
Acupuncture for Japanese Katakori (Chronic Neck Pain): A Randomized Placebo-Controlled Double-Blind Study
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Setting and Participants
2.1.1. Inclusion of Volunteers
2.1.2. Exclusion of Volunteers
- Patients with a plan within 24 h to receive acupuncture, massage, medication or any other treatment for neck/shoulder stiffness.
- Patients with a plan within 24 h to do self-care for neck/shoulder stiffness, e.g., exercise, stretching and/or supplements.
- Patients who had any neurological symptoms, such as paralysis or numbness in the neck, shoulder or upper extremities.
- Patients who were diagnosed with diseases that produce neck/shoulder stiffness according to the last annual medical examination.
- Systolic blood pressure was over 140 mmHg and/or diastolic pressure was over 90 mmHg just before the treatment.
2.2. Acupuncture Needles
2.3. Randomization
2.4. Explanation to Patients
2.5. Patients’ Evaluation of Neck/Shoulder Stiffness before Treatment
2.6. Needle Application and Acupoints
2.7. Patients’ Evaluation after Treatment
2.8. Practitioners’ Guess as to Treatment
2.9. Outcomes
2.9.1. Primary Measurements
2.9.2. Secondary Outcome Measurements
2.10. Adverse Events
2.11. Statistical Analysis
3. Results
3.1. Baseline Characteristics
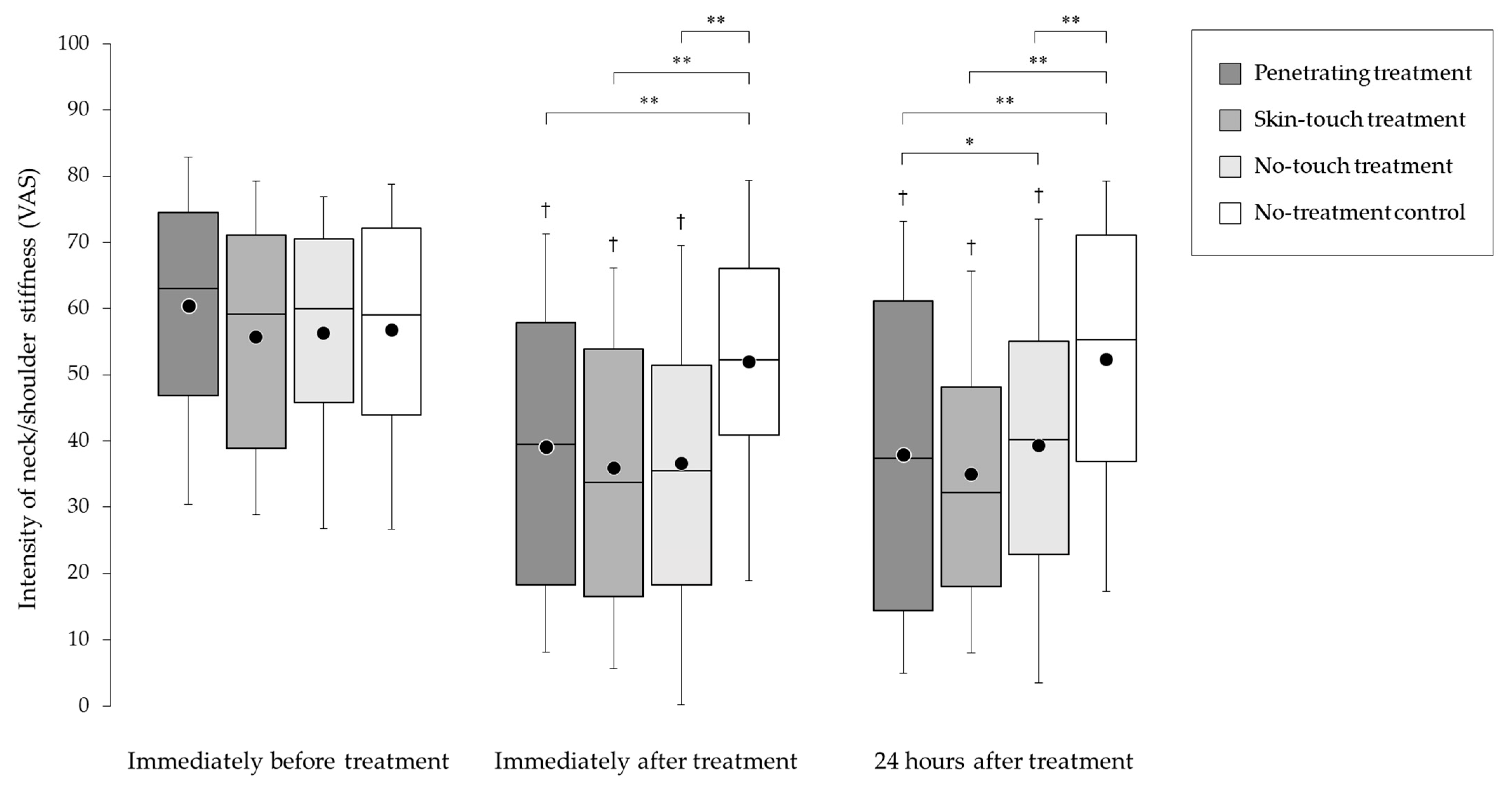
3.2. Improvement of Neck/Shoulder Stiffness Score Immediately and 24 h after the Treatment
3.3. Effect of Blinding
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sawada, T.; Matsudaira, K.; Muto, Y.; Koga, T.; Takahashi, M. Potential risk factors for onset of severe neck and shoulder discomfort (Katakori) in urban Japanese workers. Ind. Health 2016, 54, 230–236. [Google Scholar] [CrossRef]
- Fujii, T.; Matsudaira, K.; Yoshimura, N.; Hirai, M.; Tanaka, S. Associations between neck and shoulder discomfort (Katakori) and job demand, job control, and worksite support. Mod. Rheumatol. 2013, 23, 1198–1204. [Google Scholar] [CrossRef]
