
Quality of Life after Treatment for Pelvic Organ Prolapse in Real-World Study: Recommendations, Vaginal Pessary, and Surgery
 ,
,
Abstract
:1. Introduction
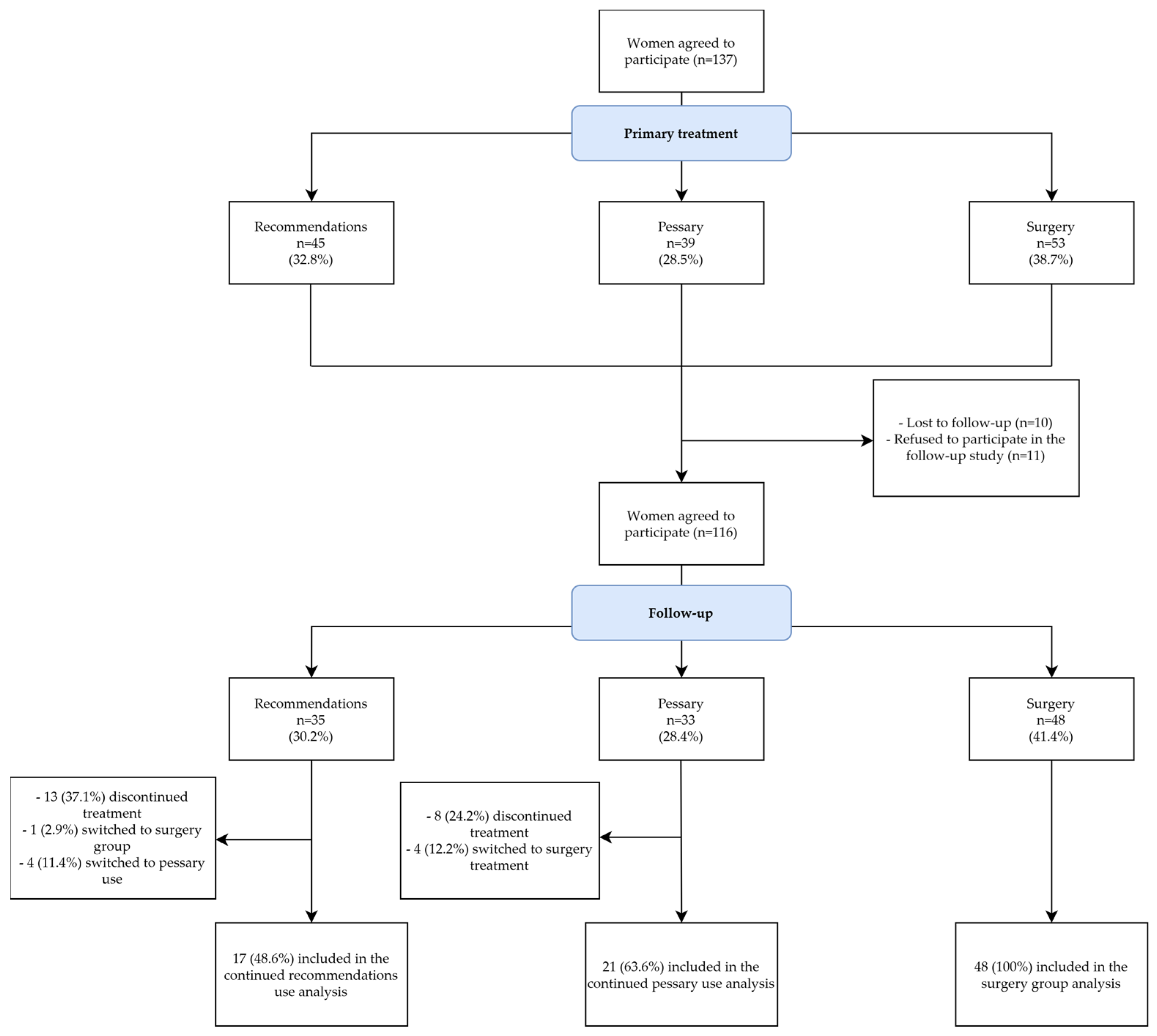
2. Materials and Methods
3. Results
4. Discussion
4.1. Main Findings
4.2. Primary Outcomes
4.3. Secondary Outcomes
4.4. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kinman, C.L.; Lemieux, C.A.; Agrawal, A.; Gaskins, J.T.; Meriwether, K.V.; Francis, S.L. The relationship between age and pelvic organ prolapse bother. Int. Urogynecol. J. 2017, 28, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Bodner-Adler, B.; Bodner, K.; Stinglmeier, A.; Kimberger, O.; Halpern, K.; Koelbl, H.; Umek, W. Prolapse surgery versus vaginal pessary in women with symptomatic pelvic organ prolapse: Which factors influence the choice of treatment? Arch. Gynecol. Obstet. 2019, 299, 773. [Google Scholar] [CrossRef] [PubMed]
- Bugge, C.; Adams, E.J.; Gopinath, D.; Stewart, F.; Dembinsky, M.; Sobiesuo, P.; Kearney, R. Pessaries (mechanical devices) for managing pelvic organ prolapse in women. Cochrane Database Syst. Rev. 2020, 11, CD004010. [Google Scholar] [PubMed]
- Bugge, C.; Dembinsky, M.; Kearney, R.; Hagen, S. Does self-management of vaginal pessaries improve care for women with pelvic organ prolapse? BMJ 2021, 372, 310. [Google Scholar] [CrossRef] [PubMed]
- Zeiger, B.B.; da Silva Carramão, S.; Del Roy, C.A.; da Silva, T.T.; Hwang, S.M.; Auge, A.P.F. Vaginal pessary in advanced pelvic organ prolapse: Impact on quality of life. Int. Urogynecol. J. 2022, 33, 2018–2020. [Google Scholar] [CrossRef] [PubMed]
- Raju, R.; Linder, B.J. Evaluation and Management of Pelvic Organ Prolapse. Mayo Clin. Proc. 2021, 96, 3122–3129. [Google Scholar] [CrossRef]
- Murphy, A.M.; Clark, C.B.; Denisenko, A.A.; D’Amico, M.J.; Vasavada, S.P. Surgical management of vaginal prolapse: Current surgical concepts. Can. J. Urol. 2021, 28, 22–26. [Google Scholar] [PubMed]
- Barber, M.D.; Brubaker, L.; Burgio, K.L.; Richter, H.E.; Nygaard, I.; Weidner, A.C.; Menefee, S.A.; Lukacz, E.S.; Norton, P.; Schaffer, J.; et al. Factorial comparison of two transvaginal surgical approaches and of perioperative behavioral therapy for women with apical vaginal prolapse: The OPTIMAL Randomized Trial. JAMA 2014, 311, 1023. [Google Scholar] [CrossRef]
