
The Risk Perception of the Chinese Diaspora during the COVID-19 Pandemic: Targeting Cognitive Dissonance through Storytelling
 , , and
, , and 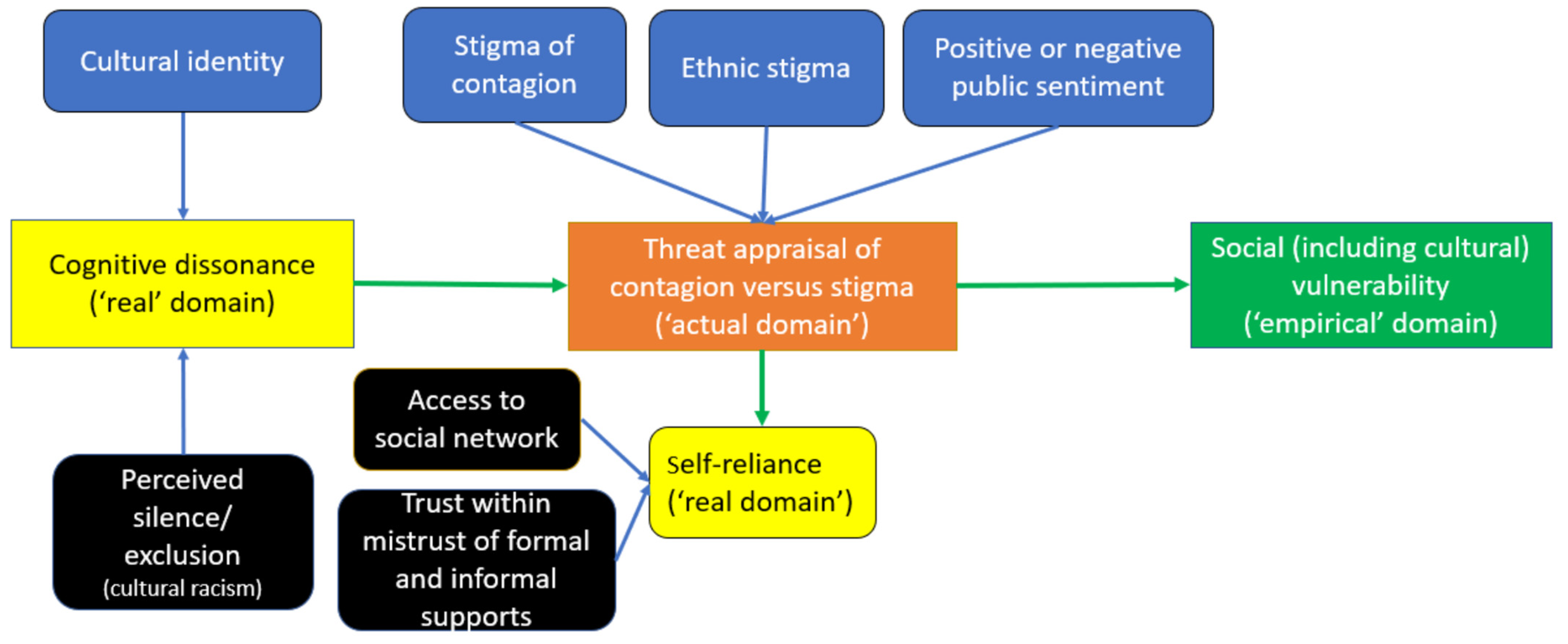{kind=link}
Abstract
:1. Introduction
1.1. Risk Perception
1.2. Cognitive Dissonance
1.3. Context of Stigma towards Chinese Diaspora in Canada
2. Material and Methods
2.1. Study Design, Location, and Research Question
2.2. Theoretical–Conceptual Framework
2.3. Researcher Characteristics and Reflexivity
2.4. Recruitment of Participants
2.5. Data Collection
2.6. Data Analysis
2.7. Trustworthiness
2.8. Ethical Aspects
3. Results
3.1. Participants’ Socio–Demographic Characteristics
3.2. Cultural Identity Recognition
‘I believe I heard a news report [CNN World News] that somebody from London [UK] got attacked, punched by a crazy person… Just because he was Asian and wearing a mask… By that time, the outbreak wasn’t in Canada or wasn’t in Toronto yet so I was thinking, well, maybe it’s not that mandatory [that] I’ll have to wear the mask. Maybe for self-protection, I put a mask in my pocket just in case… if somebody’s coughing or looks sick, and yeah, but I can’t. I was too scared to put on my mask. Too scared.’(#39, female student, resident of GTA for 5 years)
‘I’m seeing it through the CBC [Canadian-born Chinese] lens…Because I’m not tight with that, you know… you go down to the market and down in Chinatown to [name of store]. And no line up to get in but people are also not regulating the same kind of awareness of physical distancing, they were wearing gloves, they were doing things, but the aisles are so narrow they don’t have that sort of Western medical sensibility. And so, we actually felt kind of scared going in there. We were holding our breath more.’(#45, male, resident for 32 years)
‘I think it is not racial. It is because of the class… Maybe if I was taking the bus in China town, the drivers wouldn’t really be so polite. My area is mostly WASP [White Anglo-Saxon Protestant], they are very polite, even if I am Asian-looking.’(#46, female, resident for 54 years)
3.3. (Mis)trust in Authorities’ Information
‘Actually, put it this way, I always look at the official news first, no matter what it is. There are some facts, and I would look for more on my own. I think Canada is neutral up until now [May 2020]. I read the government news there, even Dr. Teresa Tam said not to wear masks, the government promoted that don’t wear mask if you are not sick, this…because I came from Hong Kong, I experienced SARS. When it seriously contradicts my opinions, I tend not to believe it, or I would look at and check with the media that I can trust.’(#66, female, resident for 2.5 years)
