
Successful Needle Aspiration of a Traumatic Pneumothorax: A Case Report and Literature Review
 , , and
, , and
Abstract
:1. Introduction
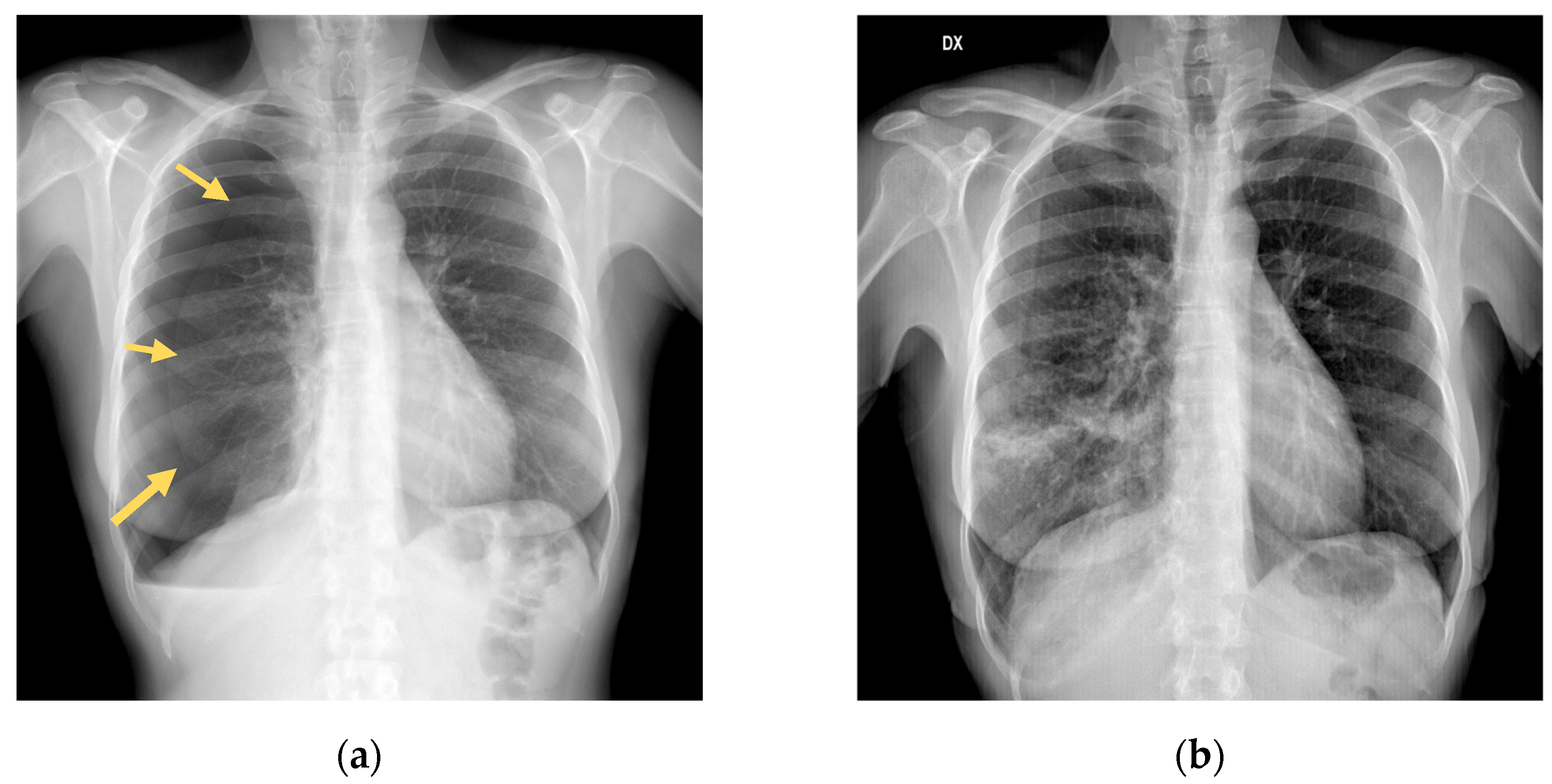
2. Case Presentation
3. Materials and Methods
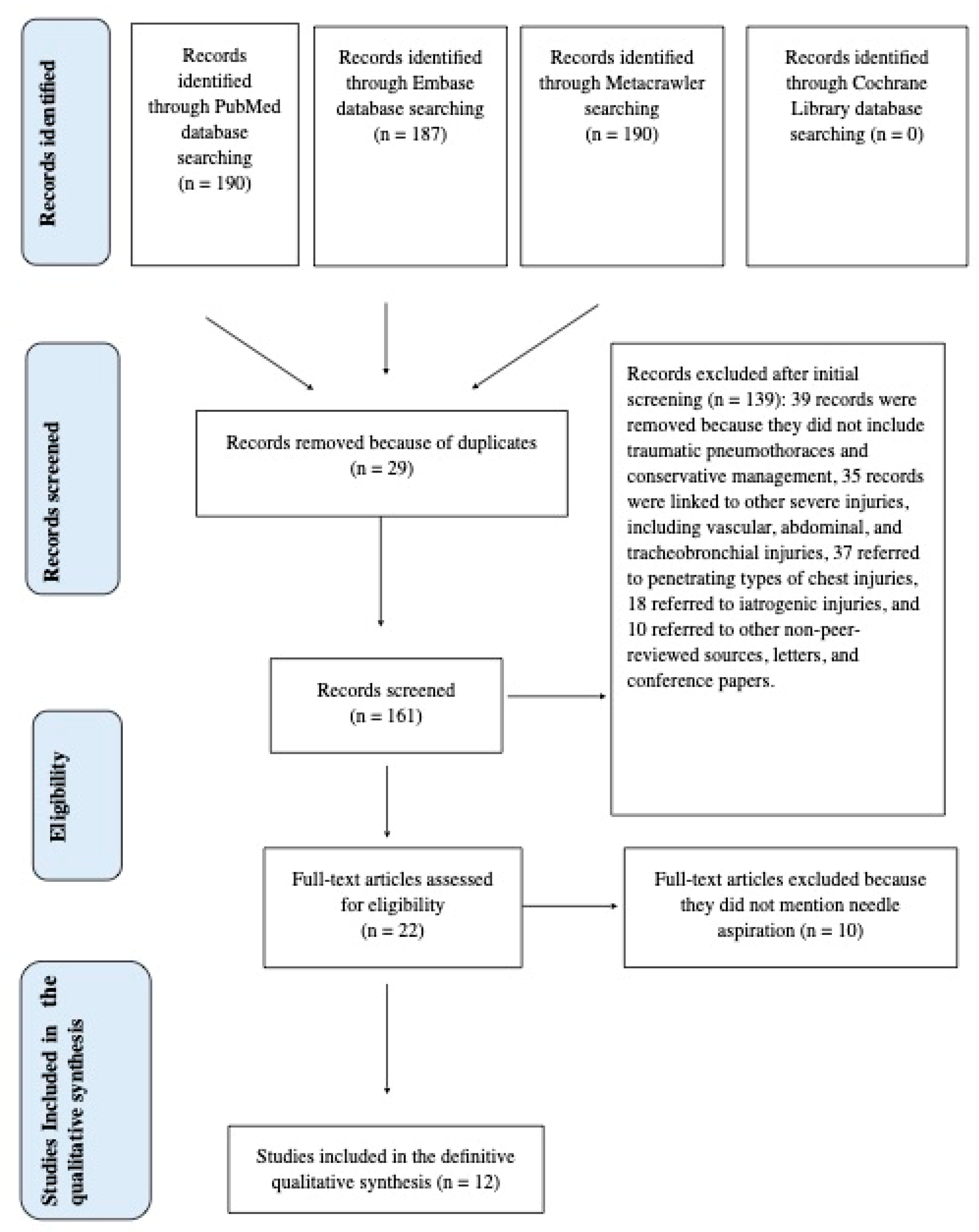
3.1. Research Methodology
3.2. Technical Details of Pneumothorax Needle Aspiration
4. Results
5. Discussion
6. Conclusions
7. Future Directions
- -
- Assessing comparative effectiveness. Conducting large-scale randomized controlled trials (RCTs) comparing conservative management (observation, oxygen therapy) with invasive interventions (chest tube insertion, needle decompression) in terms of patient outcomes such as mortality rates, length of hospital stay, complications, and quality of life;
- -
- Patient risk assessment and stratification. Identifying specific patient subgroups that may benefit more from conservative management vs. invasive treatment based on factors such as symptomatic or asymptomatic patients, age, comorbidities, mechanism of injury, severity of pneumothorax, presence of other injuries, and comorbidities;
- -
- Complications and long-term outcomes. Longitudinal studies assessing long-term outcomes and complications associated with conservative vs. invasive treatment approaches, including rates of recurrence, chronic pain, pulmonary function impairment, and risk of developing pleural adhesions or fibrosis;
- -
- Assessing the cost-effectiveness of conservative vs. invasive management strategies based on the utilization of healthcare resources, the direct medical costs, and indirect costs resulting from decreased quality of life and productivity;
- -
- Development and implementation of guidelines by updating clinical practice guidelines based on the latest evidence and consensus recommendations to guide healthcare professionals in the management of traumatic pneumothorax, including recommendations for initial assessment, treatment selection, and follow-up care.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baumann, M.H.; Noppen, M. Pneumothorax. Respirology 2004, 9, 157–164. [Google Scholar] [CrossRef] [PubMed]
- American College of Surgeons. ATLS: Advanced Trauma and Life Support. 10th Edition Student Course Manual; American College of Surgeons: Chicago, IL, USA, 2018; ISBN 9780996826235. [Google Scholar]
