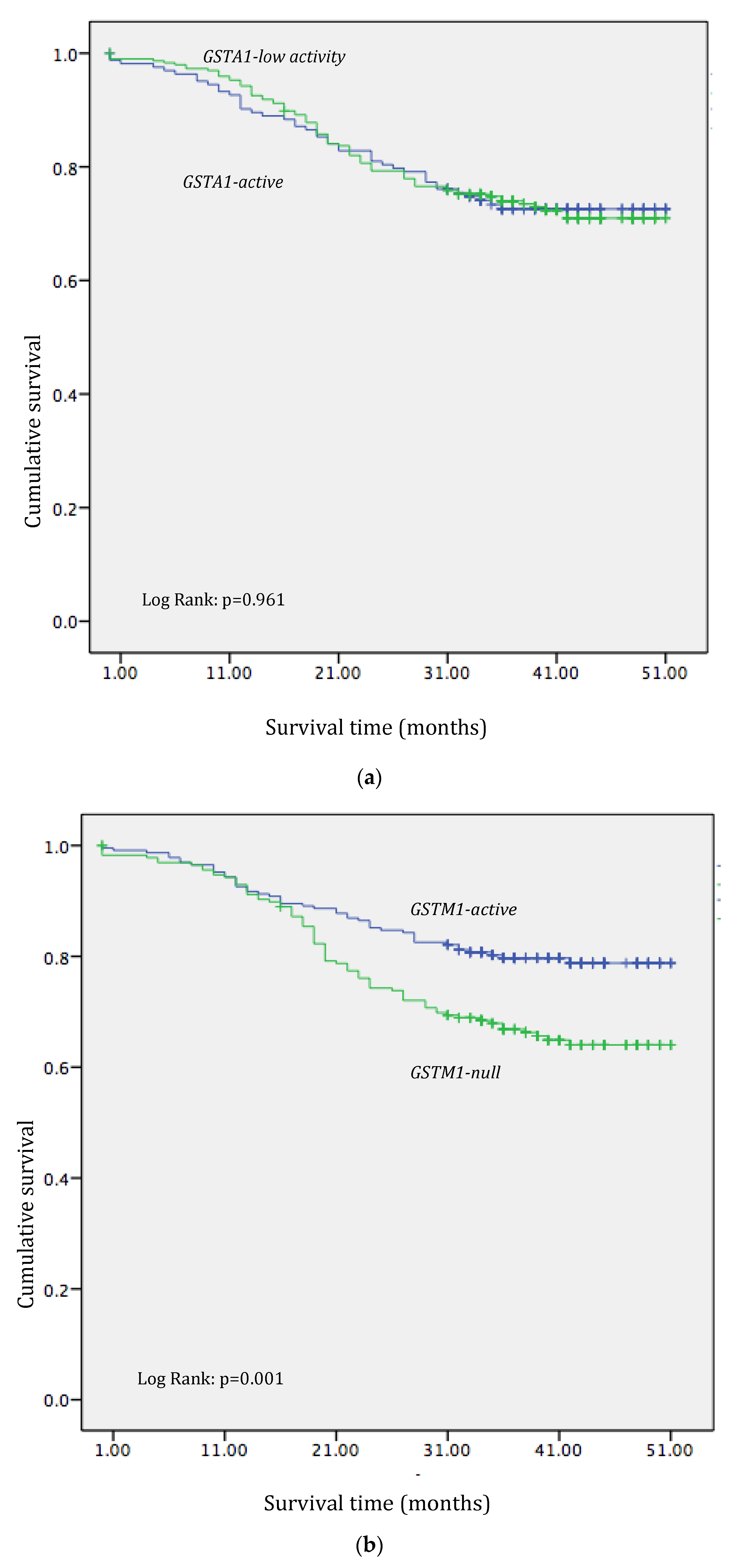
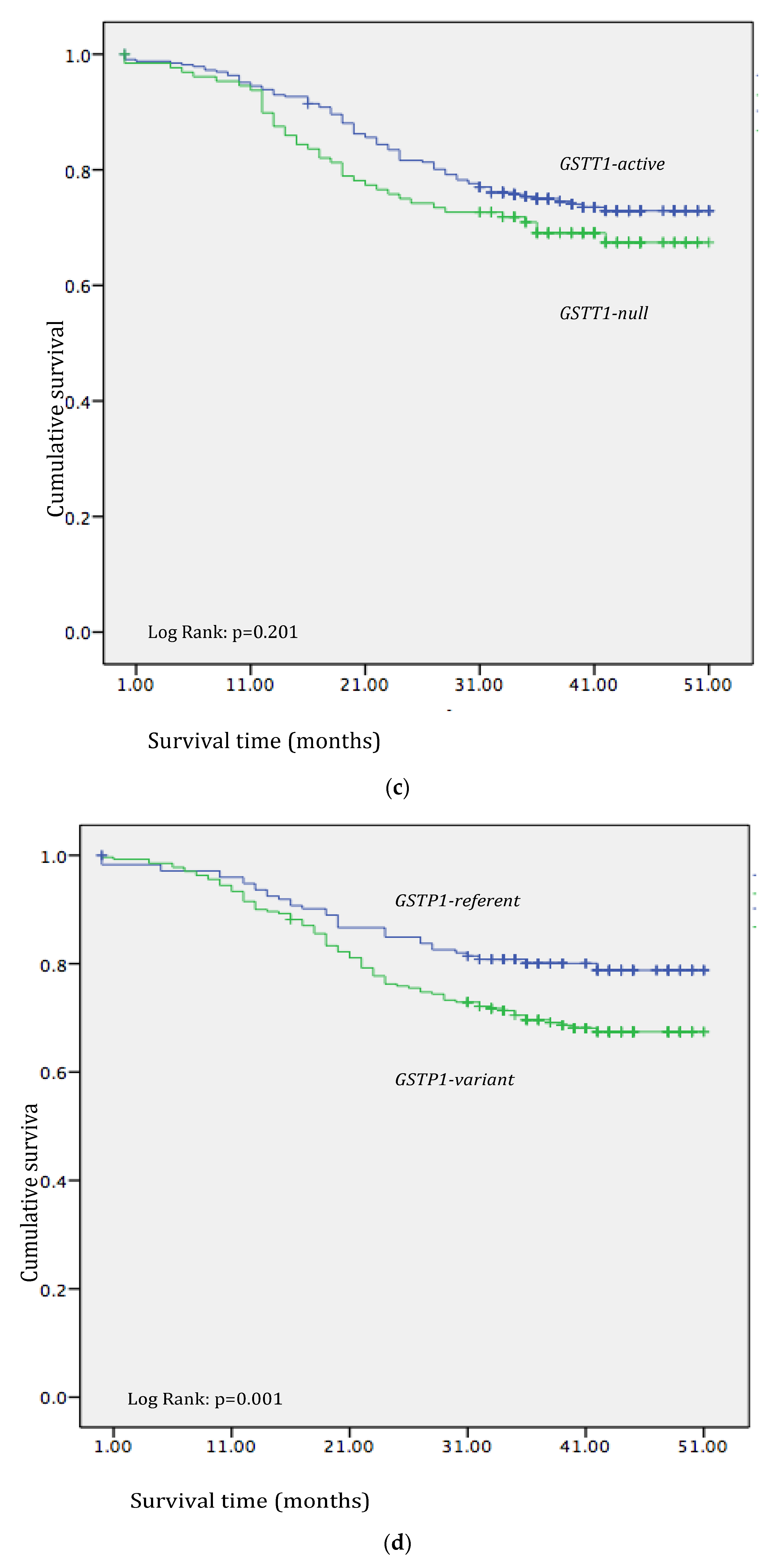
3.2. Effect of GST Polymorphisms on CRC Patients’ Overall Survival
3.3. The Relevance of GST Polymorphisms in the Overall Survival of CRC Patients
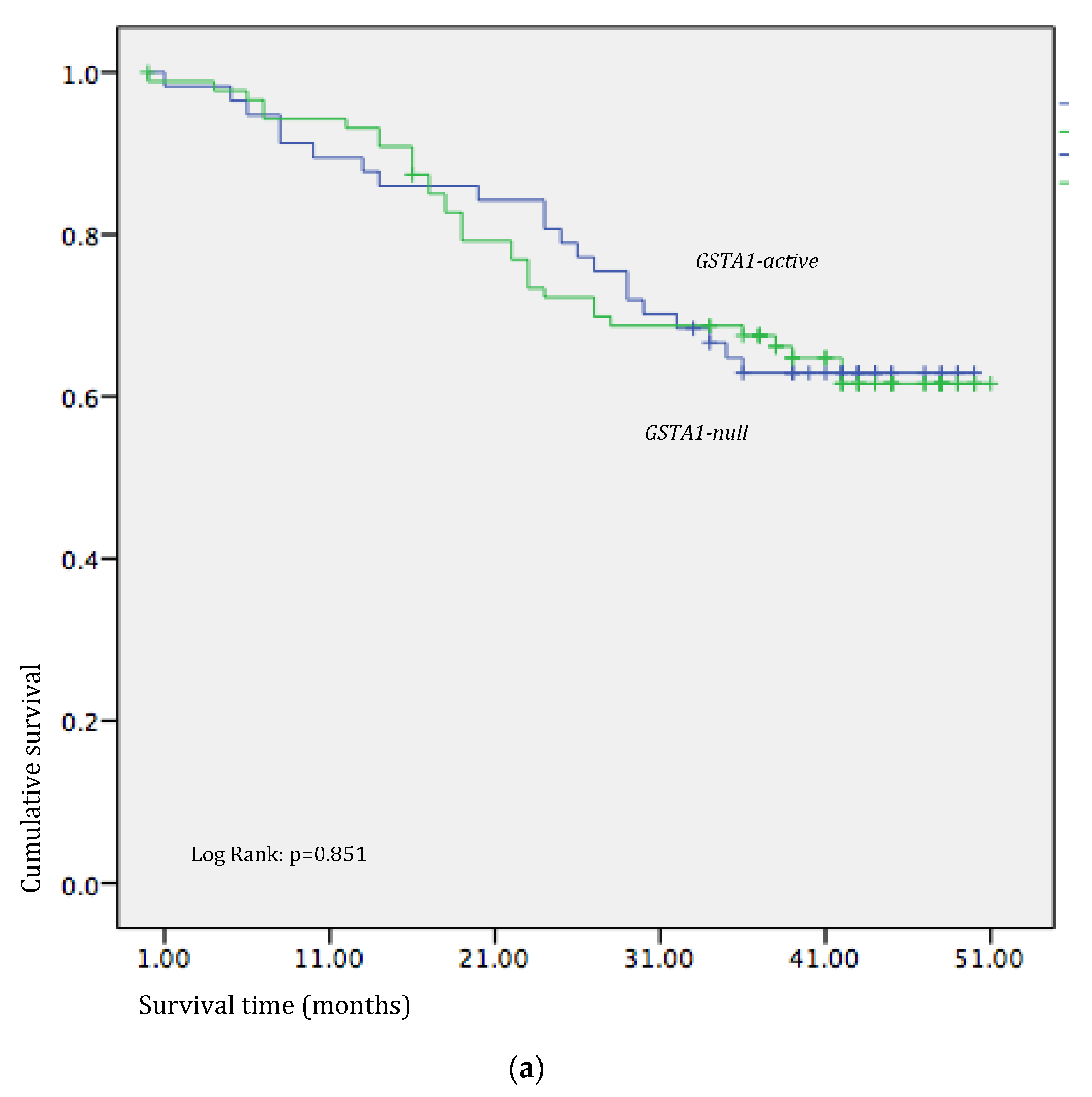
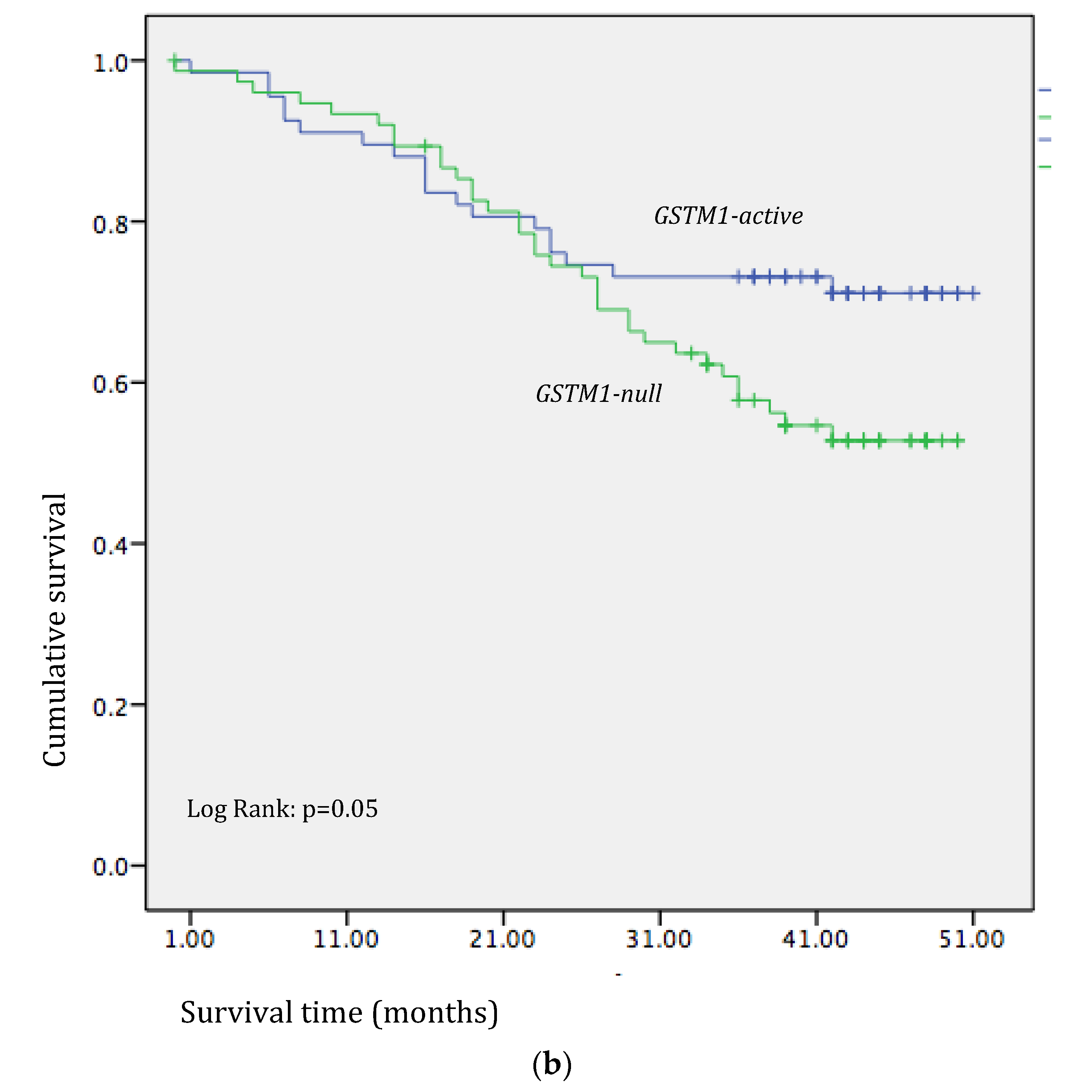
3.4. Effects of GST Polymorphisms on the Overall Survival of CRC Patients on 5-FU-Based Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Douaiher, J.; Ravipati, A.; Grams, B.; Chowdhury, S.; Alatise, O.; Are, C. Colorectal cancer-global burden, trends, and geographical variations. J. Surg. Oncol. 2017, 115, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Tauriello, D.V.F.; Calon, A.; Lonardo, E.; Batlle, E. Determinants of metastatic competency in colorectal cancer. Mol. Oncol. 2017, 11, 97–119. [Google Scholar] [CrossRef] [PubMed]
- Moghimi-Dehkordi, B.; Safaee, A. An overview of colorectal cancer survival rates and prognosis in Asia. World J. Gastrointest. Oncol. 2012, 4, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Guo, E.; Wei, H.; Liao, X.; Wu, L.; Zeng, X. Clinical significance and biological mechanisms of glutathione S-transferase mu gene family in colon adenocarcinoma. BMC Med. Genet. 2020, 21, 130. [Google Scholar] [CrossRef] [PubMed]
- Fearon, E.R.; Vogelstein, B. A genetic model for colorectal tumorigenesis. Cell 1990, 61, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Giglia, M.D.; Chu, D.I. Familial Colorectal Cancer: Understanding the Alphabet Soup. Clin. Colon Rectal Surg. 2016, 29, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Haggar, F.A.; Boushey, R.P. Colorectal cancer epidemiology: Incidence, mortality, survival, and risk factors. Clin. Colon Rectal Surg. 2009, 22, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Economopoulos, K.P.; Sergentanis, T.N. GSTM1, GSTT1, GSTP1, GSTA1 and colorectal cancer risk: A comprehensive meta-analysis. Eur. J. Cancer 2010, 46, 1617–1631. [Google Scholar] [CrossRef] [PubMed]
