
Changes in Maternal Heart Rate Variability and Photoplethysmography Morphology after Corticosteroid Administration: A Prospective, Observational Study

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Main Analysis: The Effect of Administering Betamethasone on mHRV
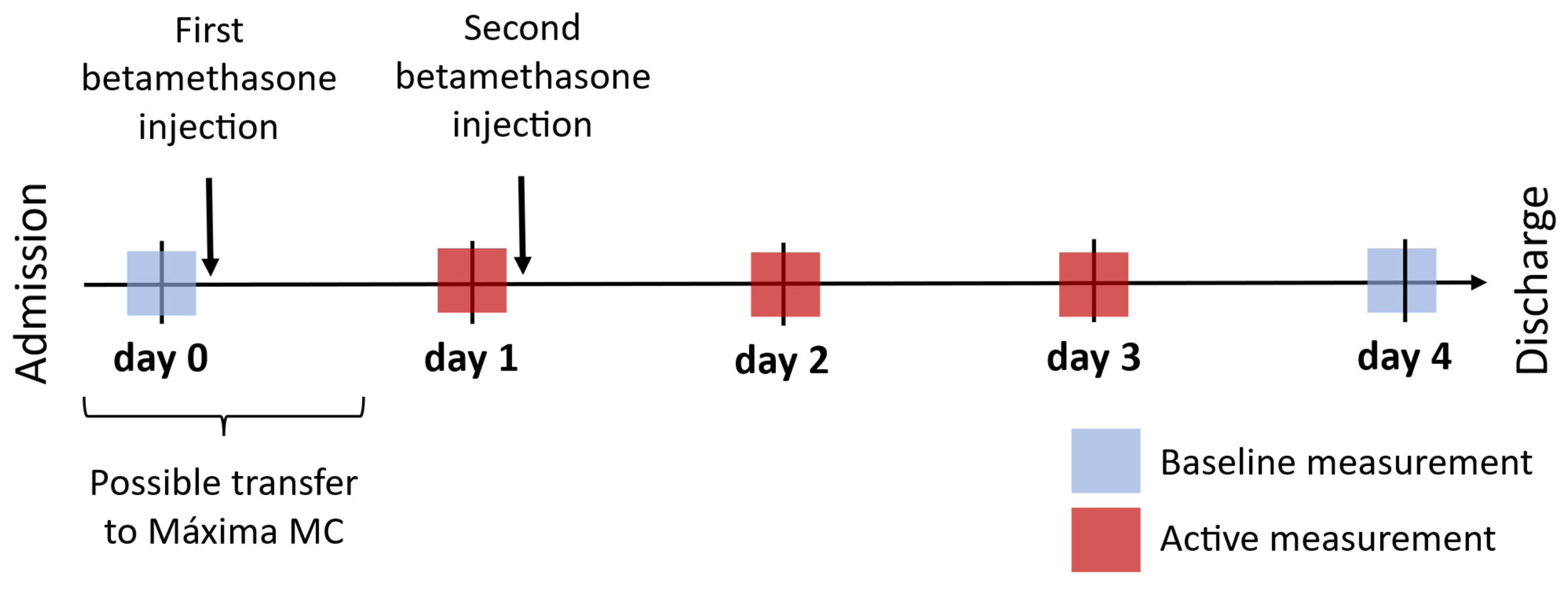
2.2.1. Timing of Measurements

2.2.2. Segment Selection
2.2.3. Preprocessing of PPG Measurements for HRV Analysis
2.2.4. Determining HR and HRV Features
2.3. Sub-Analysis: The Effect of Administering Betamethasone on the Morphology of the PPG Pulse Wave
2.3.1. Preprocessing of PPG Measurements for Analysis of Morphological Features
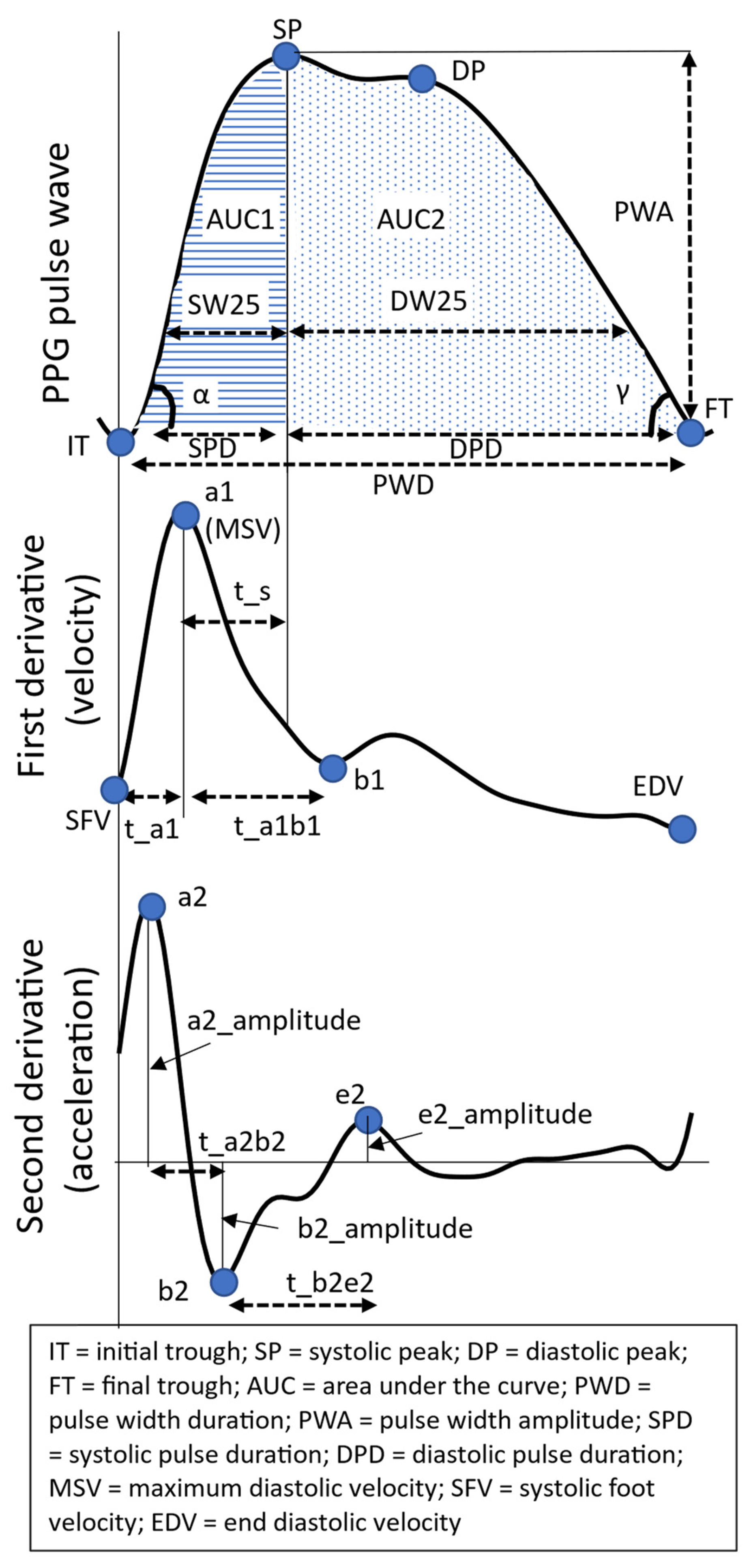
2.3.2. PPG Morphology Features
2.4. Statistical Analysis
3. Results
3.1. Study Group
3.2. Main Analysis: The Effect of Administering Betamethasone on mHRV
3.2.1. Mean HR and Time-Domain HRV Features

3.2.2. Frequency-Domain HRV Features

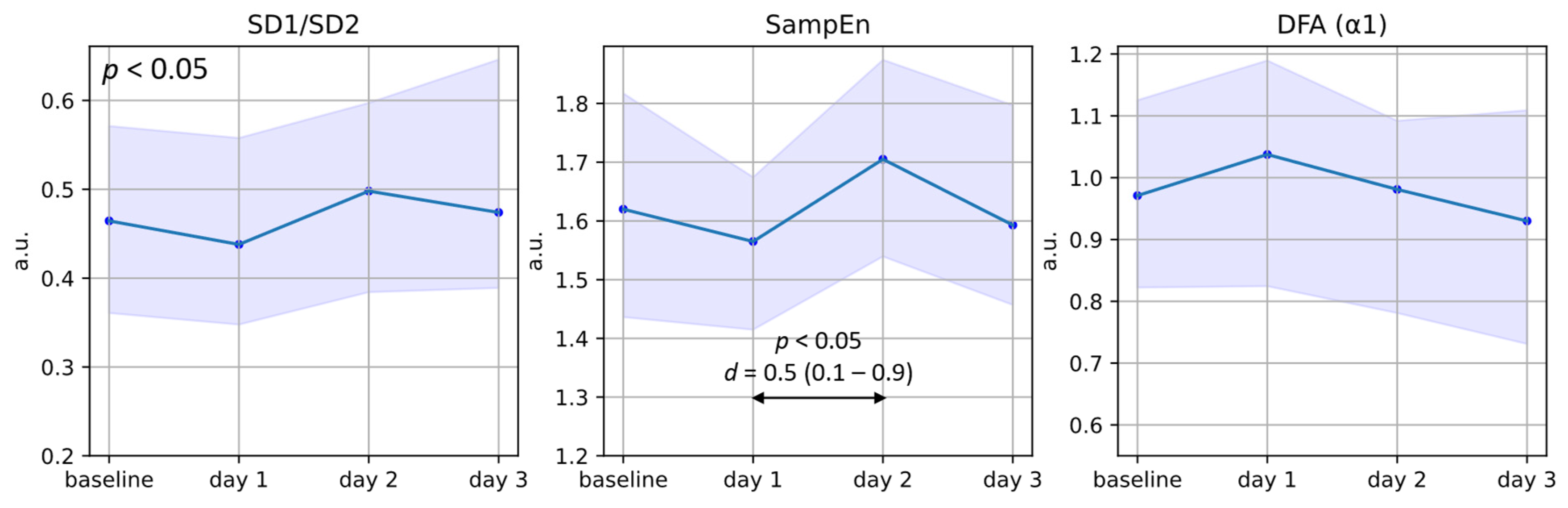
3.2.3. Non-Linear HRV Features

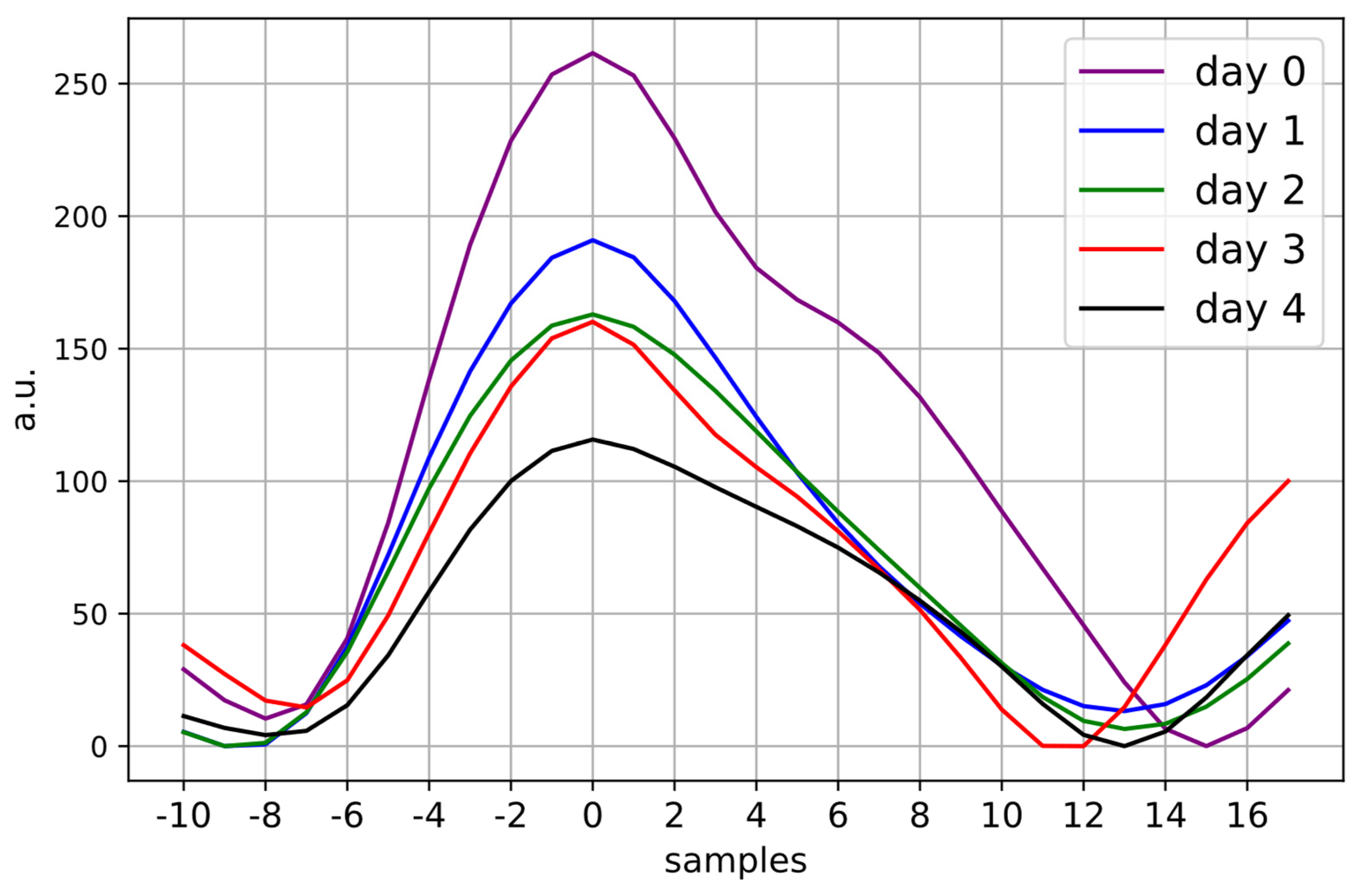
3.3. Changes in Maternal Morphological Features Extracted from the PPG Waveform

4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANS | autonomic nervous system |
| HPA | hypothalamus–pituitary–adrenal |
| HR | heart rate |
| HRV | heart rate variability |
| IPI | inter-pulse interval |
| PPG | photoplethysmography |
References
- Mate, A.; Reyes-Goya, C.; Santana-Garrido, Á.; Vázquez, C.M. Lifestyle, Maternal Nutrition and Healthy Pregnancy. Curr. Vasc. Pharmacol. 2021, 19, 132–140. [Google Scholar] [CrossRef]
- Cui, Y.; Zhu, B.; Zheng, F. Low-dose aspirin at ≤16 weeks of gestation for preventing preeclampsia and its maternal and neonatal adverse outcomes: A systematic review and meta-analysis. Exp. Ther. Med. 2018, 15, 4361–4369. [Google Scholar] [CrossRef] [PubMed]
- Rang, S.; Wolf, H.; Montfrans, G.A.; Karemaker, J.M. Non-invasive assessment of autonomic cardiovascular control in normal human pregnancy and pregnancy-associated hypertensive disorders: A review. J. Hypertens. 2002, 20, 2111–2119. [Google Scholar] [CrossRef] [PubMed]
- Pal, G.; Shyma, P.; Habeebullah, S.; Shyjus, P.; Pal, P. Spectral Analysis of Heart Rate Variability for Early Prediction of Pregnancy-Induced Hypertension. Clin. Exp. Hypertens. 2009, 31, 330–341. [Google Scholar] [CrossRef] [PubMed]