- Yabuki, S. Pathogenesis of the neck-shoulder stiffness (Katakori). Clin. Orthop. Surg. 2007, 42, 413–417. (In Japanese) [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare of Japan. Comprehensive Survey of Living Conditions 2019, Figure 14 in Health of Household Members. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa22/dl/04.pdf (accessed on 27 September 2023).
- Matsudaira, K.; Isomura, T.; Miyoshi, K.; Okazaki, H.; Konishi, H. Risk factors for low back pain and katakori: A new concept. Nihon Rinsho Jpn. J. Clin. Med. 2014, 72, 244–250. (In Japanese) [Google Scholar]
- Kitahara, M.; Shibata, M. “Katakori”: A pain syndrome specific to the Japanese. Curr. Pain Headache Rep. 2016, 20, 64. [Google Scholar] [CrossRef]
- Musculoskeletal Disorders in Visual Display Unit (VDU) Tasks. Available online: https://oshwiki.osha.europa.eu/en/themes/musculoskeletal-disorders-visual-display-unit-vdu-tasks (accessed on 27 September 2023).
- Kimura, T.; Tsuda, Y.; Uchida, S.; Eboshida, A. Association of perceived stress and stiff neck/shoulder with health status: Multiple regression models by gender. Hiroshima J. Med. Sci. 2006, 55, 101–107. [Google Scholar] [PubMed]
- Lundberg, U.; Kadefors, R.; Melin, B.; Palmerud, G.; Hassmén, P.; Engström, M.; Dohns, I.E. Psychophysiological stress and EMG activity of the trapezius muscle. Int. J. Behav. Med. 1994, 1, 354–370. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, T.; Yamaguchi, S.; Igarashi, H.; Omata, H.; Suzuki, M.; Tanaka, K.; Isobe, H.; Mimura, T. Efficacy of acupuncture on VDT workers (2). J. Jpn. Soc. Acupunct. Moxibustion 2011, 61, 51–58. (In Japanese) [Google Scholar]
- Suzuki, M.; Yamaguchi, S.; Igarashi, H.; Omata, H.; Kikuchi, T.; Tanaka, K.; Isobe, H.; Oono, S.; Mimura, T.; Kimijima, M. Efficacy of acupuncture on VDT workers (1). J. Jpn. Soc. Acupunct. Moxibustion 2010, 60, 829–836. (In Japanese) [Google Scholar]
- The World Health Organisation Recommends Acupuncture for over 100 Conditions. Available online: https://holistic-health.org.uk/world-health-organisation-recommends-acupuncture-100-conditions/ (accessed on 27 September 2023).
