
Systemic Inflammatory Response Index (SIRI) as a Predictive Marker for Adverse Outcomes in Children with New-Onset Type 1 Diabetes Mellitus
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Protocol
2.2. Clinical and Laboratory Data
2.3. Key Outcome Measures
2.4. Use of OpenAI ChatGPT-3.5
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Comparison of SIRI According to Infection Status in Severe DKA Patients
3.3. Correlation Analysis of SIRI with Adverse Events
3.4. Association Analysis between SIRI and Adverse Events
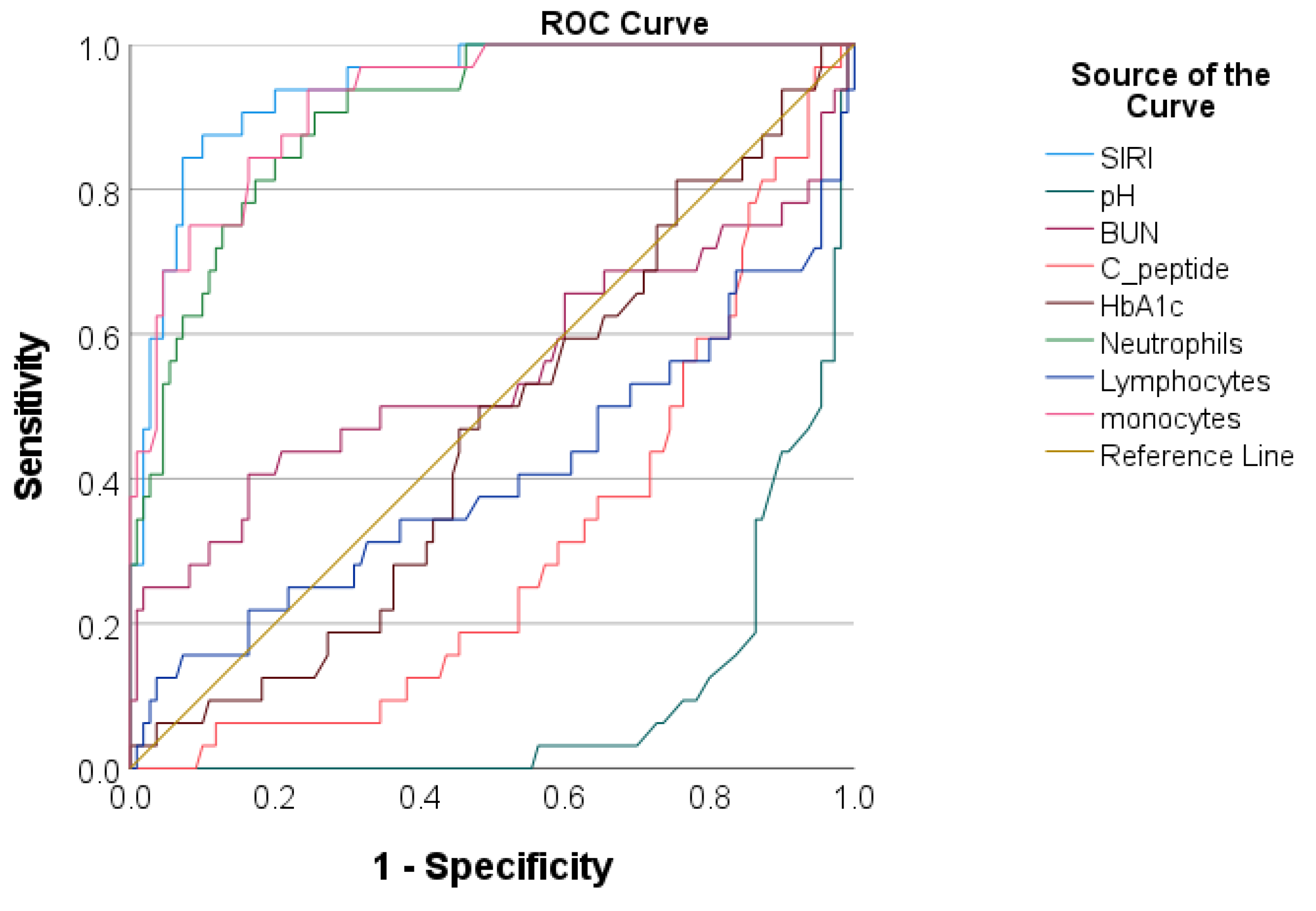
ROC Analysis Regarding the Predictive Accuracy of SIRI for Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Madrigal, M.A.; López, M.; Sánchez, A.; Cao, M.J.; Castro, M.J.; Jiménez, J.M. Type 1 Diabetes Mellitus in Pediatric Patients and Its Impact on Relationships in the Family Environment. Diabetes Metab. Syndr. Obes. 2020, 13, 4973–4980. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Del Pozo, P.; Aránguiz, D.; Córdova, G.; Scheu, C.; Valle, P.; Cerda, J.; García, H.; Hodgson, M.I.; Castillo, A. Clinical profile of children with diabetic ketoacidosis in fifteen years of management in a Critical Care Unit. Perfil clínico de niños con cetoacidosis diabética en una Unidad de Paciente Crítico. Rev. Chil. Pediatr. 2018, 89, 491–498. [Google Scholar] [PubMed]
- Souza, L.C.V.F.; Kraemer, G.C.; Koliski, A.; Carreiro, J.E.; Cat, M.N.L.; Lacerda, L.; França, S.N. Diabetic Ketoacidosis as the Initial Presentation of Type 1 Diabetes in Children and Adolescents: Epidemiological Study In Southern Brazil. Rev. Paul. Pediatr. 2019, 38, e2018204. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- International Diabetes Federation (IDF). IDF Diabetes Atlas 6; IDF: Brussels, Belgium, 2013. [Google Scholar]
- Namatame, K.; Igarashi, Y.; Nakae, R.; Suzuki, G.; Shiota, K.; Miyake, N.; Ishii, H.; Yokobori, S. Cerebral edema associated with diabetic ketoacidosis: Two case reports. Acute Med. Surg. 2023, 10, e860. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wolfsdorf, J.; Glaser, N.; Sperling, M.A. American Diabetes Association. Diabetic ketoacidosis in infants, children, and adolescents: A consensus statement from the American Diabetes Association. Diabetes Care 2006, 29, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Cameron, F.J.; Scratch, S.E.; Nadebaum, C.; Northam, E.A.; Koves, I.; Jennings, J.; Finney, K.; Neil, J.J.; Wellard, R.M.; Mackay, M.; et al. Neurological consequences of diabetic ketoacidosis at initial presentation of type 1 diabetes in a prospective cohort study of children. Diabetes Care 2014, 37, 1554–1562. