
Usefulness and Limitations of Anti-S IgG Assay in Detecting Previous SARS-CoV-2 Breakthrough Infection in Fully Vaccinated Healthcare Workers
 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting, Population, and Testing
2.2. Statistical Analysis
2.3. Ethics
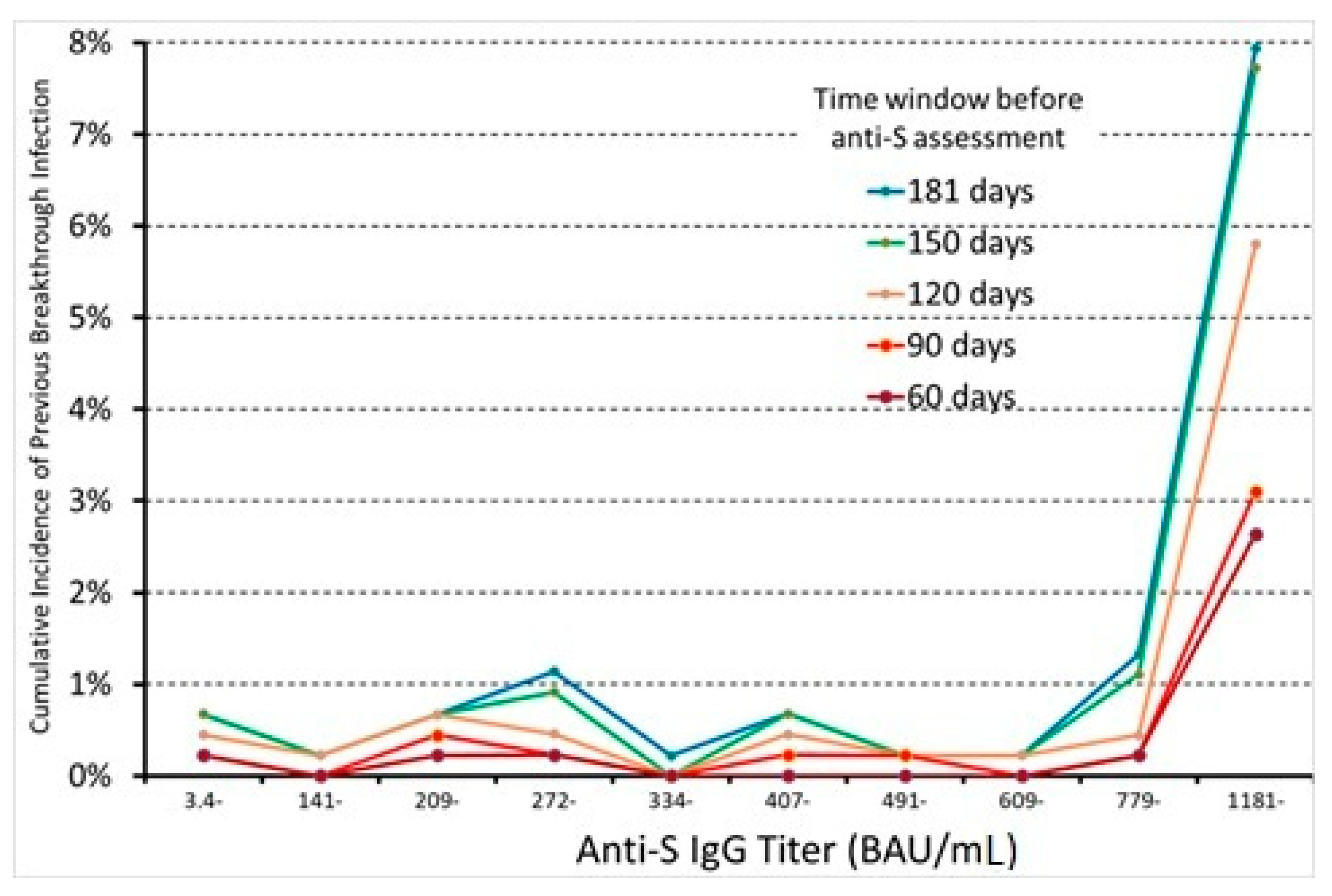
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Medicines Agency. Comirnaty. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/comirnaty (accessed on 31 July 2022).