- Rowan, S.P.; Lilly, C.L.; Claydon, E.A.; Wallace, J.; Merryman, K. Monitoring one heart to help two: Heart rate variability and resting heart rate using wearable technology in active women across the perinatal period. BMC Pregnancy Childbirth 2022, 22, 887. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Reyes, L.M.; Usselman, C.W.; Davenport, M.H.; Steinback, C.D. Sympathetic Nervous System Regulation in Human Normotensive and Hypertensive Pregnancies. Hypertension 2018, 71, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Reyes, L.M.; Khurana, R.; Usselman, C.W.; Busch, S.A.; Skow, R.J.; Boulé, N.G.; Davenport, M.H.; Steinback, C.D. Sympathetic nervous system activity and reactivity in women with gestational diabetes mellitus. Physiol. Rep. 2020, 8, e14504. [Google Scholar] [CrossRef]
- Khlybova, S.V.; Tsirkin, V.I.; Dvoryanskii, S.A.; Makarova, I.A.; Trukhin, A.N. Heart rate variability in normal and complicated pregnancies. Hum. Physiol. 2008, 34, 625–632. [Google Scholar] [CrossRef]
- Moors, S.; Staaks, K.; Westerhuis, M.; Dekker, L.; Verdurmen, K.; Oei, S.; van Laar, J. Heart rate variability in hypertensive pregnancy disorders: A systematic review. Pregnancy Hypertens. 2020, 20, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Seeck, A.; Baumert, M.; Fischer, C.; Khandoker, A.; Faber, R.; Voss, A. Advanced Poincaré plot analysis differentiates between hypertensive pregnancy disorders. Physiol. Meas. 2011, 32, 1611–1622. [Google Scholar] [CrossRef]
- Casati, D.; Stampalija, T.; Ferrazzi, E.; Alberti, A.; Scebba, I.; Paganelli, A.; Di Martino, D.; Muggiasca, M.; Bauer, A. Maternal cardiac deceleration capacity: A novel insight into maternal autonomic function in pregnancies complicated by hypertensive disorders and intrauterine growth restriction. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 206, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.M.; Lackner, H.K.; Roessler, A.; Papousek, I.; Kolovetsiou-Kreiner, V.; Lucovnik, M.; Schmid-Zalaudek, K.; Lang, U.; Moertl, M.G. Heart rate variability and baroreceptor reflex sensitivity in early- versus late-onset preeclampsia. PLoS ONE 2017, 12, e0186521. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Verdurmen, K.M.; Renckens, J.; van Laar, J.O.; Oei, S.G. The influence of corticosteroids on fetal heart rate variability: A systematic review of the literature. Obstet. Gynecol. Surv. 2013, 68, 811–824. [Google Scholar] [CrossRef] [PubMed]