‘I would say in terms of the channels, news, mostly I hear them, but, like, do I 100% trust it? I don’t. I have personal opinions.’(#14, female, resident for 22 years)
3.4. Diverging Pathways/Types of Cognitive Dissonance
- Fear, shame, and dissociation from cognitive dissonance generates hesitancy and isolation.
‘Of course, for the sake of my health and other people’s health, I should follow the government’s instruction, for example, keep social distance. But my opinion is that, given so many racists going against Chinese because of COVID-19, I need to behave in the best way so that those racists have no excuses to find fault in me.’(#38, female, resident for 30 years)
‘It hasn’t happened yet. I haven’t experienced anything like that. But one thing is because I stay at home almost all the time, so I don’t have any interaction with outside people, so that’s part of the reason.’(#56, male, resident for 50 years)
‘I do see like—just sometimes even internalised racism against Mainland Chinese people. I think a good example would be when the whole COVID stuff started, like my family sending a chat, my extended family sending a chat being like “We should avoid places where Chinese people hang out”.’(#18, female, resident for 1.5 years)
- 2.
- Rationalization of and ambivalence (uncertainty) toward cognitive dissonance maintains status quo.
‘When I went to the supermarket, people stayed far from us early in March when we wore masks. But yes, they don’t look nice, but I don’t—I don’t think that’s a bad thing either. Because they’re trying to protect themselves.’(#17, male, resident of the GTA for 28 years)
‘I guess it depends, because some of the immigrants…don’t come into contact with a lot of foreign—like, the mainstream society. Maybe they run a restaurant business, you will have their own food, they are all Chinese. Right? …They are not interested in changing or they are not interested to say protest or anything like that. They are not interested. They are very comfortable in terms of staying in their own small circle.’(#27, male, resident for 7 years)
‘Frankly, I don’t think more people standing out would make a difference [to stigma]. I would think, what is next after you say it? It will only result in useless arguments.’(#66, female, resident for 2.5 years)
‘We [Chinese] might have a culture that is easy going and it is not easy for a Chinese to go to a place and complain or report or go to the government to complain. We do not have that.’(#28, male, resident for 25 years)
‘I don’t think we really care about the stigma unless we get bullied.’(#14, female, resident for 22 years)
- 3.
- Externalizing cognitive dissonance through resistance and distancing facilitates deconstructing and reauthoring (reassigning) responsibility.