- Hezova, R.; Bienertova-Vasku, J.; Sachlova, M.; Brezkova, V.; Vasku, A.; Svoboda, M.; Radová, L.; Kiss, I.; Vyzula, R.; Slaby, O. Common polymorphisms in GSTM1, GSTT1, GSTP1, GSTA1 and susceptibility to colorectal cancer in the Central European population. Eur. J. Med. Res. 2012, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Mannervik, B.; Danielson, U.H. Glutathione transferases-structure and catalytic activity. CRC Crit. Rev. Biochem. 1988, 23, 283–337. [Google Scholar] [CrossRef]
- Tew, K.D.; Townsend, D.M. Glutathione-s-transferases as determinants of cell survival and death. Antioxid. Redox Signal. 2012, 17, 1728–1737. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.-P.; Nelson, H.H.; Yuan, J.-M.; Van den Berg, D.; Jin, A.; Wang, R.; Yu, M.C. Glutathione S-transferase (GST) gene polymorphisms, cigarette smoking and colorectal cancer risk among Chinese in Singapore. Carcinogenesis 2011, 32, 1507–1511. [Google Scholar] [CrossRef] [PubMed]
- Board, P.G.; Menon, D. Glutathione transferases, regulators of cellular metabolism and physiology. Biochim. Biophys. Acta 2013, 1830, 3267–3288. [Google Scholar] [CrossRef]
- Grussy, K.; Łaska, M.; Moczurad, W.; Król-Kulikowska, M.; Ściskalska, M. The importance of polymorphisms in the genes encoding glutathione S-transferase isoenzymes in development of selected cancers and cardiovascular diseases. Mol. Biol. Rep. 2023, 50, 9649–9661. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues-Fleming, G.H.; de Mendonça Fernandes, G.M.; Russo, A.; Biselli-Chicote, P.M.; Netinho, J.G.; Pavarino, É.C.; Goloni-Bertollo, E.M. Molecular evaluation of glutathione S transferase family genes in patients with sporadic colorectal cancer. World J. Gastroenterol. 2018, 24, 4462–4471. [Google Scholar] [CrossRef] [PubMed]
