
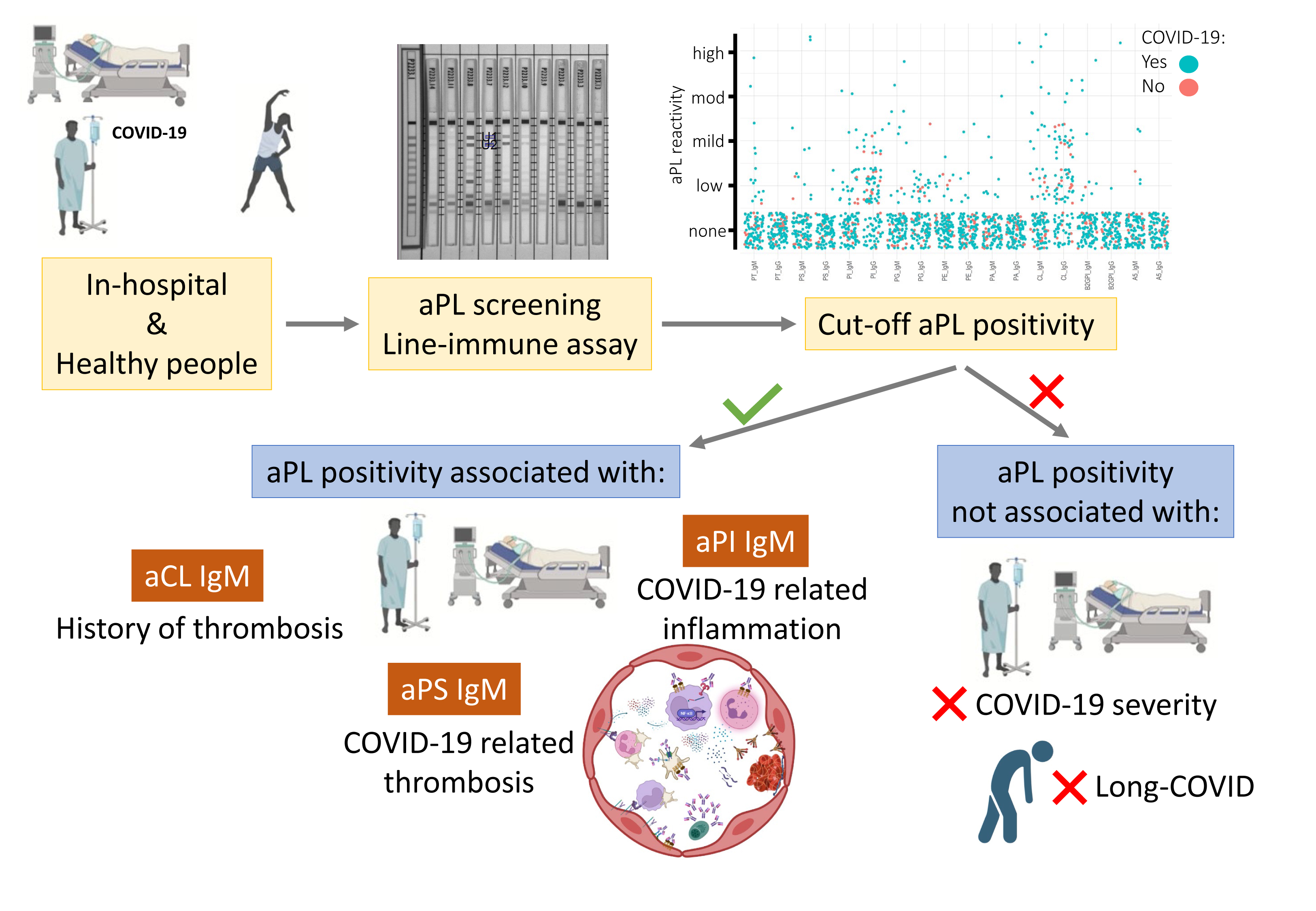
Thrombosis and Hyperinflammation in COVID-19 Acute Phase Are Related to Anti-Phosphatidylserine and Anti-Phosphatidylinositol Antibody Positivity
 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Laboratory Methods
Multiplex Line Immune Assay (LIA) for APLA Detection
2.3. Statistical Analysis
3. Results
3.1. Prevalence of APLA in COVID-19 Hospitalised Patients
3.2. APLA Is Associated with COVID-19 Thrombosis and Inflammation
3.3. Laboratory Data on Admission and Disease Outcome between APLA Positive and Negative COVID-19 Inpatients
3.4. APLA Positivity by Sex in COVID-19 Hospitalised Patients
3.5. APLA as Acute Markers of Long COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Hui, D.S.; Iazhar, E.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; Mchugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA J. Am. Med. Assoc. 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.D.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Levi, M.; Connors, J.M.; Thachil, J. Coagulopathy of Coronavirus Disease 2019. Crit. Care Med. 2020, 48, 1358–1364. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, Y.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Bradley, B.T.; Maioli, H.; Johnston, R.; Chaudhry, I.; Fink, S.L.; Xu, H.; Najafian, B.; Deutsch, G.; Lacy, J.M.; Williams, T.; et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington State: A case series. Lancet 2020, 396, 320–332. [Google Scholar] [CrossRef]
- Haberecker, M.; Schwarz, E.I.; Steiger, P.; Frontzek, K.; Scholkmann, F.; Zeng, X.; Höller, S.; Moch, H.; Varga, Z. Autopsy-Based Pulmonary and Vascular Pathology: Pulmonary Endotheliitis and Multi-Organ Involvement in COVID-19 Associated Deaths. Respiration 2022, 101, 155–165. [Google Scholar] [CrossRef]
- Iwamura, C.; Hirahara, K.; Kiuchi, M.; Ikehara, S.; Azuma, K.; Shimada, T.; Kuriyama, S.; Ohki, S.; Yamamoto, E.; Inaba, Y.; et al. Elevated Myl9 reflects the Myl9-containing microthrombi in SARS-CoV-2-induced lung exudative vasculitis and predicts COVID-19 severity. Proc. Natl. Acad. Sci. USA 2022, 119, e2203437119. [Google Scholar] [CrossRef] [PubMed]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. J. Lab. Clin. Med. 2020, 220, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Laurence, J.; Nuovo, G.; Racine-Brzostek, S.E.; Seshadri, M.; Elhadad, S.; Crowson, A.N.; Mulvey, J.J.; Harp, J.; Ahamed, J.; Magro, C. Premortem Skin Biopsy Assessing Microthrombi, Interferon Type I Antiviral and Regulatory Proteins, and Complement Deposition Correlates with Coronavirus Disease 2019 Clinical Stage. Am. J. Pathol. 2022, 192, 1282–1294. [Google Scholar] [CrossRef] [PubMed]