- Daly, R.C.; Mucha, P.; Pairolero, P.C.; Famell, M.B. The risk of percutaneous chest tube thoracostomy for blunt thoracic trauma. Ann. Emerg. Med. 1985, 14, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Kesieme, E.B.; Dongo, A.; Ezemba, N.; Irekpita, E.; Jebbin, N.; Kesieme, C. Tube thoracostomy: Complications and its management. Pulm. Med. 2012, 2012, 256878. [Google Scholar] [CrossRef] [PubMed]
- Menger, R.; Telford, G.; Kim, P.; Bergey, M.R.; Foreman, J.; Sarani, B.; Pascual, J.; Reilly, P.; Schwab, C.W.; Sims, C.A. Complications following thoracic trauma managed with tube thoracostomy. Injury 2012, 43, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Wall, S.D.; Federle, M.P.; Jeffrey, R.B.; Brett, C.M. CT diagnosis of unsuspected pneumothorax after blunt abdominal trauma. AJR Am. J. Roentgenol. 1983, 141, 919–921. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, I.; Younis, B.; Ahmed, K.; Mustafa, F.; El-Menyar, A.; Alabdallat, M.; Parchani, A.; Peralta, R.; Nabir, S.; Ahmed, N.; et al. Occult pneumothorax in patients presenting with blunt chest trauma: An observational analysis. Qatar Med. J. 2020, 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Zarogoulidis, P.; Kioumis, I.; Pitsiou, G.; Porpodis, K.; Lampaki, S.; Papaiwannou, A.; Katsikogiannis, N.; Zaric, B.; Branislav, P.; Secen, N.; et al. Pneumothorax: From definition to diagnosis and treatment. J. Thorac. Dis. 2014, 6, S372–S376. [Google Scholar] [CrossRef] [PubMed]
- Tanizaki, S.; Maeda, S.; Sera, M.; Nagai, H.; Hayashi, M.; Azuma, H.; Kano, K.I.; Watanabe, H.; Ishida, H. Small tube thoracostomy (20-22 Fr) in emergent management of chest trauma. Injury 2017, 48, 1884–1887. [Google Scholar] [CrossRef] [PubMed]
- Sahota, H.; Hinton, J.; Worley, E.; Milner, A.; Kay, E.; Badger, S. A critical appraisal on whether a traumatic pneumothorax should be managed conservatively. Clin. Med. 2016, 16, s35. [Google Scholar] [CrossRef]
- Eddine, B.Z.S.; Boyle, K.A.; Dodgion, C.M.; Davis, C.S.; Webb, T.P.; Juern, J.S.; Milia, D.J.; Carver, T.W.; Beckman, M.A.; Codner, P.A.; et al. Observing pneumothoraces: The 35-millimeter rule is safe for both blunt and penetrating chest trauma. J. Trauma. Acute Care Surg. 2019, 86, 557–864. [Google Scholar] [CrossRef]
- Chan, S.S. The role of simple aspiration in the management of primary spontaneous pneumothorax. J. Emerg. Med. 2008, 34, 131–138. [Google Scholar] [CrossRef]
- Johnson, G. Traumatic pneumothorax: Is a chest drain always necessary? J. Accid. Emerg. Med. 1996, 13, 173–174. [Google Scholar] [CrossRef] [PubMed]
