
Spatial Distribution of Macrophage and Lymphocyte Subtypes within Tumor Microenvironment to Predict Recurrence of Non-Muscle-Invasive Papillary Urothelial Carcinoma after BCG Immunotherapy

 , ,
, ,
Abstract
:1. Introduction
2. Results
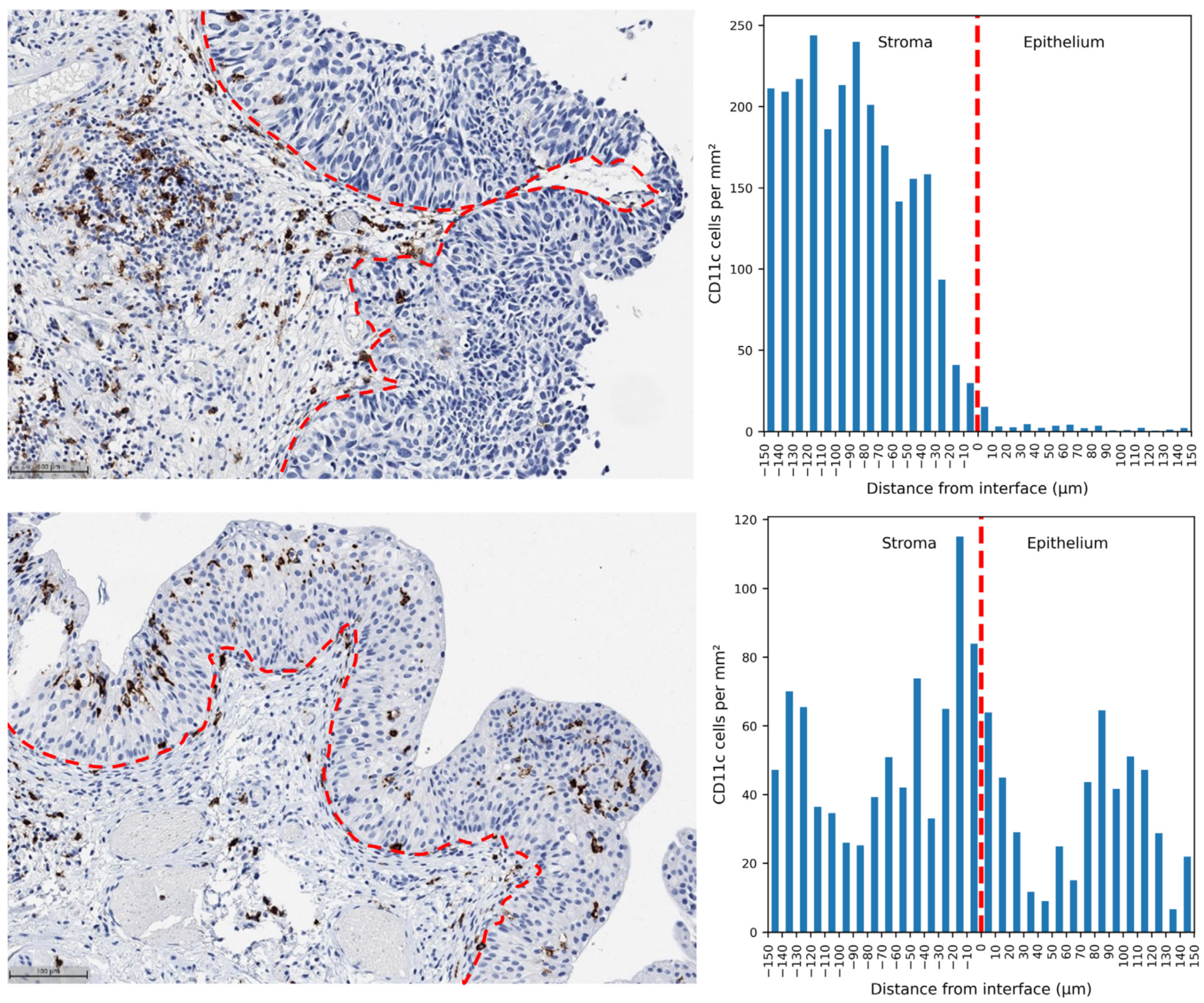
2.1. Exploring the Interface Zone Width Settings to Optimize Predictive Indicators
2.2. Univariate Cox Regression for Prediction of RFS
2.3. Multiple Cox Regression
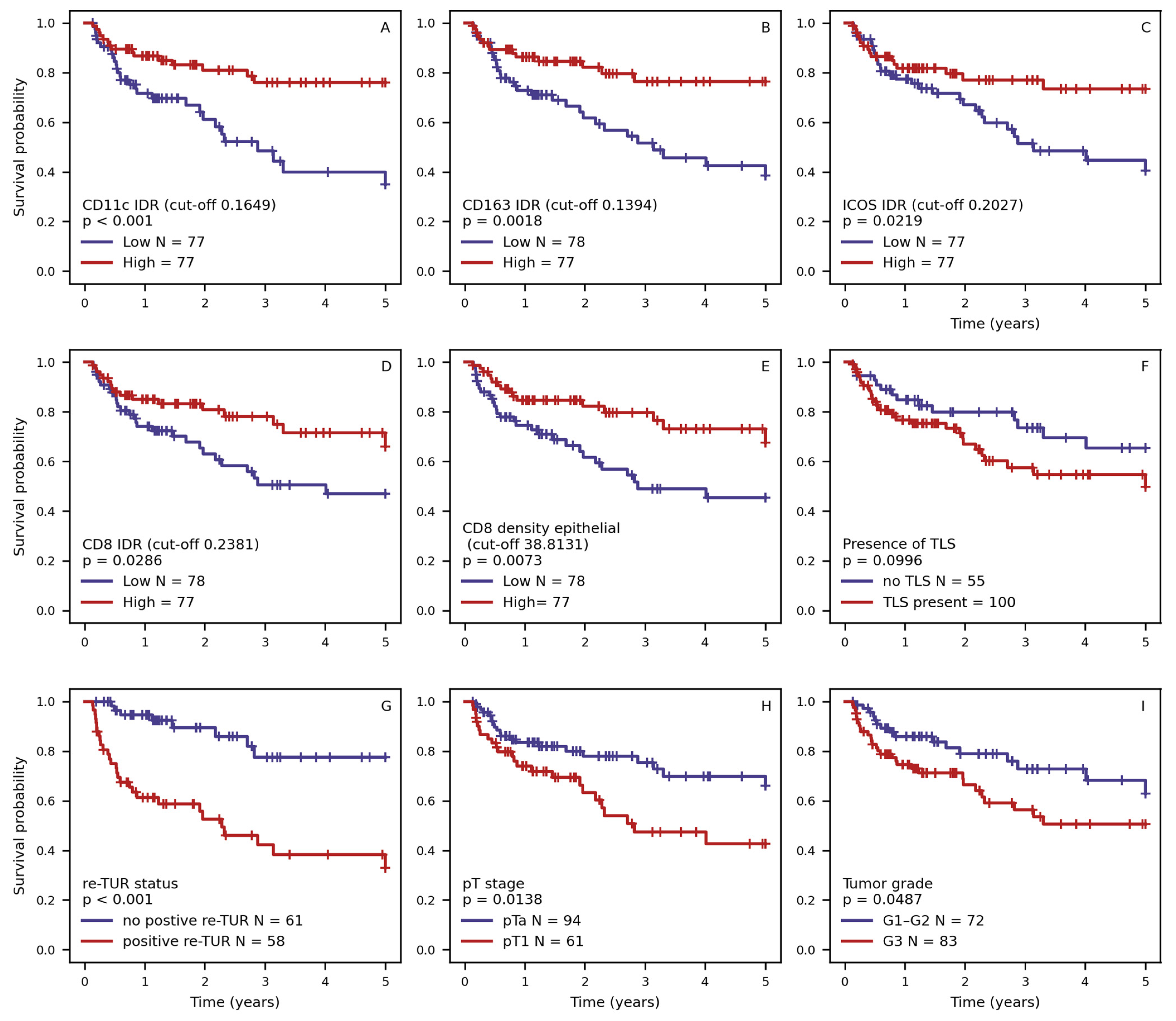
2.4. Kaplan–Meier RFS Analysis of the Selected Features
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. IHC Slide Preparation and Digitization
4.3. Digital Image Analysis
4.4. Assessment of the Spatial Distribution of the Immune Cells
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Čapoun, O.; Cohen, D.; Compérat, E.; Escrig, J.L.D.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, H.; et al. European Association of Urology Guidelines on Non-Muscle-Invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2021, 81, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Kamat, A.M.; Li, R.; O’Donnell, M.A.; Black, P.C.; Roupret, M.; Catto, J.W.; Comperat, E.; Ingersoll, M.A.; Witjes, W.P.; McConkey, D.J.; et al. Predicting Response to Intravesical Bacillus Calmette-Guérin Immunotherapy: Are We There Yet? A Systematic Review. Eur. Urol. 2018, 73, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Jäger, W.; Thomas, C.; Haag, S.; Hampel, C.; Salzer, A.; Thüroff, J.W.; Wiesner, C. Early vs Delayed Radical Cystectomy for ‘High-Risk’ Carcinoma Not Invading Bladder Muscle: Delay of Cystectomy Reduces Cancer-Specific Survival. BJU Int. 2011, 108, E284–E288. [Google Scholar] [CrossRef] [PubMed]
- Song, D.; Powles, T.; Shi, L.; Zhang, L.; Ingersoll, M.A.; Lu, Y.-J. Bladder Cancer, a Unique Model to Understand Cancer Immunity and Develop Immunotherapy Approaches. J. Pathol. 2019, 249, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Hanada, T.; Nakagawa, M.; Emoto, A.; Nomura, T.; Nasu, N.; Nomura, Y. Prognostic Value of Tumor-Associated Macrophage Count in Human Bladder Cancer. Int. J. Urol. 2000, 7, 263–269. [Google Scholar] [CrossRef]