- Anantawat, T.; Manonai, J.; Wattanayingcharoenchai, R.; Sarit-apirak, S. Impact of a vaginal pessary on the quality of life in women with pelvic organ prolapse. Asian Biomed. 2016, 10, 249–252. [Google Scholar]
- Li, C.; Gong, Y.; Wang, B. The efficacy of pelvic floor muscle training for pelvic organ prolapse: A systematic review and meta-analysis. Int. Urogynecol. J. 2016, 27, 981–992. [Google Scholar] [CrossRef]
- Coolen, A.L.W.M.; Troost, S.; Mol, B.W.J.; Roovers, J.P.W.R.; Bongers, M.Y. Primary treatment of pelvic organ prolapse: Pessary use versus prolapse surgery. Int. Urogynecol. J. 2018, 29, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Lone, F.; Thakar, R.; Sultan, A.H. One-year prospective comparison of vaginal pessaries and surgery for pelvic organ prolapse using the validated ICIQ-VS and ICIQ-UI (SF) questionnaires. Int. Urogynecol. J. 2015, 26, 1305–1312. [Google Scholar] [CrossRef]
- De Albuquerque, S.C.C.; de Castro, E.B.; Juliato, C.R.T. Female pelvic organ prolapse using pessaries: Systematic review. Int. Urogynecol. J. 2016, 27, 1797–1803. [Google Scholar] [CrossRef]
- Van der Vaart, L.R.; Vollebregt, A.; Milani, A.L.; Lagro-Janssen, A.L.; Duijnhoven, R.G.; Roovers, J.P.W.R.; Van der Vaart, C.H. Pessary or surgery for a symptomatic pelvic organ prolapse: The PEOPLE study, a multicentre prospective cohort study. Int. J. Obstet. Gynaecol. 2022, 129, 820–829. [Google Scholar] [CrossRef]
- Thys, S.; Hakvoort, R.; Milani, A.; Roovers, J.P.; Vollebregt, A. Can we predict continued pessary use as primary treatment in women with symptomatic pelvic organ prolapse (POP)? A prospective cohort study. Int. Urogynecol. J. 2021, 32, 2159–2167. [Google Scholar] [CrossRef] [PubMed]
- Nebel, S.; Creveuil, C.; Briex, M.; Fauvet, R.; Villot, A.; Pizzoferrato, A.C. How Satisfied Are Women 6 Months after a Pessary Fitting for Pelvic Organ Prolapse? J. Clin. Med. 2022, 11, 5972. [Google Scholar] [CrossRef]
- Abdool, Z.; Thakar, R.; Sultan, A.H.; Oliver, R.S. Prospective evaluation of outcome of vaginal pessaries versus surgery in women with symptomatic pelvic organ prolapse. Int. Urogynecol. J. 2011, 22, 273–278. [Google Scholar] [CrossRef]
- Thys, S.D.; Roovers, J.P.; Geomini, P.M.; Bongers, M.Y. Do Patients Prefer a Pessary or Surgery as Primary Treatment for Pelvic Organ Prolapse. Gynecol. Obstet. Investig. 2012, 74, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Miceli, A.; Dueñas-Diez, J.L. Effectiveness of ring pessaries versus vaginal hysterectomy for advanced pelvic organ prolapse. A cohort study. Int. Urogynecol. J. 2019, 30, 2161–2169. [Google Scholar] [CrossRef]