‘As soon as he saw me, he covered his face and then ran away. So, once I saw that, I was like-…I was really shocked because Toronto, right?… This is the biggest city in Canada and then the most multicultural city in Canada—in the world, I would say. I’m surprised that people react like that. I’m shocked more than disappointed.’(#62, female, resident for 7 years)
‘I thought it [overt stigma] was really funny, but they were being jerks. But it was really funny because they would like oh they wanted a seat, they’d start coughing and people would form of black plague ring around them like, whoa, empty seat and they sit down and they start laughing to themselves because they knew people are freaking out. Like, hey, you’re going to look at me because I’m Asian and I’m coughing. And you’re going to treat me like that? I’m going to take your seat.’(#45, male to son, the former a resident for 32 years)
‘Well, I don’t think the Chinese community needs to be treated like any differently…But I don’t think you should do anything differently the way you treat Chinese people. I think maybe just like, I don’t know how to destigmatise it, but yeah, like more awareness.’(#51, female student, resident for 11 years who denied racism)
‘I think it should be done at some very grassroot events… It could affect the questions in Liberal Education, we could teach the children we shouldn’t discriminate, and then we have these different cases. If they have gone through this process, it would be easier for them.’(#66, female, resident for 2.5 years)
‘So together with these so-called exchanges and advocacy, I think this is a really hard thing to do. I personally like this to take place in the form of a video or use a video to tell a story. It is more straightforward and figurative.’(#80, female student, resident for less than one year)
4. Discussion
4.1. Mapping Our Results to Risk Perception Targeting Cognitive Dissonance
‘When reality clashes with our deepest convictions, we’d rather recalibrate reality than amend our worldview. Not only that, but we become even more rigid in our beliefs than before’(p. 44).
4.2. Implications for Health Policy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization [WHO]. Timeline: WHO’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline (accessed on 30 January 2023).
- Mamuji, A.; Lee, C.; Rozdilsky, J.; D’Souza, J.; Chu, T. Anti-Chinese stigma in the Greater Toronto Area during COVID-19: Aiming the spotlight towards community capacity. Soc. Sci. Humanit. Open 2021, 4, 100232. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, M. How a Toronto hospital handled Canada’s first COVID-19 case: ‘We didn’t know this was a moment in history’. Toronto Star, 25 July 2020. Available online: https://www.thestar.com/news/gta/how-a-toronto-hospital-handled-canada-s-first-covid-19-case-we-didn-t-know/article_c9204901-9111-5745-aea1-0ff4abbc142c.html (accessed on 5 April 2024).
- Chinese Canadian National Council for Social Justice, CCNC-SJ. Anti- Asian racism rife amid COVID-19 in Canada’s largest cities. 27 April 2020. Available online: https://ccncsj.ca/nationalpollbias/ (accessed on 3 June 2023).
- Angus Reid Institute. Blame, Bullying and Disrespect: Chinese Canadians Reveal Their Experiences with Racism during COVID-19. 2020. Available online: http://angusreid.org/racism-chinese-canadians-covid19/ (accessed on 21 March 2021).
- Alqahtani, M.M.; Arnout, B.A.; Fadhel, F.H.; Sufyan, N.S.S. Risk perceptions of COVID-19 and its impact on precautionary behavior: A qualitative study. Patient Educ. Couns. 2021, 104, 1860–1867. [Google Scholar] [CrossRef] [PubMed]
- Demirtaş-Madran, H.A. Exploring the motivation behind discrimination and stigmatization related to COVID-19: A social psychological discussion based on the main theoretical explanations. Front. Psychol. 2020, 11, 569528. [Google Scholar] [CrossRef] [PubMed]
