1. Introduction
Total knee arthroplasty (TKA) is a well-established knee reconstruction procedure for treating advanced osteoarthritis (OA) and a reliable surgical procedure for alleviating pain, accelerating functional recovery, and improving quality of life (QoL) with respect to patient-reported outcomes [
1,
2]. The number of patients undergoing TKA has steadily increased every year, and primary TKA patients aged <65 years are estimated to comprise more than half of all TKA patients in the United States [
3]. Postoperative rehabilitation following TKA is an important issue. A decrease in the strength of both the quadriceps and hamstring occurs following TKA. This decline in the muscle strength of the lower limbs is associated with a decline in functional outcomes [
4,
5]. Postoperative rehabilitation aims to increase the range of motion of the knee, muscle strength, and proprioceptive functions after TKA. Various exercise interventions have been associated with different levels of positive effects in patients after TKA [
6,
7,
8,
9]; however, these effects are inconsistent because of poor supervision, impaired exercise adherence, and low compliance with exercise regimens [
10,
11,
12].
Walking is the most common and essential physical activity of daily living (ADL). It is also a complex activity involving all levels of the neuromuscular and cardiorespiratory systems and has numerous health benefits [
13]. Meanwhile, walking training has a positive effect on the health-related and perceived quality of Life in older persons [
14,
15]. Thus, we performed an easy training regimen, walk training (WT), on patients in TKA recovery for the purpose of reducing the bias of poor supervision. Because the number of female patients who had undergone TKA was approximately twice that of men between 2001 and 2010 [
16], this study focused only on female patients who had undergone TKA. Additionally, patient-reported outcome measurements are routinely used in clinical research for assessing patients’ health statuses [
17]. The Knee Injury and Osteoarthritis Outcome Score (KOOS) questionnaire is the most reliable and relevant patient-reported outcome measurement to assess knee-specific and related problems, including patients’ quality of life [
18]. Therefore, we used the KOOS questionnaire to evaluate the health status of TKA. This study aimed to evaluate the effect of a supervised walking regimen on lower limb muscle strength, functional fitness, and patient-reported outcomes in female patients with TKA. We hypothesized that the WT would have positive effects on low limb muscle strength, performance on the functional fitness test, and KOOS in female TKA.
3. Results
The patients’ demographic data are shown in
Table 1. The mean age was 68.5 ± 6.6 and 69.7 ± 2.8 years in the CON and WT groups, respectively. Height and weight were similar between the CON and WT groups. Lower extremity muscle strength, functional test results, and KOOS scores were similar between the CON and WT groups (
p > 0.05).
In the lower extremity muscle strength assessment, the WT group exhibited a significant increase in hip extensor, knee extensor, and knee flexor muscle strengths compared to the CON group at the post-exercise assessment, and the differences in knee extensor and flexor muscle strengths lasted until the follow-up (
Table 2). When participants were compared within each group in a temporal manner (
Table 3), the CON group exhibited a significant increase only in knee extensor muscle strength at the final follow-up compared with the baseline measurement. However, the WT group exhibited a significant increase in hip extensor, knee extensor, and knee flexor measurements at the post-exercise assessment compared with the baseline. The knee extensors even exhibited a significant increase in muscle strength during the mid-exercise assessment.
The functional outcomes of the functional fitness tests (
Table 4) revealed that the results of the 6MWT, 8UG, and 30CST did not differ significantly between the CON and WT groups at each assessment time point. However, in the temporal comparison (
Table 5), the results of the 6MWT and 8UG showed significant improvements at the mid-exercise, post-exercise, and follow-up measurements compared with baseline measurements in the WT group, but not in the CON group.
The self-explanatory KOOS questionnaire revealed (
Table 6) that the QoL subscale was significantly increased in the WT group compared to the CON group at follow-up. When a temporal comparison was performed within each group (
Table 7), scores for the subscales of symptoms, pain, and ADL exhibited significant improvements in both the CON and WT groups at the follow-up compared with the baseline. The improvement in scores in the pain and ADL subscales in the WT group occurred at an earlier time point (pain scores decreased at the post-exercise evaluation; ADL scores increased at the mid-and post-exercise evaluations). Among these subcategories, scores for the QoL subscale in the WT group exhibited a significant increase in the post-exercise and follow-up assessments compared with the baseline; however, these improvements were not observed in the CON group.