- Krpina, K.; Babarović, E.; Španjol, J.; Đorđević, G.; Maurer, T.; Jonjić, N. Correlation of Tumor-Associated Macrophages and NK Cells with Bladder Cancer Size and T Stage in Patients with Solitary Low-Grade Urothelial Carcinoma. Wien. Klin. Wochenschr. 2016, 128, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Pichler, R.; Fritz, J.; Zavadil, C.; Claudia, Z.; Schäfer, G.; Culig, Z.; Brunner, A. Tumor-Infiltrating Immune Cell Subpopulations Influence the Oncologic Outcome after Intravesical Bacillus Calmette-Guérin Therapy in Bladder Cancer. Oncotarget 2016, 7, 39916–39930. [Google Scholar] [CrossRef] [PubMed]
- Ajili, F.; Kourda, N.; Darouiche, A.; Chebil, M.; Boubaker, S. Prognostic Value of Tumor-Associated Macrophages Count in Human Non-Muscle-Invasive Bladder Cancer Treated by BCG Immunotherapy. Ultrastruct. Pathol. 2013, 37, 56–61. [Google Scholar] [CrossRef]
- Boström, M.M.; Irjala, H.; Mirtti, T.; Taimen, P.; Kauko, T.; Ålgars, A.; Jalkanen, S.; Boström, P.J. Tumor-Associated Macrophages Provide Significant Prognostic Information in Urothelial Bladder Cancer. PLoS ONE 2015, 10, e0133552. [Google Scholar] [CrossRef]
- Ayari, C.; LaRue, H.; Hovington, H.; Decobert, M.; Harel, F.; Bergeron, A.; Têtu, B.; Lacombe, L.; Fradet, Y. Bladder Tumor Infiltrating Mature Dendritic Cells and Macrophages as Predictors of Response to Bacillus Calmette-Guérin Immunotherapy. Eur. Urol. 2009, 55, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Suriano, F.; Santini, D.; Perrone, G.; Amato, M.; Vincenzi, B.; Tonini, G.; Muda, A.O.; Boggia, S.; Buscarini, M.; Pantano, F. Tumor Associated Macrophages Polarization Dictates the Efficacy of BCG Instillation in Non-Muscle Invasive Urothelial Bladder Cancer. J. Exp. Clin. Cancer Res. 2013, 32, 87. [Google Scholar] [CrossRef]
- Miyake, M.; Tatsumi, Y.; Gotoh, D.; Ohnishi, S.; Owari, T.; Iida, K.; Ohnishi, K.; Hori, S.; Morizawa, Y.; Itami, Y.; et al. Regulatory T Cells and Tumor-Associated Macrophages in the Tumor Microenvironment in Non-Muscle Invasive Bladder Cancer Treated with Intravesical Bacille Calmette-Guérin: A Long-Term Follow-Up Study of a Japanese Cohort. Int. J. Mol. Sci. 2017, 18, 2186. [Google Scholar] [CrossRef] [PubMed]
- Ayari, C.; LaRue, H.; Hovington, H.; Caron, A.; Bergeron, A.; Têtu, B.; Fradet, V.; Fradet, Y. High Level of Mature Tumor-Infiltrating Dendritic Cells Predicts Progression to Muscle Invasion in Bladder Cancer. Hum. Pathol. 2013, 44, 1630–1637. [Google Scholar] [CrossRef] [PubMed]