- Chon, T.Y.; Lee, M.C. Acupuncture. Mayo Clin. Proc. 2013, 88, 1141–1146. [Google Scholar] [CrossRef]
- Vas, J.; Perea-Milla, E.; Méndez, C.; Sánchez Navarro, C.; León Rubio, J.M.; Brioso, M.; García Obrero, I. Efficacy and safety of acupuncture for chronic uncomplicated neck pain: A randomised controlled study. Pain 2006, 126, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Michalsen, A. Management of chronic pain using complementary and integrative medicine. BMJ 2017, 357, j1284. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, H.; Vertosick, E.A.; Foster, N.E.; Lewith, G.; Linde, K.; Sherman, K.J.; Witt, C.M.; Vickers, A.J.; Acupuncture Trialists’ Collaboration. The persistence of the effects of acupuncture after a course of treatment: A meta-analysis of patients with chronic pain. Pain 2017, 158, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Vertosick, E.A.; Lewith, G.; MacPherson, H.; Foster, N.E.; Sherman, K.J.; Irnich, D.; Witt, C.M.; Linde, K.; Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: Update of an individual patient data meta-analysis. J. Pain 2018, 19, 455–474. [Google Scholar] [CrossRef] [PubMed]
- Filshie, J.; White, A.; Cummings, M. Medical Acupuncture: A Western Scientific Approach, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 45–65, 91–169. [Google Scholar]
- Matsuura, Y.; Fujimoto, H.; Muko, A.; Koga, Y.; Yasuno, F.; Sakai, T. Effects of acupuncture treatment on changes in salivary cortisol concentration in patients with neck pain—A pilot randomized c_ontrolled trial. J. Jpn. Soc. Acupunct. Moxibustion 2017, 67, 124–132. (In Japanese) [Google Scholar] [CrossRef]
- Jimbo, S.; Atsuta, Y.; Kobayashi, T.; Matsuno, T. Effects of dry needling at tender points for neck pain (Japanese: Katakori): Near-infrared spectroscopy for monitoring muscular oxygenation of the trapezius. J. Orthop. Sci. 2008, 13, 101–106. [Google Scholar] [CrossRef]
- Huruya, E.; Nayuki, T.; Yakame, M.; Furuumi, H.; Shinohara, R.; Nimura, R.; Kaneko, Y.; Sakamoto, A. Effect of press tack needle treatment on shoulder stiffness. J. Jpn. Soc. Acupunct. Moxibustion 2002, 52, 553–561. (In Japanese) [Google Scholar]
- Nabeta, T.; Kawakita, K. Relief of chronic neck and shoulder pain by manual acupuncture to tender points—A sham-controlled randomized trial. Complement. Ther. Med. 2002, 10, 217–222. [Google Scholar] [CrossRef]
- Itoh, K.; Kitakoji, H. Acupuncture for chronic pain in Japan: A review. Evid. Based Complement. Alternat. Med. 2007, 4, 431–438. [Google Scholar] [CrossRef]
- Streitberger, K.; Kleinhenz, J. Introducing a placebo needle into acupuncture research. Lancet 1998, 352, 364–365. [Google Scholar] [CrossRef]
- Park, J.; White, A.; Lee, H.; Ernst, E. Developing of a new sham needle. Acupunct. Med. 1999, 17, 110–112. [Google Scholar] [CrossRef]
- Kaptchuk, T.J. Placebo needle for acupuncture. Lancet 1998, 352, 992. [Google Scholar] [CrossRef]
- Kaptchuk, T.J. Methodological issues in trials of acupuncture. JAMA 2001, 285, 1015–1016, author reply 1016. [Google Scholar] [CrossRef]
- Marchant, J. Acupuncture in cancer study reignites debate about controversial technique. Nature 2017, 552, 157–158. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.K.; Shapiro, E. The Powerful Placebo: From Ancient Priest to Modern Physician; The Johns Hopkins University Press: London, UK, 1997; pp. 137–174, 190–216. [Google Scholar]