- Funke, S.; Timofeeva, M.; Risch, A.; Hoffmeister, M.; Stegmaier, C.; Seiler, C.M.; Brenner, H.; Chang-Claude, J. Genetic polymorphisms in GST genes and survival of colorectal cancer patients treated with chemotherapy. Pharmacogenomics 2010, 11, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Kap, E.J.; Richter, S.; Rudolph, A.; Jansen, L.; Ulrich, A.; Hoffmeister, M.; Ulrich, C.M.; Brenner, H.; Chang-Claude, J. Genetic variants in the glutathione S-transferase genes and survival in colorectal cancer patients after chemotherapy and differences according to treatment with oxaliplatin. Pharmacogenetics Genom. 2014, 24, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Liu, J.; Liu, X.; Qian, J.; Meng, C.; Zhu, P.; Hang, J.; Wang, Y.; Xiong, B.; Qiu, X.; Zhu, W.; et al. Development of pH/Glutathione-Responsive Theranostic Agents Activated by Glutathione S-Transferase π for Human Colon Cancer. J. Med. Chem. 2020, 63, 9271–9283. [Google Scholar] [CrossRef] [PubMed]
- Kumamoto, K.; Ishibashi, K.; Okada, N.; Tajima, Y.; Kuwabara, K.; Kumagai, Y.; Baba, H.; Haga, N.; Ishida, H. Polymorphisms of GSTP1, ERCC2 and TS-3′UTR are associated with the clinical outcome of mFOLFOX6 in colorectal cancer patients. Oncol. Lett. 2013, 6, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Tournigand, C.; André, T.; Achille, E.; Lledo, G.; Flesh, M.; Mery-Mignard, D.; Quinaux, E.; Couteau, C.; Buyse, M.; Ganem, G.; et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: A randomized GERCOR study. J. Clin. Oncol. 2004, 22, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, S.Z.; el-Zein, R.A.; Anwar, W.A.; Au, W.W. A multiplex PCR procedure for polymorphic analysis of GSTM1 and GSTT1 genes in population studies. Cancer Lett. 1996, 107, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Ping, J.; Wang, H.; Huang, M.; Liu, Z.-S. Genetic analysis of glutathione S-transferase A1 polymorphism in the Chinese population and the influence of genotype on enzymatic properties. Toxicol. Sci. 2006, 89, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Stojkovic Lalosevic, M.L.; Coric, V.M.; Pekmezovic, T.D.; Simic, T.P.; Pljesa Ercegovac, M.S.; Pavlovic Markovic, A.R.; Krivokapic, Z.V. Deletion and Single Nucleotide Polymorphisms in Common Glutathione-S Transferases Contribute to Colorectal Cancer Development. Pathol. Oncol. Res. 2019, 25, 1579–1587. [Google Scholar] [CrossRef] [PubMed]