- Ahern, D.J.; Ai, Z.; Ainsworth, M.; Allan, C.; Allcock, A.; Angus, B.; Ansari, M.A.; Arancibia-Cárcamo, C.V.; Aschenbrenner, D.; Attar, M.; et al. A blood atlas of COVID-19 defines hallmarks of disease severity and specificity. Cell 2022, 185, 916–938.e58. [Google Scholar] [CrossRef]
- Kousathanas, A.; Pairo-Castineira, E.; Rawlik, K.; Stuckey, A.; Odhams, C.A.; Walker, S.; Russell, C.D.; Malinauskas, T.; Wu, Y.; Millar, J.; et al. Whole-genome sequencing reveals host factors underlying critical COVID-19. Nature 2022, 607, 97–103. [Google Scholar] [CrossRef]
- Engelmann, B.; Massberg, S. Thrombosis as an intravascular effector of innate immunity. Nat. Rev. Immunol. 2013, 13, 34–45. [Google Scholar] [CrossRef]
- Pfeiler, S.; Massberg, S.; Engelmann, B. Biological basis and pathological relevance of microvascular thrombosis. Thromb. Res. 2014, 133 (Suppl. S1), S35–S37. [Google Scholar] [CrossRef]
- Iba, T.; Helms, J.; Levi, M.; Levy, J.H. Thromboinflammation in acute injury: Infections, heatstroke, and trauma. J. Thromb. Haemost. JTH 2023, in press. [Google Scholar] [CrossRef]
- Martinod, K.; Deppermann, C. Immunothrombosis and thromboinflammation in host defense and disease. Platelets 2021, 32, 314–324. [Google Scholar] [CrossRef]
- Petito, E.; Falcinelli, E.; Paliani, U.; Cesari, E.; Vaudo, G.; Sebastiano, M.; Cerotto, V.; Guglielmini, G.; Gori, F.; Malvestiti, M.; et al. Association of Neutrophil Activation, More Than Platelet Activation, With Thrombotic Complications in Coronavirus Disease 2019. J. Infect. Dis. 2021, 223, 933–944. [Google Scholar] [CrossRef]
- Burzynski, L.C.; Humphry, M.; Pyrillou, K.; Wiggins, K.A.; Chan, J.N.E.; Figg, N.; Kitt, L.L.; Summers, C.; Tatham, K.C.; Martin, P.B.; et al. The Coagulation and Immune Systems Are Directly Linked through the Activation of Interleukin-1α by Thrombin. Immunity 2019, 50, 1033–1042.e6. [Google Scholar] [CrossRef] [PubMed]
- Meroni, P.L.; Borghi, M.O.; Raschi, E.; Tedesco, F. Pathogenesis of antiphospholipid syndrome: Understanding the antibodies. Nat. Rev. Rheumatol. 2011, 7, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.; Erkan, D.; Lee, A.I. COVID-19 and antiphospholipid antibodies. Best. Pract. Res. Clin. Haematol. 2022, 35, 101402. [Google Scholar] [CrossRef] [PubMed]
- Knight, J.S.; Kanthi, Y. Mechanisms of immunothrombosis and vasculopathy in antiphospholipid syndrome. Semin. Immunopathol. 2022, 44, 347–362. [Google Scholar] [CrossRef]