- Pichler, R.; Gruenbacher, G.; Culig, Z.; Brunner, A.; Fuchs, D.; Fritz, J.; Gander, H.; Rahm, A.; Thurnher, M. Intratumoral Th2 Predisposition Combines with an Increased Th1 Functional Phenotype in Clinical Response to Intravesical BCG in Bladder Cancer. Cancer Immunol. Immunother. 2017, 66, 427–440. [Google Scholar] [CrossRef] [PubMed]
- Villoldo, G.M.; Pombo, M.T.; Aris, M.; Chemi, J.; Mandó, P.; Nagaraju, S.; Camean, J.; Burioni, A.; Egea, D.; Amat, M.; et al. A Th2-Score in the Tumor Microenvironment as a Predictive Biomarker of Response to Bacillus Calmette Guérin in Patients with Non-Muscle Invasive Bladder Carcinoma: A Retrospective Study. Oncol. Res. 2023, 31, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group. Adv. Anat. Pathol. 2017, 24, 235–251. [Google Scholar] [CrossRef] [PubMed]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group. Adv. Anat. Pathol. 2017, 24, 311–335. [Google Scholar] [CrossRef]
- Galon, J.; Pagès, F.; Marincola, F.M.; Angell, H.K.; Angell, H.K.; Thurin, M.; Lugli, A.; Zlobec, I.; Berger, A.; Bifulco, C.; et al. Cancer Classification Using the Immunoscore: A Worldwide Task Force. J. Transl. Med. 2012, 10, 205. [Google Scholar] [CrossRef]
- Masson-Lecomte, A.; Maillé, P.; Pineda, S.; Soyeux, P.; Sagrera, A.; Rava, M.; Lopez de Maturana, E.; Márquez, M.; Tardón, A.; Carrato, A.; et al. CD8+ Cytotoxic Immune Infiltrate in Non-Muscle Invasive Bladder Cancer: A Standardized Methodology to Study Association with Clinico-Pathological Features and Prognosis. Bladder Cancer 2019, 5, 159–169. [Google Scholar] [CrossRef]
- Kates, M.; Matoso, A.; Choi, W.; Baras, A.S.; Daniels, M.J.; Lombardo, K.; Brant, A.; Mikkilineni, N.; McConkey, D.J.; Kamat, A.M.; et al. Adaptive Immune Resistance to Intravesical BCG in Non-Muscle Invasive Bladder Cancer: Implications for Prospective BCG-Unresponsive Trials. Clin. Cancer Res. 2020, 26, 882–891. [Google Scholar] [CrossRef]
- Lillesand, M.; Kvikstad, V.; Mangrud, O.M.; Gudlaugsson, E.; van Diermen-Hidle, B.; Skaland, I.; Baak, J.P.A.; Janssen, E.A.M. Mitotic Activity Index and CD25+ Lymphocytes Predict Risk of Stage Progression in Non-Muscle Invasive Bladder Cancer. PLoS ONE 2020, 15, e0233676. [Google Scholar] [CrossRef]
