

Suicidal Ideations in Major Depressed Subjects: Role of the Temporal Dynamics of Anhedonia

Service de Psychiatrie et Laboratoire du Sommeil, Hôpital Universitaire de Bruxelles, Université libre de Bruxelles (ULB), Route de Lennik, 808-1070 Anderlecht, Belgium
*
Author to whom correspondence should be addressed.
Brain Sci. 2023, 13(7), 1065; https://doi.org/10.3390/brainsci13071065
Submission received: 27 June 2023
/
Revised: 10 July 2023
/
Accepted: 12 July 2023
/
Published: 13 July 2023
(This article belongs to the Special Issue Clinical Research on Mood Disorders: Opportunities and Challenges)
Abstract
:Given the limited data available in the literature, the aim of this study was to investigate the potential role played by the temporal dynamics of anhedonia (lifelong anhedonia and recent changes in anhedonia) in the occurrence of suicidal ideations in major depressed subjects. The clinical data of 285 major depressed subjects recruited from the database of the Erasme Hospital Sleep Laboratory were analyzed. A score on item nine of the Beck Depression Inventory (BDI-II) ≥1 and/or an identification during the systematic psychiatric assessment were used to determine the presence of suicidal ideations. The association between anhedonia complaints (lifelong anhedonia and recent change in anhedonia) and suicidal ideations in major depressed subjects was assessed by logistic regression analyzes. The prevalence of suicidal ideations was 39.3% in our sample of major depressed subjects. After adjusting for the main confounding factors, multivariate logistic regression analysis demonstrated that unlike lifelong anhedonia, only recent changes in anhedonia were a risk factor for suicidal ideations in major depressed subjects. Given this potential involvement of the recent change in anhedonia in the occurrence of suicidal ideations in major depressed subjects, it seems essential to better identify and adequately manage this specific form of anhedonia in order to open new perspectives for the prevention of suicide in this particular sub-population.
1. Introduction
Given recent data from the World Health Organization, suicide remains an important public health problem despite the various prevention strategies implemented in recent years [1]. Indeed, the annual number of deaths by suicide is estimated at 700,000 worldwide, and suicide remains one of the leading causes of death among 15–29 year-olds [1]. In the general population, major depressive disorder is one of the main risk factors for suicide since this psychiatric disorder is very frequently found during psychological autopsies in subjects who died by suicide [2,3]. However, in major depressed subjects, the occurrence of suicidal behavior (suicide attempt and suicide) is generally preceded by the development of suicidal ideations, which is a marker of the severity of major depressive episodes [4,5]. Nevertheless, despite a high prevalence (37.7%), suicidal ideations are frequently underdiagnosed in major depressed subjects, although they are associated with suicidal acts in 15% of cases [6,7,8]. Thus, since suicidal ideations seem to be the first step of the suicidal plan in major depressed subjects [9], it is essential to identify the potential factors involved in the occurrence of these suicidal ideations in order to better prevent excess mortality by suicide in this particular population.
In the literature, the available studies seem to indicate that some specific depressive symptoms play a central role in the development of suicidal ideations [10]. Among these, depressive symptoms are associated with a more frequent occurrence of suicidal ideations, and anhedonia is characterized by an inability to feel positive emotions during life situations that were previously considered pleasant [11]. However, despite the fact that anhedonia is a cardinal symptom of major depressive disorder [12], few studies have investigated the role played by this depressive symptom in the occurrence of suicidal ideations in major depressed subjects [13,14,15]. Moreover, unlike other specific subpopulations [16,17,18], the potential impact of the temporal dynamics of anhedonia (lifelong anhedonia and recent changes in anhedonia) on the risk of suicidal ideations has been few studied in major depressed subjects [19], which could limit the interpretation of most of the studies available in the literature. Thus, given these limited data, it seems necessary to carry out additional investigations to better understand the potential role played by the temporal dynamics of anhedonia (lifelong anhedonia and recent changes in anhedonia) in the occurrence of suicidal ideations in major depressed subjects.
The aim of this study was to investigate the risk of suicidal ideations associated with lifelong anhedonia and recent changes in anhedonia in a large sample of major depressed subjects. Our hypothesis was that, similar to other specific subpopulations, only recent changes in anhedonia are associated with a higher risk of suicidal ideations in major depressed subjects. The objective of this approach was to provide healthcare professionals with reliable data regarding the potential role played by the temporal dynamics of anhedonia (lifelong anhedonia and recent changes in anhedonia) in the occurrence of suicidal ideations in major depressed subjects to enable better prevention of mortality by suicide in this particular subpopulation.
2. Materials and Methods
2.1. Population
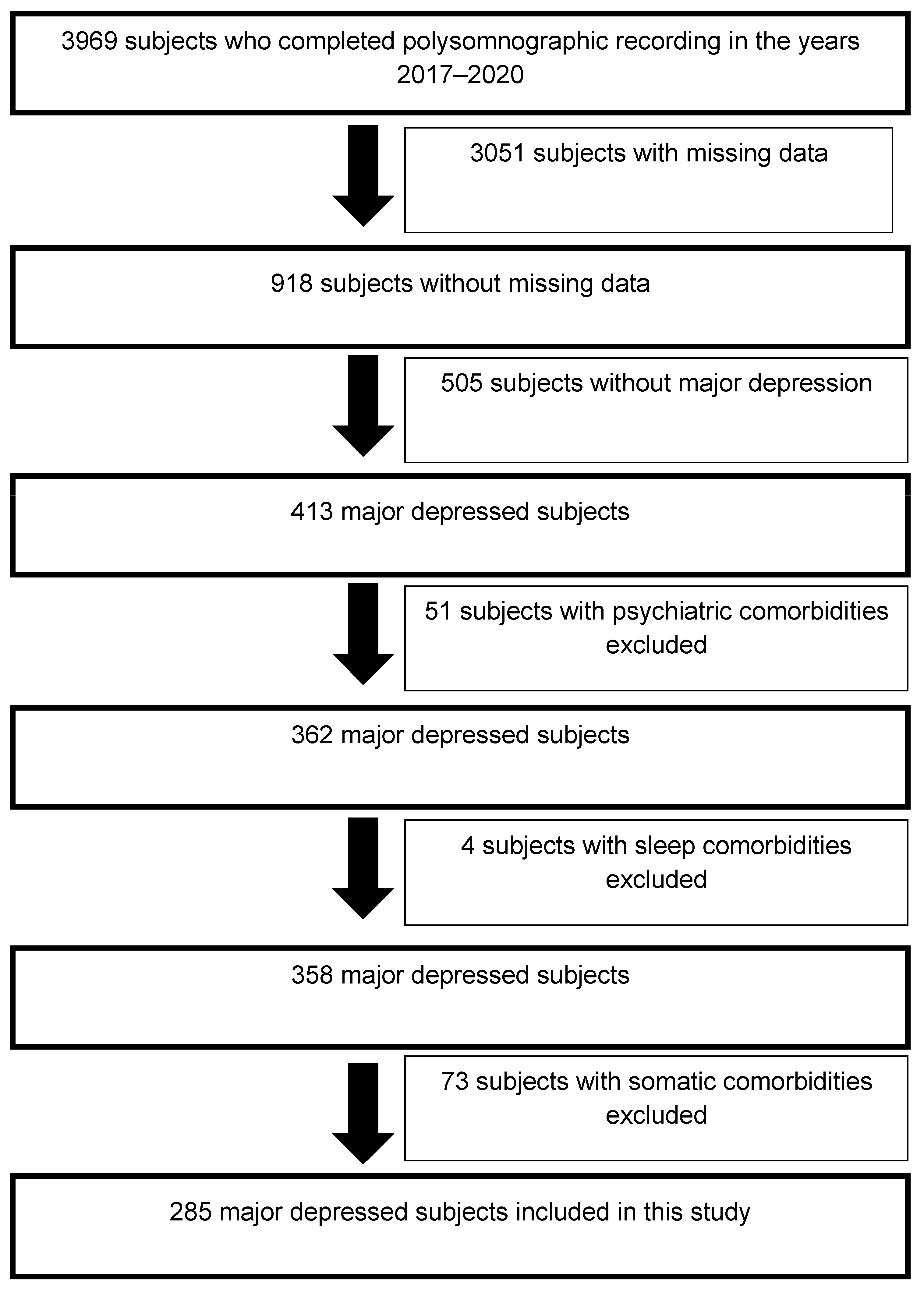