- Schreiber, K.; Sciascia, S.; De Groot, P.G.; Devreese, K.; Jacobsen, S.; Ruiz-Irastroza, G.; Salmon, J.E.; Shoenfeld, Y.; Shovman, O.; Hunt, B.J.; et al. Antiphospholipid syndrome. Nat. Rev. Dis. Primer 2018, 4, 17104. [Google Scholar] [CrossRef]
- Shoenfeld, Y.; Blank, M.; Cervera, R.; Font, J.; Raschi, E.; Meroni, P. Infectious origin of the antiphospholipid syndrome. Ann. Rheum. Dis. 2006, 65, 2–6. [Google Scholar] [CrossRef]
- Blank, M.; Krause, I.; Fridkin, M.; Keller, N.; Kopolovic, J.; Goldberg, I.; Tobar, A.; Shoenfeld, Y. Bacterial induction of autoantibodies to β2-glycoprotein-I accounts for the infectious etiology of antiphospholipid syndrome. J. Clin. Investig. 2002, 109, 797–804. [Google Scholar] [CrossRef]
- Asherson, R.A.; Cervera, R. Antiphospholipid antibodies and infections. Ann. Rheum. Dis. 2003, 62, 388–393. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Zuo, Y.; Estes, S.K.; Ali, R.A.; Gandhi, A.A.; Yalavarthi, S.; Shi, H.; Sule, G.; Gockman, K.; Madison, J.A.; Zuo, M.; et al. Prothrombotic autoantibodies in serum from patients hospitalized with COVID-19. Sci. Transl. Med. 2020, 12, 3876. [Google Scholar] [CrossRef]
- Hollerbach, A.; Müller-Calleja, N.; Pedrosa, D.; Canisius, A.; Sprinzl, M.F.; Falter, T.; Rossmann, H.; Bodenstein, M.; Werner, C.; Sagoschen, I.; et al. Pathogenic lipid-binding antiphospholipid antibodies are associated with severity of COVID-19. J. Thromb. Haemost. 2021, 19, 2335–2347. [Google Scholar] [CrossRef] [PubMed]
- Devreese, K.M.J.J.; Linskens, E.A.; Benoit, D.; Peperstraete, H. Antiphospholipid antibodies in patients with COVID-19: A relevant observation? J. Thromb. Haemost. JTH 2020, 18, 2191–2201. [Google Scholar] [CrossRef] [PubMed]
- Gatto, M.; Perricone, C.; Tonello, M.; Bistoni, O.; Cattelan, A.M.; Bursi, R.; Cafaro, G.; De Robertis, E.; Mencacci, A.; Bozza, S.; et al. Frequency and clinical correlates of antiphospholipid antibodies arising in patients with SARS-CoV-2 infection: Findings from a multicentre study on 122 cases. Clin. Exp. Rheumatol. 2020, 38, 754–759. [Google Scholar] [PubMed]
- Amezcua-Guerra, L.M.; Rojas-Velasco, G.; Brianza-Padilla, M.; Vázquez-Rangel, A.; Márquez-Velasco, R.; Baranda-Tovar, F.; Springall, R.; Gonzalez-Pacheco, H.; Juárez-Vicuña, Y.; Tavera-Alonso, C.; et al. Presence of antiphospholipid antibodies in COVID-19: A case series study. Ann. Rheum. Dis. 2021, 80, e73. [Google Scholar] [CrossRef]
