
Cyclin-Dependent Kinase 4/6 Inhibitors Plus Endocrine Therapy versus Endocrine Therapy Alone for HR-Positive, HER-2-Negative Early Breast Cancer: Meta-Analysis of Phase III Randomized Clinical Trials

 , , , , , ,
, , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Data Extraction
2.5. Risk-of-Bias Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
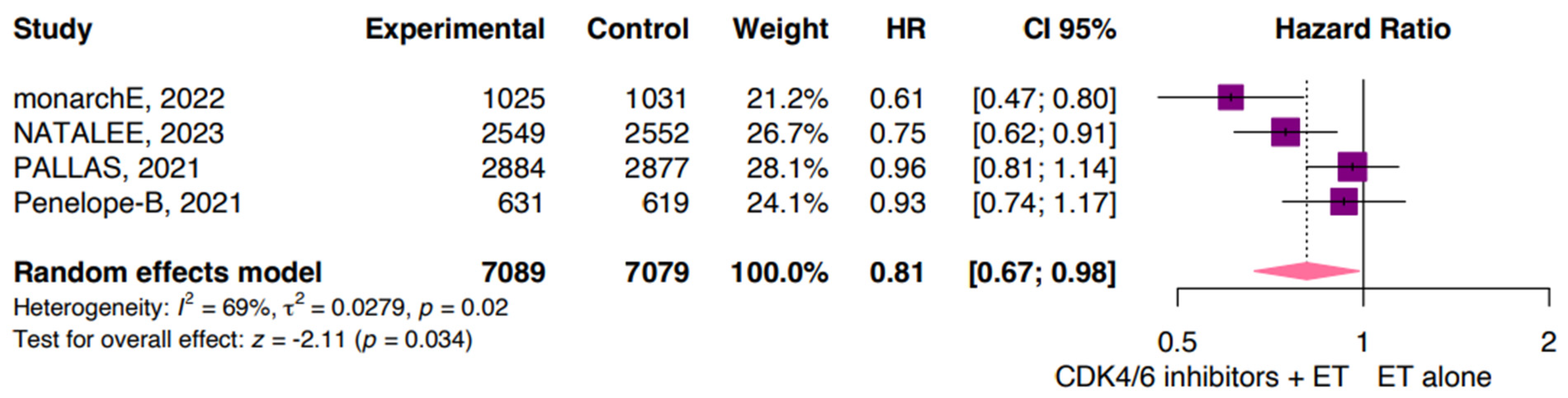
3.2. Invasive Disease-Free Survival
3.3. Distant Relapse-Free Survival
3.4. Overall Survival
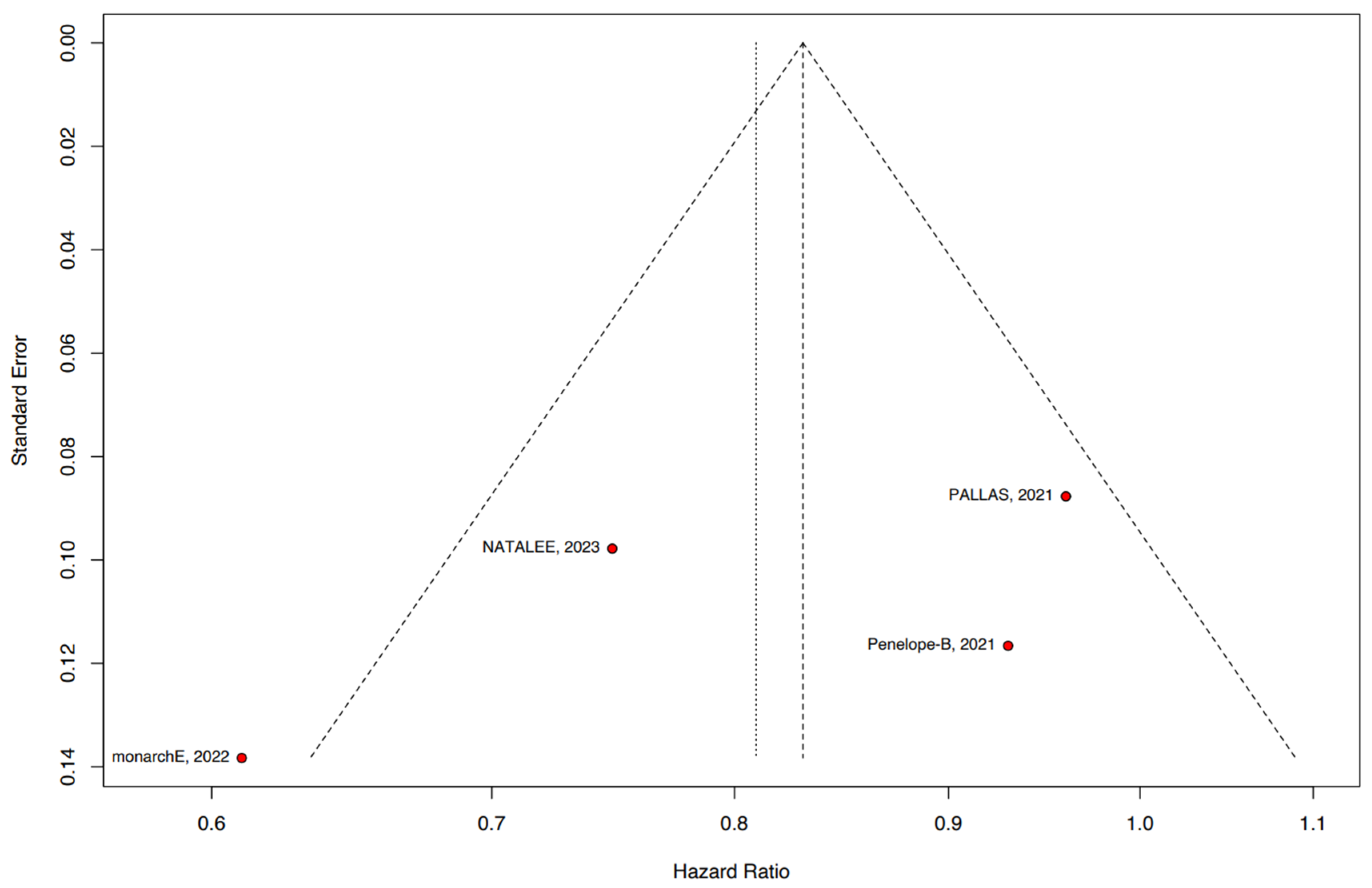
3.5. Sensitivity Analyses
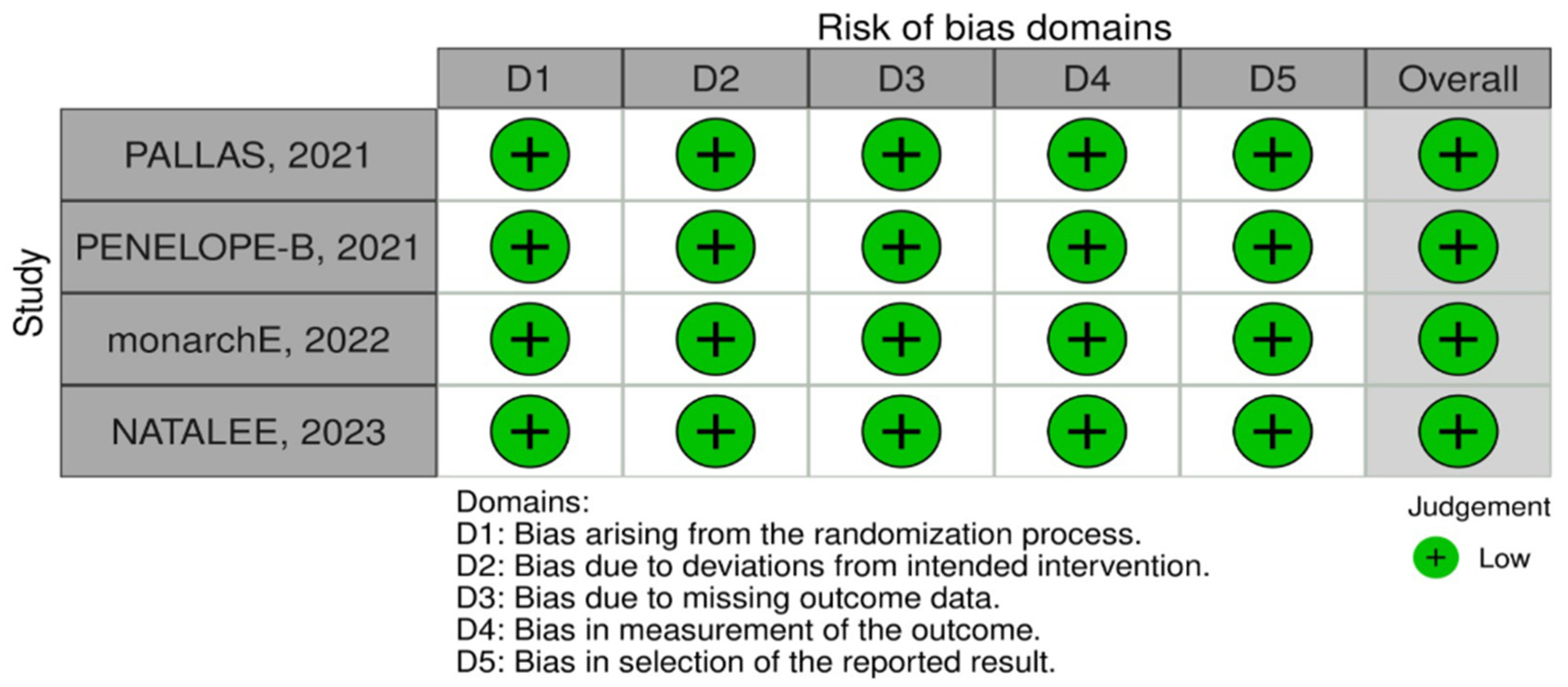
3.6. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and Future Burden of Breast Cancer: Global Statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Reeves, R.A.; Kaufman, T. Mammography. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- da Costa Nunes, G.G.; de Freitas, L.M.; Monte, N.; Gellen, L.P.A.; Santos, A.P.; de Moraes, F.C.A.; da Costa, A.C.A.; de Lima, M.C.; Fernandes, M.R.; Dos Santos, S.E.B.; et al. Genomic Variants and Worldwide Epidemiology of Breast Cancer: A Genome-Wide Association Studies Correlation Analysis. Genes 2024, 15, 145. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Li, T.; Niu, M.; Luo, S.; Chu, Q.; Wu, K. Epidemiological Trends of Women’s Cancers from 1990 to 2019 at the Global, Regional, and National Levels: A Population-Based Study. Biomark. Res. 2021, 9, 55. [Google Scholar] [CrossRef] [PubMed]
- Dafni, U.; Tsourti, Z.; Alatsathianos, I. Breast Cancer Statistics in the European Union: Incidence and Survival across European Countries. Breast Care 2019, 14, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Gnant, M. Breast Cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef] [PubMed]
- Zelnak, A.B.; O’Regan, R.M. Optimizing Endocrine Therapy for Breast Cancer. J. Natl. Compr. Cancer Netw. 2015, 13, e56–e64. [Google Scholar] [CrossRef] [PubMed]
- Arpino, G.; De Angelis, C.; Giuliano, M.; Giordano, A.; Falato, C.; De Laurentiis, M.; De Placido, S. Molecular Mechanism and Clinical Implications of Endocrine Therapy Resistance in Breast Cancer. Oncology 2009, 77 (Suppl. S1), 23–37. [Google Scholar] [CrossRef] [PubMed]