- Verdurmen, K.M.; Warmerdam, G.J.; Lempersz, C.; Hulsenboom, A.D.; Renckens, J.; Dieleman, J.P.; Vullings, R.; van Laar, J.O.; Oei, S.G. The influence of betamethasone on fetal heart rate variability, obtained by non-invasive fetal electrocardiogram recordings. Early Hum. Dev. 2018, 119, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Noben, L.; Verdurmen, K.; Warmerdam, G.; Vullings, R.; Oei, S.; van Laar, J. The fetal electrocardiogram to detect the effects of betamethasone on fetal heart rate variability. Early Hum. Dev. 2019, 130, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Sapolsky, R.M.; Romero, L.M.; Munck, A.U. How Do Glucocorticoids Influence Stress Responses? Integrating Permissive, Suppressive, Stimulatory, and Preparative Actions. Endocr. Rev. 2000, 21, 35. [Google Scholar]
- Bester, M.; Moors, S.; Joshi, R.; Nichting, T.J.; van der Hout-van der Jagt, M.B.; Oei, S.G.; Mischi, M.; Vullings, R.; van Laar, J.O.E.H. Changes in Maternal Heart Rate Variability in Response to the Administration of Routine Obstetric Medication in Hospitalized Patients: Study Protocol for a Cohort Study (MAMA-Heart Study). Clin. Parct. 2021, 11, 13–25. [Google Scholar] [CrossRef]
- ACOG Practice Bulletin No. 188: Prelabor Rupture of Membranes. Obstet. Gynecol. 2018, 131, 2455. [CrossRef]
- ACOG practice Bulletin No. 127: Management of preterm labor. Obstet. Gynecol. 2012, 119, 1308–1317. [CrossRef]
- ACOG Practice Bulletin No. 202: Gestational Hypertension and Preeclampsia. Obstet. Gynecol. 2019, 133, 1. [CrossRef]
- Bester, M.; Joshi, R.; Linders, A.; Mischi, M.; van Laar, J.O.E.H.; Vullings, R. Characterizing the effect of demographics, cardiorespiratory factors, and inter-subject variation on maternal heart rate variability in pregnancy with statistical modeling: A retrospective observational analysis. Sci. Rep. 2022, 12, 19305. [Google Scholar] [CrossRef] [PubMed]
- Ekholm, E.M.K.; Hartiala, J.; Huikuri, H.V. Circadian rhythm of frequency-domain measures of heart rate variability in pregnancy. BJOG Int. J. Obstet. Gynaecol. 1997, 104, 825–828. [Google Scholar] [CrossRef] [PubMed]
- Jobe, A.H.; Milad, M.A.; Peppard, T.; Jusko, W.J. Pharmacokinetics and Pharmacodynamics of Intramuscular and Oral Betamethasone and Dexamethasone in Reproductive Age Women in India. Clin. Transl. Sci. 2019, 13, 391–399. [Google Scholar] [CrossRef] [PubMed]
- MSD. Celestone Chronodose, Suspensie Voor Injectie 5,7 mg/mL; Samenvatting van de productkenmerken RVG 05399; Merck Sharp & Dohme B.V.: Haarlen, The Netherlands, 2018. [Google Scholar]