- Zhunussova, G.; Zhunusbekova, B.; Djansugurova, L. Association between glutathione S-transferase M1 and T1 polymorphisms and colorectal cancer risk in patients from Kazakhstan. Clin. Lab. 2015, 61, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Klusek, J.; Nasierowska-Guttmejer, A.; Kowalik, A.; Wawrzycka, I.; Chrapek, M.; Lewitowicz, P.; Radowicz-Chil, A.; Klusek, J.; Głuszek, S. The Influence of Red Meat on Colorectal Cancer Occurrence Is Dependent on the Genetic Polymorphisms of S-Glutathione Transferase Genes. Nutrients 2019, 11, 1682. [Google Scholar] [CrossRef] [PubMed]
- Allocati, N.; Masulli, M.; Di Ilio, C.; Federici, L. Glutathione transferases: Substrates, inihibitors and pro-drugs in cancer and neurodegenerative diseases. Oncogenesis 2018, 7, 8. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Shi, W.; Zhao, L.; Dai, D.; Gao, J.; Kong, X. Can GSTM1 and GSTT1 polymorphisms predict clinical outcomes of chemotherapy in gastric and colorectal cancers? A result based on the previous reports. OncoTargets Ther. 2016, 9, 3683–3694. [Google Scholar] [CrossRef]
- Huang, M.; Zeng, Y.; Zhao, F.; Huang, Y. Association of glutathione S-transferase M1 polymorphisms in the colorectal cancer risk: A meta-analysis. J. Cancer Res. Ther. 2018, 14, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Polimanti, R.; Carboni, C.; Baesso, I.; Piacentini, S.; Iorio, A.; De Stefano, G.F.; Fuciarelli, M. Genetic variability of glutathione S-transferase enzymes in human populations: Functional inter-ethnic differences in detoxification systems. Gene 2013, 512, 102–107. [Google Scholar] [CrossRef]
- Csejtei, A.; Tibold, A.; Varga, Z.; Koltai, K.; Ember, A.; Orsos, Z.; Feher, G.; Horvath, O.P.; Ember, I.; Kiss, I. GSTM, GSTT and p53 polymorphisms as modifiers of clinical outcome in colorectal cancer. Anticancer Res. 2008, 28, 1917–1922. [Google Scholar] [PubMed]