- Espinosa, G.; Zamora-Martínez, C.; Pérez-Isidro, A.; Neto, D.; Bravo-Gallego, L.Y.; Prieto-González, S.; Viñas, O.; Moreno-Castaño, A.B.; Ruiz-Ortiz, E.; Cervera, R. Persistent Antiphospholipid Antibodies Are Not Associated with Worse Clinical Outcomes in a Prospective Cohort of Hospitalised Patients With SARS-CoV-2 Infection. Front. Immunol. 2022, 13, 1979. [Google Scholar] [CrossRef]
- Foret, T.; Dufrost, V.; du Mont, L.S.; Costa, P.; Lefevre, B.; Lacolley, P.; Regnault, V.; Zuily, S.; Wahl, D. Systematic Review of Antiphospholipid Antibodies in COVID-19 Patients: Culprits or Bystanders? Curr. Rheumatol. Rep. 2021, 23, 65. [Google Scholar] [CrossRef]
- Stelzer, M.; Henes, J.; Saur, S. The Role of Antiphospholipid Antibodies in COVID-19. Curr. Rheumatol. Rep. 2021, 23, 72. [Google Scholar] [CrossRef]
- Taha, M.; Samavati, L. Antiphospholipid antibodies in COVID-19: A meta-analysis and systematic review. RMD Open 2021, 7, e001580. [Google Scholar] [CrossRef]
- Anunciación-Llunell, A.; Muñoz, C.; Roggenbuck, D.; Frasca, S.; Pardos-Gea, J.; Esteve-Valverde, E.; Alijotas-Reig, J.; Miro-Mur, F. Differences in Antiphospholipid Antibody Profile between Patients with Obstetric and Thrombotic Antiphospholipid Syndrome. Int. J. Mol. Sci. 2022, 23, 12819. [Google Scholar] [CrossRef]
- Roggenbuck, D.; Egerer, K.; von Landenberg, P.; Hiemann, R.; Feist, E.; Burmester, G.R.; Dörner, T. Antiphospholipid antibody profiling—Time for a new technical approach? Autoimmun. Rev. 2012, 11, 821–826. [Google Scholar] [CrossRef]
- Egerer, K.; Roggenbuck, D.; Büttner, T.; Lehmann, B.; Kohn, A.; von Landenberg, P.; Hiemann, R.; Feist, E.; Burmester, G.R.; Dörner, T. Single-step autoantibody profiling in antiphospholipid syndrome using a multi-line dot assay. Arthritis Res. Ther. 2011, 13, R118. [Google Scholar] [CrossRef] [PubMed]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.; Groot, P.G.D.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Ahamed, J.; Laurence, J. Long COVID endotheliopathy: Hypothesized mechanisms and potential therapeutic approaches. J. Clin. Investig. 2022, 132, e161167. [Google Scholar] [CrossRef]
- Zhou, Y.; Han, T.; Chen, J.; Hou, C.; Hua, L.; He, S.; Guo, Y.; Zhang, S.; Wang, Y.; Yuan, J.; et al. Clinical and Autoimmune Characteristics of Severe and Critical Cases of COVID-19. Clin. Transl. Sci. 2020, 13, 1077–1086. [Google Scholar] [CrossRef]
- Serrano, M.; Espinosa, G.; Serrano, A.; Cervera, R. Antigens and Antibodies of the Antiphospholipid Syndrome as New Allies in the Pathogenesis of COVID-19 Coagulopathy. Int. J. Mol. Sci. 2022, 23, 4946. [Google Scholar] [CrossRef]