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Presidenza del Consiglio dei Ministri. Report Vaccini Anti COVID-19. Available online: https://www.governo.it/it/cscovid19/report-vaccini/ (accessed on 31 July 2022).
- Bettini, E.; Locci, M. SARS-CoV-2 mRNA Vaccines: Immunological Mechanism and Beyond. Vaccines 2021, 9, 147. [Google Scholar] [CrossRef]
- Kontopoulou, K.; Ainatzoglou, A.; Ifantidou, A.; Nakas, C.T.; Gkounti, G.; Adamopoulos, V.; Papadopoulos, N.; Papazisis, G. Immunogenicity after the first dose of the BNT162b2 mRNA COVID-19 vaccine: Real-world evidence from Greek healthcare workers. J. Med. Microbiol. 2021, 70, 001387. [Google Scholar] [CrossRef]
- Visci, G.; Zunarelli, C.; Mansour, I.; Porru, S.; De Palma, G.; Duval, X.; Monaco, M.G.L.; Spiteri, G.; Carta, A.; Lippi, G.; et al. Serological response after SARS-CoV2 vaccination in healthcare workers: A multicenter study. Med. Lav. 2022, 113, e2022022. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Sarabia, K.; Gutiérrez-Torres, M.; Mendoza-Renteria, E.M.; Leyva-Vázquez, M.A.; Vences-Velázquez, A.; Hernández-Sotelo, D.; Beltrán-Anaya, F.O.; Del Moral-Hernández, O.; Illades-Aguiar, B. Variation in the Humoral Immune Response Induced by the Administration of the BNT162b2 Pfizer/BioNTech Vaccine: A Systematic Review. Vaccines 2022, 10, 909. [Google Scholar] [CrossRef] [PubMed]
- Carrat, F.; Villarroel, P.M.S.; Lapidus, N.; Fourié, T.; Blanché, H.; Dorival, C.; Nicol, J.; Deleuze, J.F.; Robineau, O.; SAPRIS-SERO Study Group; et al. Heterogeneous SARS-CoV-2 humoral response after COVID-19 vaccination and/or infection in the general population. Sci. Rep. 2022, 12, 8622, Erratum in Sci. Rep. 2022, 12, 9405. [Google Scholar] [CrossRef] [PubMed]
- Notarte, K.I.; Guerrero-Arguero, I.; Velasco, J.V.; Ver, A.T.; Santos de Oliveira, M.H.; Catahay, J.A.; Khan, M.S.R.; Pastrana, A.; Juszczyk, G.; Torrelles, J.B.; et al. Characterisation of the significant decline in humoral immune response six months post-SARS-CoV-2 mRNA vaccination: A systematic review. J. Med. Virol. 2022, 94, 2939–2961. [Google Scholar] [CrossRef]
- Gazit, S.; Shlezinger, R.; Perez, G.; Lotan, R.; Peretz, A.; Ben-Tov, A.; Herzel, E.; Alapi, H.; Cohen, D.; Muhsen, K.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Naturally Acquired Immunity versus Vaccine-induced Immunity, Reinfections versus Breakthrough Infections: A Retrospective Cohort Study. Clin. Infect. Dis. 2022, 75, e545–e551. [Google Scholar] [CrossRef]