- Eerikäinen, L.M.; Bonomi, A.G.; Schipper, F.; Dekker, L.R.C.; Vullings, R.; de Morree, H.M.; Aarts, R.M. Comparison between electrocardiogram- and photoplethysmogram-derived features for atrial fibrillation detection in free-living conditions. Physiol. Meas. 2018, 39, 084001. [Google Scholar] [CrossRef] [PubMed]
- Task Force of The European Society of Cardiology and The North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Khandoker, A.H.; Karmakar, C.; Brennan, M.; Palaniswami, M.; Voss, A. Poincaré Plot Methods for Heart Rate Variability Analysis; Springer: Boston, MA, USA, 2013. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed]
- Bakhchina, A.V.; Arutyunova, K.R.; Sozinov, A.A.; Demidovsky, A.V.; Alexandrov, Y.I. Sample Entropy of the Heart Rate Reflects Properties of the System Organization of Behaviour. Entropy 2018, 20, 449. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.-K.; Havlin, S.; Stanley, H.E.; Goldberger, A.L. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos 1995, 5, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Yeh, R.-G.; Shieh, J.-S.; Chen, G.-Y.; Kuo, C.-D. Detrended fluctuation analysis of short-term heart rate variability in late pregnant women. Auton. Neurosci. 2009, 150, 122–126. [Google Scholar] [CrossRef]
- Makowski, D.; Pham, T.; Lau, Z.J.; Brammer, J.C.; Lespinasse, F.; Pham, H.; Schölzel, C.; Chen, S.H.A. NeuroKit2: A Python toolbox for neurophysiological signal processing. Behav. Res. Methods 2021, 53, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1–R39. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.; Domer, B.; Wibmer, T.; Penzel, T. An Algorithm for Real-Time Pulse Waveform Segmentation and Artifact Detection in Photoplethysmograms. IEEE J. Biomed. Health Inform. 2017, 21, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Yang, L.; Shi, H.; Liu, C. Differences in photoplethysmography morphological features and feature time series between two opposite emotions: Happiness and sadness. Artery Res. 2017, 18, 7–13. [Google Scholar] [CrossRef]
- El Hajj, C.; Kyriacou, P.A. Recurrent Neural Network Models for Blood Pressure Monitoring Using PPG Morphological Features. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 1–5 November 2021; pp. 1865–1868. [Google Scholar] [CrossRef]
- Kelley, K. The Effects of Nonnormal Distributions on Confidence Intervals Around the Standardized Mean Difference: Bootstrap and Parametric Confidence Intervals. Educ. Psychol. Meas. 2005, 65, 51–69. [Google Scholar] [CrossRef]