- Bieri, U.; Enderlin, D.; Buser, L.; Wettstein, M.S.; Eberli, D.; Moch, H.; Hermanns, T.; Poyet, C. Modified Immunoscore Improves the Prediction of Progression-Free Survival in Patients with Non-Muscle-Invasive Bladder Cancer: A Digital Pathology Study. Front. Oncol. 2022, 12, 964672. [Google Scholar] [CrossRef]
- Drachneris, J.; Rasmusson, A.; Morkunas, M.; Fabijonavicius, M.; Cekauskas, A.; Jankevicius, F.; Laurinavicius, A. CD8+ Cell Density Gradient across the Tumor Epithelium–Stromal Interface of Non-Muscle Invasive Papillary Urothelial Carcinoma Predicts Recurrence-Free Survival after BCG Immunotherapy. Cancers 2023, 15, 1205. [Google Scholar] [CrossRef] [PubMed]
- Amatore, F.; Gorvel, L.; Olive, D. Role of Inducible Co-Stimulator (ICOS) in Cancer Immunotherapy. Expert Opin. Biol. Ther. 2020, 20, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Viveiros, N.; Flores, B.C.; Lobo, J.; Martins-Lima, C.; Cantante, M.; Lopes, P.; Deantonio, C.; Palu, C.; Sainson, R.C.; Hen-rique, R.; et al. Detailed Bladder Cancer Immunoprofiling Reveals New Clues for Immunotherapeutic Strategies. Clin. Transl. Immunol. 2022, 11, e1402. [Google Scholar] [CrossRef]
- Vaghjiani, R.G.; Skitzki, J.J. Tertiary Lymphoid Structures as Mediators of Immunotherapy Response. Cancers 2022, 14, 3748. [Google Scholar] [CrossRef] [PubMed]
- Koti, M.; Xu, A.S.; Ren, K.Y.M.; Visram, K.; Ren, R.; Berman, D.M.; Siemens, D.R. Tertiary Lymphoid Structures Associate with Tumour Stage in Urothelial Bladder Cancer. Bladder Cancer 2017, 3, 259–267. [Google Scholar] [CrossRef]
- van Dijk, N.; Gil-Jimenez, A.; Silina, K.; Montfoort, M.L.v.; Einerhand, S.; Jonkman, L.; Voskuilen, C.S.; Peters, D.; Sanders, J.; Lubeck, Y.; et al. The Tumor Immune Landscape and Architecture of Tertiary Lymphoid Structures in Urothelial Cancer. Front. Immunol. 2021, 12, 793964. [Google Scholar] [CrossRef]
- Jeong, H.; Hwang, I.; Kang, S.H.; Shin, H.C.; Kwon, S.Y. Tumor-Associated Macrophages as Potential Prognostic Biomarkers of Invasive Breast Cancer. J. Breast Cancer 2019, 22, 38–51. [Google Scholar] [CrossRef]