- Porru, S.; Monaco, M.G.L.; Spiteri, G.; Carta, A.; Pezzani, M.D.; Lippi, G.; Gibellini, D.; Tacconelli, E.; Dalla Vecchia, I.; Sala, E.; et al. SARS-CoV-2 Breakthrough Infections: Incidence and Risk Factors in a Large European Multicentric Cohort of Health Workers. Vaccines 2022, 10, 1193. [Google Scholar] [CrossRef]
- Jiang, C.; Li, X.; Ge, C.; Ding, Y.; Zhang, T.; Cao, S.; Meng, L.; Lu, S. Molecular detection of SARS-CoV-2 being challenged by virus variation and asymptomatic infection. J. Pharm. Anal. 2021, 11, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Demmer, R.T.; Baumgartner, B.; Wiggen, T.D.; Ulrich, A.K.; Strickland, A.J.; Naumchik, B.M.; Bohn, B.; Walsh, S.; Smith, S.; Kline, S.; et al. Identification of natural SARS-CoV-2 infection in seroprevalence studies among vaccinated populations. medRxiv 2021. medRxiv:2021.04.12.21255330. [Google Scholar] [CrossRef] [PubMed]
- Dörschug, A.; Frickmann, H.; Schwanbeck, J.; Yilmaz, E.; Mese, K.; Hahn, A.; Groß, U.; Zautner, A.E. Comparative Assessment of Sera from Individuals after S-Gene RNA-Based SARS-CoV-2 Vaccination with Spike-Protein-Based and Nucleocapsid-Based Serological Assays. Diagnostics 2021, 11, 426. [Google Scholar] [CrossRef] [PubMed]
- Mizoue, T.; Yamamoto, S.; Konishi, M.; Oshiro, Y.; Inamura, N.; Nemoto, T.; Ozeki, M.; Horii, K.; Okudera, K.; Sugiyama, H.; et al. Sensitivity of anti-SARS-CoV-2 nucleocapsid protein antibody for breakthrough infections during the epidemic of the Omicron variants. J. Infect. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.; Brady, M.; Carrion Martin, A.I.; Domegan, L.; Walsh, C.; Doherty, L.; Riain, U.N.; Bergin, C.; Fleming, C.; Conlon, N. Serological markers of SARS-CoV-2 infection; anti-nucleocapsid antibody positivity may not be the ideal marker of natural infection in vaccinated individuals. J. Infect. 2021, 83, e9–e10. [Google Scholar] [CrossRef]
- Tutukina, M.; Kaznadzey, A.; Kireeva, M.; Mazo, I. IgG Antibodies Develop to Spike but Not to the Nucleocapsid Viral Protein in Many Asymptomatic and Light COVID-19 Cases. Viruses 2021, 13, 1945. [Google Scholar] [CrossRef]