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jefferies, C.A.; Nakhla, M.; Derraik, J.G.; Gunn, A.J.; Daneman, D.; Cutfield, W.S. Preventing Diabetic Ketoacidosis. Pediatr. Clin. N. Am. 2015, 62, 857–871. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.K.; Huang, C.Y.; Lin, C.H.; Cheng, B.W.; Chiang, Y.T.; Lee, Y.C.; Yeh, S.N.; Chan, C.I.; Chua, W.K.; Lee, Y.J.; et al. Acute kidney injury is a common complication in children and adolescents hospitalized for diabetic ketoacidosis. PLoS ONE 2020, 15, e0239160. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meena, J.; Yadav, J.; Kumar, J.; Dawman, L.; Tiewosh, K.; Mittal, A.; Kumar, R.; Dayal, D. Incidence, predictors, and short-term outcomes of acute kidney injury in children with diabetic ketoacidosis: A systematic review. Pediatr. Nephrol. 2023, 38, 2023–2031. [Google Scholar] [CrossRef] [PubMed]
- Abbas, Q.; Arbab, S.; Haque, A.U.; Humayun, K.N. Spectrum of complications of severe DKA in children in pediatric Intensive Care Unit. Pak. J. Med. Sci. 2018, 34, 106–109. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bialo, S.R.; Agrawal, S.; Boney, C.M.; Quintos, J.B. Rare complications of pediatric diabetic ketoacidosis. World J. Diabetes 2015, 6, 167–174. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rubinow, K.B.; Rubinow, D.R. In immune defense: Redefining the role of the immune system in chronic disease. Dialogues Clin. Neurosci. 2017, 19, 19–26. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Imtiaz, F.; Shafique, K.; Mirza, S.S.; Ayoob, Z.; Vart, P.; Rao, S. Neutrophil lymphocyte ratio as a measure of systemic inflammation in prevalent chronic diseases in Asian population. Int. Arch. Med. 2012, 5, 2. [Google Scholar] [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.K. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Eizirik, D.L.; Colli, M.L.; Ortis, F. The role of inflammation in insulitis and beta-cell loss in type 1 diabetes. Nat. Rev. Endocrinol. 2009, 5, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Eizirik, D.L.; Mandrup-Poulsen, T. A choice of death—The signal-transduction of immune-mediated beta-cell apoptosis. Diabetologia 2001, 44, 2115–2133. [Google Scholar] [CrossRef] [PubMed]
- Cnop, M.; Welsh, N.; Jonas, J.C.; Jörns, A.; Lenzen, S.; Eizirik, D.L. Mechanisms of pancreatic beta-cell death in type 1 and type 2 diabetes: Many differences, few similarities. Diabetes 2005, 54 (Suppl. S2), S97–S107. [Google Scholar] [CrossRef] [PubMed]
- Zeb, A.; Khurshid, S.; Bano, S.; Rasheed, U.; Zammurrad, S.; Khan, M.S.; Aziz, W.; Tahir, S. The Role of the Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio as Markers of Disease Activity in Ankylosing Spondylitis. Cureus 2019, 11, e6025. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cheng, Y.; Yu, W.; Zhou, Y.; Zhang, T.; Chi, H.; Xu, C. Novel predictor of the occurrence of DKA in T1DM patients without infection: A combination of neutrophil/lymphocyte ratio and white blood cells. Open Life Sci. 2021, 16, 1365–1376. [Google Scholar] [CrossRef] [PubMed]