The data of 285 major depressed subjects who carried out a polysomnographic recording between 1 January 2017 and 31 December 2020 were collected from the database of the Erasme Hospital Sleep Laboratory (Figure 1). Table 1 presents the inclusion and exclusion criteria applied for the recruitment of these major depressed subjects. In addition, in this study, we only recruited major depressed subjects since the objective was to focus on this particular subpopulation where anhedonia complaints seem to play a central role in the occurrence of suicidal ideations [13,14,15,19]. Finally, Annex S1 (Supplementary Data) describes the outpatient recruitment procedure for the major depressed subjects included in this study.
2.2. Medical, Psychiatric, and Sleep Assessments of Major Depressed Subjects
The description of these different assessments and their objectives is available in Table 2. Regarding the assessment of anhedonia complaints (lifelong anhedonia and recent changes in anhedonia) and type D personality, three specific scales were used:
- -
- Recent changes in anhedonia were investigated by the Anhedonia subscale of Beck Depression Inventory (items 4, 12, and 21 of the Beck Depression Inventory [BDI-II]) [20]. However, given the absence of validated cut-offs for this Anhedonia subscale of Beck Depression Inventory, recent changes in anhedonia were considered present when the score of this subscale was >3, which seemed to be most consistent with the psychometric properties of this subscale demonstrated in the article by Joiner et al. (2003) [20].
- -
- Lifelong anhedonia was investigated by the Temporal Pleasure Experience Scale (TEPS) (Annex S2—Supplementary Data) [21]. However, given the absence of validated cut-offs for TEPS, lifelong anhedonia was considered present when the score on this scale was <76, which corresponded to the median of the TEPS distribution in our study.
- -
- The presence of type D personality (stable personality structure characterized by negative affectivity and social inhibition) was assessed with the Type-D Personality Scale (DS14). This scale consists of 14 items that may be scored from 0 to 4. It is subdivided into 2 subscales of 7 items: a negative affectivity scale and a social inhibition scale. A score ≥10 on each subscale indicates the presence of type D personality [22].
Based on the psychiatric assessment and the self-questionnaires, the potential presence of suicidal ideations was determined in all major depressed subjects. Indeed, suicidal ideations were considered present if the score on item 9 of the Beck Depression Inventory (BDI-II) was ≥1 and/or if they were highlighted during the systematic psychiatric assessment [16,23,24].

{kind=link}
Table 2.
Description of medical, psychiatric, and sleep assessments.
| Different Assessments | Objectives | |
|---|---|---|
| Medical assessment | Review of the medical record Complete somatic check-up (including blood test, electrocardiogram, and daytime electroencephalogram) | Systematic diagnosis of potential somatic comorbidities |
| Psychiatric assessment | Standardized semi-structured psychiatric interview based on DSM 5 diagnostic criteria [9] specific to Erasme Hospital Sleep Laboratory conducted by a junior psychiatrist and supervised by a senior psychiatrist to guarantee the best possible reliability of psychiatric diagnoses | Systematic diagnosis of potential psychiatric comorbidities |
| Self-questionnaires | Beck Depression Inventory (BDI-II) Spielberger Anxiety Inventory (state–trait) Insomnia Severity Index Epworth Sleepiness Scale | Assessment of subjective complaints of depression, anxiety, insomnia, and daytime sleepiness (Annex S2—Supplementary Data) |
| Sleep assessment | Semi-structured sleep interview Polysomnographic recording | Systematic diagnosis of potential comorbid sleep disorders according to the diagnostic criteria of the American Academy of Sleep Medicine [25] (Annex S3—Supplementary Data) |
2.3. Statistical Analyzes
Stata software (version 14) was used to perform the statistical analyzes. Histograms, boxplots, and quantile-quantile plots were performed to control for the distribution of the data, whereas Levene’s tests were performed to control for the equality of variances.
Based on the criteria used in this study to identify the presence of suicidal ideations in major depressed subjects, a control group without suicidal ideations and a patient group with suicidal ideations were defined to allow for the different analyzes.
Given the asymmetrical distribution of most continuous data, their medians (P25–P75) were used for descriptive analyzes, and non-parametric tests (Wilcoxon test) were used for comparative analyzes. Concerning categorical data, percentages were used for descriptive analyzes and Chi² tests were used for comparative analyzes.
Univariate logistic regression models were used to study the risk of suicidal ideations associated with anhedonia complaints and potential confounding factors (Annex S4—Supplementary Data). Methodologically, even in the case of pre-existing lifelong anhedonia, all major depressed subjects with an Anhedonia subscale of Beck Depression Inventory score of >3 were included in the “recent change of anhedonia” group, given the occurrence of a recent change in their anhedonia complaints compared to their pre-morbid state [16]. In multivariate logistic regression models, the risk of suicidal ideations associated with anhedonia complaints was only adjusted for significant confounders in univariate analyzes. These different confounding factors were introduced hierarchically into the different multivariate models.