- Due, U.; Brostrøm, S.; Lose, G. Lifestyle advice with or without pelvic floor muscle training for pelvic organ prolapse: A randomized controlled trial. Int. Urogynecol. J. 2016, 27, 555–563. [Google Scholar] [CrossRef]
- Torres-Lacomba, M.; Navarro-Brazález, B.; Yuste-Sánchez, M.J.; Sánchez-Sánchez, B.; Prieto-Gómez, V.; Vergara-Pérez, F. Women’s Experiences with Compliance with Pelvic Floor Home Exercise Therapy and Lifestyle Changes for Pelvic Organ Prolapse Symptoms: A Qualitative Study. J. Pers. Med. 2022, 12, 498. [Google Scholar] [CrossRef] [PubMed]
- Aimjirakul, K.; Pumtako, M.; Manonai, J. Quality of Life After Treatment for Pelvic Organ Prolapse: Vaginal Pessary versus Surgery. Int. J. Womens Health 2023, 15, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Linder, B.J.; Gebhart, J.B.; Weaver, A.L.; Fick, F.R.; Harvey-Springer, R.R.; Trabuco, E.C.; Klingele, C.J.; Occhino, J.A. Comparison of outcomes between pessary use and surgery for symptomatic pelvic organ prolapse: A prospective self-controlled study. Investig. Clin. Urol. 2022, 63, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque Coelho, S.C.; Marangoni-Junior, M.; Brito, L.G.O.; De Castro, E.B.; Juliato, C.R.T. Quality of life and vaginal symptoms of postmenopausal women using pessary for pelvic organ prolapse: A prospective study. Rev. Assoc. Med. Bras. 2018, 64, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Limbutara, W.; Bunyavejchevin, S.; Ruanphoo, P.; Chiengthong, K. Patient-reported goal achievements after pelvic floor muscle training versus pessary in women with pelvic organ prolapse. A randomised controlled trial. J. Obstet. Gynaecol. 2023, 43, 2181061. [Google Scholar] [CrossRef] [PubMed]
- Manonai, J.; Sarit-Apirak, S.; Udomsubpayakul, U. Vaginal ring pessary use for pelvic organ prolapse: Continuation rates and predictors of continued use. Menopause 2018, 26, 665–669. [Google Scholar] [CrossRef]
- Van Der, L.R.V.; Vollebregt, A.; Milani, A.L.; Lagro-Janssen, A.L.; Duijnhoven, R.G.; Roovers, J.P.W.R.; van der Vaart, C.H. Effect of Pessary vs Surgery on Patient-Reported Improvement in Patients with Symptomatic Pelvic Organ Prolapse: A Randomized Clinical Trial. JAMA 2022, 328, 2312–2323. [Google Scholar] [CrossRef]


{kind=link}