- Maloney, E.K.; Lapinski, M.K.; Witte, K. Fear Appeals and Persuasion: A Review and Update of the Extended Parallel Process Model. Soc. Personal. Psychol. Compass 2011, 5, 206–219. [Google Scholar] [CrossRef]
- Wallace-Williams, D.M.; Tiu Wright, L.; Dandis, A.O. Social norms, cues and improved communication to influence behaviour change of smokers. J. Mark. Commun. 2021, 29, 288–313. [Google Scholar] [CrossRef]
- Hullett, C.R.; Witte, K. Predicting intercultural adaptation and isolation: Using the extended parallel process model to test anxiety/uncertainty management theory. Int. J. Intercult. Relat. 2001, 25, 125–139. [Google Scholar] [CrossRef]
- Poston, D.L.; Wong, J.H. The Chinese diaspora: The current distribution of the overseas Chinese population. Chin. J. Sociol. 2016, 2, 348–373. [Google Scholar] [CrossRef]
- Kline, N.S. Rethinking COVID-19 vulnerability: A call for LGBTQ+ Im/migrant health equity in the United States during and after a pandemic. Health Equity 2020, 4, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z. Unsettled belongings: Chinese immigrants’ mental health vulnerability as a symptom of international politics in the COVID-19 pandemic. J. Humanist. Psychol. 2021, 61, 198–218. [Google Scholar] [CrossRef]
- Leung, D.Y.L.; Hwu, H.; Khan, S.; Mamuji, A.; Rozdilsky, J.; Chu, T.; Lee, C. Understanding the Risk of Social Vulnerability for the Chinese Diaspora during the COVID-19 Pandemic: A Model Driving Risk Perception and Threat Appraisal of Risk Communication—A Qualitative Study. Int. J. Environ. Res. Public Health 2024, 21, 512. [Google Scholar] [CrossRef]
- Cooper, J. Cognitive dissonance: Where we’ve been and where we’re going. Int. Rev. Soc. Psychol. 2019, 32. [Google Scholar] [CrossRef]
- Aguilar, P.; Correia, I.; de Vries, J.; Tortora, L. Cognitive dissonance induction as an “inoculator” against negative attitudes towards victims. Soc. Personal. Psychol. Compass 2022, 16, e12715. [Google Scholar] [CrossRef]
- Canseco, M. Canadians Satisfied with Governments on COVID-19 Handling. 2020. Available online: https://researchco.ca/2020/03/24/covid-19-governments/ (accessed on 4 April 2022).
- Mamuji, A.; Rozdilsky, J.; Lee, C.; Mwarumba, N.; Tubula, M.; Chu, T. Expanding the Narrative on Anti-Chinese Stigma during COVID-19. August 2020. Available online: https://figshare.com/articles/preprint/EXPANDING_THE_NARRATIVE_ON_ANTI-CHINESE_STIGMA_DURING_COVID-19_-_Initial_Report_pdf/12759512/1. [CrossRef]
- Stats Canada. Census Profile. Census Population. Toronto, Ontario 2021. Census Metropolitan Area. Available online: https://www12.statcan.gc.ca/census-recensement/2021/dp-pd/prof/details/page.cfm?Lang=E&GENDERlist=1,2,3&STATISTIClist=1,4&HEADERlist=0&DGUIDlist=2021S0503535&SearchText=Toronto (accessed on 29 June 2023).
- Leung, V.W.Y.; Tan, W.; Chuang, D.-M.; Tsang, K.T.; Lai, D.W.L. A Multidimensional Approach to Explore the Experiences with Ethnic Matching amongst Chinese Social Service Practitioners in the Greater Toronto Area. Br. J. Soc. Work. 2022, 52, 1592–1611. [Google Scholar] [CrossRef]
- Adekunle, T.B.; Mohammed, W.F. Communication in context: How culture, structure, and agency shape health and risk communication about COVID-19 in Ghana. World Med. Health Policy 2022, 14, 437–444. [Google Scholar] [CrossRef]
- Elder-Vass, D. The Causal Power of Social Structures: Emergence, Structure and Agency, 1st ed.; Cambridge University Press: Cambridge, UK, 2011; pp. 1–221. [Google Scholar]
- Vasileiou, K.; Barnett, J.; Thorpe, S.; Young, T. Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15-year period. BMC Med. Res. Methodol. 2018, 18, 148. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. NVivo. 2020. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 21 May 2021).