- Ilhan, C.; Citirik, M.; Uzel, M.M.; Kiziltoprak, H.; Tekin, K. The usefulness of systemic inflammatory markers as diagnostic indicators of the pathogenesis of diabetic macular edema. Arq. Bras. Oftalmol. 2020, 83, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Zhu, Y.; Wang, J.; Wang, G.; Wu, Y. The Predictive Value of Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Levels of Diabetic Peripheral Neuropathy. J. Pain Res. 2021, 14, 2049–2058. [Google Scholar] [CrossRef] [PubMed]
- Scutca, A.C.; Nicoară, D.M.; Mărăzan, M.; Brad, G.F.; Mărginean, O. Neutrophil-to-Lymphocyte Ratio Adds Valuable Information Regarding the Presence of DKA in Children with New-Onset T1DM. J. Clin. Med. 2022, 12, 221. [Google Scholar] [CrossRef]
- Thiem, K.; van Dierendonck XA, M.H.; Janssen AW, M.; Boogaard, J.P.; Riksen, N.P.; Tack, C.J.; Stienstra, R. A High Glycemic Burden Relates to Functional and Metabolic Alterations of Human Monocytes in Patients with Type 1 Diabetes. Diabetes 2020, 69, 2735–2746. [Google Scholar] [CrossRef] [PubMed]
- Min, D.; Brooks, B.; Wong, J.; Salomon, R.; Bao, W.; Harrisberg, B.; Twigg, S.M.; Yue, D.K.; McLennan, S.V. Alterations in monocyte CD16 in association with diabetes complications. Mediat. Inflamm. 2012, 2012, 649083. [Google Scholar] [CrossRef]
- Bradshaw, E.M.; Raddassi, K.; Elyaman, W.; Orban, T.; Gottlieb, P.A.; Kent, S.C.; Hafler, D.A. Monocytes from patients with type 1 diabetes spontaneously secrete proinflammatory cytokines inducing Th17 cells. J. Immunol. 2009, 183, 4432–4439. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Josefsen, K.; Nielsen, H.; Lorentzen, S.; Damsbo, P.; Buschard, K. Circulating monocytes are activated in newly diagnosed type 1 diabetes mellitus patients. Clin. Exp. Immunol. 1994, 98, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Glaser, N.; Chu, S.; Hung, B.; Fernandez, L.; Wulff, H.; Tancredi, D.; ODonnell, M.E. Acute and chronic neuroinflammation is triggered by diabetic ketoacidosis in a rat model. BMJ Open Diabetes Res. Care 2020, 8, e001793. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zeng, H.; Ouyang, X.; Zhu, M.; Huang, Q.; Yu, W.; Ling, L.; Lan, H.Y.; Xu, A.; Tang, Y. The incidence, risk factors, and long-term outcomes of acute kidney injury in hospitalized diabetic ketoacidosis patients. BMC Nephrol. 2020, 21, 48. [Google Scholar] [CrossRef] [PubMed]