- Trahtemberg, U.; Rottapel, R.; Dos Santos, C.C.; Slutsky, A.S.; Baker, A.; Fritzler, M.J. Anticardiolipin and other antiphospholipid antibodies in critically ill COVID-19 positive and negative patients. Ann. Rheum. Dis. 2021, 80, 1236–1240. [Google Scholar] [CrossRef] [PubMed]
- Meroni, P.L.; Borghi, M.O. Antiphospholipid antibodies and COVID-19 thrombotic vasculopathy: One swallow does not make a summer. Ann. Rheum. Dis. 2021, 80, 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Pavoni, V.; Gianesello, L.; Horton, A. Antiphospholipid antibodies in critically ill COVID-19 patients with thromboembolism: Cause of disease or epiphenomenon? J. Thromb. Thrombolysis 2021, 52, 542–552. [Google Scholar] [CrossRef]
- Kernan, K.F.; Carcillo, J.A. Hyperferritinemia and inflammation. Int. Immunol. 2017, 29, 401–409. [Google Scholar] [CrossRef]
- Cruz-Tapias, P.; Blank, M.; Anaya, J.-M.M.; Shoenfeld, Y. Infections and vaccines in the etiology of antiphospholipid syndrome. Curr. Opin. Rheumatol. 2012, 24, 389–393. [Google Scholar] [CrossRef]
- Gharavi, A.E.; Pierangeli, S.S.; Espinola, R.G.; Liu, X.; Colden-Stanfield, M.; Harris, E.N. Antiphospholipid antibodies induced in mice by immunization with a cytomegalovirus-derived peptide cause thrombosis and activation of endothelial cells in vivo. Arthritis Rheum. 2002, 46, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, N.; Talathi, S.; Lopez-Olivo, M.A.; Suarez-Almazor, M.E. Risk of developing antiphospholipid antibodies following viral infection: A systematic review and meta-analysis. Lupus 2018, 27, 572–583. [Google Scholar] [CrossRef] [PubMed]
- Gharavi, E.E.; Chaimovich, H.; Cucurull, E.; Celli, C.M.; Tang, H.; Wilson, W.A.; Gharavi, A.E. Induction of antiphospholipid antibodies by immunization with synthetic viral and bacterial peptides. Lupus 1999, 8, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Favaloro, E.J.; Henry, B.M.; Lippi, G. COVID-19 and Antiphospholipid Antibodies: Time for a Reality Check? Semin. Thromb. Hemost. 2022, 48, 72–92. [Google Scholar] [CrossRef] [PubMed]
- Borghi, M.O.; Beltagy, A.; Garrafa, E.; Curreli, D.; Cecchini, G.; Bodio, C.; Grossi, C.; Blengino, S.; Tincani, A.; Franceschini, F.; et al. Anti-Phospholipid Antibodies in COVID-19 Are Different From Those Detectable in the Anti-Phospholipid Syndrome. Front. Immunol. 2020, 11, 584241. [Google Scholar] [CrossRef]
- Hunt, J.E.; McNeil, H.P.; Morgan, G.J.; Crameri, R.M.; Krilis, S.A. A phospholipid-beta 2-glycoprotein I complex is an antigen for anticardiolipin antibodies occurring in autoimmune disease but not with infection. Lupus 1992, 1, 75–81. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef]