4. Discussion
The most important findings of the present study were the statistical increase in the QoL subcategory of KOOS and the knee muscle strength (extensors and flexors) in the WT group compared to the CON group at follow-up (
Table 2 and
Table 6). While the comparison was performed within the individual group in a temporal manner (
Table 3 and
Table 5), the knee extensors and functional fitness test (6 MWT: ambulatory capacity, 8UG: motor agility) in the WT group were improved at the mid-exercise, post-exercise, and follow-up measurements compared with the baseline, suggesting that WT enhanced the recovery of functional mobility after TKA [
30,
31,
32,
33]. These increases were based on the concomitant improvements in the pain, symptoms, and ADL subcategories of KOOS after TKA, quadriceps training, and range of motion exercises [
10,
34,
35]. In addition to the range of motion of knee and muscle strength on which the TKA standard exercises focus, WT may provide extra endurance and proprioception.
Many studies have shown that an increase in the quadriceps strength of TKA patients is associated with superior outcomes and performance [
36,
37,
38,
39,
40]. Previous studies have also revealed that muscle strengthening improves quadriceps strength and functional fitness test scores (timed up-and-go, stair-climbing test, and 6MWT) [
41,
42]. Our results were similar to other findings in the literature, and showed that the knee extensor and flexor strength in the WT group significantly improved compared with the CON group (
Table 2). In the temporal comparison within individual groups, the knee extensor improvement in the WT group occurred simultaneously with the improvements in the 6MWT and 8UG functional tests (
Table 4 and
Table 5), as well as in the ADL domains of KOOS (
Table 6 and
Table 7). These results imply that lower leg muscle strength is a determinant physical factor and plays a pivotal role in functional outcomes in TKA patients [
43,
44]. However, no significant difference in the 6MWT, 8UG, or the ADL subscales of KOOS was observed between the two groups. The lack of a significant difference might have resulted from the small sample size.