- Pandey, K.; An, H.-J.; Kim, S.K.; Lee, S.A.; Kim, S.; Lim, S.M.; Kim, G.M.; Sohn, J.; Moon, Y.W. Molecular Mechanisms of Resistance to CDK4/6 Inhibitors in Breast Cancer: A Review. Int. J. Cancer 2019, 145, 1179–1188. [Google Scholar] [CrossRef]
- Piezzo, M.; Chiodini, P.; Riemma, M.; Cocco, S.; Caputo, R.; Cianniello, D.; Di Gioia, G.; Di Lauro, V.; Rella, F.D.; Fusco, G.; et al. Progression-Free Survival and Overall Survival of CDK 4/6 Inhibitors Plus Endocrine Therapy in Metastatic Breast Cancer: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2020, 21, 6400. [Google Scholar] [CrossRef]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.-A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef]
- Tripathy, D.; Im, S.-A.; Colleoni, M.; Franke, F.; Bardia, A.; Harbeck, N.; Hurvitz, S.A.; Chow, L.; Sohn, J.; Lee, K.S.; et al. Ribociclib plus Endocrine Therapy for Premenopausal Women with Hormone-Receptor-Positive, Advanced Breast Cancer (MONALEESA-7): A Randomised Phase 3 Trial. Lancet Oncol. 2018, 19, 904–915. [Google Scholar] [CrossRef]
- Verma, S.; O’Shaughnessy, J.; Burris, H.A.; Campone, M.; Alba, E.; Chandiwana, D.; Dalal, A.A.; Sutradhar, S.; Monaco, M.; Janni, W. Health-Related Quality of Life of Postmenopausal Women with Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer Treated with Ribociclib+Letrozole: Results from MONALEESA-2. Breast Cancer Res. Treat. 2018, 170, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.-S.; Sonke, G.S.; Hart, L.; Campone, M.; Petrakova, K.; Winer, E.P.; Janni, W.; et al. Overall Survival with Ribociclib plus Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2022, 386, 942–950. [Google Scholar] [CrossRef] [PubMed]
- ESMO Congress|OncologyPRO. Available online: https://oncologypro.esmo.org/meeting-resources/esmo-congress/monarch-3-interim-overall-survival-os-results-of-abemaciclib-plus-a-nonsteroidal-aromatase-inhibitor-nsai-in-patients-pts-with-hr-her2-ad (accessed on 13 August 2023).