- Shapiro, A.K.; Shapiro, E. The placebo: Is it much ado about nothing? In The Placebo Effect: An Interdisciplinary Exploration; Harrington, A., Ed.; Harvard University Press: Boston, MA, USA, 1997; pp. 12–36. [Google Scholar]
- Gracely, R.H.; Dubener, R.; Deeter, W.R.; Wolskee, P.J. Clinicians’ expectations influence placebo analgesia. Lancet 1985, 1, 43. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.A.; Deyo, R.A.; Losser, J.D.; Korff, M.V.; Fordyce, W.E. The importance of placebo effects in pain treatment and research. JAMA 1994, 271, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Chalmers, I.; Hayes, R.J.; Altman, D.G. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995, 273, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Takakura, N.; Yajima, H. A placebo acupuncture needle with potential for double blinding—A validation study. Acupunct. Med. 2008, 26, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Takayama, M.; Yajima, H.; Kawase, A.; Homma, I.; Izumizaki, M.; Takakura, N. The potential of double blinding with two placebo acupuncture needles: A randomized controlled pilot-trial. Medicines 2014, 2, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Takakura, N.; Takayama, M.; Kawase, A.; Kaptchuk, T.J.; Kong, J.; Yajima, H. Design of a randomised acupuncture trial on functional neck/shoulder stiffness with two placebo controls. BMC Complement. Altern. Med. 2014, 14, 246. [Google Scholar] [CrossRef]
- Takagishi, K.; Hoshino, Y.; Ide, J.; Sugihara, T.; Hata, Y.; Sano, H.; Hamada, J.; Yabuki, S.; Mochiduki, Y.; Suzuki, K.; et al. A project study for Katakori (2004–2006). Nihon Seikeigeka Gakkai Zasshi J. Jpn. Orthop. Assoc. 2008, 82, 901–911. (In Japanese) [Google Scholar]
- Fujii, T.; Matsudaira, K.; Noma, K.; Ishizuka, A.; Yamada, K.; Arisaka, M.; Higashikawa, A. Objective measurement of neck-shoulder discomfort and analysis of associated factors. Rinsho Seikei Geka Clin. Orthop. Surg. 2012, 47, 619–624. (In Japanese) [Google Scholar] [CrossRef]
- Kelly, A.M. The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain. Emerg. Med. J. 2001, 18, 205–207. [Google Scholar] [CrossRef]
- Lundeberg, T.; Lund, I.; Näslund, J.; Thomas, M. The emperors sham—Wrong assumption that sham needling is sham. Acupunct. Med. 2008, 26, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Birch, S. A review and analysis of placebo treatments, placebo effects, and placebo controls in trials of medical procedures when sham is not inert. J. Altern. Complement. Med. 2006, 12, 303–310. [Google Scholar] [CrossRef]
- Kaptchuk, T.J.; Miller, F.G. Open label placebo: Can honestly prescribed placebos evoke meaningful therapeutic benefits? BMJ 2018, 363, k3889. [Google Scholar] [CrossRef]
- Benedetti, F. Placebo Effects, 2nd ed.; Oxford University Press: Oxford, UK, 2014; pp. 109–139, 157–169, 295–300. [Google Scholar]
- Onda, A.; Onozato, K.; Kimura, M. Clinical features of neck and shoulder pain (Katakori) in Japanese hospital workers. Fukushima J. Med. Sci. 2022, 68, 79–87. [Google Scholar] [CrossRef]
- Natsume, K.; Handa, Y.; Takasaki, H. Determination of the conceptual structures of the disturbed activities of daily living due to Katakori by evaluating patients’ values or perceptions using a patient-elicitation technique. J. Phys. Ther. Sci. 2021, 33, 683–688. [Google Scholar] [CrossRef]