- Marchi, F.; Pylypiv, N.; Parlanti, A.; Storti, S.; Gaggini, M.; Paradossi, U.; Berti, S.; Vassalle, C. Systemic Immune-Inflammation Index and Systemic Inflammatory Response Index as Predictors of Mortality in ST-Elevation Myocardial Infarction. J. Clin. Med. 2024, 13, 1256. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- American Diabetes Association. Standards of Medical Care in Diabetes-2021 Abridged for Primary Care Providers. Clin. Diabetes 2021, 39, 14–43. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44 (Suppl. S1), S111–S124. [Google Scholar]
- Muir, A.B.; Quisling, R.G.; Yang, M.C.; Rosenbloom, A.L. Cerebral Edema in Childhood Diabetic Ketoacidosis: Natural history, radiographic findings, and early identification. Diabetes Care 2004, 27, 1541–1546. [Google Scholar] [CrossRef] [PubMed]
- Marzuillo, P.; Coppola, C.; Caiazzo, R.; Macchini, G.; Di Sessa, A.; Guarino, S.; Esposito, F.; Miraglia Del Giudice, E.; Tipo, V. Acute Kidney Injury in Children with Acute Appendicitis. Children 2022, 9, 620. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.J.; Work, D.F. Measurement and estimation of GFR in children and adolescents. Clin. J. Am. Soc. Nephrol. 2009, 4, 1832–1843. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.K.; Kaddourah, A.; Terrell, T.; Mottes, T.; Arnold, P.; Jacobs, J.; Andringa, J.; Goldstein, S.L.; Prospective Pediatric AKI Research Group. Assessment of worldwide acute kidney injury, renal angina and epidemiology in critically ill children (AWARE): Study protocol for a prospective observational study. BMC Nephrol. 2015, 16, 24. [Google Scholar] [CrossRef] [PubMed]
- Avner, E.D.; Harmon, W.E.; Niaudet, P.; Yoshikawa, N.; Emma, F.; Goldstein, S.L. Pediatric Nephrology. In Management of Chronic Kidney Disease, 6th ed.; Rene, G., VanDeVoorde, B., Warady, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; p. 1662. [Google Scholar]
- Zhou, V.L.; Shofer, F.S.; Desai, N.G.; Lorincz, I.S.; Mull, N.K.; Adler, D.H.; Greenwood, J.C. Predictors of Short Intensive Care Unit Stay for Patients with Diabetic Ketoacidosis Using a Novel Emergency Department-Based Resuscitation and Critical Care Unit. J. Emerg. Med. 2019, 56, 127–134. [Google Scholar] [CrossRef]
- Goldstein, B.; Giroir, B.; Randolph, A. International Consensus Conference on Pediatric Sepsis. International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr. Crit. Care Med. 2005, 6, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Zhuang, L.; Shen, Y.; Geng, Y.; Yu, S.; Chen, H.; Liu, L.; Meng, Z.; Wang, P.; Chen, Z. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer 2016, 122, 2158–2167. [Google Scholar] [CrossRef] [PubMed]
- OpenAI—Research. Available online: https://openai.com/research (accessed on 14 March 2024).