- Banks, K.C.; Mooney, C.M.; Mazzolini, K.; Browder, T.D.; Victorino, G.P. Comparison of outcomes between observation and tube thoracostomy for small traumatic pneumothoraces. Am. J. Emerg. Med. 2023, 66, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Partyka, C.; Lawrie, K.; Bliss, J. Clinical outcomes of traumatic pneumothoraces undergoing conservative management following detection by prehospital physicians. Injury 2023, 54, 110886. [Google Scholar] [CrossRef]
- Anderson, D.E.; Kocik, V.I.; Rizzo, J.A.; Fisher, A.D.; Mould-Millman, N.K.; April, M.D.; Schauer, S.G. A Narrative Review of Traumatic Pneumothorax Diagnoses and Management. Med. J. 2023, Per 23-1/2/3, 3–10. [Google Scholar]
- Mattila, S.; Laustela, E.; Tala, P. Penetrating and perforating thoracic injuries. Scand. J. Thorac. Cardiovasc. Surg. 1981, 15, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.P.; Barratt, S.L.; Thompson, J.; Maskell, N.A. Conservative Management in Traumatic Pneumothoraces: An Observational Study. Chest 2018, 153, 946–953. [Google Scholar] [CrossRef]
- Ramirez, M.A.G.; Delos Santos, N.C.; Doble, F.C.; Baltazar, E.A.; Talens, E.S.; De Castro, E.C.; Baquir, A.T.D. Comparative study between manual aspiration and closed tube thoracostomy in the management of pneumothorax secondary to trauma: A prospective randomized control trial done in a tertiary hospital specialized in trauma. J. Am. Coll. Surg. 2012, 215, S100–S101. [Google Scholar] [CrossRef]
- Kirkpatrick, A.W.; Rizoli, S.; Ouellet, J.F.; Roberts, D.J.; Sirois, M.; Ball, C.G.; Xiao, Z.J.; Tiruta, C.; Meade, M.; Trottier, V.; et al. Canadian Trauma Trials Collaborative and the Research Committee of the Trauma Association of Canada. Occult pneumothoraces in critical care: A prospective multicenter randomized controlled trial of pleural drainage for mechanically ventilated trauma patients with occult pneumothoraces. J. Trauma. Acute Care Surg. 2013, 74, 747–754; Discussion 754–755. [Google Scholar] [CrossRef]
- Obeid, F.N.; Shapiro, M.J.; Richardson, H.H.; Horst, H.M.; Bivins, B.A. Catheter aspiration for simple pneumothorax (CASP) in the outpatient management of simple traumatic pneumothorax. J. Trauma. 1985, 25, 882–886. [Google Scholar] [CrossRef]
- Panjwani, A. Management of pneumothorax with oxygen therapy: A case series. Chest Dis. Rep. 2017, 7, 6–9. [Google Scholar] [CrossRef]