- Watt, A.C.; Goel, S. Cellular Mechanisms Underlying Response and Resistance to CDK4/6 Inhibitors in the Treatment of Hormone Receptor-Positive Breast Cancer. Breast Cancer Res. 2022, 24, 17. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Chapter 8: Assessing Risk of Bias in a Randomized Trial. Available online: https://training.cochrane.org/handbook/current/chapter-08 (accessed on 11 August 2023).
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE Guidelines: 3. Rating the Quality of Evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- IntHout, J.; Ioannidis, J.P.A.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman Method for Random Effects Meta-Analysis Is Straightforward and Considerably Outperforms the Standard DerSimonian-Laird Method. BMC Med. Res. Methodol. 2014, 14, 25. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Gnant, M.; Dueck, A.C.; Frantal, S.; Martin, M.; Burstein, H.J.; Greil, R.; Fox, P.; Wolff, A.C.; Chan, A.; Winer, E.P.; et al. Adjuvant Palbociclib for Early Breast Cancer: The PALLAS Trial Results (ABCSG-42/AFT-05/BIG-14-03). J. Clin. Oncol. 2022, 40, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; Marmé, F.; Martin, M.; Untch, M.; Bonnefoi, H.; Kim, S.-B.; Bear, H.; McCarthy, N.; Melé Olivé, M.; Gelmon, K.; et al. Palbociclib for Residual High-Risk Invasive HR-Positive and HER2-Negative Early Breast Cancer-The Penelope-B Trial. J. Clin. Oncol. 2021, 39, 1518–1530. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Hegg, R.; Kim, S.-B.; Schenker, M.; Grecea, D.; Garcia-Saenz, J.A.; Papazisis, K.; Ouyang, Q.; Lacko, A.; Oksuzoglu, B.; et al. Treatment with Adjuvant Abemaciclib Plus Endocrine Therapy in Patients with High-Risk Early Breast Cancer Who Received Neoadjuvant Chemotherapy: A Prespecified Analysis of the monarchE Randomized Clinical Trial. JAMA Oncol. 2022, 8, 1190–1194. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.; Lipatov, O.; Nowecki, Z.; McAndrew, N.; Kukielka-Budny, B.; Stroyakovskiy, D.; Yardley, D.A.; Huang, C.S.; Fasching, P.A.; Crown, J.; et al. Ribociclib plus Endocrine Therapy in Early Breast Cancer. N. Engl. J. Med. 2024, 390, 1080–1091. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; ESMO Guidelines Committee. Electronic address: [email protected] Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up†. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed]