- Xu, W.; Wu, H.F.; Ma, S.G.; Bai, F.; Hu, W.; Jin, Y.; Liu, H. Correlation between peripheral white blood cell counts and hyperglycemic emergencies. Int. J. Med. Sci. 2013, 10, 758–765. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhou, D.; Wang, J.; Li, X. The Red Blood Cell Distribution Width-Albumin Ratio Was a Potential Prognostic Biomarker for Diabetic Ketoacidosis. Int. J. Gen. Med. 2021, 14, 5375–5380. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rains, J.L.; Jain, S.K. Oxidative stress, insulin signaling, and diabetes. Free Radic. Biol. Med. 2011, 50, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, M.; Shen, X. The association of oxidative stress and pro-inflammatory cytokines in diabetic patients with hyperglycemic crisis. J. Diabetes Complicat. 2014, 28, 662–666. [Google Scholar] [CrossRef]
- Shen, T.; Braude, S. Changes in serum phosphate during treatment of diabetic ketoacidosis: Predictive significance of severity of acidosis on presentation. Intern. Med. J. 2012, 42, 1347–1350. [Google Scholar] [CrossRef]
- Parackova, Z.; Zentsova, I.; Horvath, R.; Malcova, H.; Cebecauerova, D.; Sediva, A.; Klocperk, A. Immunomodulation of neutrophils and platelets by TNF blockage in patients with juvenile idiopathic arthritis. Clin. Immunol. 2022, 245, 109170. [Google Scholar] [CrossRef] [PubMed]
- Koulmanda, M.; Budo, E.; Bonner-Weir, S.; Qipo, A.; Putheti, P.; Degauque, N.; Shi, H.; Fan, Z.; Flier, J.S.; Auchincloss, H., Jr.; et al. Modification of adverse inflammation is required to cure new-onset type 1 diabetic hosts. Proc. Natl. Acad. Sci. USA 2007, 104, 13074–13079. [Google Scholar] [CrossRef] [PubMed]
- Ablamunits, V.; Sherry, N.A.; Kushner, J.A.; Herold, K.C. Autoimmunity and beta cell regeneration in mouse and human type 1 diabetes: The peace is not enough. Ann. N. Y. Acad. Sci. 2007, 1103, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Zipris, D. Innate immunity and its role in type 1 diabetes. Curr. Opin. Endocrinol. Diabetes Obes. 2008, 15, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.; Peng, J.; Li, Z.; Wong, F.S. The effect of innate immunity on autoimmune diabetes and the expression of Toll-like receptors on pancreatic islets. J. Immunol. 2004, 172, 3173–3180. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, P.; Dotta, F.; Ling, Z.; Lupi, R.; Del Guerra, S.; Santangelo, C.; Realacci, M.; Marselli, L.; Di Mario, U.; Navalesi, R. Function of pancreatic islets isolated from a type 1 diabetic patient. Diabetes Care 2000, 23, 701–703. [Google Scholar] [CrossRef] [PubMed]
- López-Verdugo, F.; Furuzawa-Carballeda, J.; Romero-Hernández, F.; Coss-Adame, E.; Valdovinos, M.A.; Priego-Ranero, A.; Olvera-Prado, H.; Narváez-Chavez, S.; Peralta-Figueroa, J.; Torres-Villalobos, G. Hematological indices as indicators of silent inflammation in achalasia patients: A cross-sectional study. Medicine 2020, 99, e19326. [Google Scholar] [CrossRef] [PubMed]
- Wan, H.; Wang, Y.; Fang, S.; Chen, Y.; Zhang, W.; Xia, F.; Wang, N.; Lu, Y. Associations between the Neutrophil-to-Lymphocyte Ratio and Diabetic Complications in Adults with Diabetes: A Cross-Sectional Study. J. Diabetes Res. 2020, 2020, 6219545. [Google Scholar] [CrossRef] [PubMed]
- Scutca, A.C.; Nicoară, D.M.; Mang, N.; Jugănaru, I.; Brad, G.F.; Mărginean, O. Correlation between Neutrophil-to-Lymphocyte Ratio and Cerebral Edema in Children with Severe Diabetic Ketoacidosis. Biomedicines 2023, 11, 2976. [Google Scholar] [CrossRef] [PubMed]