The Hosmer and Lemeshow test was performed to control for the adequacy of the final model, whereas the Link test was performed to control for the specificity of the final model.
A p-value of < 0.05 was used to identify significant results.
3. Results
3.1. Univariate Analyzes
The prevalence of suicidal ideations was 39.3% (n = 112) in our sample of major depressed subjects. Age, use of benzodiazepine receptor agonists, use of antidepressant therapy, presence of anxiety symptoms, depression severity, presence of type D personality, and anhedonia complaints were significantly associated with a higher risk of suicidal ideations in major depressed subjects. Additionally, compared to those without suicidal ideation, major depressed subjects with suicidal ideations had higher scores on the Beck Depression Inventory (BDI-II), the Anhedonia subscale of Beck Depression Inventory, the Beck Depression Inventory (BDI-II) reduced to 17 items (without items 4, 9, 12, and 21), the Spielberger Anxiety Inventory–Trait, the Spielberger Anxiety Inventory–State, the Type-D Personality Scale (DS-14), the Type-D Personality Subscale–Negative Affectivity, and Type-D Personality Subscale–Social Inhibition. The two groups of major depressed subjects did not differ significantly for the other demographic parameters (Table 3).
3.2. Multivariate Regression Analysis
After adjusting for the main significant confounding factors during the univariate analysis, multivariate logistic regression analyzes demonstrate that unlike lifelong anhedonia, only recent changes in anhedonia were significantly associated with a higher risk of suicidal ideations in major depressed subjects (Table 4).
3.3. Polysomnographic Data
Compared to those without suicidal ideations, major depressed subjects with suicidal ideations had prolonged REM latency. The two groups of major depressed subjects did not differ significantly for the other polysomnographic parameters (Table 5).
4. Discussion
In this study, we have shown that suicidal ideations were present in 39.3% of the major depressed subjects in our sample. However, this prevalence seems to be lower than that of some studies investigating the specific relationship between anhedonia and suicidal ideations in major depressed subjects. Indeed, in the study by Xie et al. (2014) [14], 67.5% of major depressed subjects had suicidal ideations, which could be explained by the fact that unlike our study, where major depressed subjects were recruited from an outpatient consultation, all major depressed subjects included in the study by Xie et al. (2014) were recruited from psychiatric units [14]. However, in the literature, it has been shown that hospitalized major depressed subjects have a higher prevalence of suicidal ideations than ambulatory major depressed subjects [6,26,27]. On the other hand, the prevalence of suicidal ideation highlighted in our sample of major depressed subjects seems to be consistent with that of other studies investigating the association between anhedonia complaints and the occurrence of suicidal ideations in major depressed subjects. Indeed, in the study by Ducasse et al. (2020), the prevalence of suicidal ideations was 40.6% in subjects with mood disorders [15]. However, similar to our study, all subjects with mood disorders included in the study by Ducasse et al. (2020) were recruited from an outpatient consultation [15], which could explain this concordance in the prevalence of suicidal ideations in our respective samples of patients. Thus, similar to the available literature [28], we have demonstrated that suicidal ideations are a significant problem in major depressed subjects recruited from an outpatient consultation, which seems to justify a better identification of their specific risk factors in this particular subpopulation.
Consistent with the literature [29,30], we demonstrated that anhedonia complaints were frequent (67.7%) in major depressed subjects. Indeed, lifelong anhedonia and recent changes in anhedonia were present in 26.0% and 41.7% of the major depressed subjects in our sample, respectively. Additionally, similar to other specific subpopulations [16,17,31,32], we demonstrated that unlike lifelong anhedonia, only recent changes in anhedonia were associated with a higher risk of suicidal ideations in major depressed subjects. Pathophysiologically, several elements could help to better understand this high prevalence of recent changes in anhedonia and their implication in the development of suicidal ideations in major depressed subjects. First, in major depressed subjects, there is evidence for reduced activity of the nucleus accumbens and the anterior cingulate cortex, which plays a central role in the normal functioning of the reward circuit [33,34]. However, these alterations in the normal functioning of the reward circuit induced by major depression may be associated with an aberrant treatment of the reward phenomenon favoring the occurrence of a reduced reactivity to experiences generating pleasure [33,34], which could explain the high prevalence of recent changes in anhedonia demonstrated in our sample of major depressed subjects. Second, the inability to respond to positive internal and external stimuli associated with recent changes in anhedonia may promote the emergence of major psychological pain [14,35]. However, in order to escape this major psychological pain, subjects with recent changes in anhedonia seem to tend to develop avoidance strategies characterized by the occurrence of suicidal ideations [14,35], which could explain the increased risk of suicidal ideations associated with recent changes in anhedonia highlighted in our sample of major depressed subjects. Third, there are differences in the temporal dynamics of lifelong anhedonia and recent changes in anhedonia. Indeed, the chronic inability to respond to positive internal and external stimuli associated with lifelong anhedonia is relatively stable over time, whereas the diminished responsiveness to pleasure-generating experiences associated with recent changes in anhedonia corresponds to a transient disruption of normal pre-morbid functioning by somatic and/or psychiatric pathologies [36]. However, these distinct temporal dynamics, according to the type of anhedonia complaints, seem to be associated with a more frequent development of psychological pain avoidance strategies characterized by the occurrence of suicidal ideations in subjects with recent changes in anhedonia than in those with lifelong anhedonia [37], which could help to better understand the lack of association between lifelong anhedonia and suicidal ideations in our study. Thus, based on these different elements, a better identification of the recent changes in anhedonia seems to be necessary in major depressed subjects in order to allow the establishment of more targeted, preventive, and therapeutic strategies in this subpopulation at high risk of suicide.
Although conventional treatments for major depression may improve complaints of suicidal ideations [38], highlighting this higher risk of suicidal ideations associated with recent changes in anhedonia in our sample of major depressed subjects could open new therapeutic perspectives for better management of suicidal ideations in this particular subpopulation. Indeed, given the potential central role played by this specific form of anhedonia in the occurrence of suicidal ideations in major depressed subjects, the establishment of therapeutic strategies targeting anhedonia that are complementary to conventional treatments for major depression could be an interesting option to reduce complaints of suicidal ideations in this particular subpopulation [39]. However, among the therapeutic strategies targeting anhedonia currently available, some pharmacological treatments (intravenous ketamine and intranasal esketamine) and some specific psychotherapeutic interventions (Positive affect treatment) seem to show promising results for both the improvement of depressive symptoms and suicidal ideations in anhedonic major depressed subjects [40,41,42]. Finally, independently of this potential positive impact of therapeutic strategies targeting anhedonia on suicidal ideations in major depressed subjects, it remains essential to respect the treatment recommendations for major depression in order to avoid the maintenance of residual depressive symptoms that may promote the persistence of suicidal ideations in this particular subpopulation [43,44,45].