- Musa, S. A8393 Sympathetic activity in preeclampsia, a study of heart rate variability. J. Hypertens. 2018, 36, e5. [Google Scholar] [CrossRef]
- Chaswal, M.; Kapoor, R.; Batra, A.; Verma, S.; Yadav, B.S. Heart Rate Variability and Cardiovascular Reflex Tests for Assessment of Autonomic Functions in Preeclampsia. Int. J. Hypertens. 2018, 2018, 8163824. [Google Scholar] [CrossRef] [PubMed]
- Tejera, E.; Areias, M.J.; Rodrigues, A.I.; Nieto-Villar, J.M.; Rebelo, I. Blood Pressure and Heart Rate Variability Complexity Analysis in Pregnant Women with Hypertension. Hypertens. Pregnancy 2011, 31, 91–106. [Google Scholar] [CrossRef]
- Faber, R.; Baumert, M.; Stepan, H.; Wessel, N.; Voss, A.; Walther, T. Baroreflex sensitivity, heart rate, and blood pressure variability in hypertensive pregnancy disorders. J. Hum. Hypertens. 2004, 18, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Brooks, V.L. Autonomic control during pregnancy. In Primer on the Autonomic Nervous System; Elsevier: Amsterdam, The Netherlands, 2023; pp. 273–277. [Google Scholar] [CrossRef]
- Brooks, V.L.; Fu, Q.; Shi, Z.; Heesch, C.M. Adaptations in autonomic nervous system regulation in normal and hypertensive pregnancy. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2020; Volume 171, pp. 57–84. [Google Scholar] [CrossRef]
- Bester, M.; Joshi, R.; van Dooren, J.H.A.M.; Mischi, M.; Vullings, R.; van Laar, J.O.E.H. Changes in Maternal Heart Rate and Autonomic Regulation following the Antenatal Administration of Corticosteroids: A Secondary Analysis. J. Clin. Med. 2023, 12, 588. [Google Scholar] [CrossRef] [PubMed]
- Haddad, S.; Souza, R.; Cecatti, J.; The WHO Intrapartum Care Algorithms Working Group. Management of maternal pulse and blood pressure abnormalities during labour and childbirth: Evidence-based algorithms for intrapartum care decision support. BJOG 2022. [Google Scholar] [CrossRef] [PubMed]
- Shields, L.E.; Wiesner, S.; Klein, C.; Pelletreau, B.; Hedriana, H.L. Use of Maternal Early Warning Trigger tool reduces maternal morbidity. Am. J. Obstet. Gynecol. 2016, 214, 527.e1–527.e6. [Google Scholar] [CrossRef]
- Moran, N.F.; Khaliq, O.P.; Ngene, N.C.; Moodley, J. Persistent maternal tachycardia: A clinical alert for healthcare professionals providing maternity care in South Africa. SAMJ 2022, 112, 403–404. [Google Scholar] [CrossRef]