- Jarpe, A.J.; Hickman, M.R.; Anderson, J.T.; Winter, W.E.; Peck, A.B. Flow cytometric enumeration of mononuclear cell population infiltrating the islets of Langerhans in prediabetic NOD mice: Development of a model of autoimmune insulitis for type I diabetes. Reg. Immunol. 1990, 91, 305–317. [Google Scholar]
- Papaccio, G.; Esposito, V. Ultrastructural observations on cytotoxic effector cells infiltrating pancreatic islets of low-dose streptozotocin treated mice. Virchows Arch. A Pathol. Anat. Histopathol. 1992, 420, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Kolb-Bachofen, V.; Epstein, S.; Kiesel, U.; Kolb, H. Low dose streptozocin-induced diabetes in mice. Electron microscopy reveals singlecell insulitis before diabetes onset. Diabetes 1988, 37, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Saha, P.; Geissmann, F. Toward a functional characterization of blood monocytes. Immunol. Cell Biol. 2011, 89, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Mysliwska, J.; Smardzewski, M.; Marek-Trzonkowska, N.; Mysliwiec, M.; Raczynska, K. Expansion of CD14+ CD16+ monocytes producing TNF-alpha in complication-free diabetes type 1 juvenile onset patients. Cytokine 2012, 60, 309–317. [Google Scholar] [CrossRef]
- Joussen, A.M.; Doehmen, S.; Le, M.L.; Koizumi, K.; Radetzky, S.; Krohne, T.U.; Poulaki, V.; Semkova, I.; Kociok, N. TNF-α mediated apoptosis plays an important role in the development of early diabetic retinopathy and long-term histopathological alterations. Mol. Vis. 2009, 15, 1418–1428. [Google Scholar] [PubMed]
- Zorena, K.; Mysliwska, J.; Mysliwiec, M.; Balcerska, A.; Hak, L.; Lipowski, P.; Raczynska, K. Serum TNF-α level predicts nonproliferative diabetic retinopathy in children. Mediat. Inflamm. 2007, 2007, 92196. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; Mou, W.; Su, C.; Chen, X.; Zhang, H.; Cao, B.; Li, X.; Wu, D.; Ni, X.; Gui, J.; et al. Increase in Peripheral Blood Intermediate Monocytes is Associated with the Development of Recent-Onset Type 1 Diabetes Mellitus in Children. Int. J. Biol. Sci. 2017, 13, 209–218. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, S.; Pan, X.; Jia, B.; Chen, S. Exploring the Correlation Between the Systemic Immune Inflammation Index (SII), Systemic Inflammatory Response Index (SIRI), and Type 2 Diabetic Retinopathy. Diabetes Metab. Syndr. Obes. 2023, 16, 3827–3836. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lin, K.; Lan, Y.; Wang, A.; Yan, Y.; Ge, J. The association between a novel inflammatory biomarker, systemic inflammatory response index and the risk of diabetic cardiovascular complications. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Fan, X.; Xu, Y.; Wang, K.; Xu, T.; Han, T.; Hu, C.; Li, R.; Lin, X.; Jin, L. Association between inflammatory biomarkers and mortality in individuals with type 2 diabetes: NHANES 2005–2018. Diabetes Res. Clin. Pract. 2024, 209, 111575. [Google Scholar] [CrossRef] [PubMed]