Limitations
Since the data used were extracted retrospectively without direct verification with the recruited subjects, additional prospective studies are needed to confirm the results obtained in this study. Furthermore, we only focused on anhedonia, which means that our results cannot be generalized to other affective symptoms. Moreover, since we only included major depressed subjects, our results are not generalizable to subjects with other psychiatric disorders, which may potentially limit their interpretation. On the other hand, given the inability to ensure sufficient surveillance and the presence of multiple cables in the rooms of the Erasme Hospital Sleep Laboratory, subjects with active suicidal ideations at high risk of suicidal behaviors are not admitted to this unit to avoid any risk of suicidal act but are referred to the Psychiatry Department to benefit from adequate management. However, this exclusion of subjects with active suicidal ideations at high risk of suicidal behaviors could limit the generalization of our findings to all major depressed subjects with suicidal ideations. Finally, our database only contains major depressed subjects who agreed to perform a polysomnographic recording, which may limit the generalizability of our results.
5. Conclusions
In this study, we confirmed that the prevalence of suicidal ideations is high (39.3%) in major depressed subjects. Furthermore, we demonstrated that unlike lifelong anhedonia, only recent changes in anhedonia were associated with a higher risk of suicidal ideations in major depressed subjects, which seems to justify better identification and adequate management of this specific form of anhedonia in order to open new perspectives for the prevention of suicide in this particular subpopulation.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/brainsci13071065/s1, Annex S1: Procedure used for outpatient recruitment of major depressed subjects; Annex S2: Description of self-questionnaires used; Annex S3: Description of sleep assessment; Annex S4: Description of the confounding factors included in the univariate analyzes. References [46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61] are cited in the supplementary materials.
Author Contributions
Conceptualization: G.D., G.L. and M.H.; Methodology: G.D., B.W. and M.H.; Formal Analysis: G.D. and M.H.; Investigation: G.D. and M.H.; Software: B.W.; Data Curation: G.D., B.W. and M.H.; Writing—Original Draft Preparation: G.D., B.W., G.L. and M.H.; Supervision: G.L. and M.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. In addition, the protocol for this study was carried out according to the recommendations of the Biomedical Research Department of Erasme Hospital (SRB2023002TFE) and was approved by the Ethics Committee of Erasme Hospital (P2023/032).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on reasonable request from the corresponding author.
Acknowledgments
This study would not have been possible without the support of the technical staff from the Erasme Hospital Sleep Laboratory.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Suicide Worldline in 2019: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Favril, L.; Yu, R.; Uyar, A.; Sharpe, M.; Fazel, S. Risk factors for suicide in adults: Systematic review and meta-analysis of psychological autopsy studies. Evid. Based Ment. Health 2022, 25, 148–155. [Google Scholar] [CrossRef] [PubMed]
- McMahon, E.M.; Greiner, B.A.; Corcoran, P.; Larkin, C.; Leitao, S.; McCarthy, J.; Cassidy, E.; Bradley, C.; McAuliffe, C.; Griffin, E.; et al. Psychosocial and psychiatric factors preceding death by suicide: A case-control psychological autopsy study involving multiple data sources. Suicide Life Threat. Behav. 2022, 52, 1037–1047. [Google Scholar] [CrossRef]
- Wiebenga, J.X.M.; Dickhoff, J.; Mérelle, S.Y.M.; Eikelenboom, M.; Heering, H.D.; Gilissen, R.; van Oppen, P.; Penninx, B.W.J.H. Prevalence, course, and determinants of suicide ideation and attempts in patients with a depressive and/or anxiety disorder: A review of NESDA findings. J. Affect. Disord. 2021, 283, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.J.; Simeonova, D.I.; Koleva, H.; Muzik, M.; Clark, K.D.; Ozerdem, A.; Cooper, B.; Ammerman, R.T. Potential paths to suicidal ideation and suicide attempts among high-risk women. J. Psychiatr. Res. 2022, 155, 493–500. [Google Scholar] [CrossRef]
- Cai, H.; Jin, Y.; Liu, S.; Zhang, Q.; Zhang, L.; Cheung, T.; Balbuena, L.; Xiang, Y.T. Prevalence of suicidal ideation and planning in patients with major depressive disorder: A meta-analysis of observation studies. J. Affect. Disord. 2021, 293, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Vuorilehto, M.; Valtonen, H.M.; Melartin, T.; Sokero, P.; Suominen, K.; Isometsä, E.T. Method of assessment determines prevalence of suicidal ideation among patients with depression. Eur. Psychiatry 2014, 29, 338–344. [Google Scholar] [CrossRef]
- Choi, Y.J.; Lee, W.Y. The prevalence of suicidal ideation and depression among primary care patients and current management in South Korea. Int. J. Ment. Health Syst. 2017, 11, 18. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Cai, H.; Li, Z.L.; He, F.; Li, S.Y.; Zhao, Y.J.; Zhang, W.Y.; Zhang, Y.; Su, Z.; Jackson, T.; Xiang, Y.T. Suicide ideation and anhedonia among clinically stable adolescents with the recurrent depressive disorder during the COVID-19 pandemic: A network perspective. J. Affect. Disord. 2023, 324, 317–324. [Google Scholar] [CrossRef]
- Loas, G.; Solibieda, A.; Rotsaert, M.; Englert, Y. Suicidal ideations among medical students: The role of anhedonia and type D personality. PLoS ONE 2019, 14, e0217841. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Leri, F.; Rizvi, S.J. Anhedonia as a central factor in depression: Neural mechanisms revealed from preclinical to clinical evidence. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 110, 110289. [Google Scholar] [CrossRef] [PubMed]