- Colleoni, M.; Sun, Z.; Price, K.N.; Karlsson, P.; Forbes, J.F.; Thürlimann, B.; Gianni, L.; Castiglione, M.; Gelber, R.D.; Coates, A.S.; et al. Annual Hazard Rates of Recurrence for Breast Cancer during 24 Years of Follow-Up: Results From the International Breast Cancer Study Group Trials I to V. J. Clin. Oncol. 2016, 34, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E.; Dees, E.C.; Goetz, M.P.; Olson, J.A.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Sirico, M.; Virga, A.; Conte, B.; Urbini, M.; Ulivi, P.; Gianni, C.; Merloni, F.; Palleschi, M.; Gasperoni, M.; Curcio, A.; et al. Neoadjuvant Endocrine Therapy for Luminal Breast Tumors: State of the Art, Challenges and Future Perspectives. Crit. Rev. Oncol. Hematol. 2023, 181, 103900. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Gray, R.; Braybrooke, J.; Davies, C.; Taylor, C.; McGale, P.; Peto, R.; Pritchard, K.I.; Bergh, J.; Dowsett, M.; et al. 20-Year Risks of Breast-Cancer Recurrence after Stopping Endocrine Therapy at 5 Years. N. Engl. J. Med. 2017, 377, 1836–1846. [Google Scholar] [CrossRef]
- Pedersen, R.N.; Esen, B.Ö.; Mellemkjær, L.; Christiansen, P.; Ejlertsen, B.; Lash, T.L.; Nørgaard, M.; Cronin-Fenton, D. The Incidence of Breast Cancer Recurrence 10-32 Years After Primary Diagnosis. J. Natl. Cancer Inst. 2022, 114, 391–399. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological Complete Response and Long-Term Clinical Benefit in Breast Cancer: The CTNeoBC Pooled Analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Salvo, E.M.; Ramirez, A.O.; Cueto, J.; Law, E.H.; Situ, A.; Cameron, C.; Samjoo, I.A. Risk of Recurrence among Patients with HR-Positive, HER2-Negative, Early Breast Cancer Receiving Adjuvant Endocrine Therapy: A Systematic Review and Meta-Analysis. Breast 2021, 57, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Wander, S.A.; O’Brien, N.; Litchfield, L.M.; O’Dea, D.; Morato Guimaraes, C.; Slamon, D.J.; Goel, S. Targeting CDK4 and 6 in Cancer Therapy: Emerging Preclinical Insights Related to Abemaciclib. Oncologist 2022, 27, 811–821. [Google Scholar] [CrossRef] [PubMed]