| Recommendations (n = 45) | Pessary (n = 39) | Surgery (n = 53) | p Value | |
|---|---|---|---|---|
| Age (median (IQR)) | 57 (51–66) a | 63 (58–68.5) b | 70 (61–76) ab | <0.001 * |
| BMI (kg/m2, median (IQR)) | 27.45 (24.6–32.8) | 26.4 (25.14–29.5) | 28.95 (24.1–31.62) | 0.847 * |
| Smoking (n (%)) | 6 (13.3) | 2 (5.1) | 1 (1.9) | 0.068 ** |
| Constipation (n (%)) | 14 (31.1) | 9 (23.1) | 13 (24.5) | 0.659 ** |
| Parity (median (IQR)) | 2 (2–2) | 2 (2–3) | 2 (2–3) | 0.342 * |
| Vaginal delivery (n (%)) | ||||
| 0 | 1 (2.2) | 0 (0) | 2 (3.8) | 0.376 ** |
| 1 | 10 (22.2) | 4 (10.5) | 5 (9.6) | |
| 2 | 26 (57.8) | 23 (60.5) | 32 (61.5) | |
| ≥3 | 8 (17.8) | 11 (28.9) | 13 (25) | |
| Cesarean section (n (%)) | 4 (8.9) | 2 (5.3) | 1 (1.9) | 0.285 ** |
| Postmenopausal status (n (%)) | 30 (66.7) ac | 36 (92.3) c | 51 (96.2) a | <0.001 ** |
| Vaginal atrophy (n (%)) | 28 (62.2) ac | 35 (89.7) c | 47 (88.7) a | <0.001 ** |
| POP-Q stage (n (%)) | ||||
| 1 | 11 (24.4) ac | 1 (2.6) c | 0 (0) a | <0.001 ** |
| 2 | 25 (55.6) d | 6 (15.4) d | 1 (1.9) d | |
| 3 | 9 (20) ac | 32 (82.1) c | 47 (88.7) a | |
| 4 | 0 (0) a | 0 (0) b | 5 (9.4) ab | |
| Primary Treatment Methods | Continued Primary Treatment Methods | |||||||
|---|---|---|---|---|---|---|---|---|
| Recommendations (n = 35) | Pessary (n = 33) | Surgery (n = 48) | p Value * | Recommendations (n = 17) | Pessary (n = 21) | Surgery (n = 48) | p Value * | |
| PGI-I: improvement (n (%)) | 8 (22.9) a | 22 (66.7) a | 43 (89.6) a | <0.001 | 6 (35.3) bc | 19 (90.5) b | 43 (89.6) c | <0.001 |
| Recommendations (n = 35) | Pessary (n = 33) | |
|---|---|---|
| Reasons for discontinuation or switching to another treatment method (n (%)) | ||
| Inadequate symptom relief/did not meet expectations | 8 (22.9) | 3 (9.1) |
| Excessive vaginal discharge | 0 (0) | 3 (9.1) |
| Pessary expulsion | n/a | 1 (3.0) |
| Vaginal pain, discomfort | 3 (8.6) | 3 (9.1) |
| No reason | 6 (17.1) | 0 (0) |
| Prefer surgery | 1 (2.9) | 2 (6.0) |
| Another treatment used (n (%)) | ||
| Pessary | 4 (11.4) | n/a |
| Prolapse surgery | 1 (2.9) | 4 (12.1) |
| Period of primary treatment (median month (IQR)) | 2 (0–5) | 3 (3–3) |
| Baseline | 24 Months | |||||||
|---|---|---|---|---|---|---|---|---|
| P-QoL Domains | Recommendations (n = 35) Median (IQR) | Pessary (n = 33) Median (IQR) | Surgery (n = 48) Median (IQR) | p Value * | Recommendations (n = 17) Median (IQR) | Pessary (n = 21) Median (IQR) | Surgery (n = 48) Median (IQR) | p Value * |