- Koenen, S.V.; Mulder, E.J.H.; Wijnberger, L.D.; Visser, G.H.A. Transient Loss of the Diurnal Rhythms of Fetal Movements, Heart Rate, and Its Variation after Maternal Betamethasone Administration. Pediatr. Res. 2005, 57, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Ballard, L.; Ballard, A. Scientific basis and therapeutic regimens for use of antenatal glucocorticoids. Am. J. Obstet. Gynecol. 1995, 173, 9. [Google Scholar] [CrossRef] [PubMed]
- Yuda, E.; Shibata, M.; Ogata, Y.; Ueda, N.; Yambe, T.; Yoshizawa, M.; Hayano, J. Pulse rate variability: A new biomarker, not a surrogate for heart rate variability. J. Physiol. Anthr. 2020, 39, 21. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.; Shin, H. Photoplethysmography sampling frequency: Pilot assessment of how low can we go to analyze pulse rate variability with reliability? Physiol. Meas. 2017, 38, 586–600. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, A.; Pantelopoulos, A.; Emir-Farinas, H.; Natarajan, P. Heart rate variability with photoplethysmography in 8 fmillion individuals: A cross-sectional study. Lancet Digit. Health 2020, 2, e650–e657. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-K.; Hu, Y.-F.; Lin, S.-F. Methodological considerations in calculating heart rate variability based on wearable device heart rate samples. Comput. Biol. Med. 2018, 102, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Kiselev, A.R.; Karavaev, A.S. The intensity of oscillations of the photoplethysmographic waveform variability at frequencies 0.04–0.4 Hz is effective marker of hypertension and coronary artery disease in males. Blood Press. 2019, 29, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Middleton, P.M.; Chan, G.S.H.; Steel, E.; Malouf, P.; Critoph, C.; Flynn, G.; O’lone, E.; Celler, B.G.; Lovell, N.H. Fingertip photoplethysmographic waveform variability and systemic vascular resistance in intensive care unit patients. Med. Biol. Eng. Comput. 2011, 49, 859–866. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age 18 years and above | History of severe arrhythmia and/or maternal congenital heart disease |
| Gestational age 23 5/7 to 33 6/7 weeks | Diseases with known effects on ANS |
| Yet to receive the second betamethasone injection | Known allergies to hard plastic (e.g., used in sport watches) or elastic band material |
| Proficient in Dutch or English | Wounds, injuries, or infectious diseases on the wrist where the PPG device will be worn |