- Delius, R.E.; Obeid, F.N.; Horst, H.M.; Sorensen, V.J.; Fath, J.J.; Bivins, B.A. Catheter aspiration for simple pneumothorax. Experience with 114 patients. Arch. Surg. 1989, 124, 833–836. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Haussner; Shah, K. Traumatic Pneumothorax: A Review of Current Diagnostic Practices and Evolving Management. J. Emerg. Med. 2021, 61, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Stradling, P.; Poole, G. Conservative management of spontaneous pneumothorax. Thorax 1966, 21, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Carson-Chahoud, K.V.; Wakai, A.; van Agteren, J.E.; Smith, B.J.; McCabe, G.; Brinn, M.P.; O’Sullivan, R. Simple aspiration versus intercostal tube drainage for primary spontaneous pneumothorax in adults. Cochrane Database Syst. Rev. 2017, 9, CD004479. [Google Scholar] [CrossRef]
- Homma, T.; Ojima, T.; Shimada, Y.; Tanabe, K.; Yamamoto, Y.; Akemoto, Y.; Kitamura, N. Effectiveness and failure factors of manual aspiration using a small needle for large pneumothorax in stable patients. J. Thorac. Dis. 2022, 14, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Gerhardy, B.C.; Liebenberg, P.; Simpson, G. Conservative management of traumatic pneumothoraces: A retrospective cohort study. Emerg. Med. Australas. 2022, 34, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Tran, J.; Schmidt, L. Traumatic pneumothorax: Updates in diagnosis and management in the emergency department. Emerg. Med. Pract. 2022, 25, 1–28. [Google Scholar]
- Foley, J.; Walker, S.; Carlton, E. Large-bore versus small-bore chest drains in traumatic haemopneumothorax: An international survey of current practice. Emerg. Med. J. 2023, 40, 651–652. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Reference | Patient Group | Study Type and Level of Evidence | Outcomes | Key Results |
|---|---|---|---|---|
| Johnson et al., 1996 [13] | 29 patients | Retrospective study | Progression to chest drainage | 2/29 required chest drain for radiological progression |
| Banks et al., 2023 [14] | 73 patients with pneumothorax size < 30 mm | Retrospective study | LOS with secondary outcomes of pulmonary infection, failed trial of observation, readmission, and mortality | 39/73 observation <LOS than thoracostomy group |
| Partyka et al., 2023 [15] | 181 patients with suspected PTX | Retrospective study | Prehospital management: 75 patients out of 181 with traumatic PTX were safely identified and transported without needle decompression to the hospital. | 41.4% managed conservatively 58.6% underwent pleural decompression |