- George, M.A.; Qureshi, S.; Omene, C.; Toppmeyer, D.L.; Ganesan, S. Clinical and Pharmacologic Differences of CDK4/6 Inhibitors in Breast Cancer. Front. Oncol. 2021, 11, 693104. [Google Scholar] [CrossRef] [PubMed]
- Hafner, M.; Mills, C.E.; Subramanian, K.; Chen, C.; Chung, M.; Boswell, S.A.; Everley, R.A.; Liu, C.; Walmsley, C.S.; Juric, D.; et al. Multiomics Profiling Establishes the Polypharmacology of FDA-Approved CDK4/6 Inhibitors and the Potential for Differential Clinical Activity. Cell Chem. Biol. 2019, 26, 1067–1080.e8. [Google Scholar] [CrossRef] [PubMed]
- Cousins, E.M.; Goldfarb, D.; Yan, F.; Roques, J.; Darr, D.; Johnson, G.L.; Major, M.B. Competitive Kinase Enrichment Proteomics Reveals That Abemaciclib Inhibits GSK3β and Activates WNT Signaling. Mol. Cancer Res. 2018, 16, 333–344. [Google Scholar] [CrossRef]
- Harbeck, N.; Rastogi, P.; Martin, M.; Tolaney, S.M.; Shao, Z.M.; Fasching, P.A.; Huang, C.S.; Jaliffe, G.G.; Tryakin, A.; Goetz, M.P.; et al. Adjuvant Abemaciclib Combined with Endocrine Therapy for High-Risk Early Breast Cancer: Updated Efficacy and Ki-67 Analysis from the monarchE Study. Ann. Oncol. 2021, 32, 1571–1581. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.R.D.; Toi, M.; O’Shaughnessy, J.; Rastogi, P.; Campone, M.; Neven, P.; Huang, C.-S.; Huober, J.; Jaliffe, G.G.; Cicin, I.; et al. Abemaciclib plus Endocrine Therapy for Hormone Receptor-Positive, HER2-Negative, Node-Positive, High-Risk Early Breast Cancer (monarchE): Results from a Preplanned Interim Analysis of a Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2023, 24, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Gnant, M.; Turner, N.C.; Hernando, C. Managing a Long and Winding Road: Estrogen Receptor-Positive Breast Cancer. Am. Soc. Clin. Oncol. Educ. Book 2023, 43, e390922. [Google Scholar] [CrossRef]
- Mayer, E.L.; Fesl, C.; Hlauschek, D.; Garcia-Estevez, L.; Burstein, H.J.; Zdenkowski, N.; Wette, V.; Miller, K.D.; Balic, M.; Mayer, I.A.; et al. Treatment Exposure and Discontinuation in the PALbociclib CoLlaborative Adjuvant Study of Palbociclib With Adjuvant Endocrine Therapy for Hormone Receptor-Positive/Human Epidermal Growth Factor Receptor 2-Negative Early Breast Cancer (PALLAS/AFT-05/ABCSG-42/BIG-14-03). J. Clin. Oncol. 2022, 40, 449–458. [Google Scholar] [CrossRef]