- Sagud, M.; Tudor, L.; Šimunić, L.; Jezernik, D.; Madžarac, Z.; Jakšić, N.; Mihaljević Peleš, A.; Vuksan-Ćusa, B.; Šimunović Filipčić, I.; Stefanović, I.; et al. Physical and social anhedonia are associated with suicidality in major depression, but not in schizophrenia. Suicide Life Threat. Behav. 2021, 51, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Li, H.; Luo, X.; Fu, R.; Ying, X.; Wang, N.; Yin, Q.; Zou, Y.; Cui, Y.; Wang, X.; et al. Anhedonia and pain avoidance in the suicidal mind: Behavioral evidence for motivational manifestations of suicidal ideation in patients with major depressive disorder. J. Clin. Psychol. 2014, 70, 681–692. [Google Scholar] [CrossRef]
- Ducasse, D.; Dubois, J.; Jaussent, I.; Azorin, J.M.; Etain, B.; Gard, S.; Henry, C.; Bougerol, T.; Kahn, J.P.; Aubin, V.; et al. Association between anhedonia and suicidal events in patients with mood disorders: A 3-year prospective study. Depress. Anxiety 2021, 38, 17–27. [Google Scholar] [CrossRef]
- Dosogne, M.; Wacquier, B.; Al Faker, M.; Willame, H.; Point, C.; Loas, G.; Hein, M. Risk of current suicidal ideations associated with lifelong anhedonia and recent change of anhedonia in individuals with insomnia: A cross-sectional study. J. Psychiatr. Res. 2022, 150, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Hawes, M.; Galynker, I.; Barzilay, S.; Yaseen, Z.S. Anhedonia and suicidal thoughts and behaviors in psychiatric outpatients: The role of acuity. Depress. Anxiety 2018, 35, 1218–1227. [Google Scholar] [CrossRef] [PubMed]
- Winer, E.S.; Nadorff, M.R.; Ellis, T.E.; Allen, J.G.; Herrera, S.; Salem, T. Anhedonia predicts suicidal ideation in a large psychiatric inpatient sample. Psychiatry Res. 2014, 218, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Dekeuleneer, F.X.; Hennebert, O.; Skrjanc, D.; Oudart, E.; Mungo, A.; Rotsaert, M.; Loas, G. Relationships between Recent Suicidal Ideation and Recent, State, Trait and Musical Anhedonias in Depression. Int. J. Environ. Res. Public Health 2022, 19, 16147. [Google Scholar] [CrossRef] [PubMed]
- Joiner, T.E.; Brown, J.S.; Metalsky, G.I. A test of the tripartite model’s prediction of anhedonia’s specificity to depression: Patients with major depression versus patients with schizophrenia. Psychiatry Res. 2003, 119, 243–250. [Google Scholar] [CrossRef]
- Loas, G.; Monestes, J.-L.; Ameller, A.; Bubrovszky, M.; Yon, V.; Wallier, J.; Berthoz, S.; Corcos, M.; Thomas, P.; Gard, D.E. Traduction et étude de validation de la version française de l’échelle d’expérience temporelle du plaisir (EETP, Temporal Experience of Pleasure Scale [TEPS], Gard et al., 2006): Étude chez 125 étudiants et chez 162 sujets présentant un trouble psychiatrique. Ann. Méd. Psychol. 2009, 167, 641–648. [Google Scholar]
- Batselé, E.; Denollet, J.; Lussier, A.; Loas, G.; Vanden Eynde, S.; Van de Borne, P.; Fantini-Hauwel, C. Type D personality: Application of DS14 French version in general and clinical populations. J. Health Psychol. 2017, 22, 1075–1083. [Google Scholar] [CrossRef]
- Zeoli, I.; Lanquart, J.P.; Wacquier, B.; Mungo, A.; Loas, G.; Hein, M. Polysomnographic markers of suicidal ideation in untreated unipolar major depressed individuals. Int. J. Psychophysiol. 2021, 166, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Laoufi, M.A.; Wacquier, B.; Lartigolle, T.; Loas, G.; Hein, M. Suicidal Ideation in Major Depressed Individuals: Role of Type D Personality. J. Clin. Med. 2022, 11, 6611. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Høyen, K.S.; Solem, S.; Cohen, L.J.; Prestmo, A.; Hjemdal, O.; Vaaler, A.E.; Galynker, I.; Torgersen, T. Non-disclosure of suicidal ideation in psychiatric inpatients: Rates and correlates. Death Stud. 2022, 46, 1823–1831. [Google Scholar] [CrossRef] [PubMed]
- Lan, X.; Zhou, Y.; Zheng, W.; Zhan, Y.; Liu, W.; Wang, C.; Jiang, M.; Yu, M.; Zhang, B.; Ning, Y. Association between cognition and suicidal ideation in patients with major depressive disorder: A longitudinal study. J. Affect. Disord. 2020, 272, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Wang, S.B.; Li, Y.; Xu, D.D.; Ungvari, G.S.; Ng, C.H.; Chow, I.H.I.; Xiang, Y.T. Prevalence of suicidal behaviors in patients with major depressive disorder in China: A comprehensive meta-analysis. J. Affect. Disord. 2018, 225, 32–39. [Google Scholar] [CrossRef]
- Cao, B.; Park, C.; Subramaniapillai, M.; Lee, Y.; Iacobucci, M.; Mansur, R.B.; Zuckerman, H.; Phan, L.; McIntyre, R.S. The Efficacy of Vortioxetine on Anhedonia in Patients With Major Depressive Disorder. Front. Psychiatry 2019, 10, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willame, H.; Wacquier, B.; Point, C.; Dosogne, M.; Al Faker, M.; Loas, G.; Hein, M. The association between type 2 diabetes and anhedonic subtype of major depression in hypertensive individuals. J. Clin. Hypertens. 2022, 24, 156–166. [Google Scholar] [CrossRef]
- Yang, X.; Tian, K.; Wang, D.; Liu, G.; Liu, X.; Harrison, P. State Anhedonia and Suicidal Ideation in Adolescents. Crisis 2021, 42, 247–254. [Google Scholar] [CrossRef]
- Yang, X.; Liu, S.; Wang, D.; Liu, G.; Harrison, P. Differential effects of state and trait social anhedonia on suicidal ideation at 3-months follow up. J. Affect. Disord. 2020, 262, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Heshmati, M.; Russo, S.J. Anhedonia and the brain reward circuitry in depression. Curr. Behav. Neurosci. Rep. 2015, 2, 146–153. [Google Scholar] [CrossRef]
- Höflich, A.; Michenthaler, P.; Kasper, S.; Lanzenberger, R. Circuit Mechanisms of Reward, Anhedonia, and Depression. Int. J. Neuropsychopharmacol. 2019, 22, 105–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonanni, L.; Gualtieri, F.; Lester, D.; Falcone, G.; Nardella, A.; Fiorillo, A.; Pompili, M. Can Anhedonia Be Considered a Suicide Risk Factor? A Review of the Literature. Medicina 2019, 55, 458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Wang, D.; Liu, S.; Liu, G.; Harrison, P. Trajectories of state anhedonia and recent changes in anhedonia in college students: Associations with other psychiatric syndromes. J. Affect. Disord. 2020, 262, 337–343. [Google Scholar] [CrossRef]