- Feng, Z.; Liu, Z.; Peng, K.; Wu, W. A Prognostic Model Based on Nine DNA Methylation-Driven Genes Predicts Overall Survival for Colorectal Cancer. Front. Genet. 2021, 12, 779383. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.; Cao, Y.; Wu, L.; Huang, J.; Gao, F. An updating meta-analysis of the glutathione S-transferase T1 polymorphisms and colorectal cancer risk: A HuGE review. Int. J. Color. Dis. 2010, 25, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Martínez, C.; Martín, F.; Fernández, J.M.; García-Martín, E.; Sastre, J.; Díaz-Rubio, M.; Agúndez, J.A.; Ladero, J.M. Glutathione S-transferases mu 1, theta 1, pi 1, alpha 1 and mu 3 genetic polymorphisms and the risk of colorectal and gastric cancers in humans. Pharmacogenomics 2006, 7, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Doğru-Abbasoğlu, S.; Mutlu-Türkoğlu, U.; Türkoğlu, S.; Erbil, Y.; Barbaros, U.; Uysal, M.; Aykaç-Toker, G. Glutathione S-transferase-pi in malignant tissues and plasma of human colorectal and gastric cancers. J. Cancer Res. Clin. Oncol. 2002, 128, 91–95. [Google Scholar] [CrossRef]
- Sau, A.; Pellizzari Tregno, F.; Valentino, F.; Federici, G.; Caccuri, A.M. Glutathione transferases and development of new principles to overcome drug resistance. Arch. Biochem. Biophys. 2010, 500, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Mehrzad, V.; Roayaei, M.; Peikar, M.S.; Nouranian, E.; Mokarian, F.; Khani, M.; Farzannia, S. Bevacizumab plus FOLFOX or FOLFIRI regimens on patients with unresectable liver-only metastases of metastatic colorectal cancer. Adv. Biomed. Res. 2016, 5, 10. [Google Scholar] [CrossRef]
- Shahnam, A.; Ridha, Z.; Wiese, M.D.; Kichenadasse, G.; Sorich, M.J. Pharmacogenetic and ethnicity influence on oxaliplatin therapy for colorectal cancer: A meta-analysis. Pharmacogenomics 2016, 17, 1725–1732. [Google Scholar] [CrossRef] [PubMed]