- Council for International Organizations of Medical Sciences (CIOMS). International Ethical Guidelines for Health-Related Research Involving Humans; Council for International Organizations of Medical Sciences (CIOMS): Geneva, Switzerland, 2016. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| IHC Marker | Feature | Optimal IZ Width (µm) | CI Mean (SD) |
|---|---|---|---|
| CD8 | Total density | 10 | 0.591 (0.157) |
| Stromal density | 10 | 0.574 (0.156) | |
| Epithelial density | 130 | 0.62 (0.146) | |
| IDR | 50 | 0.637 (0.146) | |
| CD20 | Total density | 150 | 0.488 (0.162) |
| Stromal density | 150 | 0.503 (0.152) | |
| Epithelial density | 140 | 0.51 (0.149) | |
| IDR | 150 | 0.566 (0.151) | |
| ICOS | Total density | 10 | 0.503 (0.1417) |
| Stromal density | 10 | 0.504 (0.141) | |
| Epithelial density | 30 | 0.513 (0.142) | |
| IDR | 40 | 0.583 (0.162) | |
| CD11c | Total density | 10 | 0.518 (0.148) |
| Stromal density | 10 | 0.493 (0.147) | |
| Epithelial density | 140 | 0.572 (0.157) | |
| IDR | 50 | 0.64 (0.134) | |
| CD163 | Total density | 40 | 0.51 (0.149) |
| Stromal density | 10 | 0.427 (0.132) | |
| Epithelial density | 70 | 0.567 (0.142) | |
| IDR | 140 | 0.603 (0.149) |
| Feature | HR | p-Value |
|---|---|---|
| Positive re-TUR | 4.9321 | 0.0001 |
| CD11c IDR | 0.0012 | 0.0002 |
| CD8 IDR | 0.0379 | 0.005 |
| pT1 | 2.0445 | 0.0159 |
| ICOS IDR | 0.0768 | 0.0388 |
| G3 grade (WHO 1973) | 1.8254 | 0.0522 |
| CD163 IDR | 0.0712 | 0.0549 |
| CD8 density total | 0.9984 | 0.0648 |
| CD8 density epithelial | 0.996 | 0.0857 |
| CD8 density stroma | 0.9988 | 0.0988 |
| Tertiary lymphoid structures | 1.6915 | 0.1033 |
| ICOS density epithelial | 0.9963 | 0.1375 |
| High grade (WHO 2004) | 2.5873 | 0.1899 |
| Features | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Model: positive re-TUR + CD11c IDR | |||
| Positive re-TUR | 4.3411 | 1.9616–9.6072 | <0.001 |
| CD11c IDR | 0.0282 | 0.00097–0.824 | 0.038 |
| Model: pT1 stage + CD11c IDR | |||
| pT1 stage | 2.2524 | 1.2449–4.075 | 0.007 |
| CD11c IDR | 0.00067 | 0.000017–0.268 | <0.001 |
| Model | AIC | Mean CI |
|---|---|---|
| CD11c IDR + positive re-TUR | 257.8785 | 0.7427 |
| CD11c IDR + pT1 | 338.225 | 0.703 |
| CD8 IDR + TLS | 352.2153 | 0.6449 |
| ICOS IDR + G3 | 361.1213 | 0.6364 |
| CD8 IDR + pT1 | 354.4931 | 0.6308 |
| CD163 IDR + TLS | 358.9342 | 0.6204 |