- Yang, X.; Wang, D.; Liu, S.; Liu, G.; Harrison, P. Stress and Suicidal Ideation: The Role of State or Trait Anhedonia in a Moderated Mediation Model. Suicide Life Threat. Behav. 2020, 50, 502–514. [Google Scholar] [CrossRef]
- Weissman, C.R.; Hadas, I.; Yu, D.; Jones, B.; Kong, D.; Mulsant, B.H.; Blumberger, D.M.; Daskalakis, Z.J. Predictors of change in suicidal ideation across treatment phases of major depressive disorder: Analysis of the STAR*D data. Neuropsychopharmacology 2021, 46, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- Winer, E.S.; Jordan, D.G.; Collins, A.C. Conceptualizing anhedonias and implications for depression treatments. Psychol. Res. Behav. Manag. 2019, 12, 325–335. [Google Scholar] [CrossRef] [Green Version]
- Borentain, S.; Gogate, J.; Williamson, D.; Carmody, T.; Trivedi, M.; Jamieson, C.; Cabrera, P.; Popova, V.; Wajs, E.; DiBernardo, A.; et al. Montgomery-Åsberg Depression Rating Scale factors in treatment-resistant depression at onset of treatment: Derivation, replication, and change over time during treatment with esketamine. Int. J. Methods Psychiatr. Res. 2022, 31, e1927. [Google Scholar] [CrossRef]
- Bartoli, F.; Riboldi, I.; Crocamo, C.; Di Brita, C.; Clerici, M.; Carrà, G. Ketamine as a rapid-acting agent for suicidal ideation: A meta-analysis. Neurosci. Biobehav. Rev. 2017, 77, 232–236. [Google Scholar] [CrossRef]
- Craske, M.G.; Meuret, A.E.; Ritz, T.; Treanor, M.; Dour, H.; Rosenfield, D. Positive affect treatment for depression and anxiety: A randomized clinical trial for a core feature of anhedonia. J. Consult. Clin. Psychol. 2019, 87, 457–471. [Google Scholar] [CrossRef]
- Malhi, G.S.; Bell, E.; Singh, A.B.; Bassett, D.; Berk, M.; Boyce, P.; Bryant, R.; Gitlin, M.; Hamilton, A.; Hazell, P.; et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders: Major depression summary. Bipolar. Disord. 2020, 22, 788–804. [Google Scholar] [CrossRef]
- Lam, R.W.; McIntosh, D.; Wang, J.; Enns, M.W.; Kolivakis, T.; Michalak, E.E.; Sareen, J.; Song, W.Y.; Kennedy, S.H.; MacQueen, G.M.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 1. Disease Burden and Principles of Care. Can. J. Psychiatry 2016, 61, 510–523. [Google Scholar] [CrossRef]
- Heuschen, C.B.B.C.M.; Mocking, R.J.T.; Zantvoord, J.B.; Figueroa, C.A.; Schene, A.H.; Denys, D.A.J.P.; Ruhé, H.G.; Bockting, C.L.H.; Lok, A. Suicidal ideation in remitted major depressive disorder predicts recurrence. J. Psychiatr. Res. 2022, 151, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W. Comparison of Beck Depression Inventories-IA and -II in psychiatric outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Test Manual for the State Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kushida, C.A.; Littner, M.R.; Morgenthaler, T.; Alessi, C.A.; Bailey, D.; Coleman, J.; Friedman, L.; Hirshkowitz, M.; Kapen, S.; Kramer, M.; et al. Practice parameters for the indications for polysomnography and related procedures: An update for 2005. Sleep 2005, 28, 499–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iber, C.; Ancoli-Israel, S.; Chesson, A. Quan SF for the American Academy of Sleep Medicine. In The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, 1st ed.; American Academy of Sleep Medicine: Westchester, IL, USA, 2007. [Google Scholar]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleetham, J.; Ayas, N.; Bradley, D.; Ferguson, K.; Fitzpatrick, M.; George, C.; Hanly, P.; Hill, F.; Kimoff, J.; Kryger, M.; et al. Canadian Thoracic Society guidelines: Diagnosis and treatment of sleep disordered breathing in adults. Can. Respir. J. 2006, 13, 387–392. [Google Scholar] [CrossRef] [Green Version]
- Ferri, R.; Koo, B.B.; Picchietti, D.L.; Fulda, S. Periodic leg movements during sleep: Phenotype, neurophysiology, and clinical significance. Sleep Med. 2017, 31, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Haba-Rubio, J.; Marti-Soler, H.; Tobback, N.; Andries, D.; Marques-Vidal, P.; Vollenweider, P.; Preisig, M.; Heinzer, R. Clinical significance of periodic limb movements during sleep: The HypnoLaus study. Sleep Med. 2018, 41, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.P.; Picchietti, D.L.; Garcia-Borreguero, D.; Ondo, W.G.; Walters, A.S.; Winkelman, J.W.; Zucconi, M.; Ferri, R.; Trenkwalder, C.; Lee, H.B.; et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: Updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria--history, rationale, description, and significance. Sleep Med. 2014, 15, 860–873. [Google Scholar] [CrossRef]
- Edinger, J.D.; Bonnet, M.H.; Bootzin, R.R.; Doghramji, K.; Dorsey, C.M.; Espie, C.A.; Jamieson, A.O.; McCall, W.V.; Morin, C.M.; Stepanski, E.J.; et al. Derivation of research diagnostic criteria for insomnia: Report of an American Academy of Sleep Medicine Work Group. Sleep 2004, 27, 1567–1596. [Google Scholar] [CrossRef] [PubMed]
- Hein, M.; Lanquart, J.P.; Loas, G.; Hubain, P.; Linkowski, P. Insomnia with short sleep duration as risk factor for type 2 diabetes: A systematic review of the literature. Rev. Med. Brux. 2020, 41, 98–104. [Google Scholar] [CrossRef]
- Reutfors, J.; Andersson, T.M.; Tanskanen, A.; DiBernardo, A.; Li, G.; Brandt, L.; Brenner, P. Risk Factors for Suicide and Suicide Attempts Among Patients With Treatment-Resistant Depression: Nested Case-Control Study. Arch. Suicide Res. 2021, 25, 424–438. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Rodrigues, V.; Sanchez-Carro, Y.; Lagunas, L.N.; Rico-Uribe, L.A.; Pemau, A.; Diaz-Carracedo, P.; Diaz-Marsa, M.; Hervas, G.; de la Torre-Luque, A. Risk factors for suicidal behaviour in late-life depression: A systematic review. World J. Psychiatry 2022, 12, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Mu, F.; Liu, D.; Zhu, J.; Yue, S.; Liu, M.; Liu, Y.; Wang, J. Predictors of suicidal ideation, suicide attempt and suicide death among people with major depressive disorder: A systematic review and meta-analysis of cohort studies. J. Affect. Disord. 2022, 302, 332–351. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Selection diagram of major depressed subjects included in this study.