- McLeod, H.L.; Sargent, D.J.; Marsh, S.; Green, E.M.; King, C.R.; Fuchs, C.S.; Ramanathan, R.K.; Williamson, S.K.; Findlay, B.P.; Thibodeau, S.N.; et al. Pharmacogenetic Predictors of Adverse Events and Response to Chemotherapy in Metastatic Colorectal Cancer: Results From North American Gastrointestinal Intergroup Trial N9741. J. Clin. Oncol. 2010, 28, 3227–3233. [Google Scholar] [CrossRef] [PubMed]
- Boige, V.; Mendiboure, J.; Pignon, J.-P.; Loriot, M.-A.; Castaing, M.; Barrois, M.; Malka, D.; Trégouët, D.-A.; Bouché, O.; Le Corre, D.; et al. Pharmacogenetic assessment of toxicity and outcome in patients with metastatic colorectal cancer treated with LV5FU2, FOLFOX, and FOLFIRI: FFCD 2000-05. J. Clin. Oncol. 2010, 28, 2556–2564. [Google Scholar] [CrossRef] [PubMed]
- Stoehlmacher, J.; Park, D.J.; Zhang, W.; Yang, D.; Groshen, S.; Zahedy, S.; Lenz, H.-J. A multivariate analysis of genomic polymorphisms: Prediction of clinical outcome to 5-FU/oxaliplatin combination chemotherapy in refractory colorectal cancer. Br. J. Cancer 2004, 91, 344–354. [Google Scholar] [CrossRef] [PubMed]
- Pljesa-Ercegovac, M.; Savic-Radojevic, A.; Matic, M.; Coric, V.; Djukic, T.; Radic, T.; Simic, T. Glutathione Transferases: Potential Targets to Overcome Chemoresistance in Solid Tumors. Int. J. Mol. Sci. 2018, 19, 3785. [Google Scholar] [CrossRef]
- Thévenin, A.F.; Zony, C.L.; Bahnson, B.J.; Colman, R.F. GST pi modulates JNK activity through a direct interaction with JNK substrate, ATF2. Protein Sci. 2011, 20, 834–848. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Living, n% | Deceased, n% | p-Value | |
|---|---|---|---|
| Sex | |||
| Male | 203 (70) | 86 (30) | 0.235 |
| Female | 137 (75) | 45 (25) | |
| Age (mean ± SD) | 62.42 ± 10.47 | 62.71 ± 13.09 | 0.815 |
| Localization | |||
| Left side | 65 (78) | 23 (22) | 0.697 |
| Right side | 275 (73) | 108 (27) | |
| TNM | |||
| I | 123 (93) | 9 (7) | 0.001 |
| II | 106 (88) | 14 (12) | |
| III | 86 (58) | 62 (42) | |