| General health perception | 50 (37.5–50) a | 50 (50–50) | 50 (50–75) a | 0.008 | 50 (25–50) ab | 0 (0–25) b | 0 (0–25) a | <0.001 |
| Prolapse impact | 66.67 (33.33–100) | 66.67 (66.67–100) | 66.67 (66.67–100) | 0.059 | 33.33 (33.33–66.67) ab | 0 (0–33.33) b | 0 (0–0) a | <0.001 |
| Role limitations | 33.33 (8.33–58.33) a | 33.33 (0–66.67) c | 66.67 (33.33–83.33) ac | 0.005 | 0 (0–33.33)a | 0 (0–0) | 0 (0–0) a | 0.016 |
| Physical limitations | 50 (16.67–83.33) | 50 (16.67–66.67) | 66.67 (33.33–100) | 0.082 | 16.67 (0–50) ab | 0 (0–16.67) b | 0 (0–0) a | 0.003 |
| Social limitations | 11.11 (0–38.89) | 0 (0–33.33) | 22.22 (0–61.11) | 0.068 | 0 (0–22.22) | 0 (0–0) | 0 (0–0) | 0.149 |
| Personal relationships | 33.3 (0–66.6) | 16.6 (0–33.33) | 50 (33.3–83.3) | 0.142 | 50 (0–100) | 33.33 (0–66.66) | 0 (0–0) | 0.110 |
| Emotional disturbances | 33.33 (11.11–77.78) a | 33.33 (22.22–66.67) c | 66.67 (33.33–88.89) ac | 0.018 | 0 (0–33.33) ab | 0 (0–0) b | 0 (0–0) a | 0.007 |
| Sleep or energy disturbances | 33.33 (0–50) | 16.67 (0–33.33) | 33.33 (16.67–50) | 0.071 | 33.33 (0–66.67) ab | 0 (0–16.67) b | 0 (0–0) a | <0.001 |
| Severity measures score | 25 (16.67–33.33) a | 25 (16.67–41.67) c | 37.5 (20.83–66.67) ac | 0.009 | 16.67 (0–41.67) a | 8.33 (0–25) | 0 (0–8.33) a | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mančinskienė, D.; Mikėnaitė, M.; Barakat, M.; Kačerauskienė, J.; Railaitė, D.R.; Maleckienė, L.; Bartusevičius, A.; Bartusevičienė, E. Quality of Life after Treatment for Pelvic Organ Prolapse in Real-World Study: Recommendations, Vaginal Pessary, and Surgery. Medicina 2024, 60, 547. https://doi.org/10.3390/medicina60040547
Mančinskienė D, Mikėnaitė M, Barakat M, Kačerauskienė J, Railaitė DR, Maleckienė L, Bartusevičius A, Bartusevičienė E. Quality of Life after Treatment for Pelvic Organ Prolapse in Real-World Study: Recommendations, Vaginal Pessary, and Surgery. Medicina. 2024; 60(4):547. https://doi.org/10.3390/medicina60040547
Chicago/Turabian StyleMančinskienė, Dominyka, Miglė Mikėnaitė, Mark Barakat, Justina Kačerauskienė, Dalia Regina Railaitė, Laima Maleckienė, Arnoldas Bartusevičius, and Eglė Bartusevičienė. 2024. "Quality of Life after Treatment for Pelvic Organ Prolapse in Real-World Study: Recommendations, Vaginal Pessary, and Surgery" Medicina 60, no. 4: 547. https://doi.org/10.3390/medicina60040547