- Dżygało, K.; Nowaczyk, J.; Szwilling, A.; Kowalska, A. Increased Frequency of Severe Diabetic Ketoacidosis at Type 1 Diabetes Onset Among Children During COVID-19 Pandemic Lockdown: An Observational Cohort Study. Pediatr. Endocrinol. Diabetes Metab. 2020, 26, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Dilek, S.Ö.; Gürbüz, F.; Turan, İ.; Celiloğlu, C.; Yüksel, B. Changes in the presentation of newly diagnosed type 1 diabetes in children during the COVID-19 pandemic in a tertiary center in Southern Turkey. J. Pediatr. Endocrinol. Metab. J. Pediatr. Endocrinol. Metab. 2021, 34, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Boboc, A.A.; Novac, C.N.; Ilie, M.T.; Ieșanu, M.I.; Galoș, F.; Bălgrădean, M.; Berghea, E.C.; Ionescu, M.D. The Impact of SARS-CoV-2 Pandemic on the New Cases of T1DM in Children. A Single-Centre Cohort Study. J. Pers. Med. 2021, 11, 551. [Google Scholar] [CrossRef] [PubMed]
- Bogale, K.T.; Hale, D.E.; Schaefer, E.; Bangalore Krishna, K. Prevalence and factors associated with diabetic ketoacidosis at diagnosis of type 1 diabetes: A report from a tertiary medical center in Central Pennsylvania. Endocrinol. Diabetes Metab. 2020, 4, e00186. [Google Scholar] [CrossRef] [PubMed]
- Poovazhagi, V. Risk factors for mortality in children with diabetic keto acidosis from developing countries. World J. Diabetes 2014, 5, 932–938. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Whang, J.E.; Wu, Y.-L.; Chen, J.-Y.; Kor, C.-T.; Lee, M.-S. Factors Associated with Prolonged Intensive Care Unit Treatment and Organ Failure in Pediatric Patients with Diabetic Ketoacidosis. Pediatr. Respirol. Crit. Care Med. 2023, 7, 13–19. [Google Scholar] [CrossRef]
- Everett, E.M.; Copeland, T.P.; Moin, T.; Wisk, L.E. National Trends in Pediatric Admissions for Diabetic Ketoacidosis, 2006–2016. J. Clin. Endocrinol. Metab. 2021, 106, 2343–2354. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Tertiles of SIRI | p-Value | ||
|---|---|---|---|---|
| 1 (0.14–1.07) n = 62 | 2 (1.19–5.04) n = 62 | 3 (5.31–69.88) n = 62 | ||
| Demographic characteristics | ||||
| 9.05 (4.07, 12.7) | 8.10 (4.75, 12.2) | 10.8 (7.05, 14) | 0.086 |
| 46.8 (29) | 54.8 (34) | 61.3 (38) | 0.267 |
| 134 (105–158) | 127 (109–153) | 143 (122–156) | 0.192 |
| 28.5 (16.6–44) | 25 (15.7–44) | 33.5 (19–47.7) | 0.213 |
| 15.6 (14.3–18.06) | 15.9 (13.8–18.1) | 16.1 (13.9–19.9) | 0.695 |
| Co-infection | 11.3 (7) | 16.1 (10) | 32.3 (20) | 0.011 |
| DKA status: | ||||
| 56.5 (35) | 24.2 (15) | 0 (0) | <0.001 |
| 22.6 (14) | 11.3 (7) | 0 (0) | <0.001 |
| 12.9 (8) | 24.2 (15) | 6.5 (4) | <0.001 |
| 8.1 (5) | 40.3 (25) | 93.5 (58) | <0.001 |
| GCS | 15 (15, 15) | 15 (15, 15) | 14 (12, 15) | 0.001 |
| LOS in ICU (days) | 0 (0, 0) | 0 (0, 39) | 55.5 (38, 73) | 0.001 |
| Acute complications: | ||||
| 0 (0) | 0 (0) | 12.9 (8) | <0.001 |
| 3.2 (2) | 19.4 (12) | 67.7 (42) | 0.003 |
| 1.6 (1) | 0 (0, 0) | 11.3 (7) | <0.001 |
| 3.2 (2) | 4.8 (3) | 12.9 (8) | 0.003 |
| Mechanical ventilation | 1.6 (1) | 0 (0) | 9.7 (6) | 0.002 |
| Death | 0 (0) | 0 (0) | 0 (0) | - |
| Laboratory parameters | ||||
| 7.8 (6.29, 10.08) | 11.43 (8.66, 15.08) | 18.91 (15.98, 25.76) | 0.001 |
| 3.63 (2.86, 4.53) | 7.27 (5.27, 9.46) | 14.68 (11.87, 23.98) | 0.001 |
| 3.43 (2.43, 4.67) | 2.89 (2.06, 4.01) | 2.40 (1.70, 3.44) | <0.001 |
| 0.56 (0.41, 0.71) | 0.90 (0.68, 1.25) | 2.01 (1.38, 2.81) | 0.001 |
| 0.10 (0.05, 0.19) | 0.05 (0.02, 0.14) | 0.01 (0, 0.02) | <0.001 |
| 283 (188, 342) | 319 (255, 400) | 363 (298, 438) | <0.001 |
| 7.31 (7.23, 7.36) | 7.14 (7.01, 7.28) | 6.95 (6.88, 7.02) | 0.001 |
| 347 (269, 463) | 430 (344, 500) | 471 (379, 560) | <0.001 |
| 11.70 (9.95, 13.24) | 11.30 (10.15, 12.72) | 11.53 (10.20, 12.69) | 0.871 |