| IV | 25 (36) | 46 (64) | |
| Grade | |||
| Well differentiated | 267 (76) | 84 (24) | 0.005 |
| Moderately differentiated | 61 (60) | 38 (40) | |
| Poorly differentiated | 12 (57) | 9 (43) |
| GST Genotype | Living, n% | Deceased, n% | p-Value |
|---|---|---|---|
| GSTM1 | |||
| active a | 182 (80) | 47 (20) | 0.001 |
| null b | 150 (66) | 79 (34) | |
| GSTT1 | |||
| null b | 89 (69) | 41 (31) | 0.246 |
| active a | 243 (74) | 89 (26) | |
| GSTA1 (rs 3957357) | |||
| CC (active) | 120 (73) | 44 (27) | 0.913 |
| CT+TT (low activity) c | 215 (72) | 82 (28) | |
| GSTP1 (rs1695) | |||
| IleIle (referent) | 139(80) | 35 (20) | 0.009 |
| IleVal+ValVal (variant) d | 185 (68) | 86 (32) |
| Model 1 | |
|---|---|
| HR (95% CI) | p-Value |
| Risk of mortality in carriers of GSTM1-null a genotype compared to carriers of GSTM1-active b genotype | |
| 1.81 (1.22–2.68) | 0.003 |
| Risk of mortality in carriers of GSTT1-null a genotype compared to carriers of GSTT1-active b genotype | |
| 1.24 (0.82–1.87) | 0.301 |
| Risk of mortality in carriers of GSTA1-low activity c genotype compared to carriers of GSTA1-active b genotype | |
| 1.03 (0.69–1.53) | 0.873 |
| Risk of mortality in carriers of GSTP1-variant d genotype compared to carriers of GSTP1-referent genotype | |
| 1.53 (0.67–2.46) | 0.048 |
| Model 2 | |
|---|---|
| HR (95% CI) | p-Value |
| Risk of mortality in carriers of GSTM1-null a genotype compared to carriers of GSTM1-active b genotype | |
| 1.79 (1.21–2.65) | 0.004 |
| Risk of mortality in carriers of GSTT1-null a genotype compared to carriers of GSTT1-active b genotype | |
| 1.24 (0.82–1.88) | 0.300 |
| Risk of mortality in carriers of GSTA1-low activity c genotype compared to carriers of GSTA1-active b genotype | |
| 1.00 (0.67–1.50) | 0.986 |
| Risk of mortality in carriers of GSTP1-variant d genotype compared to carriers of GSTP1-referent genotype | |
| 1.57 (1.03–2.39) | 0.035 |
| Model 3 | |
|---|---|
| HR (95% CI) | p-Value |