| Anderson et al., 2023 [16] | 266 patients with traumatic PTX | Review | 90% treated successfully without surgical intervention or subsequent tube drainage | |
| Mattilla et al., 1981 [17] | 511 patients with penetrating thoracic injuries | Case series | - | 117/511 tube thoracostomy 88/511 needle aspiration |
| Walker et al., 2018 [18] | 602 TARN patients 277/602 treated conservatively | Observational study | Progression to tube drainage intervention: 90% of patients were managed conservatively and did not require tube drainage | Mean ISS 26 252/277 (90%) did not require subsequent thoracic intervention |
| Ramirez et al., 2012 [19] | 31 patients | RCT (Manual aspiration vs Closed tube thoracostomy) | LOS, number of complications | 16/31 MA: <LOS, minimal use of analgesia, no need for antibiotic therapy |
| Kirkpatrick et al., 2013 [20] | 90 patients | RCT (Observation vs pleural drainage) | Progression to respiratory distress | No difference in RD |
| Obeid et al., 1985 [21] | 17 patients | Observational study | - | 16/17 catether aspiration: no complications, no hospitalization, less cost |
| Panjwani et al., 2017 [22] | 1 patient | Case report | - | Successfully treated with O2 administration |
| Delius et al., 1989 [23] | 16 patients | Retrospective study | - | 12/16 catheter aspiration (<LOS, less cost) 4/16 progressed to tube thoracostomy |
| Tran et al., 2021 [24] | - | Review | - | Modern management of traumatic PTX is shifting toward more conservative management practices (smaller catheters or observation) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bettoni, G.; Gheda, S.; Altomare, M.; Cioffi, S.P.B.; Ferrazzi, D.; Cazzaniga, M.; Bonacchini, L.; Cimbanassi, S.; Aseni, P. Successful Needle Aspiration of a Traumatic Pneumothorax: A Case Report and Literature Review. Medicina 2024, 60, 548. https://doi.org/10.3390/medicina60040548
Bettoni G, Gheda S, Altomare M, Cioffi SPB, Ferrazzi D, Cazzaniga M, Bonacchini L, Cimbanassi S, Aseni P. Successful Needle Aspiration of a Traumatic Pneumothorax: A Case Report and Literature Review. Medicina. 2024; 60(4):548. https://doi.org/10.3390/medicina60040548
Chicago/Turabian StyleBettoni, Giuseppe, Silvia Gheda, Michele Altomare, Stefano Piero Bernardo Cioffi, Davide Ferrazzi, Michela Cazzaniga, Luca Bonacchini, Stefania Cimbanassi, and Paolo Aseni. 2024. "Successful Needle Aspiration of a Traumatic Pneumothorax: A Case Report and Literature Review" Medicina 60, no. 4: 548. https://doi.org/10.3390/medicina60040548