- Wahlström, J.; Hagberg, M.; Toomingas, A.; Wigaeus Tornqvist, E. Perceived muscular tension, job strain, physical exposure, and associations with neck pain among VDU users; A prospective cohort study. Occup. Environ. Med. 2004, 61, 523–528. [Google Scholar] [CrossRef]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, M.R. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Gollub, R.L.; Kong, J. For placebo effects in medicine, seeing is believing. Sci. Transl. Med. 2011, 3, 70ps5. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L.; Miller, F.G. Harnessing the placebo effect: The need for translational research. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 2011, 366, 1922–1930. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.G.; Colloca, L. The legitimacy of placebo treatments in clinical practice: Evidence and ethics. Am. J. Bioeth. 2009, 9, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Bäumler, P.; Zhang, W.; Stübinger, T.; Irnich, D. Acupuncture-related adverse events: Systematic review and meta-analyses of prospective clinical studies. BMJ Open 2021, 11, e045961. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Arms of Acupuncture Treatments | p-Value * | ||||
|---|---|---|---|---|---|
| Penetrating Treatments | Skin-Touch Treatments | No-Touch Treatments | No-Treatment Control | ||
| Patients included in analysis (number) | 100 | 99 | 99 | 100 | |
| Age (mean (SD) in years) | 29.5 (8.6) | 29.1 (8.3) | 29.2 (10.2) | 28.3 (8.2) | 0.81 (0.44) |
| Gender (numbers: male/female) | 41/59 | 41/58 | 44/55 | 33/67 | 0.4 |
| Duration of neck/shoulder stiffness before treatment (numbers: ≤2 weeks/<2 weeks and <3 months/≥3 months) | 23/15/62 | 29/17/53 | 18/24/57 | 30/20/50 | 0.27 |
| Intensity of neck/shoulder stiffness before treatment (mean (SD) on 100 mm visual analogue scale) | 60.7 (19.5) | 56.0 (19.9) | 56.5 (18.8) | 57.0 (18.9) | 0.3 (0.92) |
| Arms of Acupuncture Treatments | p-Value * | |||
|---|---|---|---|---|
| Penetrating Treatments | Skin-Touch Treatments | No-Touch Treatments | ||
| Patients’ guesses to treatment (‘penetrating’/‘skin-touch’/‘no-touch’/‘cannot identify’) | ||||
| Immediately after treatment (number) | 83/14/0/3 | 75/19/2/3 | 26/27/39/7 | <0.01 |
| 24 h after treatment (number) | 80/14/3/3 | 74/18/3/4 | 28/25/38/8 | <0.01 |
| Practitioners’ guesses to treatment (‘penetrating’/‘skin-touch’/‘no-touch’/‘cannot identify’) | 30/35/27/8 | 29/36/23/11 | 17/38/31/13 | 0.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takakura, N.; Takayama, M.; Kawase, A.; Kaptchuk, T.J.; Kong, J.; Vangel, M.; Yajima, H. Acupuncture for Japanese Katakori (Chronic Neck Pain): A Randomized Placebo-Controlled Double-Blind Study. Medicina 2023, 59, 2141. https://doi.org/10.3390/medicina59122141
Takakura N, Takayama M, Kawase A, Kaptchuk TJ, Kong J, Vangel M, Yajima H. Acupuncture for Japanese Katakori (Chronic Neck Pain): A Randomized Placebo-Controlled Double-Blind Study. Medicina. 2023; 59(12):2141. https://doi.org/10.3390/medicina59122141
Chicago/Turabian StyleTakakura, Nobuari, Miho Takayama, Akiko Kawase, Ted J. Kaptchuk, Jian Kong, Mark Vangel, and Hiroyoshi Yajima. 2023. "Acupuncture for Japanese Katakori (Chronic Neck Pain): A Randomized Placebo-Controlled Double-Blind Study" Medicina 59, no. 12: 2141. https://doi.org/10.3390/medicina59122141