- Shrotri, M.; Harris, R.J.; Rodger, A.; Planche, T.; Sanderson, F.; Mahungu, T.; McGregor, A.; Heath, P.T.; London COVID Group; Brown, C.S.; et al. Persistence of SARS-CoV-2 N-Antibody Response in Healthcare Workers, London, UK. Emerg. Infect. Dis. 2021, 27, 1155–1158. [Google Scholar] [CrossRef]
- Van Elslande, J.; Oyaert, M.; Lorent, N.; Vande Weygaerde, Y.; Van Pottelbergh, G.; Godderis, L.; Van Ranst, M.; André, E.; Padalko, E.; Lagrou, K.; et al. Lower persistence of anti-nucleocapsid compared to anti-spike antibodies up to one year after SARS-CoV-2 infection. Diagn. Microbiol. Infect. Dis. 2022, 103, 115659. [Google Scholar] [CrossRef]
- Nakagama, Y.; Komase, Y.; Kaku, N.; Nitahara, Y.; Tshibangu-Kabamba, E.; Tominaga, T.; Tanaka, H.; Yokoya, T.; Hosokawa, M.; Kido, Y. Detecting Waning Serological Response with Commercial Immunoassays: 18-Month Longitudinal Follow-up of Anti-SARS-CoV-2 Nucleocapsid Antibodies. Microbiol. Spectr. 2022, 10, e0098622. [Google Scholar] [CrossRef]
- Yang, S.L.; Mat Ripen, A.; Leong, C.T.; Lee, J.V.; Yen, C.H.; Chand, A.K.; Koh, K.; Abdul Rahim, N.A.B.; Gokilavanan, V.; Mohamed, N.N.E.B.; et al. COVID-19 breakthrough infections and humoral immune response among BNT162b2 vaccinated healthcare workers in Malaysia. Emerg. Microbes. Infect. 2022, 11, 1262–1271. [Google Scholar] [CrossRef]
- Abu Jabal, K.; Edelstein, M. Using SARS-CoV-2 anti-S IgG levels as a marker of previous infection: Example from an Israeli healthcare worker cohort. Int. J. Infect. Dis. 2022, 120, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; Gorska, A.; Carrara, E.; Davis, R.J.; Bonten, M.; Friedrich, A.W.; Glasner, C.; Goossens, H.; Hasenauer, J.; Abad, J.M.H.; et al. Challenges of data sharing in European COVID-19 projects: A learning opportunity for advancing pandemic preparedness and response. Lancet Reg Health Eur. 2022, 21, 100467. [Google Scholar] [CrossRef] [PubMed]
- Diasorin. LIAISON® SARS-CoV-2 TrimericS IgG Assay. A Quantitative Assay for Immune Status Monitoring with an Accurate Correlation of Neutralising IgG Antibodies. Available online: https://www.diasorin.com/sites/default/files/allegati_prodotti/liaisonr_sars-cov-2_trimerics_igg_assay_m0870004408_a_lr_0.pdf (accessed on 30 June 2022).
- Liu, X. Classification accuracy and cut point selection. Stat. Med. 2012, 31, 2676–2686. [Google Scholar] [CrossRef] [PubMed]