- Scully, E.P.; Haverfield, J.; Ursin, R.L.; Tannenbaum, C.; Klein, S.L. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat. Rev. Immunol. 2020, 20, 442–447. [Google Scholar] [CrossRef]
- Takahashi, T.; Iwasaki, A. Sex differences in immune responses. Science 2021, 371, 347–348. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Henry, B.M.; Lippi, G. Is Lupus Anticoagulant a Significant Feature of COVID-19? A Critical Appraisal of the Literature. Semin. Thromb. Hemost. 2022, 48, 55–71. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, O.; Tacquard, C.; Dieudonné, Y.; Nespola, B.; Sattler, L.; Grunebaum, L.; Gies, V.; Radosavljevic, M.; Kaeuffer, C.; Hansmann, Y.; et al. Follow-up of COVID-19 patients: LA is transient but other aPLs are persistent. Autoimmun. Rev. 2021, 20, 102822. [Google Scholar] [CrossRef] [PubMed]
- Nalli, C.; Somma, V.; Andreoli, L.; Büttner, T.; Schierack, P.; Mahler, M.; Roggenbuck, D.; Tincani, A. Anti-phospholipid IgG antibodies detected by line immunoassay differentiate patients with anti-phospholipid syndrome and other autoimmune diseases. Autoimmun. Highlights 2018, 9, 6. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Gu, J.Y.; Jung, H.S.; Kim, H.K. Thrombotic risk of non-criteria anti-phospholipid antibodies measured by line immunoassay: Superiority of anti-phosphatidylserine and anti-phosphatidic acid antibodies. Clin. Lab. 2019, 65, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Barrett, T.J.; Bilaloglu, S.; Cornwell, M.; Burgess, H.M.; Virginio, V.W.; Drenkova, K.; Ibrahim, H.; Yuriditsky, E.; Aphinyanaphongs, Y.; Lifshitz, M.; et al. Platelets contribute to disease severity in COVID-19. J. Thromb. Haemost. 2021, 19, 3139–3153. [Google Scholar] [CrossRef]
- Zhu, A.; Real, F.; Capron, C.; Rosenberg, A.R.; Silvin, A.; Dunsmore, G.; Zhu, J.; Cottoignies-Callamarte, A.; Massé, J.M.; Moine, P.; et al. Infection of lung megakaryocytes and platelets by SARS-CoV-2 anticipate fatal COVID-19. Cell Mol. Life Sci. 2022, 79, 365. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet Lond. Engl. 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef]
- Bertin, D.; Kaphan, E.; Weber, S.; Babacci, B.; Arcani, R.; Faucher, B.; Ménard, A.; Brodovitch, A.; Mege, J.L.; Bardin, N. Persistent IgG anticardiolipin autoantibodies are associated with post-COVID syndrome. Int. J. Infect. Dis. 2021, 113, 23–25. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 92) | APLA Positive (N = 30) | APLA Negative (N = 62) | p-Value | |
|---|---|---|---|---|
| Sex (female) 1 | 42 (45.7%) | 12 (40.0%) | 30 (48.4%) | 0.51 † |
