- Review

Non-Lysosomal Glycogen Storage Cardiomyopathy with Hypertrophic Phenotype Due to PRKAG2 c.905G>A (p.Arg302Gln): Case Report and Narrative Review
- Pasquale Crea,
- Alice Moncada and
- Gianluca Di Bella
- + 10 authors
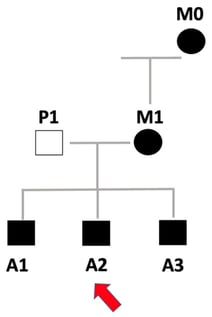
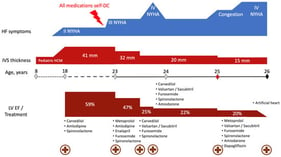
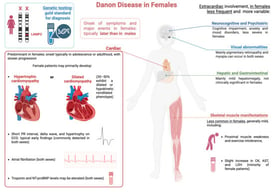
Background: PRKAG2 cardiac syndrome is a rare autosomal dominant glycogen-storage cardiomyopathy that mimics sarcomeric hypertrophic cardiomyopathy (HCM) but features ventricular pre-excitation, progressive conduction disease and concentric hypertrophy due to intracellular glycogen accumulation. The c.905G>A (p.Arg302Gln) variant is one of the most frequently reported pathogenic substitutions. Case summary: We describe a three-generation family carrying the heterozygous PRKAG2 p.Arg302Gln variant. The proband, a 41-year-old man, presented with paroxysmal atrial fibrillation, short PR interval and abnormal intraventricular conduction associated with concentric left ventricular hypertrophy and preserved ejection fraction. Holter monitoring disclosed episodes of high-grade atrioventricular block, prompting implantation of a primary-prevention dual-chamber ICD. Two gene-positive brothers exhibited milder hypertrophy but shared sinus bradycardia, ventricular pre-excitation and supraventricular arrhythmias; one underwent catheter ablation of a posteroseptal accessory pathway. The affected mother displayed a hypertrophic phenotype complicated by sick sinus syndrome and permanent atypical atrial flutter requiring pacemaker implantation. No relevant extracardiac involvement was detected in any family member. Review and novelty: Using this family as a starting point, we provide a concise narrative review of PRKAG2 syndrome with emphasis on the Arg302Gln genotype, molecular mechanisms and emerging treatment strategies. We highlight key multimodality imaging and tissue-characterization features that help distinguish diffuse, concentric glycogen-storage hypertrophy from the often-asymmetric pattern of sarcomeric HCM. Integration of our findings with published Arg302Gln cohorts illustrates the broad phenotypic variability in conduction disease, pre-excitation and atrial arrhythmias. Conclusions: PRKAG2 p.Arg302Gln-related cardiomyopathy should be suspected in patients with otherwise unexplained left ventricular hypertrophy associated with short PR interval, pre-excitation or early brady–tachy arrhythmias. Early recognition of red-flag features, systematic genetic testing, family screening and tailored arrhythmia/device management are crucial, while emerging gene- and pathway-targeted therapies may offer future disease-modifying potential.
21 February 2026