| ICOS IDR + TLS + G3 | 356.6093 | 0.6143 |
| CD163 IDR + G3 | 359.7073 | 0.6102 |
| CD8 total density + TLS | 360.0685 | 0.6084 |
| ICOS IDR + pT1 + TLS | 357.7706 | 0.6078 |
| ICOS IDR + pT1 | 359.8559 | 0.6019 |
| ICOS epithelial density + G3 | 360.1979 | 0.5974 |
| CD163 IDR + pT1 | 358.9573 | 0.5972 |
| Characteristic | Value (%) |
|---|---|
| Patients | 155 (100%) |
| Age, years | |
| Median (range) | 69.8 (33–89) |
| Gender | |
| Male | 127 (81.9%) |
| Female | 28 (18.1%) |
| RFS time, months | |
| Median (range) | 16.3 (1.6–60) |
| Recurrences | 46 (30%) |
| Tumor grade WHO 2004 | |
| Low | 12 (7.7%) |
| High | 143 (92.2%) |
| Tumor grade WHO 1973 | |
| G1 | 5 (3.2%) |
| G2 | 67 (43.2%) |
| G3 | 83 (53.6%) |
| pT stage | |
| Ta | 94 (60.6%) |
| T1 | 61 (39.4%) |
| Carcinoma in situ association | 8 (52%) |
| Positive re-TUR | 55 (45.5%) |
| Recurrent tumor | 45 (29%) |
| Multiple tumors | 76 (49%) |
| Tumor size > 30 mm | 43 (31.9%) |
| EORTC risk group | |
| Intermediate | 71 (45.8%) |
| High | 67 (43.2%) |
| Very high | 5 (3.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drachneris, J.; Morkunas, M.; Fabijonavicius, M.; Cekauskas, A.; Jankevicius, F.; Laurinavicius, A. Spatial Distribution of Macrophage and Lymphocyte Subtypes within Tumor Microenvironment to Predict Recurrence of Non-Muscle-Invasive Papillary Urothelial Carcinoma after BCG Immunotherapy. Int. J. Mol. Sci. 2024, 25, 4776. https://doi.org/10.3390/ijms25094776
Drachneris J, Morkunas M, Fabijonavicius M, Cekauskas A, Jankevicius F, Laurinavicius A. Spatial Distribution of Macrophage and Lymphocyte Subtypes within Tumor Microenvironment to Predict Recurrence of Non-Muscle-Invasive Papillary Urothelial Carcinoma after BCG Immunotherapy. International Journal of Molecular Sciences. 2024; 25(9):4776. https://doi.org/10.3390/ijms25094776
Chicago/Turabian StyleDrachneris, Julius, Mindaugas Morkunas, Mantas Fabijonavicius, Albertas Cekauskas, Feliksas Jankevicius, and Arvydas Laurinavicius. 2024. "Spatial Distribution of Macrophage and Lymphocyte Subtypes within Tumor Microenvironment to Predict Recurrence of Non-Muscle-Invasive Papillary Urothelial Carcinoma after BCG Immunotherapy" International Journal of Molecular Sciences 25, no. 9: 4776. https://doi.org/10.3390/ijms25094776