- Mayer, E.L.; Dueck, A.C.; Martin, M.; Rubovszky, G.; Burstein, H.J.; Bellet-Ezquerra, M.; Miller, K.D.; Zdenkowski, N.; Winer, E.P.; Pfeiler, G.; et al. Palbociclib with Adjuvant Endocrine Therapy in Early Breast Cancer (PALLAS): Interim Analysis of a Multicentre, Open-Label, Randomised, Phase 3 Study. Lancet Oncol. 2021, 22, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, P.; Jin, Q.; Mittendorf, E.A.; King, T.A.; Curigliano, G.; Tolaney, S.M. Clinical and Pathological Features of Breast Cancer Patients Eligible for Adjuvant Abemaciclib. Ann. Oncol. 2022, 33, 845–847. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study/Year | Design /NCT | No. of pts | Median * Follow-Up | Median Age ** | Pre-M Status | Post-M Status | Tx Duration *** | Pathological Grade | Lymph Node Status | Tx | Central Ki-67 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PALLAS 2021 | RCT Phase III 2513394 | I: 2884 C: 2877 | 31 mo (24.5–37.3) | I: 55 (29–84) C: 53 (30–85) | I: 1303 (45.2%) C: 1323 (46.0%) | I: 1562 (54.2%) C: 1534 (53.3%) | 12 | I: I or IIA: 513 (17.8) IIB or III: 2370 (82.2) Unk: 1 (0) C: I or IIA: 519 (18) IIB or III: 2358 (82) Unk: 0 (0) | I: N0: 365 (12.7) N1:1421(49.6) N2: 700 (24.3) N3: 386 (13.4) NX: 1 (0.0) Unk: 1(0) C: N0: 385 (13.4) N1:1411(49.0) N2: 709 (24.5) N3: 372 (12.9) NX: 1 (0.0) Unk:1(0) | I: Palbo + ET C: ET alone | N/A |
| PENELOPE-B 2021 | RCT Phase III 1864746 | I: 631 C: 619 | 42.8 mo | I: 49 (22–76) C: 48 (19–79) | I: 300 (47.5%) C: 331 (52.5%) | I: 316 (51.1%) C: 303 (48.9%) | †11.34 | N/A | I: N0: 66 (10.5) N1: 433 (68.6) N2: 80 (12.7) N3: 52 (8.2) C: N0: 71 (11.5) N1: 417 (67.4) N2: 82 (13.2) N3: 49 (7.9) | I: Palbo + ET C: PBO of Palbo + ET | I: ≤15%:470(74.5) >15%:161(25.5) C: ≤15%:461(74.5) >15%:158(25.5) |
