



- Review

The 50 Highest Cited Papers on Patellofemoral Instability
- Federica Denami,
- David H. Dejour and
- Michele Mercurio
- + 6 authors
The aim of this research was to identify the 50 articles most frequently referenced concerning patellofemoral instability (PFI) and to analyze their features. A search was performed in the Thomson ISI Web of Science using keywords such as “patellofemoral instability,” “patellar instability,” “patellar dislocation,” and “patella luxation.” This research included all publications related to PFI, covering aspects such as diagnostic and both nonoperative and operative treatment. The citation counts for the 50 articles ranged from 165 to 1024 citations. Notably, the top ten articles received a minimum of 348 citations each. In total, 84% (n = 42) of the studies were clinical, while the remainder consisted of basic science investigations (including three anatomical and five biomechanical studies). The predominant level of evidence was IV, accounting for 32%. The American Journal of Sport Medicine was responsible for publishing 34% of these articles. Most of the research took place in the United States and twelve additional countries. The years when the most-referenced papers were published spanned from 1985 to 2020, with the 2000s representing the highest share of articles (74%), and the years between 2006 and 2010 showing the peak quantity of articles (n = 15). This article provides a building block in the PFI management. The selection of these articles is useful for learning more about current trends on PFI and anticipating future developments.
10 February 2026
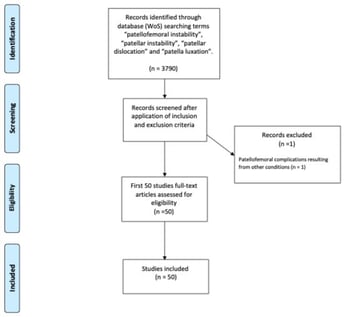

![PRISMA flow diagram illustrating the study selection process [16]. * Databases searched include MEDLINE (via PubMed), Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL). ** Records were excluded by human reviewers during the title and abstract screening phase based on the predefined eligibility criteria; no automation tools were utilized for this process.](https://mdpi-res.com/cdn-cgi/image/w=281,h=192/https://mdpi-res.com/surgeries/surgeries-07-00020/article_deploy/html/images/surgeries-07-00020-g001-550.jpg)