Table 1.
Inclusion and exclusion criteria.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Patients (≥18 years) with moderate to severe major depressive episodes meeting the diagnostic criteria of DSM-5 [9] | Presence of psychiatric disorders other than major depression, active suicidal ideations with a high risk of suicidal behaviors, or abuse of substances |
| Absence of current severe uncontrolled somatic pathologies affecting the cardiopulmonary, digestive, renal, neurologic, endocrine, or immune systems | Presence of structural or functional brain lesions secondary to cranial trauma or neurological pathologies |
| Absence of craniofacial anomalies or thoracic malformations | Presence of central hypersomnia, current parasomnia, or sleep apnea syndrome with a predominantly central component |
| Pregnancy |
Table 3.
Univariate analyzes (n = 285).
| Variables | Categories | % | Major Depression without Suicidal Ideation | Major Depression with Suicidal Ideation | p-Value Chi2 | OR (CI 95%) | p-Value |
|---|---|---|---|---|---|---|---|
| Gender | Female (n = 162) Male (n = 123) | 56.8% 43.2% | 56.1% 43.9% | 58.0% 42.0% | 0.743 | 1 0.92 (0.57 to 1.49) | 0.743 |
| BMI (kg/m2) | <25 (n = 84) ≥25 and <30 (n = 98) ≥30 (n = 103) | 29.5% 34.4% 36.1% | 31.2% 32.4% 36.4% | 26.8% 37.5% 35.7% | 0.612 | 1 1.35 (0.74 to 2.46) 1.14 (0.63 to 2.08) | 0.613 |
| Age (years) | 30–45 (n = 112) <30 (n = 58) >45 (n = 115) | 39.3% 20.4% 40.3% | 45.7% 19.1% 35.2% | 29.5% 22.3% 48.2% | 0.021 | 1 1.81 (0.94 to 3.51) 2.12 (1.23 to 3.66) | 0.022 |
| Benzodiazepine receptor agonists | No (n = 227) Yes (n = 58) | 79.6% 20.4% | 85.5% 15.5% | 70.5% 29.5% | 0.002 | 1 2.47 (1.37 to 4.45) | 0.003 |
| Antidepressant therapy | No (n = 196) Yes (n = 89) | 68.8% 31.2% | 76.3% 23.7% | 57.1% 42.9% | 0.001 | 1 2.41 (1.45 to 4.03) | 0.001 |
| Other psychotropic treatments | No (n = 237) Yes (n = 48) | 83.2% 16.8% | 85.5% 15.5% | 79.5% 20.5% | 0.180 | 1 1.53 (0.82 to 2.86) | 0.182 |
| Smoking | No (n = 221) Yes (n = 64) | 77.5% 22.5% | 79.2% 20.8% | 75.0% 25.0% | 0.408 | 1 1.27 (0.72 to 2.23) | 0.408 |
| Alcohol | No (n = 151) Yes (n = 134) | 53.0% 47.0% | 53.2% 46.8% | 52.7% 47.3% | 0.934 | 1 1.02 (0.63 to 1.64) | 0.934 |
| Somatic treatments | No (n = 146) Yes (n = 139) | 51.2% 48.8% | 52.0% 48.0% | 50.0% 50.0% | 0.739 | 1 1.08 (0.67 to 1.74) | 0.739 |
| OSAS | No (n = 164) Mild (n = 60) Moderate to severe (n = 61) | 57.5% 21.1% 21.4% | 57.2% 20.8% 22.0% | 58.1% 21.4% 20.5% | 0.958 | 1 1.02 (0.56 to 1.86) 0.92 (0.50 to 1.69) | 0.958 |
| Sleep duration (hours) | ≥6 (n = 187) <6 (n = 98) | 65.6% 34.4% | 63.6% 36.4% | 68.8% 31.2% | 0.370 | 1 0.79 (0.48 to 1.32) | 0.370 |
| Sleep movement disorders | No (n = 223) Yes (n = 62) | 78.2% 21.8% | 82.1% 17.9% | 72.3% 27.7% | 0.051 | 1 1.75 (0.99 to 3.09) | 0.053 |
| Excessive daytime sleepiness | No (n = 127) Yes (n = 158) | 44.6% 55.4% | 42.2% 57.8% | 48.2% 51.8% | 0.318 | 1 0.78 (0.49 to 1.26) | 0.318 |
| Insomnia Severity Index | <15 (n = 81) ≥15 (n = 204) | 28.4% 71.6% | 29.5% 70.5% | 26.8% 73.2% | 0.622 | 1 1.14 (0.67 to 1.94) | 0.622 |
| Anxiety symptoms | No (n = 108) Trait anxiety alone (n = 38) State anxiety alone (n = 45) Trait + state anxiety (n = 94) | 37.9% 13.3% 15.8% 33.0% | 46.8% 11.0% 17.9% 24.3% | 24.1% 17.0% 12.5% 46.4% | <0.001 | 1 3.00 (1.39 to 6.48) 1.35 (0.63 to 2.92) 3.71 (2.05 to 6.74) | <0.001 |
| BDI (17 items) | <15 (n = 76) ≥15 (n = 209) | 26.7% 73.3% | 31.8% 68.2% | 18.8% 81.2% | 0.015 | 1 2.02 (1.14 to 3.58) | 0.016 |
| Type D personality | No (n = 120) Yes (n = 165) | 42.1% 57.9% | 50.9% 49.1% | 28.6% 71.4% | <0.001 | 1 2.59 (1.56 to 4.30) | <0.001 |
| Anhedonia | No (n = 92) Lifelong (n = 74) Recent change (n = 119) | 32.3% 26.0% 41.7% | 40.5% 26.0% 33.5% | 19.6% 25.9% 54.5% | <0.001 | 1 2.05 (1.05 to 4.00) 3.35 (1.84 to 6.09) | <0.001 |
| Suicidal ideation | No (n = 173) Yes (n = 112) | 60.7% 39.3% | |||||
| Median (P25–P75) | Wilcoxon test | ||||||
| BMI (kg/m2 | 27.8 (24.2–32.0) | 28.1 (23.9–32.9) | 27.7 (24.7–31.2) | 0.683 | |||
| Age (years) | 42 (32–52) | 41 (33–51) | 44 (31–54) | 0.374 | |||
| ESS | 11 (7–14) | 11 (8–14) | 11 (7–14) | 0.462 | |||
| BDI | 20 (17–27) | 18 (16–22) | 26 (19–33) | <0.001 | |||
| BDI–anhedonia | 3 (2–4) | 3 (1–4) | 4 (2–5) | <0.001 | |||
| BDI (17 items) | 17 (14–23) | 16 (14–20) | 22 (15–27) | <0.001 | |||
| ISI | 17 (14–21) | 17 (13–21) | 18 (14–20) | 0.733 | |||
| Spielberger Anxiety Inventory–Trait | 52 (46–58) | 50 (45–56) | 56 (49–63) | <0.001 | |||
| Spielberger Anxiety Inventory–State | 45 (36–54) | 42 (35–49) | 51 (40–59) | <0.001 | |||
| TEPS | 76 (68–85) | 78 (68–85) | 74 (67–82) | 0.072 | |||
| TEPS–Anticipatory | 40 (34–46) | 41 (35–46) | 38 (33–44) | 0.065 | |||
| TEPS–Consummatory | 37 (30–41) | 37 (31–42) | 36 (30–40) | 0.148 | |||
| DS-14 | 28 (20–36) | 25 (18–32) | 34 (26–41) | <0.001 | |||
| DS–Negative affectivity | 16 (11–19) | 13 (9–17) | 18 (15–22) | <0.001 | |||
| DS–Social inhibition | 13 (7–19) | 12 (6–17) | 16 (10–21) | 0.001 |
BMI = body mass index, OSAS = obstructive sleep apnea syndrome, BDI = Beck depression inventory, TEPS = temporal experience of pleasure scale, ESS = Epworth sleepiness scale, ISI = insomnia severity index, DS = type-D personality scale.