| Tattoo location on wrist interfering with the positioning of the PPG device | |
| Both wrists unavailable for wearing the PPG device (e.g., owing to intravenous lines) | |
| Dexamethasone (another brand of corticosteroid) administered instead of betamethasone |
| Features | Explanation | |
|---|---|---|
| Ampli-tude | PWA | Pulse width amplitude, i.e., the difference between SP and IT. |
| b2_amplitude | The absolute value of the amplitude of the deepest trough of the second derivative signal (b2) | |
| Time differences | PWD | Pulse width duration; time interval between IT and FT |
| SPD | Systolic phase duration; time interval between IT and SP | |
| DPD | Diastolic phase duration; time interval between SP and FT | |
| t_a1 | Time interval between IT and a1 on the first derivative signal | |
| t_a1b1 | Time interval between the a1 and the first valley of the first derivative signal (b1) | |
| t_a2b2 | Time interval between points a2 and b2 on the second derivative signal | |
| t_b2e2 | Time interval between points b2 and e2 on the second derivative signal | |
| AUC | AUC_total | AUC of the full pulse wave, i.e., between IT and FT |
| AUC1 | AUC of systolic phase, i.e., between IT and SP | |
| AUC2 | AUC of diastolic phase, i.e., between SP and FT | |
| Velocity and acceleration | mean(V) | Mean velocity, i.e., mean of the first derivative signal |
| IDR(V) | Interdecile range of velocity, i.e., interdecile range of the first derivative signal | |
| Mean (Acc) | Mean of the second derivative signal | |
| MSV | Max systolic velocity; a1 on the first derivative | |
| SFV | Systolic foot velocity, i.e., value of the point on the first derivative signal corresponding to IT of the pulse wave | |
| Ratio | DW10/SW10 | The ratio of systolic width to diastolic width at 10% of the pulse wave amplitude; similar features are calculated at 25%, 50%, and 60%. |
| t_s/PWD | The ratio between the time interval between a1 and SP (i.e., t_s), and the pulse width duration (PWD), which is the time interval between IT and FT | |
| t_a1/PWD | The ratio of the time interval between the IT and a1 (i.e., t_a1) to PWD | |
| t_a1b1/PWD | The ratio of t_a1b1 to PWD | |
| t_a2b2/PWD | The ratio of t_a2b2 to PWD | |
| t_b2e2/PWD | The ratio of t_b2e2 to PWD | |
| b2/a2 | The ratio of b2_amplitude to a2_amplitude, found on the second derivative signal | |
| e2/a2 | The ratio of e2_amplitude to a2_amplitude, found on the second derivative signal | |