- Hachim, A.; Kavian, N.; Cohen, C.A.; Chin, A.W.H.; Chu, D.K.W.; Mok, C.K.P.; Tsang, O.T.Y.; Yeung, Y.C.; Perera, R.A.P.M.; Poon, L.L.M.; et al. ORF8 and ORF3b antibodies are accurate serological markers of early and late SARS-CoV-2 infection. Nat. Immunol. 2020, 21, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lam, J.Y.; Wong, W.M.; Yuen, C.K.; Cai, J.P.; Au, S.W.; Chan, J.F.; To, K.K.W.; Kok, K.H.; Yuen, K.Y. Accurate Diagnosis of COVID-19 by a Novel Immunogenic Secreted SARS-CoV-2 orf8 Protein. mBio 2020, 11, e02431-20. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Best Cut-Off | ||||||
|---|---|---|---|---|---|---|
| Elapsed Time (Days) | N | BI Cases | ROC (AUC) | Cut-Off Value | Se | Sp |
| All (13–181) | 4462 | 59 (1.32%) | 0.777 | 935 | 0.68 | 0.86 |
| <150 (13–148) | 4458 | 55 (1.23%) | 0.785 | 938.5 | 0.69 | 0.86 |
| 120 days | 4442 | 39 (0.88%) | 0.784 | 935 | 0.69 | 0.86 |
| 90 days | 4432 | 20 (0.45%) | 0.795 | 935 | 0.70 | 0.86 |
| 60 days | 4418 | 15 (0.34%) | 0.831 | 935 | 0.80 | 0.86 |
| Best Cut-Off | |||||
|---|---|---|---|---|---|
| Elapsed Time (Days) | N | ROC (AUC) | Cut-Off Value | Se | Sp |
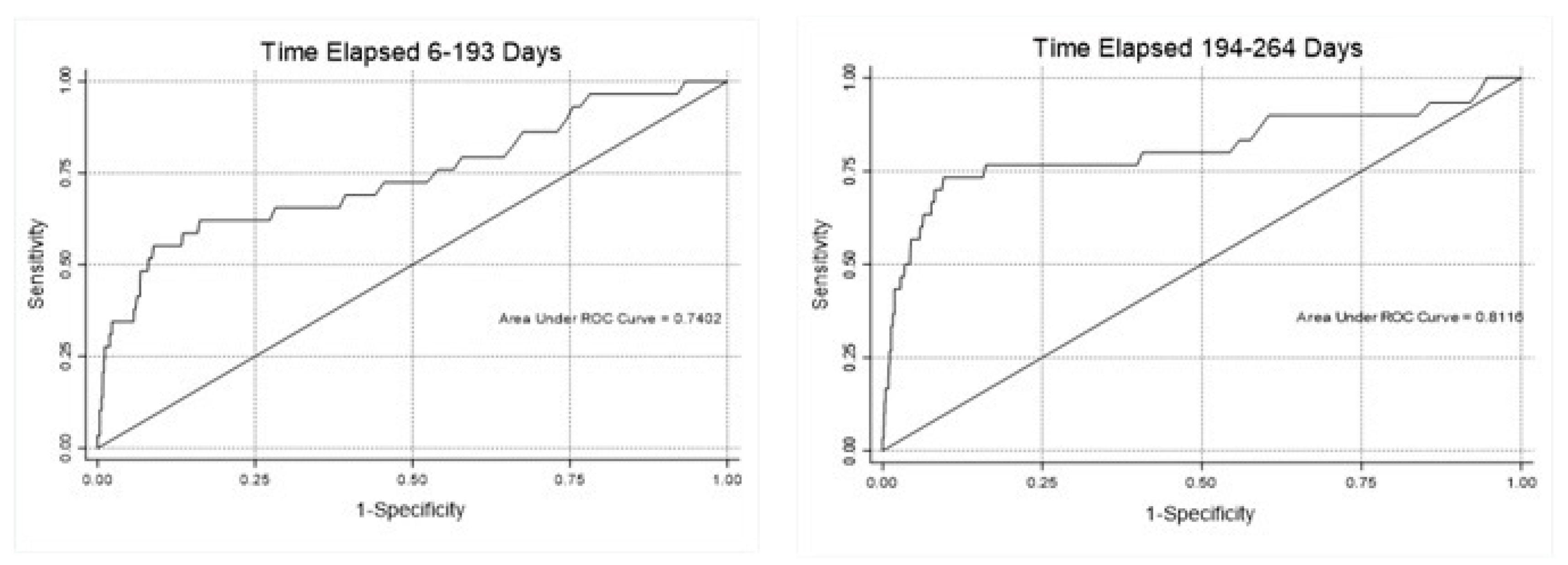
| 6–193 | 2629 | 0.7402 | 935 | 0.62 | 0.84 |
| 194–264 | 1832 | 0.8116 | 1035 | 0.73 | 0.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spiteri, G.; Monaco, M.G.L.; Caliskan, G.; Carta, A.; Pezzani, M.D.; Lippi, G.; Gibellini, D.; Verlato, G.; Porru, S. Usefulness and Limitations of Anti-S IgG Assay in Detecting Previous SARS-CoV-2 Breakthrough Infection in Fully Vaccinated Healthcare Workers. Diagnostics 2022, 12, 2152. https://doi.org/10.3390/diagnostics12092152
Spiteri G, Monaco MGL, Caliskan G, Carta A, Pezzani MD, Lippi G, Gibellini D, Verlato G, Porru S. Usefulness and Limitations of Anti-S IgG Assay in Detecting Previous SARS-CoV-2 Breakthrough Infection in Fully Vaccinated Healthcare Workers. Diagnostics. 2022; 12(9):2152. https://doi.org/10.3390/diagnostics12092152
Chicago/Turabian StyleSpiteri, Gianluca, Maria Grazia Lourdes Monaco, Gulser Caliskan, Angela Carta, Maria Diletta Pezzani, Giuseppe Lippi, Davide Gibellini, Giuseppe Verlato, and Stefano Porru. 2022. "Usefulness and Limitations of Anti-S IgG Assay in Detecting Previous SARS-CoV-2 Breakthrough Infection in Fully Vaccinated Healthcare Workers" Diagnostics 12, no. 9: 2152. https://doi.org/10.3390/diagnostics12092152