Table 4.
Multivariate analysis (n = 285).
| Variables | Model 1 OR Adjusted (CI 95%) | p-Value | Model 2 OR Adjusted (CI 95%) | p-Value | Model 3 OR Adjusted (CI 95%) | p-Value | Model 4 OR Adjusted (CI 95%) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Anhedonia No lifelong Recent change | 1 1.98 (1.00 to 3.89) 3.46 (1.88 to 6.38) | <0.001 | 1 2.11 (1.05 to 4.23) 3.15 (1.68 to 5.91) | 0.002 | 1 1.75 (0.86 to 3.57) 2.58 (1.35 to 4.95) | 0.017 | 1 1.85 (0.89 to 3.84) 2.35 (1.21 to 4.57) | 0.041 |
Model 1 = model adjusted for age; Model 2 = model adjusted for age, benzodiazepine receptor agonists, and antidepressant therapy; Model 3 = model adjusted for age, benzodiazepine receptor agonists, antidepressant therapy, and type D personality; Model 4 = model adjusted for age, benzodiazepine receptor agonists, antidepressant therapy, type D personality, anxiety symptoms, and depression severity.
Table 5.
Polysomnographic data (n = 285).
| Whole Sample | Major Depression without Suicidal Ideation | Major Depression with Suicidal Ideation | p-Value | |
|---|---|---|---|---|
| Sleep latency (min) | 57.0 (30.5–102.0) | 58.0 (33.5–106.0) | 55.0 (28.0–93.5) | 0.150 |
| Sleep efficiency (%) | 75.3 (65.8–82.9) | 74.2 (65.9–83.0) | 75.9 (65.2–82.7) | 0.432 |
| Sleep period time (min) | 438.5 (401.5–473.0) | 438.5 (391.5–470.5) | 436.8 (409.3–478.3) | 0.434 |
| Total sleep time (min) | 389.0 (340.0–426.5) | 386.5 (332.5–427.0) | 389.8 (347.0–426.5) | 0.659 |
| % stage 1 | 7.2 (5.2–9.7) | 7.7 (5.2–9.7) | 7.0 (5.0–9.5) | 0.325 |
| % stage 2 | 50.1 (43.5–57.8) | 48.9 (43.1–56.9) | 51.1 (43.7–59.5) | 0.120 |
| % slow-wave sleep | 12.4 (5.4–19.1) | 12.7 (5.2–19.7) | 12.4 (6.1–17.8) | 0.757 |
| % REM sleep | 16.7 (11.7–21.0) | 16.7 (11.7–21.8) | 16.7 (11.7–20.2) | 0.230 |
| REM latency (min) | 88.8 (66.0–142.0) | 88.0 (62.5–136.0) | 93.0 (69.0–155.5) | 0.042 |
| % wake after sleep onset | 9.4 (5.4–16.1) | 9.2 (5.2–15.9) | 9.7 (6.2–17.1) | 0.557 |
| Number of awakenings | 22 (17–30) | 22 (17–29) | 23 (17–31) | 0.514 |
| Micro-arousal index | 9 (5–15) | 9 (5–16) | 9 (5–15) | 0.912 |
| Apnea–hypopnoea index | 4 (1–13) | 4 (1–13) | 4 (2–13) | 0.665 |
| Oxygen desaturation index | 3 (0–9) | 3 (0–8) | 3 (0–9) | 0.914 |
| Total time under 90% of SaO2 (min) | 0.0 (0.0–8.0) | 0.0 (0.0–11.0) | 0.0 (0.0–6.3) | 0.535 |
| PLMs index | 2 (0–9) | 3 (0–8) | 2 (0–13) | 0.848 |
| Median (P25–P75) | Median (P25–P75) | Median (P25–P75) | Wilcoxon test |
REM = rapid eye movement, PLMs = periodic limb movements during sleep.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Darquennes, G.; Wacquier, B.; Loas, G.; Hein, M. Suicidal Ideations in Major Depressed Subjects: Role of the Temporal Dynamics of Anhedonia. Brain Sci. 2023, 13, 1065. https://doi.org/10.3390/brainsci13071065
AMA Style
Darquennes G, Wacquier B, Loas G, Hein M. Suicidal Ideations in Major Depressed Subjects: Role of the Temporal Dynamics of Anhedonia. Brain Sciences. 2023; 13(7):1065. https://doi.org/10.3390/brainsci13071065
Chicago/Turabian StyleDarquennes, Gil, Benjamin Wacquier, Gwenolé Loas, and Matthieu Hein. 2023. "Suicidal Ideations in Major Depressed Subjects: Role of the Temporal Dynamics of Anhedonia" Brain Sciences 13, no. 7: 1065. https://doi.org/10.3390/brainsci13071065
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.