| Risk of mortality in carriers of GSTM1-null a genotype compared to carriers of GSTM1-active b genotype | |
| 1.89 (1.21–2.65) | 0.001 |
| Risk of mortality in carriers of GSTT1-null a genotype compared to carriers of GSTT1-active b genotype | |
| 1.25 (0.85–1.84) | 0.250 |
| Risk of mortality in carriers of GSTA1-low activity c genotype compared to carriers of GSTA1-active b genotype | |
| 1.02 (0.70–1.48) | 0.918 |
| Risk of mortality in carriers of GSTP1-variant d genotype compared to carriers of GSTP1-referent genotype | |
| 1.47 (0.99–2.20) | 0.050 |
| Model 4 | |
|---|---|
| HR (95% CI) | p-Value |
| Risk of mortality in carriers GSTM1-null a genotype compared to carriers of GSTM1-active b genotype | |
| 1.89 (1.31–2.74) | 0.001 |
| Risk of mortality in carriers GSTT1-null a genotype compared to carriers of GSTT1-active b genotype | |
| 1.26 (0.86–1.84) | 0.245 |
| Risk of mortality in carriers GSTA1-low activity c genotype compared to carriers of GSTA1-active b genotype | |
| 1.02 (0.70–1.49) | 0.902 |
| Risk of mortality in carriers GSTP1-variant d genotype compared to carriers of GSTP1-referent genotype | |
| 1.50 (1.01–2.24) | 0.046 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojkovic Lalosevic, M.; Coric, V.; Pekmezovic, T.; Simic, T.; Pavlovic Markovic, A.; Pljesa Ercegovac, M. GSTM1 and GSTP1 Polymorphisms Affect Outcome in Colorectal Adenocarcinoma. Medicina 2024, 60, 553. https://doi.org/10.3390/medicina60040553
Stojkovic Lalosevic M, Coric V, Pekmezovic T, Simic T, Pavlovic Markovic A, Pljesa Ercegovac M. GSTM1 and GSTP1 Polymorphisms Affect Outcome in Colorectal Adenocarcinoma. Medicina. 2024; 60(4):553. https://doi.org/10.3390/medicina60040553
Chicago/Turabian StyleStojkovic Lalosevic, Milica, Vesna Coric, Tatjana Pekmezovic, Tatjana Simic, Aleksandra Pavlovic Markovic, and Marija Pljesa Ercegovac. 2024. "GSTM1 and GSTP1 Polymorphisms Affect Outcome in Colorectal Adenocarcinoma" Medicina 60, no. 4: 553. https://doi.org/10.3390/medicina60040553