| Age (years) 2 | 63.67 (13.0) | 65.8 (11.9) | 62.6 (13.5) | 0.26 ‡ |
| Hypertension 1 | 34 (37.0%) | 15 (50.0%) | 19 (30.6%) | 0.11 † |
| Dyslipidaemia 1 | 29 (31.6%) | 8 (26.7%) | 21 (33.9%) | 0.63 † |
| Renal chronic disease 1 | 11 (12.0%) | 3 (10.0%) | 8 (12.9%) | 1.00 † |
| Diabetes Mellitus 1 | 18 (19.6%) | 6 (20.0%) | 12 (19.3%) | 1.00 † |
| Myocardiopathy 1 | 8 (8.7%) | 2 (6.7%) | 6 (9.7%) | 1.00 † |
| Peripheral vasculopathy 1 | 5 (5.4%) | 2 (6.7%) | 3 (4.8%) | 0.66 † |
| Stroke 1 | 4 (4.3%) | 0 (0.0%) | 4 (6.4%) | 0.30 † |
| COPD-Asthma 1 | 10 (10.9%) | 2 (6.6%) | 8 (12.9%) | 0.49 † |
| ILD 1 | 1 (1.1%) | 0 (0.0%) | 1 (1.6%) | 1.00 † |
| AID 1 | 8 (8.7%) | 4 (13.3%) | 4 (6.4%) | 0.43 † |
| Thrombotic history 1 | 3 (3.3%) | 2 (6.7%) | 1(1.6%) | 0.25 † |
| Inherited thrombophilia 1 | 1 (1.1%) | 1 (3.3%) | 0 (0.0%) | 0.33 † |
| Cancer 1 | 10 (10.9%) | 3 (10.0%) | 7 (11.3%) | 1.00 † |
| APLA 1 | n | Positives | Prevalence (%) | 95% CI |
|---|---|---|---|---|
| aCL IgG | 92 | 3 | 3.26 | 0.85–9.91 |
| aPA IgG | 92 | 1 | 1.09 | 0.06–6.76 |
| aPE IgG | 92 | 2 | 2.17 | 0.38–8.38 |
| aβ2GPI IgG | 92 | 1 | 1.09 | 0.06–6.76 |
| aCL IgM | 92 | 12 | 13.04 | 7.21–22.06 |
| aPA IgM | 92 | 3 | 3.26 | 0.85–9.91 |
| aPE IgM | 92 | 1 | 1.09 | 0.06–6.76 |
| aPG IgM | 92 | 8 | 8.7 | 4.1–16.9 |
| aPI IgM | 92 | 5 | 5.43 | 2.02–12.81 |
| aPS IgM | 92 | 5 | 5.43 | 2.02–12.81 |
| aAn5 IgM | 92 | 1 | 1.09 | 0.06–6.76 |
| aβ2GPI IgM | 92 | 3 | 3.26 | 0.85–9.91 |
| aPT IgM | 92 | 5 | 5.43 | 2.02–12.81 |
| APLA | Parameter | N 1 | APLA Negative | APLA Positive | p-Value | Adjusted p-Value |
|---|---|---|---|---|---|---|
| aCL IgM | Thrombotic history † | 92 | 1; 1.2% [0, 6.8] | 2; 16.7% [2.1, 48.4] | 0.044 | 0.046 |
| aPS IgM | COVID-19-related thrombosis † | 92 | 5; 5.8% [1.9, 13] | 2; 40% [5.3, 85.3] | 0.046 | 0.050 |
| aPI IgM | IL-6 †† | 72 | 27.5 [10.6, 63.5] | 150 [88.2, 335] | 0.007 | 0.012 |
| aPI IgM | ferritin †† | 82 | 472 [259, 810] | 1657 [630, 2366] | 0.034 | 0.041 |
| aPE IgG | INR †† | 78 | 1.1 [1.0, 1.2] | 1.4 [1.35, 1.45] | 0.041 | 0.043 |
| COVID-19 Severity n = 92 | Long COVID-19 n = 81 | |||||
|---|---|---|---|---|---|---|
| Moderate (n = 78) n; %; [95% CI] | Severe (n = 14) n; %; [95% CI] | p-Value † | No (n = 74) n; %; [95% CI] | Yes (n = 7) n; %; [95% CI] | p-Value † | |
| aCL IgG | 3; 3.8; [0.8, 10.8] | 0; 0; [0, 23.2] | 1.00 | 2; 2.7%; [0.4, 10.2] | 0; 0%; [0, 41] | 1.00 |
| aPA IgG | 1; 1.3; [0, 6.9] | 0; 0; [0, 23.2] | 1.00 | 1; 1.4%; [0, 7.9] | 0; 0%; [0, 41] | 1.00 |