- Fryer, T. A critical realist approach to thematic analysis: Producing causal explanations. J. Crit. Realism 2022, 21, 365–384. [Google Scholar] [CrossRef]
- Guo, S. Reimagining Chinese diasporas in a transnational world: Toward a new research agenda. J. Ethn. Migr. Stud. 2022, 48, 847–872. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Wood, E.; Miller, S.K. Cognitive dissonance and disaster risk communication. J. Emerg. Manag. Disaster Commun. 2021, 2, 39–56. [Google Scholar] [CrossRef]
- Cottle, T.J. On Narratives and the Sense of Self. Qual. Inq. 2002, 8, 535–549. [Google Scholar] [CrossRef]
- Carlson, T.S. What is a good story and how do we tell one? Narrative therapy as a counter-storytelling practice. J. Narrat. Fam. Ther. 2020, IWP Special Release, 16–37. [Google Scholar]
- Meaney, T.; Rieger, E. Integrating cognitive dissonance and social consensus to reduce weight stigma. Body Image 2021, 37, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Nunn, C. The participatory arts-based research project as an exceptional sphere of belonging. Qual. Res. 2022, 22, 251–268. [Google Scholar] [CrossRef]
- Harmon-Jones, E.; Mills, J. An introduction to cognitive dissonance theory and an overview of current perspectives on the theory. In Cognitive Dissonance: Reexamining a Pivotal Theory in Psychology, 2nd ed.; American Psychological Association: Washington, DC, USA, 2019; pp. 3–24. [Google Scholar] [CrossRef]
- Brown, B. Atlas of the Heart: Mapping Meaningful Connection and the Language of Human Experience; Random House: New York, NY, USA, 2021; pp. 1–296. [Google Scholar]
- Esholdt, H.F. Virgins, Terrorists, and Ten Children: Immigrants’ Humorous Play with Ethnic Stereotypes in Bonding with Danes in the Workplace. Symb. Interact. 2019, 42, 691–716. [Google Scholar] [CrossRef]
- Camlin, C.S.; Charlebois, E.D.; Geng, E.; Semitala, F.; Wallenta, J.; Getahun, M.; Kampiire, L.; A Bukusi, E.; Sang, N.; Kwarisiima, D.; et al. Redemption of the “spoiled identity:” the role of HIV-positive individuals in HIV care cascade interventions. J. Int. AIDS Soc. 2017, 20, e25023–e25032. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.E.; Saag, K.G.; Chiriboga, G.; Lemon, S.C.; Allison, J.J.; Mudano, A.; Rosas, G.; Foster, P.J.; Danila, M.I. A multi-step approach to develop a “storytelling” intervention to improve patient gout knowledge and improve outpatient follow-up. Contemp. Clin. Trials Commun. 2023, 33, 101149. [Google Scholar] [CrossRef] [PubMed]
- Oktavianus, J.; Lin, W.Y. Soliciting social support from migrant domestic workers’ connections to storytelling networks during a public health crisis. Health Commun. 2023, 38, 1179–1188. [Google Scholar] [CrossRef]
- Hernandez, R.A.; Haidet, P.; Gill, A.C.; Teal, C.R. Fostering students’ reflection about bias in healthcare: Cognitive dissonance and the role of personal and normative standards. Med. Teach. 2013, 35, e1082–e1089. [Google Scholar] [CrossRef]
- Ming, X.; De Jong, M.D. Mental Well-Being of Chinese Immigrants in the Netherlands during the COVID-19 Pandemic: A Survey Investigating Personal and Societal Antecedents. Sustainability 2021, 13, 4198. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, D.Y.L.; Khan, S.; Hwu, H.; Mamuji, A.; Rozdilsky, J.; Chu, T.; Lee, C. The Risk Perception of the Chinese Diaspora during the COVID-19 Pandemic: Targeting Cognitive Dissonance through Storytelling. Int. J. Environ. Res. Public Health 2024, 21, 556. https://doi.org/10.3390/ijerph21050556
Leung DYL, Khan S, Hwu H, Mamuji A, Rozdilsky J, Chu T, Lee C. The Risk Perception of the Chinese Diaspora during the COVID-19 Pandemic: Targeting Cognitive Dissonance through Storytelling. International Journal of Environmental Research and Public Health. 2024; 21(5):556. https://doi.org/10.3390/ijerph21050556
Chicago/Turabian StyleLeung, Doris Yuet Lan, Shoilee Khan, Hilary Hwu, Aaida Mamuji, Jack Rozdilsky, Terri Chu, and Charlotte Lee. 2024. "The Risk Perception of the Chinese Diaspora during the COVID-19 Pandemic: Targeting Cognitive Dissonance through Storytelling" International Journal of Environmental Research and Public Health 21, no. 5: 556. https://doi.org/10.3390/ijerph21050556