| 0.572 (0.369, 0.726) | 0.542 (0.232, 0.739) | 0.310 (0.202, 0.479) | <0.001 |
| 0.61 (0.21–1.21) | 1.10 (0.83–3.85) | 3.66 (1.34–10.49) | <0.001 |
| 3.49 (2.93, 4.29) | 3.57 (2.66, 4.31) | 4.35 (2.69, 6.50) | 0.048 |
| 43 (34, 50) | 46 (37, 60) | 61 (47, 78.2) | <0.001 |
| 12 (9–15) | 12 (10–15) | 13 (10–18) | 0.575 |
| 16.5 (13–20) | 14.5 (12–20) | 14 (10–23) | 0.283 |
| Non-Adjusted a | Model 1 b | Model 2 c | ||||
|---|---|---|---|---|---|---|
| OR (95%CIs) | p-Value | OR (95%CIs) | p-Value | OR (95%CIs) | p-Value | |
| Entire study population | ||||||
| 1.180 (1.106–1.259) | <0.001 | 1.193 (1.116–1.276) | <0.001 | 1.103 (1.035–1.176) | 0.003 |
| 1.218 (1.135–1.307) | <0.001 | 1.250 (1.157–1.350) | <0.001 | 1.154 (1.064–1.252) | <0.001 |
| Severe DKA | ||||||
| 1.091 (1.027–1.158) | 0.004 | 1.103 (1.034–1.177) | 0.003 | 1.095 (1.031–1.164) | 0.003 |
| 1.047 (1.010–1.086) | 0.012 | 1.058 (1.015–1.103) | 0.008 | 1.053 (1.012–1.095) | 0.010 |
| AUC | SE | 95%CI | Sensitivity | Specificity | Cut-Off | p-Value | |
|---|---|---|---|---|---|---|---|
| SIRI | 0.837 | 0.032 | 0.774–0.900 | 0.820 | 0.720 | 2.66 | 0.001 |
| pH | 0.811 | 0.032 | 0.748–0.874 | 0.800 | 0.607 | 7.01 | 0.001 |
| BUN | 0.586 | 0.050 | 0.488–0.685 | 0.576 | 0.549 | 3.75 | 0.064 |
| C-peptide | 0.682 | 0.045 | 0.595–0.769 | 0.673 | 0.568 | 0.374 | 0.001 |
| HbA1c | 0.463 | 0.045 | 0.374–0.551 | 0.463 | 0.508 | 11.4 | 0.431 |
| Neutrophils | 0.793 | 0.036 | 0.722–0.864 | 0.787 | 0.720 | 8.21 | 0.001 |
| Lymphocytes | 0.584 | 0.044 | 0.498–0.670 | 0.576 | 0.525 | 2.68 | 0.063 |
| Monocytes | 0.812 | 0.032 | 0.749–0.874 | 0.803 | 0.664 | 0.935 | 0.001 |
| AUC | SE | 95%CI | Sensitivity | Specificity | Cut-Off | p-Value | |
|---|---|---|---|---|---|---|---|
| SIRI | 0.900 | 0.023 | 0.855–0.945 | 0.896 | 0.739 | 3.24 | <0.001 |
| pH | 0.894 | 0.023 | 0.849–0.940 | 0.877 | 0.625 | 6.97 | 0.001 |
| BUN | 0.543 | 0.059 | 0.427–0.658 | 0.522 | 0.627 | 4.09 | 0.393 |
| C-peptide | 0.709 | 0.047 | 0.617–0.802 | 0.708 | 0.647 | 0.367 | 0.001 |
| HbA1c | 0.471 | 0.051 | 0.371–0.571 | 0.455 | 0.523 | 11.5 | 0.559 |
| Neutrophils | 0.865 | 0.028 | 0.810–0.919 | 0.854 | 0.703 | 8.32 | 0.001 |
| Lymphocytes | 0.557 | 0.053 | 0.454–0.660 | 0.551 | 0.583 | 2.83 | 0.239 |
| Monocytes | 0.882 | 0026 | 0.831–0.933 | 0.875 | 0.717 | 1.14 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scutca, A.-C.; Jugănaru, I.; Nicoară, D.-M.; Brad, G.-F.; Bugi, M.-A.; Asproniu, R.; Cristun, L.-I.; Mărginean, O. Systemic Inflammatory Response Index (SIRI) as a Predictive Marker for Adverse Outcomes in Children with New-Onset Type 1 Diabetes Mellitus. J. Clin. Med. 2024, 13, 2582. https://doi.org/10.3390/jcm13092582
Scutca A-C, Jugănaru I, Nicoară D-M, Brad G-F, Bugi M-A, Asproniu R, Cristun L-I, Mărginean O. Systemic Inflammatory Response Index (SIRI) as a Predictive Marker for Adverse Outcomes in Children with New-Onset Type 1 Diabetes Mellitus. Journal of Clinical Medicine. 2024; 13(9):2582. https://doi.org/10.3390/jcm13092582
Chicago/Turabian StyleScutca, Alexandra-Cristina, Iulius Jugănaru, Delia-Maria Nicoară, Giorgiana-Flavia Brad, Meda-Ada Bugi, Raluca Asproniu, Lucian-Ioan Cristun, and Otilia Mărginean. 2024. "Systemic Inflammatory Response Index (SIRI) as a Predictive Marker for Adverse Outcomes in Children with New-Onset Type 1 Diabetes Mellitus" Journal of Clinical Medicine 13, no. 9: 2582. https://doi.org/10.3390/jcm13092582