| aPE IgG | 2; 2.6; [0.3, 9] | 0; 0; [0, 23.2] | 1.00 | 1; 1.4%; [0, 7.9] | 0; 0%; [0, 41] | 1.00 |
| aβ2GPI IgG | 0; 0; [0, 4.6] | 1; 7.1; [0.2, 33.9] | 0.15 | 0; 0%; [0, 5.3] | 1; 14.3%; [0.4, 57.9] | 0.09 |
| aCL IgM | 10; 12.8; [6.3, 22.3] | 2; 14.3; [1.8, 42.8] | 1.00 | 8; 10.8%; [5.2, 21.9] | 2; 28.6%; [3.7, 71] | 0.23 |
| aPA IgM | 3; 3.8; [0.8, 10.8] | 0; 0; [0, 23.2] | 1.00 | 3; 4.1%; [0.9, 12.4] | 0; 0%; [0, 41] | 1.00 |
| aPE IgM | 1; 1.3; [0, 6.9] | 0; 0; [0, 23.2] | 1.00 | 1; 1.4%; [0, 7.9] | 0; 0%; [0, 41] | 1.00 |
| aPG IgM | 8; 10.3; [4.5, 19.2] | 0; 0; [0, 23.2] | 0.60 | 7; 9.5%; [4.2, 20.1] | 1; 14.3%; [0.4, 57.9] | 0.56 |
| aPI IgM | 3; 3.8; [0.8, 10.8] | 2; 14.3; [1.8, 42.8] | 0.17 | 3; 4.1%; [0.9, 12.4] | 0; 0%; [0, 41] | 1.00 |
| aPS IgM | 4; 5.1; [1.4, 12.6] | 1; 7.1; [0.2, 33.9] | 0.57 | 4; 5.4%; [1.6, 14.4] | 0; 0%; [0, 41] | 1.00 |
| aAnV IgM | 0; 0; [0, 4.6] | 1; 7.1; [0.2, 33.9] | 0.15 | 0; 0%; [0, 5.3] | 1; 14.3%; [0.4, 57.9] | 0.09 |
| aβ2GPI IgM | 2; 2.6; [0.3, 9] | 1; 7.1; [0.2, 33.9] | 0.39 | 3; 4.1%; [0.9, 12.4] | 0; 0%; [0, 41] | 1.00 |
| aPT IgM | 5; 6.4; [2.1, 14.3] | 0; 0; [0, 23.2] | 1.00 | 5; 6.8%; [2.4, 16.3] | 0; 0%; [0, 41] | 1.00 |
| APLA Positive (N = 30) | APLA Negative (N = 62) | p-Value | |
|---|---|---|---|
| Days in hospital 1 | 19.0 (28.5) | 15.5 (18.8) | 0.05 ‡ |
| Severity | 5 (16.7) | 9 (14.5) | 0.77 † |
| Mortality | 2 (6.7) | 6 (9.7) | 1.00 † |
| Thrombosis | 2 (6.7) | 5 (8.2) | 1.00 † |
| LMWH treatment | 27 (90.0) | 49 (79.0) | 0.37 † |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alijotas-Reig, J.; Anunciación-Llunell, A.; Morales-Pérez, S.; Trapé, J.; Esteve-Valverde, E.; Miro-Mur, F. Thrombosis and Hyperinflammation in COVID-19 Acute Phase Are Related to Anti-Phosphatidylserine and Anti-Phosphatidylinositol Antibody Positivity. Biomedicines 2023, 11, 2301. https://doi.org/10.3390/biomedicines11082301
Alijotas-Reig J, Anunciación-Llunell A, Morales-Pérez S, Trapé J, Esteve-Valverde E, Miro-Mur F. Thrombosis and Hyperinflammation in COVID-19 Acute Phase Are Related to Anti-Phosphatidylserine and Anti-Phosphatidylinositol Antibody Positivity. Biomedicines. 2023; 11(8):2301. https://doi.org/10.3390/biomedicines11082301
Chicago/Turabian StyleAlijotas-Reig, Jaume, Ariadna Anunciación-Llunell, Stephanie Morales-Pérez, Jaume Trapé, Enrique Esteve-Valverde, and Francesc Miro-Mur. 2023. "Thrombosis and Hyperinflammation in COVID-19 Acute Phase Are Related to Anti-Phosphatidylserine and Anti-Phosphatidylinositol Antibody Positivity" Biomedicines 11, no. 8: 2301. https://doi.org/10.3390/biomedicines11082301