All patients in the WT group were supervised by a trained physical therapist during training, and no patient in the WT group reported discomfort or needed further medical management. Our results suggest that WT is beneficial for patients who have undergone TKA. Considering the ease of standardization and performance of WT, it can be effectively applied during rehabilitation following TKA in community-dwelling patients. However, a trained physical therapist also plays an important role in the intervention. In this study, a therapist monitored the status of the participants and gave real-time assistance when the participants had an issue during the exercise. Therefore, the deployment of a trained physical therapist would be recommended.
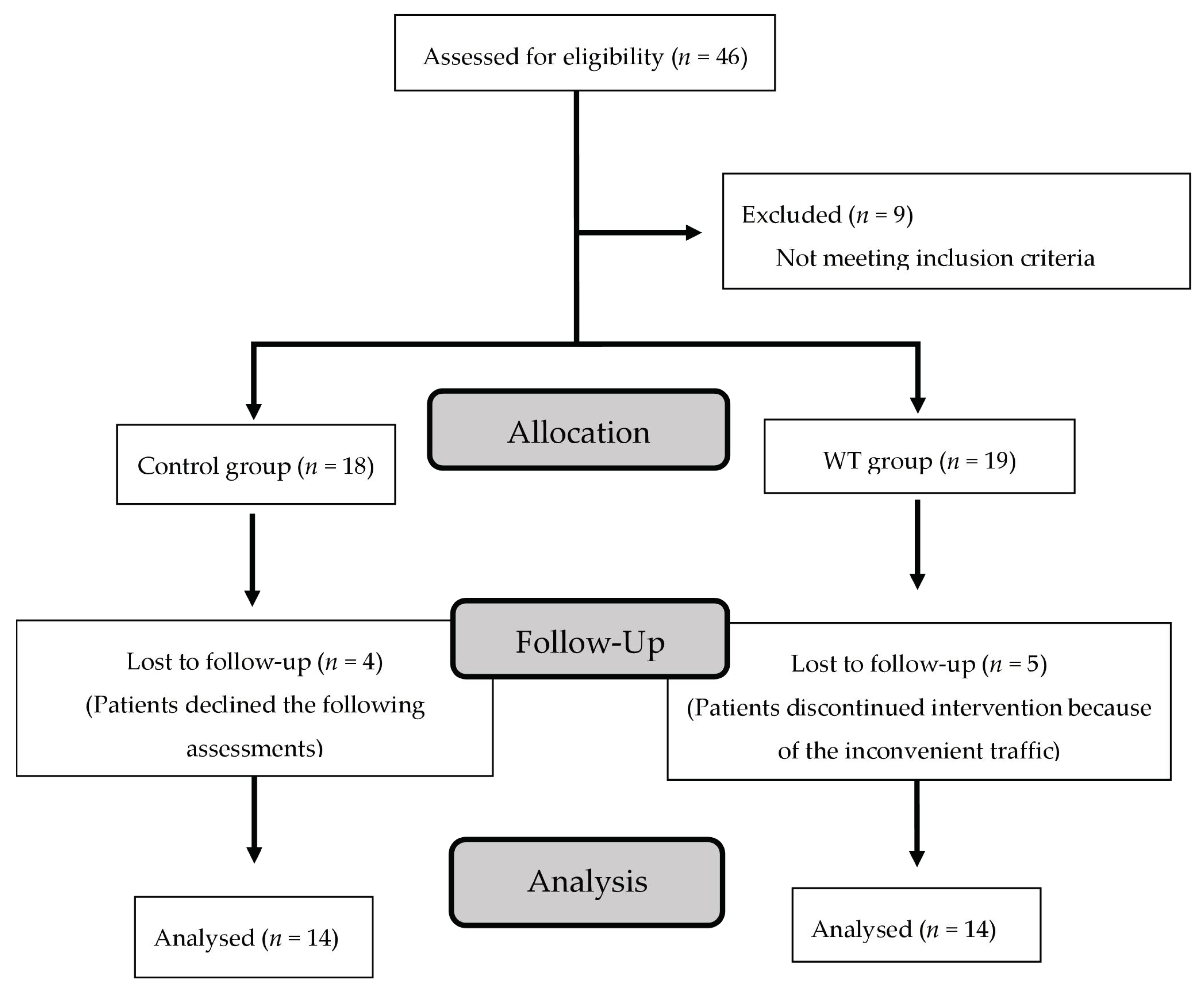
Several limitations of this study should be acknowledged. First, evidence regarding the entire effect of WT in TKA was restricted because of the small sample size in this retrospective study. Nevertheless, improvements in muscle strength and function over time indicated the benefits of WT in TKA. Second, our results (12 months after surgery) did not fully demonstrate the long-term effects of WT. The results showed that multiple metrics gradually improved in the CON group. Third, there was no random allocation, and certain participants could be more motivated, which could influence the results. Thus, a larger randomized controlled trial is needed to verify the findings of this study, as it was limited to only 28 who completed the study out of 46 total patients. Fourth, neuromuscular activation also plays a critical role in muscle function. Electromyography of the lower limbs might be included for greater clarity regarding the effect of WT on the neuromuscular system in further study.
5. Conclusions
During WT, no patient in the WT exercise group reported discomfort or injury or required further medical management. The 9 km/week WT protocol is feasible for TKA patients. The WT could significantly improve muscle strength (knee flexion and extension), functional outcome (6WT and 8UG), and QoL of patients. The simplicity of WT could reduce the limitations of poor supervision, impaired exercise adherence, and low compliance with exercise regimens, which cause poor rehabilitation outcomes. The authors believe that WT should be broadly applied in the rehabilitation of patients who have undergone TKA.


 ,
, 

{kind=link}