| SPD/PWD | The ratio of SPD to PWD | |
| SP/SPD | The ratio of the value of SP to SPD | |
| Pulsatility index | Max systolic velocity (i.e., a1 on the first derivative)–end diastolic velocity (i.e., EDV on the first derivative)/(mean of the first derivative) | |
| Slope | slope_IT_SP | The slope of line that connects IT and SP |
| slope_SP_FT | The slope of line that connects SP and FT | |
| Angle | α | The angle of the slope between IT and SP |
| γ | The angle of the slope between SP and FT | |
| Characteristic | |
|---|---|
| Indication for betamethasone (no. of participants) | |
| Threatened preterm labor | 31 |
| Vaginal bleeding | 4 |
| Preterm rupture of membranes | 8 |
| Preeclampsia and/or HELLP syndrome * | 13 |
| Pregnancy-induced hypertension | 1 |
| Fetal growth restriction | 2 |
| Non-obstetric operation | 1 |
| Suspicion of twin anemia polycythemia sequence | 1 |
| Gestational age at first betamethasone injection | 28 weeks (26 weeks 3 days–30 weeks) |
| BMI (prepregnancy) | 24.95 (22.05–27.70) kg/m2 |
| Age | 31 (27–33) years |
| Nulliparous | 59.7% |
| Pregnancy with multiples | 24.2% |
| Co-administration of medications during study period (no. of participants) | |
| Atosiban | 11 |
| Azitromycin | 11 |
| Nifidipine | 19 |
| Penicillen | 2 |
| Magnesium sulfate | 19 |
| Methyldopa | 5 |
| Labetalol | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bester, M.; Nichting, T.J.; Joshi, R.; Aissati, L.; Oei, G.S.; Mischi, M.; van Laar, J.O.E.H.; Vullings, R. Changes in Maternal Heart Rate Variability and Photoplethysmography Morphology after Corticosteroid Administration: A Prospective, Observational Study. J. Clin. Med. 2024, 13, 2442. https://doi.org/10.3390/jcm13082442
Bester M, Nichting TJ, Joshi R, Aissati L, Oei GS, Mischi M, van Laar JOEH, Vullings R. Changes in Maternal Heart Rate Variability and Photoplethysmography Morphology after Corticosteroid Administration: A Prospective, Observational Study. Journal of Clinical Medicine. 2024; 13(8):2442. https://doi.org/10.3390/jcm13082442
Chicago/Turabian StyleBester, Maretha, Thomas J. Nichting, Rohan Joshi, Lamyae Aissati, Guid S. Oei, Massimo Mischi, Judith O. E. H. van Laar, and Rik Vullings. 2024. "Changes in Maternal Heart Rate Variability and Photoplethysmography Morphology after Corticosteroid Administration: A Prospective, Observational Study" Journal of Clinical Medicine 13, no. 8: 2442. https://doi.org/10.3390/jcm13082442