| MonarchE 2022 | RCT Phase III 3155997 | I: 1025 C: 1031 | 19 mo (15.6–23.9) | I: 49 (25–84) C: 49 (22–78) | I: 512 (50.1%) C: 510 (49.9%) | I: 516 (50.0%) C: 515 (50.0%) | 24 | I: IA: 2 (0.1) IIA: 323 (11.5) IIB: 389 (13.9) IIIA: 1027 (36.6) IIIB: 104 (3.7) IIIC: 950 (33.8) C: IA: 1 (0.0) IIA: 353 (12.5) IIB: 387 (13.7) IIIA: 1024 (36.2) IIIB: 91 (3.2) IIIC: 962 (34.0) | I: N0: 3(0.3) N1−3:450(44) N4+:572(55.8) C: N0: 6(0.6) N1−3:463(45) N4+:562 (54.5) | I: Abema + ET C: ET alone | I: <20%:242(24) ≥20%:450(44) N/A:333 (32.5) C: <20%:248(24) ≥20%:452(44) N/A:331 (32.1) |
| NATALEE 2023 | RCT Phase III 3701334 | I: 2549 C: 2552 | 19.1 mo | I: 52 (24–90) C: 52 (24–89) | I: 1126 (44%) C: 1132 (44%) | I: 1423 (56%) C: 1420 (56%) | 36 | I: IIA: 479 (19) IIB: 532 (21) III: 1528 (60) C: IIA: 521 (20) IIB: 513 (20) III: 1512 (59) | N/A | I: Ribo + NSAIs C: NSAIs alone | I: ≤20%:76 (6.3) >20%:82 (8.9) C: ≤20%:95 (7.7) >20%:15 (11.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moraes, F.C.A.d.; de Oliveira Almeida, G.; Alves, V.F.C.; Priantti, J.N.; Gomes, G.d.C.; Carnevalli, S.V.B.; Madeira, T.; Vilbert, M.; Stecca, C.; Figueroa Magalhães, M.C.; et al. Cyclin-Dependent Kinase 4/6 Inhibitors Plus Endocrine Therapy versus Endocrine Therapy Alone for HR-Positive, HER-2-Negative Early Breast Cancer: Meta-Analysis of Phase III Randomized Clinical Trials. J. Pers. Med. 2024, 14, 464. https://doi.org/10.3390/jpm14050464
Moraes FCAd, de Oliveira Almeida G, Alves VFC, Priantti JN, Gomes GdC, Carnevalli SVB, Madeira T, Vilbert M, Stecca C, Figueroa Magalhães MC, et al. Cyclin-Dependent Kinase 4/6 Inhibitors Plus Endocrine Therapy versus Endocrine Therapy Alone for HR-Positive, HER-2-Negative Early Breast Cancer: Meta-Analysis of Phase III Randomized Clinical Trials. Journal of Personalized Medicine. 2024; 14(5):464. https://doi.org/10.3390/jpm14050464
Chicago/Turabian StyleMoraes, Francisco Cezar Aquino de, Gustavo de Oliveira Almeida, Vinícius Freire Costa Alves, Jonathan N. Priantti, Giovanna da Conceição Gomes, Sarah Vitória Bristot Carnevalli, Thiago Madeira, Maysa Vilbert, Carlos Stecca, Maria Cristina Figueroa Magalhães, and et al. 2024. "Cyclin-Dependent Kinase 4/6 Inhibitors Plus Endocrine Therapy versus Endocrine Therapy Alone for HR-Positive, HER-2-Negative Early Breast Cancer: Meta-Analysis of Phase III Randomized Clinical Trials" Journal of Personalized Medicine 14, no. 5: 464. https://doi.org/10.3390/jpm14050464